
Abstract
Wounds caused by human bites have a high infection rate. A 59-year-old male patient came to our poison control center because of soft tissue injuries in the left arm and left hand, pain, swelling, and necrosis. Before entering the hospital, he had a high fever. Physical examination found that the patient’s lips were dry, his tongue was dirty, his skin and mucous membranes were less pink, his pulse was 80 beats/min, and his temperature was 36.5°C. Information on May 9, 2024, the patient was bitten on the left arm by a child. The patient had a negative blood culture, a negative burn fluid culture, high-sensitivity C-reactive protein of blood chemistry is 458.1 mg/L, total blood cell analysis with white blood cell is 19.9 G/L, percent of neutrophil is 92.4, soft magnetic resonance imaging of the arm and hand areas with images is cellulitis under the skin of the left arm.The patient was injected with antitetanus toxin serum, antibiotics (Dalacin C, Linezonide, meropenem), and was infused paracetamol. After 1 day of treatment, the patient’s condition did not improve and worsened, so the patient was transferred to the National Burn Hospital for further treatment. This article aims to talk about soft tissue injuries due to soft tissue inflammation or necrosis that can occur in patients who are bitten by human. This is the first patient with soft tissue damage with cellulitis under the skin of the left arm known at our poison center.
Introduction
The human oral cavity secretes saliva. Saliva is 99% water; however, it is composed of a variety of electrolytes, including sodium, potassium, calcium, magnesium, bicarbonate, and phosphates. Also found in saliva are immunoglobulins, proteins, enzymes (amylase), mucins, and nitrogenous products, such as urea and ammonia. It is a unique secretory fluid which has many functions. Besides the human oral cavity, water contains many types of bacteria (commonly streptococci, Staphylococcus aureus, Eikenella corrodens, anaerobic bacteria; Aziz et al., 2015; Fallouji, 1990). When bitten, it can cause infection, with a rate ranging from 2% to 25% depending on many factors such as: the shallowness and depth of the bite, the location of the bite, and the physical factors of the person biting (e.g., the biter’s oral hygiene frequency; Fallouji, 1990; Moran & Talan, 1993). In most cases, signs of infection begin to appear 24 hours after the bite, but in some cases it can be as early as 2 hours after the bite. Infection may be superficial (cellulitis, with or without abscess) or deep (abscess, septic arthritis, osteomyelitis, tenosynovitis, or necrotizing soft tissue infection; Wolf et al., 1992).
Superficial signs of infection: Clinical manifestations of cellulitis include pain, erythema, swelling and warmth, possibly purulent discharge, lymphadenitis, and/or fever. Associated superficial abscesses may present as soft, erythematous, mobile nodules.
Signs of deep infection: In addition to the above manifestations, signs of deep infection include persistent or progressive pain several days after the initial injury, pain with passive movement, pain that does not correspond to the results of the examination, joint swelling, systemic signs such as fever, hemodynamic instability, and persistent signs of infection despite good initial wound care and antibiotic use (Wolf et al., 1992). The severity of infection is increased in patients with immunosuppression (including diabetes) or neurologic disease, who often present later in the course of treatment but are at increased risk of infection. Higher severity of infection due to limited pain during clinical examination (Rothe et al., 2015; Schweich & Fleisher, 1985).
Case Report
A 59-year-old male patient with history of gout for many years, self-medication, and not following doctor’s prescription entered our antipoison center in the following condition: provincial, Glasgow 15 points, soft tissue injuries in the left arm and hand, swelling with a diameter increased by 2 cm compared to the healthy side, necrosis with an area of 6 cm2 wide, edema. The swelling spreads 20 cm to the near elbow, and the patient had no fever, no convulsions, and no difficulty breathing. It is known that on the evening of May 9, 2024, the patient was playing with a 3-year-old child and was bitten on his left arm. After the bite, there were tooth marks, pain, and a little bleeding. On May 10, 2024, the patient had swelling of the left arm and hand, severe pain, and highest fever of 39.5°C. The patient was admitted to Nam Dinh Provincial General Hospital of Vietnam, was diagnosed with cellulitis of the left arm and hand, and was treated with incisions, antibiotics, and intravenous fluids, but it did not help. On May 11, 2024, the patient was transferred to the Poison Control Center of Bach Mai Hospital, Ha Noi, Vietnam.
Clinical examination: Patient weighs 67 kg, height of 172 cm, body mass index of 22.6 kg/m2, pulse of 80 times/min, and blood pressure of 130/70 mmHg. The patient is awake, able to communicate, very tired, and with Glasgow 15 points and had dry lips, dirty tongue, skin and mucous membranes less pink, and no fever with 36.5°C. The stiff neck is negative, the meningeal stripe is negative, and heart is regular, with no pathological murmur. The lungs are evenly ventilated on both sides, without rales. Abdomen is soft and not bloated, with yellow stools and no diarrhea. Soft tissue wound on the left arm and hand, swollen, spreading 2 cm2 wide compared to the healthy side, necrotic area 6 cm2 wide, edema spreading 20 cm toward the elbow. Other agencies have not detected any abnormalities (Picture 1A, B, C).

(A, B, C) Clinic Picture of the Patient
Patients are given blister fluid, blood culture, and blood tests with result:
Two locations’ blood cultures: negative
Left arm blister fluid culture: negative
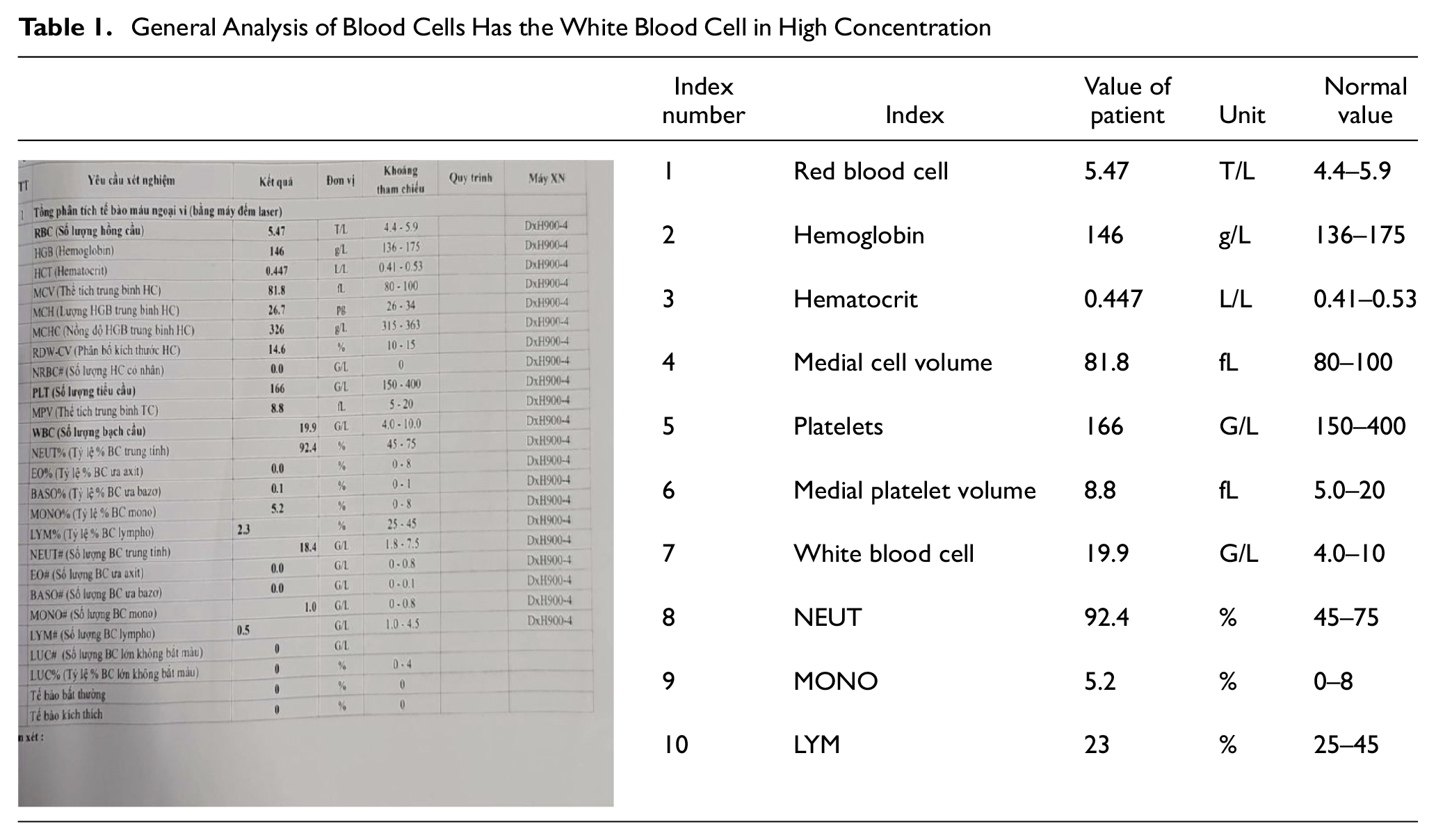
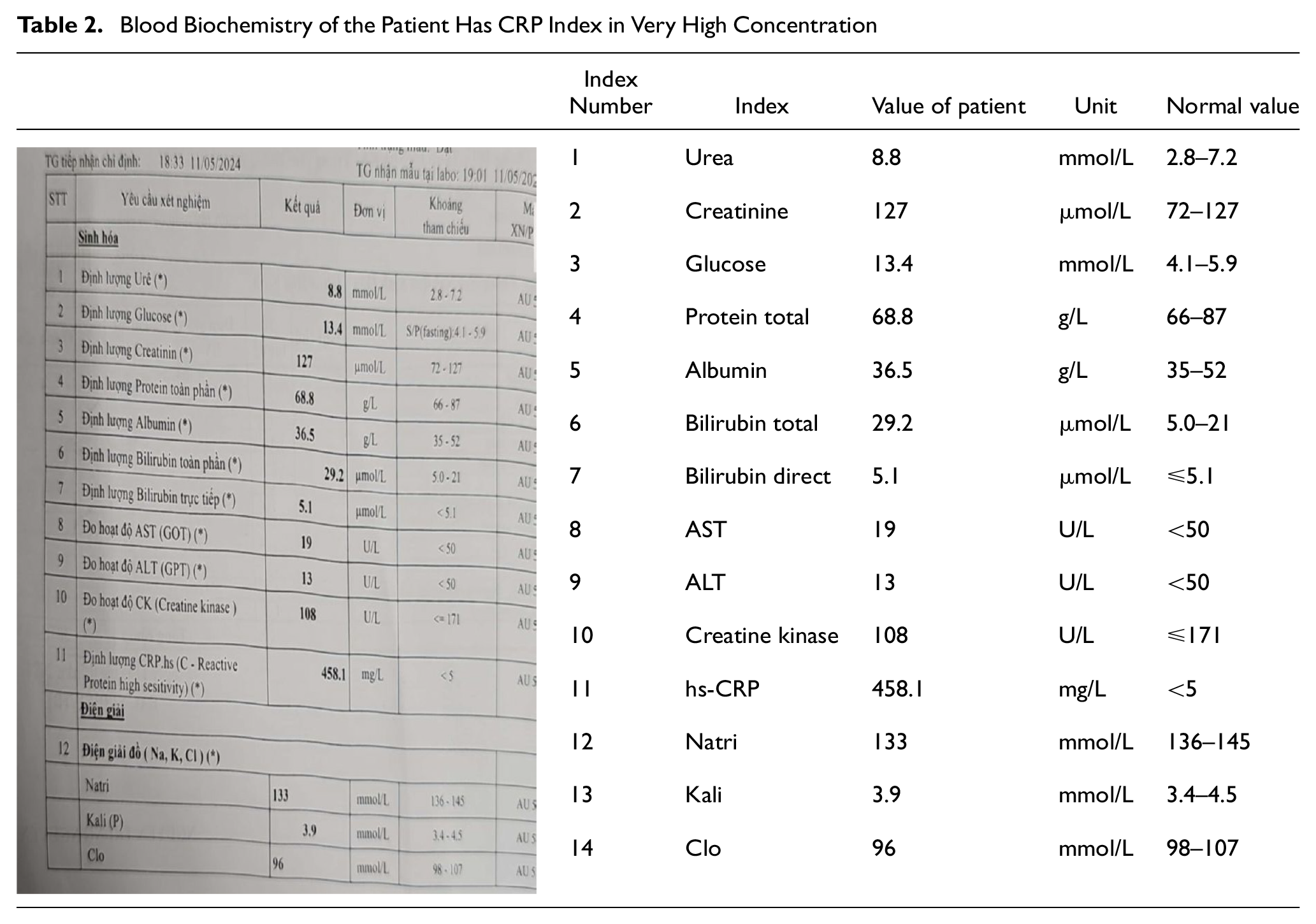
Blood coagulation tests were within normal limits. Blood cell count showed white blood cell of 19.9 G/L with neutropil 92.4% which is higher than normal value (Table 1). Blood biochemistry showed C-reactive protein of 458.1 mg/L which is much higher than normal value (Table 2). Magnetic resonance imaging of arm software shows cellulitis under the skin of the left arm (Picture 2). The patient was injected with antitetanus toxin serum, antibiotics (Dalacin C, Linezan, meropenem), and paracetamol. The patient’s condition then worsened: the patient had a fever of 38.5°C to 39°C. The soft tissue injuries in the lower left arm and left hand continued to swell more, the pain increased, and the patient was transferred to the National Burn Hospital for further treatment.
General Analysis of Blood Cells Has the White Blood Cell in High Concentration
Blood Biochemistry of the Patient Has CRP Index in Very High Concentration

Magnetic Resonance Software of the Left Arm
Discussion
The human oral cavity secretes many elements which consist of water, variety of electrolytes, sodium, potassium, calcium, magnesium, bicarbonate, phosphates and immunoglobulins, proteins, enzymes (amylase), mucins, and nitrogenous products, such as urea and ammonia. Besides it contains many types of bacteria (commonly streptococci, S. aureus, E. corrodens, anaerobic bacteria; Aziz et al., 2015; Wolf et al., 1992). Wounds caused by human bites can be accidental or intentional. When examined, a semicircular- or oval-bruised area may be found, there may be tooth marks, and the skin may or may not be intact (Bula-Rudas & Olcott, 2018; Wolf et al., 1992). Common locations are fingers, hands, and arms. People often tend to be subjective when bitten by another person. A few people will proactively give first aid to the wound, which can lead to subsequent infections. Human oral cavity water contains many types of bacteria (commonly streptococci, S. aureus, E. corrodens, anaerobic bacteria). When bitten, the skin may not be intact, combined with not being cleaned, allowing these bacteria to penetrate the tissues. The first symptoms are usually pain, swelling, heat, and redness (Aziz et al., 2015; Rothe et al., 2015). The patient may then have a high fever, with typical symptoms of infection. Our patient was admitted to the hospital because of soft tissue injuries in the lower left arm and left hand, swelling, increased diameter by 2 cm compared to the healthy side, necrosis with an area of 6 cm2 wide, edema spreading 20 cm to near elbow, anteriorly. At home, the patient noted fever, with the highest temperature of 39.5°C. The patient was injected with antitetanus toxin serum, antibiotics (Dalacin C, Linezan, meropenem), and infused paracetamol. The patient’s condition then worsened. The patient had a fever of 38.5°C to 39°C. The soft tissue injuries in the lower left arm and left hand continued to swell more, the pain increased, and the patient was transferred to the National Burn Hospital for further treatment.
Conclusion
In our patient, there were local and systemic signs of infection. Identifying patients with cellulitis after being bitten by a human is through taking medical history, clinical examination, and performing tests for the purposes of diagnosis and treatment (Kennedy et al., 2015; Wolf et al., 1992). Once again, we would like to emphasize that: wounds caused by human bites can cause serious infections, with a quite high rate, so they need to be treated promptly (Schweich & Fleisher, 1985). Early identification of signs of infection and close monitoring of the patient’s clinical and paraclinical condition help patients avoid more serious complications (Moran & Talan, 1993). This is the first case of a human bite causing cellulitis recorded at the Vietnam national poison control center.
Supplemental Material
sj-docx-1-jmh-10.1177_15579883241309766 – Supplemental material for Soft Tissue Inflammation of the Arm and Hand Caused by Human Bites
Supplemental material, sj-docx-1-jmh-10.1177_15579883241309766 for Soft Tissue Inflammation of the Arm and Hand Caused by Human Bites by Nguyen Dang Duc, Nguyen Phuong Sinh and Lam Nguyen Hong Anh in American Journal of Men's Health
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.