
Abstract
Several studies report that men, just like women, go through a complex emotional upheaval when they are about to become parents and that men need support to be able to tackle parenthood in the best way possible. This qualitative study addresses the extent to which parenting courses attended by both the mother and the father constitute an appealing institutional service for first-time fathers and whether they find them useful in tackling the challenges they face during the pregnancy and after the birth. The article explores difficulties with recruiting fathers to such courses and ensuring their continued attendance since men’s masculinity dilemmas can affect the extent to which they are willing to seek help and to complete such courses. The findings indicated that fathers’ sense of responsibility and awareness of their role as a father in their child’s life was strengthened, and overall, they were satisfied both with the topics addressed during the course and with the teaching. Strong networks were formed among some of the parents at the parenting course. Caution is called for when drawing general conclusions about the benefits of such courses for first-time parents, as they are seldom attended by parents with minority ethnic backgrounds or by vulnerable and underprivileged parents.
Keywords
Most studies on pregnancy and childbirth address mothers, thus focusing mainly on the importance of motherhood and the relationship between mother and child (Friedewald et al., 2005). Studies on guidance from health professionals have concentrated mostly on how mothers can be helped to improve their parental skills (Cabrera et al., 2018; Widarsson et al., 2015). While the focus on fathers and fathering has gained momentum over the past 20–30 years, inadequate acknowledgment of fathers as equal parents remains a central concern (Pålsson et al., 2017).
The present study addresses fatherhood and, in particular, what institutional assistance is available to help prepare first-time fathers for their roles and responsibilities. A focal point of this inquiry is whether it is appropriate to educate fathers and mothers together in courses or whether fathers draw greater benefit from male-only courses.
Fatherhood often has a long-term positive and protective effect on men’s health (Philpott et al. 2017). Nevertheless, several studies reveal that men, just like women, go through a complex emotional upheaval when they are about to become parents and that men also need support to be able to tackle parenthood in the best way possible (Etheridge & Slade, 2017; Madsen et al., 2002; Noergaard et al., 2017; Werner-Bierwisch et al., 2018).
Fatherhood has undergone significant qualitative changes, and the way that fatherhood and masculinity are connected today is more about intimacy and engagement than about authority, discipline, and being a breadwinner, as it was in the past (Cabrera et al., 2018; Lewis & Lamb 2007; Madsen et al., 2002; Nielsen & Westerling, 2014; Reinicke, 2016). Fathers increasingly report that they do not see paternity leave as a threat to their masculinity because a close relationship between father and child has become a self-evident aspect of fatherhood. Having children can make life more deeply meaningful and trigger profound existential reflection, and becoming a father is one of the moments in men’s lives when they are most likely to stop and think about their masculinity, lifestyle, and habits (Plantin, 2001). Modern fathers are very keen to be involved in their children’s lives and to prepare for becoming parents. This can prove challenging since there are few institutional platforms where men are encouraged to talk about their expectations of, and experiences with, becoming parents (Pålsson et al., 2017; Wells, 2016). Many fathers want to be included, to receive advice and information, but they feel overlooked, marginalized, and awkward in relation to the services that are available to them. Fathers often report that they are not satisfied with the way that health professionals treat them in the traditional birth preparation classes, as they feel sidelined and are only indirectly included in the parenting process (Doherty et al., 2006; Hallberg et al., 2010; Wells, 2016). Might it be the case that some existing health services disfavor men?
Despite the above-mentioned changes in fathers’ roles and forms of masculinity, compared with mothers, there are nowhere near the same amount of direct and targeted programs aimed at helping men and including them in the transition to parenthood as equal partners. Fathers can feel helpless and powerless. How can we explain this lack of focus on fathers? Is it because fathers are reluctant to take part in such programs, or does it have more to do with narratives about mothers with legitimate needs versus fathers whose needs are not really valid and who are therefore ignored?
Fathers’ problems risk being overlooked because they manifest in ways that neither the fathers themselves nor health professionals necessarily recognize as having to do with fatherhood. Society does not always “notice” when men need help because many men are socialized to conceal and distort their feelings, so men’s unacknowledged problems and unrecognized needs are therefore of central importance (Madsen et al., 2002; Reinicke, 2012).
Parenting courses, which attempt to cater for men’s needs during the transition to parenthood, are now offered in several countries. These courses vary somewhat in terms of their theoretical and ideological premises, as well as their structure, duration, and methods and which aspects of parenting, relationships, and family life they cover (Hallberg et al., 2010). Most share a number of features; notably, they all seek to prepare parents for becoming a family and to foster positive, collaborative, and egalitarian parenting. Nevertheless, little research has yet been carried out on whether parenting courses can make a difference in fathers’ transition to parenthood (Doherty et al., 2006).
Fathers usually decide to take part in parenting courses in order to support the mother (Premberg & Lundgren, 2006). A key question is, therefore, how to motivate more men to take part in activities targeted at fathers and how to recruit them. In order to recruit men to activities related to fatherhood, it is crucial to understand the factors involved in recruiting them and that this is not merely a matter of implementing good ideas based on good intentions (Reinicke, 2016). Rather, it often requires a profound understanding of men’s response patterns, since many men find it difficult to manage situations where they risk having to share intimate thoughts and feelings with each other (Brooks 2010; Rabinowitz & Cochran, 2002).
Research Questions
The overall research question concerns the service needs of first-time fathers. In terms of the concrete research question, this study investigates the effect of interventions to engage men during pregnancy. Do men find these interventions useful in tackling the challenges they face during the pregnancy and after the birth? Furthermore, the study also explores difficulties with recruiting fathers to such courses and ensuring their continued attendance. This is based on an assumption that men’s masculinity dilemmas can affect the extent to which they are willing to seek help and to complete such courses. These dilemmas might both be internal to the fathers and embedded in the health care and other systems that surround parenthood. More specifically the study is guided by the following questions.
How do parenting courses attended by both mothers and fathers constitute an appealing institutional service for first-time fathers?
To which extent do fathers find parenting courses useful in tackling the challenges, they face during pregnancy and after birth?
What are the obstacles when motivating men to take part in activities targeted at fathers?
Parenting Courses in Denmark
Compared to Sweden, which has offered mandatory parenting courses since 1980, such courses are relatively new and still voluntary in Denmark. And compared to existing initiatives in the field, family and parenting courses are also a new and unusual phenomenon in Denmark in that fathers are also invited—unlike in traditional “mothers’ groups.” It was only as recently as 2006–2007 that such courses were introduced in Denmark. To begin with, they were only offered in very few places. This has changed, however, and today around 25 Danish municipalities offer parenting courses. In some municipalities, these courses have even replaced traditional “mothers’ groups.” Their novelty lies in the fact that both parents take part in a joint learning process which is the point of departure for these family courses—something that has seldom been in focus in conventional training courses for soon-to-be and new parents, which are usually targeted at mothers and which typically foreground the mother–child relationship.
The parenting course studied in this article took place in a medium-sized Danish city of 52,000 inhabitants 30 km outside Copenhagen. The course is available to all first-time parents in the municipality and runs from weeks 23–29 of the pregnancy and until the child is around 15 months old. The course is not focused on specific challenges or problems, and no social matching is carried out when it comes to selecting the parents who can take part. What is special about the course is that the parents are offered help and support by public services even though they may not be experiencing any particular problems in connection with their parenthood. Each group consists of around 10 couples who are allocated a health professional who acts as a coordinator and leads the meetings. Ten meetings are held in total, and three of which take place before birth.
Content of Course
The parenting course is a holistic service that focuses on social and health issues, child psychology, relationships, and family relations, as well as economic and legal matters (Table 1). The aim of the course is to strengthen parents’ knowledge of, and insight into, the child’s development and needs, so that the parents acquire practical competencies and are able to create a good, healthy environment in which the family can thrive. Another central aim of the parenting group and meetings is to support the creation of informal parent networks that can provide mutual support and enable the sharing of experiences. The goal is to motivate the parents to help and rely on each other, thereby enhancing and prolonging the effect of the courses offered by the municipality. This again should encourage the parents to take responsibility for the health of their children and challenge the notion that health issues should be left only for health professionals (Roskilde Municipality 2019).
Titles of the Courses, Which the Parents Participated in.

The topics dealt with in the course are interdisciplinary: in addition to the expertise provided by health professionals about early contact and everyday life with the child, specialists are also invited in to talk about, for example, how families can best protect themselves legally and economically. The course format is dynamic and dialogue based and shifts among teaching, exercises, and competence training. Family courses are held alongside conventional health care, medical, and midwife visits.
Socioeconomic Characteristics of Participants
Despite the aim of mixing the parents and create a course that spanned social and economic divides, the course was mainly attended by relatively stable couples with similar socioeconomic backgrounds, who had been together for several years prior to the pregnancy. This meant that, in most cases, their pregnancies had been planned and desired. Regarding the parents’ relationship status, all the parents were cohabiting, and four couples were married.
The class perspective and demographic information appear to be important since the participants were quite homogeneous: all were ethnic Danish, in a relationship, heterosexual, and were either getting an education or had completed one and had a job. Regarding the length of the education, only one of the fathers had been enrolled in higher education, whereas the other fathers had been enrolled in continuing or further education. All parents were aged between 25 and 35 years. The average age of the fathers was 31 years. This demographic and social composition reflects that of other studies on group-based parental preparation, which also identify that parents under 25 years of age seldom take advantage of such institutional services (Fabian et al., 2006; Hjelte et al., 2015).
Research Design and Methods
The research was designed as a qualitative study. The data-collection strategy did include interviews, a group interview, and observations. Nevertheless, most of the empirical data used in this article are the output of semistructured interviews with 10 fathers who had completed the parenting course described above (Brinkmann, 2013). One consideration with respect to sample size is the number needed for the data analysis. The purpose of the study and a review of similar studies have provided guidance for the sample size, which are used in this study (Sandelowski, 1995).
The interviews with fathers focused on their experiences of, and benefits from, participating in the course and on whether they had to overcome cultural and social norms in order to attend the course. Although fatherhood and masculinity are in focus in this article, mothers were also interviewed to gain insight into their assessment of what the father’s participation in the course had meant for them and for the overall family dynamics. It is not easy to determine when enough data are collected to reach data saturation. Data triangulation has been used to achieve data saturation due to the relatively small number of fathers in the study (Denzin, 2009). To enhance the credibility of the analytical process, a group interview was also carried out with five health professionals who had experience coordinating such courses in the municipality. The goal of the group interview was to encourage discussion and reflection among the health professionals about their experiences with leading family groups. Furthermore, to increase the trustworthiness of both the interviews and the group interview, the author made observations of two course sessions each lasting 2 hours where field notes were conducted. The purpose of the observations was to study the parenting course in its natural setting to better understand the meaning it brought to the fathers (Denzin & Lincoln, 2008; Mulhall, 2003).
Interview Procedures and Data Analysis
Fathers were recruited through the health-care services: specifically, the health professionals asked participants in some of the courses if they would be willing to take part in an interview about their experiences with, and the benefits of, the parenting courses. The interviews were carried out during autumn 2017 and took place on the health service premises and lasted 40–80 minutes each. The average length of the interviews was 58 minutes. The group interview with the health professionals lasted 78 minutes. A semistructured interview guide was used, which allowed the questions to be prepared ahead of time and simultaneously allowed the informants to express their views in their own terms.
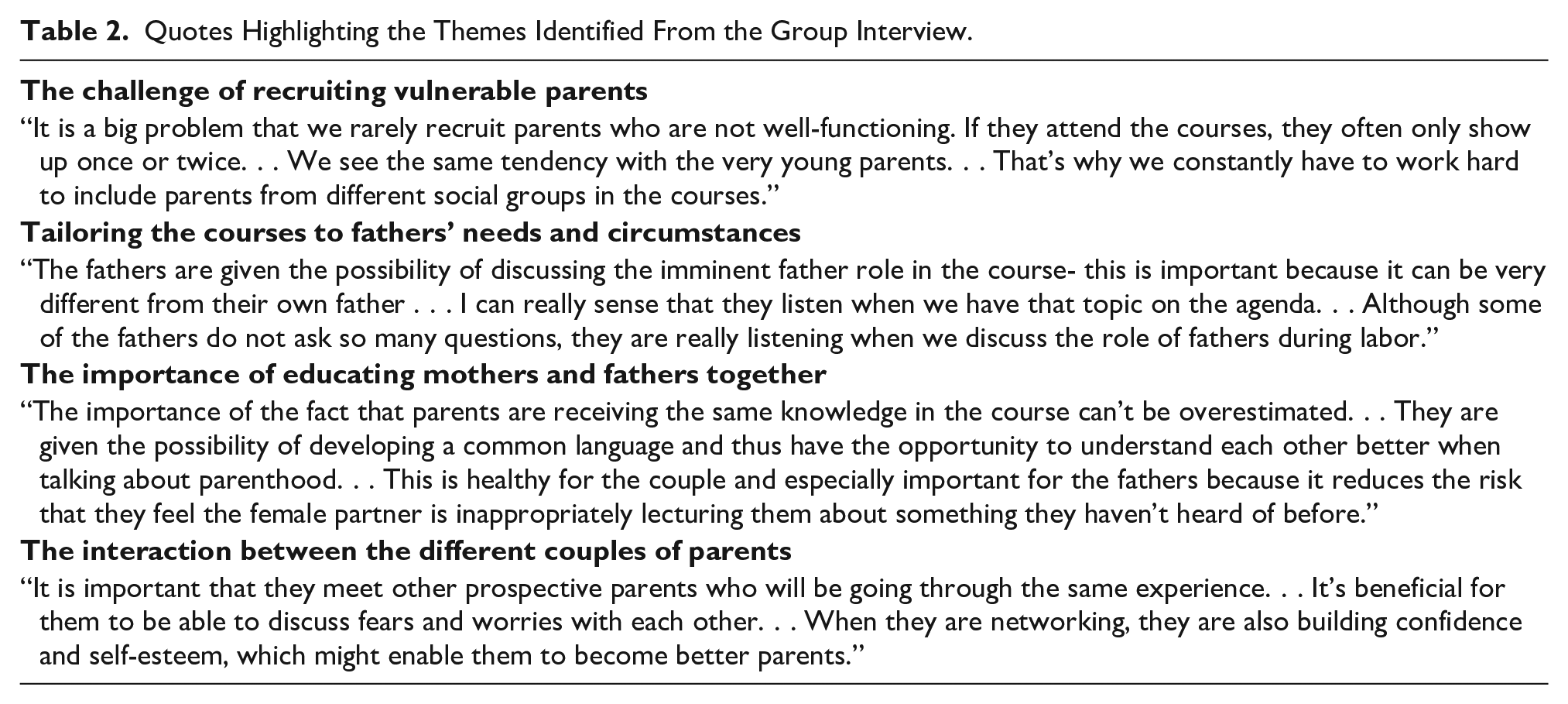
The author conducted the data analysis. The first specific step in processing the empirical data was that each interview was audiotaped and listened to by the interviewer 2–3 times to maintain the close connection to the oral discourse and to identify possible focal points prior to the next interview (Kvale & Brinkmann, 2009). This was done because new data might alter the questions that are asked. Inspired by Grounded theory (Strauss & Corbin, 1990) and as the second step in the analysis of the data, coding of the material was made inductively based on the view of the interview persons to avoid unnecessary predetermination from the researcher. Grounded theory has permitted the findings to develop and unfold in a reflexive interpretive way throughout the research process. It has been an aim to adhere closely to the raw information in order to better understand all types of reasoning and experiences (Kvale & Brinkmann, 2009). Grounded theory was used in the coding process for both the interviews with the fathers and the group interview with the health professionals to review and refine the material and to discover new themes in the narratives that had not explicitly been searched for, but which turned out to be significant for the design of the main themes in the result section (Charmaz, 2006). The data were initially coded with reference to various concepts or words describing what was being talked about. This made it easier to create an overall picture of the collected material. The following themes were identified and developed from the interviews to structure the analysis: the content of the course, the pedagogical approach, the role of the health professional, and the interaction with the other parents. The specific themes, which were determined from the group interview included the challenges of tailoring the courses to men’s needs and circumstances, the importance of educating mothers and fathers together, the challenge of recruiting vulnerable parents, and the interaction between the participating couple of parents. The coding process and identifying and labeling of concepts and phrases have also been inspired by the theoretical framework on first-time fathers with a focus on personal, relational, socioeconomic, and institutional factors. The data analysis has been a combination of a bottom-up analysis and top-down theory-led reading where the intake of information, to a certain extent, emerged from the analyses and some developed a priori. The bottom-up approach did allow a wide pool of specific characteristics to be considered in the analysis, whereas the top-down theory focuses its analysis on systematic and comprehensive factors (Table 2).
Quotes Highlighting the Themes Identified From the Group Interview.
Findings
What Did Fathers Get Out of the Parenting Course?
Regarding the course content, most fathers reported that they had appreciated the information and knowledge they had gained from the course. They identified the topics as relevant and thought that the knowledge they acquired gave them a realistic picture of what it meant to become a father. Several fathers emphasized the personal benefits and practical skills that the course had given them, as well as social aspects such as new friendships. The fathers appreciated the opportunity to share both good and bad experiences of their newly acquired identity as fathers with other men and families. One father stated: as a first-time father it can be really overwhelming . . . I think it’s very healthy for men to meet other fathers . . . there are so many things you are insecure about.
At the same time, a lot of their fears and anxiety had been dispelled. The fathers pointed out that some of the information they had been given during the course was available on the internet and in books, but that it was still more helpful to talk about the issues in question with others because they could learn from each other’s experiences.
Fathers reported that the concrete tips and advice they had been given in relation to the child’s general development had been particularly helpful—for instance, information about how to encourage their child and stimulate his or her linguistic development, about sleep and first aid, and about how they should react to various childhood illnesses. This is in line with Persson et al. (2012) who emphasized that fathers felt secure when they were heard and when they have some knowledgeable health persons to ask about concrete advice. Their views were more mixed when it came to topics that were broadly related to parenting but which did not directly address practical childcare skills, including legal aspects of parenting such as how to insure oneself and one’s child and what it costs to bring up a child. Quite a few fathers pointed out that much of this information was superfluous. Nevertheless, one additional bonus of the course may be that it helps to demystify public services in general, since the course can function as an unintended point of access to other social and health services available to first-time parents. Several of the fathers talked about how they had shared experiences regarding various support services available to them as parents.
Numerous of the fathers pointed out, however, that the course had helped them to tackle the new challenges they faced in their everyday lives and to understand their child’s development. The fathers claimed that they had become more responsible as a result of attending the course and that it had become a natural thing for them to feed their children, change their nappies, and tuck them in at night. One of the most enthusiastic fathers emphasized: I’m more active than many of my friends who also have children . . . I’m more involved in things at home than a lot of my mates are . . . it sounds to me as though they do more things with their children outside the home.
Studies report that not all fathers find parent groups very appealing, as they regard them as too intimate and competitive and as unsuitable forums for discussing sensitive issues (Pålsson et al., 2017; Premberg et al., 2008). Some of the fathers seem to have found parts of the course too intimate. One of the course sessions addressed the issue of relationships in the immediate post-birth period, such as the challenges that lack of sleep and the intense focus on the child could pose for a couple’s intimacy, including their sex life. The fathers represented different types of masculinity (Anderson & McCormack, 2018), and some of the fathers also mentioned that they had appreciated this particular session.
The Course’s Pedagogical and Didactic Approach
The teaching approach used on the course seems to have created a secure atmosphere that fostered self-reflection among participants. More than a few of the fathers pointed out that the health professional’s role had been important, since, in addition to attending all 10 sessions, she had also helped to create an informal and relaxed atmosphere which had put them at their ease. Although the participants were relatively homogeneous, it was hard for some of the fathers to open up in front of people they did not know before the course. To foster a sense of togetherness, a light meal was served at every course session, which proved to have a positive effect, especially on the fathers’ mood and involvement. As one of the fathers put it, “I love their rye crackers!”
According to the literature, some men in parent groups feel that they lack sessions that focus explicitly on the father’s role (Kerstis et al., 2017). This criticism did not arise in the study here, where it was evident that the health professionals were sufficiently good at relating to the father’s role whenever the subject arose naturally during the various course sessions. However, some of the fathers reported that they had felt overlooked during sessions with the midwife, that their presence was not really desired, and that they had felt “uncomfortable,” but that this had not been the case on the parenting course.
Based on the fathers’ accounts, it seemed as though the health professionals were very aware of men’s specific challenges and had the right communicative competences to ensure that the fathers felt welcome, included, and understood. As one father explained: I didn’t feel as though I was being ignored . . . or that it was a “women’s thing” I was attending . . . we were also asked our opinion and listened to.
In the case of this course, it appeared that the pedagogical approach was inclusive for both fathers and mothers. For instance, film clips were shown along with questions for reflection that related to the course session topics, and in the rooms where the course took place, there were mattresses, cushions, and toys so that parents could enjoy a rough and tumble with their children on the floor. One father mentioned the session on “development, play, and exercise,” which involved a visit to a sports kindergarten (a kindergarten with a special focus on developing children’s motor skills through play and physical activity), as a concrete example of how the course was adapted to men. The entire session was based on physical activity and took place in a sports hall equipped with climbing walls and ropes, stall bars, and swings. The goal was to show parents how to engage their children in exercise and play using a few simple accessories. Most of the session was spent exploring how parents could use the specially designed spinning tops, swings, etc., to capture their children’s attention.
Several of the fathers remarked that it had been useful and positive that a “men’s table” and a “women’s table” had been set up at several of the course sessions, where men could talk about their views on the day’s topic and their expectations of fatherhood. One father described it as follows: I liked the ‘men’s table’ because it was possible to speak more freely about our own challenges and the many issues surrounding labour when the women were not listening.
The above-mentioned quotation indicates that the fathers used the men’s table to reflect on their role as fathers and to share their experiences with other fathers. They emphasized that they could speak more freely when their partner was not present and that they appreciated this moment of “gender segregation” during the family course. Fathers were also asked if they would consider taking part in fathers’ groups, as studies identify that these are a good way to provide support and to ensure that the focus is on topics that are relevant to fathers (Friedewald et al., 2005; Kerstis et al., 2017). A few of the fathers interviewed thought this was a good idea, but most of them did not find the idea of fathers’ groups in the least bit appealing. One father clarified: I would never have taken part in a group for fathers only . . . that’s not my thing at all . . . it’s been great, really good, that we’ve been able to meet both other fathers and mothers.
Fathers were happy that a male perspective had been built into the course and did not request activities targeted exclusively at men. The fathers who take part in fathers’ groups are often well educated, in stable relationships, and socially and economically robust. They also tend to take longer paternity leave and to have positive attitudes toward gender equality (Kerstis et al., 2017).
Interaction and Networks With Other Parents
Several of the fathers described how other parents’ stories helped them to get a sense of what was “normal” and that it was good to get advice from people other than health professionals, in order to enjoy a more eye-to-eye exchange of ideas. Strong networks were formed among some of the parents, which evolved into genuine friendships that persisted after the course had ended. These networks were quite diverse and included social events like trips, dinners, outings to the movies, Facebook groups, and threads on Messenger. Some fathers explained how important it was for them to meet up with the same parents each time and that after the first couple of sessions, they turned up to “enjoy the socializing” since they got along so well with the other participants. One of the fathers described how he and two other fathers from the course met once a week as they were all on paternity leave at the same time. A number of fathers described the synergy that had arisen during the course due to the fact that all the couples were in the same boat and were in the midst of the same life experience. As one of the fathers put it: We all had the same questions, which meant you weren’t just sitting around getting bored.
Not all the parents got together outside the course sessions, and some admitted that they regretted that the parents had not had more contact after the course and that their participation had only resulted in superficial acquaintances.
Women’s Views of Men’s Attendance at the Course
Mothers and fathers largely seemed to be equally satisfied with the course. Studies report that it is often mothers who are the driving force behind a given couple’s participation in parenting courses and that the father’s early involvement is often due to the fact that the mother places great importance on this (Plantin et al., 2011; Premberg et al., 2008; Premberg & Lundgren, 2006; Widarsson et al., 2015). Social support from the father can have a positive and stress-reducing effect on the mother, and early involvement by the father during the pregnancy can lay the foundations for greater involvement in childcare later on (Reinicke, 2016). Several mothers stated that it was a good thing that the fathers also learned about breastfeeding and that as a result of the couple’s joint attendance at the course, mothers could no longer claim to be better informed than fathers since the latter had received exactly the same information as they had. One mother stated: I think it was important for many of us women that the men were there when we learned about breast-feeding, so they also understood what kind of feelings you can have . . . in many other contexts like at the doctor’s or with the midwife, it’s mainly targeted at the woman.
Almost all the mothers emphasized the fact that family preparation was a joint project. They underlined the importance of having a common frame of reference and that both parents had attended the course. Several mothers described how, before the course, the mothers had been used to coming home from visits to the doctor or midwife and telling the father what they had learned there, and they contrasted this with the complicity that arose during the course where both parents received the same advice and tips at the same time. This meant that fathers no longer “just” had to go along with mothers’ interpretations of health professionals’ advice but could also refer to topics and incidents that they had experienced themselves during the course. According to the mothers, this made their parenting more equal as it was now their “shared” child (rather than the “mother’s” child) whom they had to get to know together.
Which Fathers and Families Benefit From the Course?
A particular strength of the parenting course is arguable that it targets all new parents since it is impossible to know in advance which parents are vulnerable and need support. Men’s willingness to seek and accept help is affected by factors such as their social status, income level, and employment situation. In that regard, in some countries, there has been criticism that parental preparation courses mainly target socioeconomically privileged parents who are relatively well-functioning to start with (Fabian et al., 2006; Pålsson et al., 2017). The type of parents who take part in parenting courses might be expected to influence the outcomes and effectiveness of such courses. Although all participants have in common that they are soon-to-be or new parents—this being an important factor for building relationships and networks and for motivating them to attend—the parenting course did seem to be mainly designed for economically and socially robust couples who wished to improve their parenting knowledge and skills. The overall course concept and organization did not seem ideal for vulnerable parents with fewer resources. One father described his impression of a vulnerable family on the course: There was a couple there, we didn’t chat with them so much, but my impression was they came from a completely different social class . . . they were a bit younger than the other couples . . . and when we came for the first time she was standing outside smoking while heavily pregnant . . . and I thought, ‘you live in a completely different world to me’. He was the type who wears a baseball cap . . . and when it was her turn to pick a card that symbolized her, she took one with a picture of a burger and a television because she liked to eat while watching TV . . . He didn’t show up for many sessions, so then she started coming with her sister and they sat a bit apart from everyone else, and didn’t talk to the others much.
The above quotation shows how hard it can be for socially vulnerable groups to feel comfortable with this kind of course. It may be that the course design, with its 10 sessions and discussion with the other parents, assumes that parents have the mental energy, ability to articulate and reflect over personal problems, and share intimate aspects of their parenting with others, as well as the discipline to show up regularly over a 12-month period. Although the health professionals emphasized that they took great pains to integrate vulnerable couples, welcoming them back after any missed sessions with comments like “We missed you,” there is good reason to believe that vulnerable and less educated parents might not feel comfortable with this type of course format and may, therefore, be unlikely to complete it.
Recruiting and Retaining Fathers
Getting fathers to attend parenting courses involves several steps, which must take into account both the father’s motivation to start the course and his desire to complete it. Although fathers reported that they were satisfied with both the content and the organization of the course, it is not always easy to persuade fathers to take part in activities related to parenting.
As mentioned earlier, parenting courses are not very common in Denmark, and some of the difficulties in recruiting fathers may have to do with the fact that some midwives, nurses, and doctors still had the impression that family preparation is only targeted at vulnerable families and are therefore reluctant to recommend the course (Hjelte et al., 2015; Reinicke, 2016). This perception that the family course was mainly targeted at vulnerable families was confirmed by both mothers and fathers, who admitted that they had felt a bit strange and stigmatized at first for attending a course on family preparation. One of the fathers described how he had almost felt “underprivileged” because he had taken up the offer and that he had really not been sure about whether or not to attend the course: I really wasn’t sure whether or not to take part . . . what it’s all about . . . first birth preparation and now family preparation . . . but if I had known what I know now about the course, and what it would turn out to be like, I wouldn’t have thought twice about it . . . but my expectations of the course weren’t very high.
Not all fathers were so skeptical, however. As one father put it, “It can’t do any harm to take part,” and he explained that he felt that, by attending the course, he was showing that he was on top of things and that he stood for a modern kind of masculinity. Others said they had attended out of sheer curiosity, while others still claimed that they took part because they did not feel their own parents’ advice was useful.
One of the fathers explained how he had some friends who had also become fathers but who had not been offered the chance to take part in a parenting course—but that even if they had, they probably would not have done so. However, as he put it: After we’d been here the first couple of times, I could easily have argued for why it’s a good idea to take part.
This statement suggests that taking part in parenting-related activities can be stigmatizing and that men can experience barriers to doing so if other men in their circle do not support their attendance. But what points are particularly important to bear in mind when targeting fathers? The ability and desire to ask for help is a complex and dynamic process that depends on the person who needs support, the institution offering support, and the type of support needed (Mahalik et al., 2013). Thus, it is important to create a feeling of legitimacy for the men. All situations where men potentially have to seek help will inevitably give rise to tension between the benefits to be gained and the risks (Mahalik et al., 2007). Many men are therefore rather negative toward the social and health services available to them whose goal is to offer solutions to their problems (Möller-Leimkühler, 2002). Parenting courses which also include men should, therefore, be prepared for the fact that, even if the courses are adapted to men’s needs, there is no guarantee that fathers will attend them.
Apart from the problem of justifying their attendance at parenting courses, regular attendance at the courses can be problematic for men due to inflexible working hours. The meetings are held between 4 pm and 6 pm so that fathers who are not on paternity leave are also able to attend. Still, several of the fathers interviewed for this study reported that they had missed some sessions due to work. The tendency for fathers to cancel more than mothers is also reflected in the evaluations of Denmark’s most long-standing parenting and family course, where fathers account for 70% of no-shows (Mhtconsult, 2014).
Discussion
Regarding the impact of the course, it appears that the support, inspiration, and information that fathers received during the 1-year course generally met the course goal to strengthen parents’ competences and help them to feel more secure in their role as parents. Fathers’ sense of responsibility and awareness of their role as a father in their child’s life was strengthened, and overall, they were satisfied both with the topics addressed during the course and with the teaching.
It seems that the parenting course in this study did adequately address men’s needs as parents. Studies have reported that health professionals’ empowering behavior seems to be essential for fathers’ sense of security (Ekström et al., 2013; Persson et al., 2012). It is therefore crucial to emphasize the importance that parenting courses are taught by professional staff (Pinquart & Teubert, 2010). However, other studies have also revealed that, even if parenting courses are taught by health professionals, there is a risk that fathers can feel superfluous and that their needs are not in focus (Pålsson et al., 2017; Petersson et al., 2004; Steen et al., 2012).
Fatherhood is one area where it is relatively easy for men to open up and talk about their feelings and views regarding relationships (Plantin et al., 2011). Nevertheless, men’s willingness to seek and accept help is also affected by factors such as their social status, income level, and employment situation (Mahalik et al., 2013). It is important not to underestimate the personal struggle that some men go through to convince themselves that attending a parenting course can be both helpful and acceptable. Men’s “it’s a good idea in theory” attitude to taking part in “events for fathers” should be taken into account. That attitude might be prevalent among men who are not necessarily against the idea of services, which also include men who often do not proactively respond to these opportunities. There can be a mismatch between rhetoric and practice because, although many fathers think it is a good idea in principle to take part in parenting groups, they do not always find it easy to do this in practice, as many underestimate how far out of their comfort zone they will find themselves if they take part (Seidler et al., 2016).
Based on this study, it would seem that fathers saw themselves as equal in terms of their parental role and that the courses were both meaningful to them and catered for their needs, which can sometimes be a challenge in gender-mixed parent groups. Although fathers’ wishes and needs can be difficult to identify and meet, the majority of fathers reported that they were satisfied with the degree of involvement and inclusion during the course and that there had been space for debate and sharing experiences. The health professionals had both the time and the competences to attend to the fathers, and the latter described how they had been able to express their opinions during the course and that overall, they had “felt at home.” Though it is difficult to single out which elements had the greatest effect and which concrete behavioral changes the course triggered, fathers’ participation in family courses in all likelihood helps them to feel less sidelined when it comes to their imminent or new parental role. This is crucial because studies have identified that fathers often experience stress in the perinatal period (Brooks, 2010; Philpott et al., 2017).
In line with Green and Levack (2010), this study indicates that implementing gender-synchronized activities might serve to increase the synergistic effect of the work. The strategy of bringing the mother and father together in the parenting group while also working separately with them at the “men’s table” and “women’s table” promotes dialogue and knowledge and ensures a focus on both sexes and on their relationship as a couple.
Not all men, however, identify to the same extent with the new ideal of the caring and intimate father. There are still tensions between the caring and bread-winning aspects of male identity in the construction of fatherhood (Reinicke, 2020). Another pillar of some men’s masculinity is the principle of self-sufficiency and a reluctance to seek help from others, and cultural and social factors can, to a great extent, explain why fewer men than women reach out and seek support. The reason why men sometimes reject help can be that they feel less of a man if they start to open up about their worries and feelings of helplessness because they were brought up to be independent and autonomous (Mahalik et al., 2007). This aspect of male identity should not be underestimated, even though many men nowadays also focus on being caring and nurturing fathers. It is therefore crucial to design such interventions in a way that challenges fathers without threatening their masculine identity.
Based on the data presented in this study and supported by the literature, it seems that fathers’ ambivalence about the courses depends on whether they are accustomed to sharing their worries and problems with other men (Mahalik et al., 2013). With reference to the title of this article concerning the duality between fathers’ attitudes toward and experiences with parenting courses, there is clearly quite a lot of work to be done in terms of convincing some fathers that the course is designed with their needs in mind and that they are the target group. The challenge is, therefore, not only to reduce fathers’ reluctance to participate but also to make them more aware of the benefits to be had from attending.
Looking at how this study can contribute to the broader literature on fatherhood, the findings on first-time fathers are, aside from being interesting in their own right, especially interesting when comparing parenting courses with fathers who take part in fathers’ groups, which are activities only for men. It seems persuasive that it is significantly easier to recruit a broad swathe of fathers to parenting groups rather than fathers’ groups, as fathers can justify their attendance by saying that they are there to “support” the mother. All the fathers who participated in the parenting course had stable, established social circumstances, and were cohabiting with the female partner. Nevertheless, it seems that a difference between the fathers who participate in parenting groups and the fathers who participate in fathers’ groups is that the latter represents a particular section of society who more often have completed a higher level of education. The fathers who participate in the parenting courses are more likely only to have completed continuing or further education, to be in need of a push from their partner to participate in the parenting courses and to have a less positive attitude towards gender equality (Friedewald et al., 2005; Kerstis et al., 2018; Nolan, 1994).
One challenge faced by health professionals is that men are not traditionally socialized to ask for help. Although dominant perceptions of masculinity are changing, many men still believe that they should solve their problems by themselves (Seidler et al., 2016). A kind of asymmetry can, therefore, arise between the ideology and practice of modern fatherhood, in the sense that cultural expectations often change at a faster pace than concrete practices (Plantin, 2001). It can, therefore, be hard to persuade some men to ask for help, because to them, making use of institutional services can seem like a sign of weakness and vulnerability and because many men have no experience with creating or participating in networks that revolve around fatherhood. The literature reports that especially vulnerable fathers find it very awkward to turn up and articulate personal and sensitive matters in front of other fathers and admit that they need help in their role as fathers (Anderson et al., 2002).
Regarding practical issues, the organizers of parenting courses should ensure that they are held outside normal working hours to the extent possible. That is crucial in order for fathers to attend, as a relatively traditional division of labor where the father returns to work after a fairly short period of paternity leave is evidently still prevalent.
On the subject of the timing of the course start, all the interviewed mothers and fathers stated that they thought it was good that the course had begun during the pregnancy, when they had more time to focus on it, and that it had continued after the birth. However, research is not conclusive about when support services are most effective in preventing the crises that many first-time parents experience. Trillingsgaard et al. (2014) suggest that such interventions are best avoided during the pregnancy and should not begin until the child is approximately one and a half years old. Conversely, Pinquart and Teubert (2010) posit that optimal parenting courses take place over at least five sessions and should begin during the pregnancy and continue after the birth.
Limitations and Reliability
Considering the reliability of the results, the relatively small sample size makes it difficult to generalize about the outcome of the courses. In terms of the practical effects of the course, it is difficult to assess whether the knowledge and tools to which the fathers were introduced will actually be integrated into their everyday lives and whether the new knowledge, inspiration, and support provided by the course enhanced their sense of mastery and competence in relation to their role as parents. The interviews with the fathers were carried out 2–4 months after the course conclusion and, therefore, can only be used to shed light on the short-term effects of the course. It is also mentionable that there was no analysis of the dropouts due to study design.
It should also be emphasized that this study was situated in a high-income country and in the context of the Nordic policy framework known for its extensive welfare system and progressive attitudes and policies toward gender equality. Because of the father-friendly policies, new ideals of fatherhood have emerged with a focal point around engaged and involved fatherhood (Farstad & Stefansen, 2015). Thus, the findings may not be generalizable to all societies. For instance, the study by Tokhi et al. (2018) on the effectiveness of interventions aiming to involve men to improve maternal and newborn health in low-income and middle-income countries.
Conclusion and Implications for Practice
There are few moments in life when so many changes occur at the same time as when a couple becomes parents for the first time. These changes have to do with identity, responsibilities, and roles. The support that a family receives during the pregnancy and the first year of their child’s life can significantly influence both the child’s and its parents’ health and well-being. Parents who are adequately informed, able to develop the necessary parenting skills, and who have a social network as well as enough support from friends, family, and health professionals often find the transition to parenthood smoother (Reinicke, 2016).
Yet, caution is called for when drawing general conclusions about the benefits of such courses for first-time fathers, as they are seldom attended by fathers with minority ethnic backgrounds or by vulnerable and underprivileged fathers. It may be that the course design, with its 10 sessions and discussions with the other parents, assumes that parents have the mental energy, ability to articulate and reflect over personal problems, and share intimate aspects of their parenting with others, as well as the discipline to show up regularly over a 12-month period. In that regard, there has been criticism that parental preparation courses mainly target socioeconomically privileged parents who are relatively well-functioning to start with (Fabian et al., 2006; Pålsson et al., 2017).
Although in Denmark, there is no clear evidence yet of any specific effects of participating in parenting courses, it seems as though the latter focuses on factors that improve parental skills and mitigate potential relationship problems between the parents. The courses seem to have a stabilizing effect on the participating couples since they improve their ability to communicate with each other and solve conflicts. However, it may be unrealistic to assume that a 20-hour course would be likely to have a positive effect on the couple’s relationship for years to come.
As one of the health professionals put it: Our aim isn’t to prevent divorce . . . but perhaps the courses can lead to healthier relationships . . . they might end up getting divorced anyway but that might also be best for them in the end.
The success criterion for the course should be to produce more competent parents. Where fathers are concerned, this means ensuring that they take on an active and committed father role during the pregnancy and the child’s first year and that they regard fatherhood as an important part of their identity, in which case, as Ottesen (2016) points out, it is likely that they will continue to have regular contact with their children even if their relationship with the mother breaks down.
The way in which information about parenting courses is presented can greatly influence the extent to which parents find the course appealing (McCurdy & Daro, 2001). The fact that the family course is offered to all first-time parents may reduce the sense of stigmatization involved in attending. It is therefore important that, in addition to continually updating their skills so that they are also able to educate fathers, health professionals should also work holistically and in a cross-disciplinary way in order to ensure a shared sense of ownership over the courses. There may be a greater chance that parenting courses will be perceived as non-stigmatized, especially for men, if they are introduced as part of a broader restructuring of health care.
Footnotes
Acknowledgements
The author would like to thank the participants in the study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval obtained
This study and the collection of the different interview data were approved to be in accordance with standards for good scientific practice by the Committe for Research Ethics at Roskilde University, Denmark.
Informed consent obtained
Informed consent was obtained from all participants in the study in the following way: All the participants received written invitations describing the purpose and specific terms of the study. When the participants showed up on the scheduled day for the interviews, the conditions were repeated verbally with a specific emphasis on the measures taken to ensure confidentiality and anonymity in the report/article.