
Abstract
This study aimed to investigate the effects of psychotherapeutic interventions, specifically cognitive-behavioral sexual therapy, using the example of erectile dysfunction in a cohort of 58 Ukrainian men under the age of 40 years. To achieve this goal, questionnaire methods were employed, including questions from the International Index of Erectile Function and the Perceived Stress Scale, along with statistical data processing and subsequent discussion. Psychotherapeutic intervention demonstrated its effectiveness from the short-term perspective and over a period of 6 months, with a significant improvement in erectile function indicators and a reduction in distress scores in the group of patients undergoing combined therapy (p < .05). Monotherapy with phosphodiesterase-5 inhibitors, as first-line drug choices, also proved effective. However, considering that erectile dysfunction had an established psychogenic nature, the symptoms of the condition returned to the baseline level after 6 months. Providing psychosexual education and studying adaptive sexual responses with the disruption of maladaptive cognitive patterns should be a key goal in the treatment of psychogenic sexual dysfunctions. It is important to note that men may encounter difficulties in the practical application of various cognitive-behavioral sexual therapy techniques. Nevertheless, psychotherapy is considered a promising approach to treatment, especially in the context of countries where the topic of sexual education remains taboo, and the number of men seeking professional psychological help is very low, as is the case in Ukraine.
Introduction
According to the World Health Organization (WHO, 2023), half of infertile couples face difficulties conceiving due to male infertility. According to Szkodziak et al. (2020), the current prevalence of infertility among couples is 19%, with male infertility accounting for 50%, as stated by the WHO. The increase in cases of male infertility is a result of various factors, including social, economic, lifestyle, and environmental factors. Even with the advanced state of modern medicine, it is often challenging to determine the cause of reproductive disorders in men. Male sexual dysfunctions (SDs) encompass a range of pathological conditions such as erectile dysfunction (ED), delayed ejaculation, hypoactive sexual desire disorder, anorgasmia, priapism, sexual aversion disorder, genitopelvic pain associated with sexual activity, and premature ejaculation, with ED being the most prominent. However, these conditions can be interconnected, and individuals may experience more than one type of SD simultaneously (Minhas et al., 2021).
Knigavko and Dorina (2021) state in their article that the frequency of SD increases with age, considered an evolutionary mechanism of reproductive limitation associated with aging. However, in the modern context, only a small percentage of sexual activity is designated for reproductive purposes, with most sexual acts having a social and recreational character. An increasing number of young men are facing SD issues, requiring in-depth study of this problem. Etiologically, chronic prostatitis is identified as the most common cause of ED among young men, but the prevalence of diabetes, hypertension, post-COVID-19 complications, psychological stress, and obesity also plays a significant role (Gurzhenko, 2021; Luchytskiy et al., 2022).
Kornyenko et al. (2021), in their study on penile dysmorphic phobia, describe psychogenic SDs as integration problems that require collaboration between urology, psychotherapy, and reproductive specialists. In such cases, psychotherapeutic interventions such as cognitive-behavioral sexual therapy (CBST), mindfulness practices, hypnosedative therapy, and group psychotherapy are recommended. These therapeutic programs should be aimed at reducing the impact of anxiety, low self-esteem, and sexual beliefs on existing and progressing SDs.
Despite having a substantial information base, psychotherapy for various SDs still has relatively unexplored areas and merits further research. These include the influence of cultural factors on various aspects of identity (such as race, gender identity, sexual orientation), the implementation of technologies and online programs, long-term perspectives, the role of partners in psychotherapeutic interventions, the development of approaches considering traumatic experiences, and body image disorders. It is worth noting that diagnosing psychogenic SD is currently a complex process requiring detailed examinations and qualitative differential diagnostics, which may not always be available in non-specialized medical institutions (Wang et al., 2023).
Therefore, the aim of this study is to investigate the effects of psychotherapeutic interventions (specifically CBST) in the therapeutic process of male SDs, using ED as an example, in a cohort of Ukrainian men under the age of 40 years.
Materials and Methods
The design of this study is presented in the form of a cross-sectional survey of patients who underwent treatment from March 2021 to February 2022. The participants were allocated to the examination and control groups using simple randomization. The participants were allocated to one of the two groups using a random number generator, thus ensuring an unbiased allocation. The inclusion criteria for patients in the study were selected as follows:
Married men between the ages of 24 and 38 years who sought medical assistance for difficulties in conceiving due to suspected ED. The participants were required to meet specific diagnostic criteria as assessed by the International Index of Erectile Function (IIEF), with scores indicating a range from mild to severe ED. Furthermore, all participants provided written informed consent, indicating their voluntary participation in the research and understanding of the study procedures and expectations.
Regular sexual intercourse with their wives without using contraception for at least 1 year.
Seeking medical help due to difficulties in conceiving.
Providing informed consent for examination and research.
The exclusion criteria were as follows:
Diagnosed developmental defects of reproductive organs.
Severe comorbidities (oncological diseases, cardiovascular or cerebrovascular diseases, liver, and kidney diseases).
Diagnosed mental disorders.
Decompensated chronic diseases (diabetes, heart failure, chronic kidney disease).
The study included 58 patients, with 29 in the examination group and the other 29 in the control group, through randomization. The sample size of 58 male participants was determined based on the prevalence and accessibility of individuals who met the inclusion criteria, for example, married men seeking to conceive and experiencing ED. The study aimed to maintain a balanced design with an equal number of participants in both the examination and control groups (29 per group) to ensure adequate statistical power while adhering to the constraints of the study resources and the availability of participants within the specified timeframe from March 2021 to February 2022. The balanced sample size permits a comparative analysis of CBST in conjunction with pharmacotherapy versus pharmacotherapy alone. This has been demonstrated to possess sufficient power to detect meaningful changes in primary outcome measures, including the IIEF and the Perceived Stress Scale-10 (PSS-10) scores.
The preliminary assessment of fertility was conducted during consultations with a urologist and andrologist, including a detailed analysis of the spermogram. Patient surveys were conducted anonymously and included several blocks: 7 general information questions (age, height, weight, education, professional qualification, duration of marriage, presence of children), 15 questions to assess the IIEF, and 10 questions from the PSS-10.
The IIEF was used to assess the severity of ED, ranging from 5 to 25 points. Scores of 22 to 25 indicated no ED, 12 to 21 mild ED, 8 to 11 moderate ED, and 5 to 7 severe ED. The PSS-10 was used to screen the psychological distress level, with interpretation criteria as follows: 0 to 13 points for low distress, 14 to 26 for moderate distress, and 27 to 40 for high distress.
Each participant completed a paper questionnaire and self-assessed their reproductive and psychological health three times—within the last 6 months before the study, at the end of the study, and 6 months later during a follow-up consultation. All patients, regardless of the group, received basic treatment with phosphodiesterase-5 inhibitors (iPDE-5) according to local and national treatment protocols.
The examination group (No. 1) underwent an 8-week individual course of CBST twice a week for 50 minutes with a research psychologist. Missing fewer than three sessions was allowed, as the absence of more than 25% of course sessions was considered unsuccessful completion of the study conditions and led to exclusion. Each session was accompanied by assigning homework, which men were required to practice with their partners twice a week, followed by control by the research psychologist.
Data were analyzed using Microsoft Excel 2016 with the Analysis ToolPak. Continuous variables were presented as mean ± standard deviation (M±SD) and analyzed using the independent samples T-test for comparisons between Groups 1 and 2, as well as the dependent samples t-test for comparisons before and after interventions. p < .05 was considered statistically significant.
Results
During the introductory interview in the first psychotherapy session, participants were asked to respond to several questions related to their sexual experience and views on their own psychological and sexual health. When asked, “Do you believe that erection problems make you feel less complete?” 93% (55 individuals) of men responded affirmatively. On the question, “Do you believe that your erection problems may be related to stress/depression/anxiety?” only 55% (32 individuals) answered “Yes.” The other half of men either deny the impact of their psychological state on their sexual life or deny the existence of psychological problems altogether.
After the question, “Have you previously sought psychological help from specialists (psychologists/psychotherapists)?” only 10% (6 individuals) responded positively, indicating that men may often ignore the need for professional help. Various psychosomatic reactions, including SDs, may mask the development of intrapersonal conflicts that can evolve against the backdrop of stigmas associated with their own sexual health.
As shown in Table 1, patients in Group 1 underwent psychotherapy for ED to correct negative attitudes and automatic thoughts that hinder achieving adequate erection and sexual satisfaction during sexual intercourse. During the sessions, patients learned to derive non-sexual satisfaction together with their partners instead of instantly engaging in sexual intercourse. Ultimately, patients were guided through the process of cognitive restructuring of the myth that penetration is necessary for sexual satisfaction during every sexual encounter. This liberates the man from the intrusive idea of needing an erection, consequently reducing anxiety and stress levels before and during sex.
Content of Each Week of Psychocorrection by the Method of Cognitive-Behavioral Sexual Therapy

Source. Created by the author.
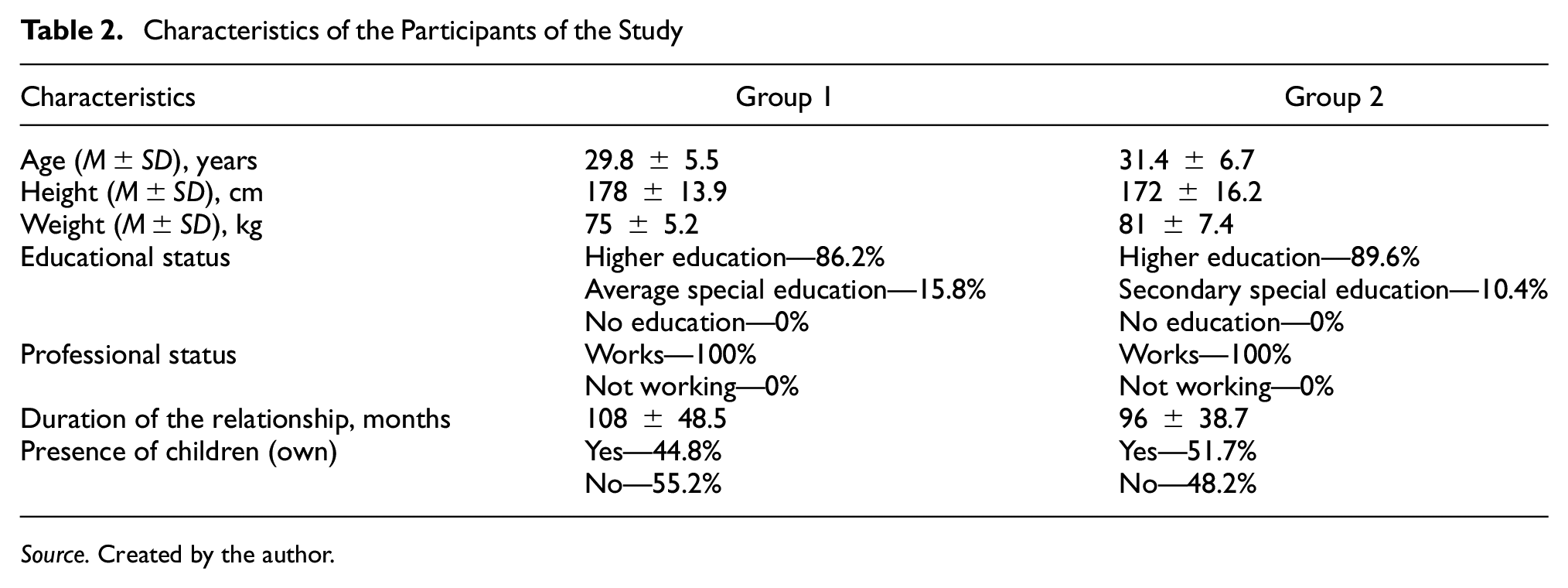
Participants’ characteristics are presented in Table 2. The minimum age of participants was 24 years, while the maximum age was 38 years for both treatment groups. It is worth noting that the anthropometric indicators of patients corresponded to age norms and likely could not have an impact on a man’s reproductive capabilities. All participants had educational qualifications, predominantly higher education—86.2% in Group 1 and 89.6% in Group 2, respectively. Moreover, 100% of the patients were employed (income levels and financial well-being were not assessed).
Characteristics of the Participants of the Study
Source. Created by the author.
The presence or absence of children in both groups was balanced at a ratio of 1:1, indicating that about half of the families seeking help for sexual health had already succeeded in conceiving a child. However, for certain reasons, new attempts to conceive were unsuccessful due to male factors. While this study did not conduct a factor analysis, a hypothesis can be formulated that the level of education, career responsibilities, and the presence of children may be influential factors in the state of sexual health. This could serve as a basis for further research, including in the current patient sample.
According to Table 3, the effect of combined therapy significantly differed from the standard pharmacological approach to treatment, as the CBST + iPDE-5 group demonstrated significant differences in IIEF scores after treatment compared to pre-intervention values, with the average score increasing in favor of mild ED, as compared to the control group (p < .001). These improvements also significantly differed during further observation after a repeat survey 6 months later, as more demonstratively depicted in Figure 1. Participants showed stability in IIEF scores with a slight decrease.
Received Estimates of the International Erectile Function Index

Source. Created by the author.

Dynamics of Changes in Index Values Under the Influence of Combined Therapy
The absence of further improvement could be explained either by the short time interval between the end of the conducted therapy and subsequent assessments, or it may be attributed to the imperfection of the developed program, as the duration and approaches of therapy may vary and be adjusted according to the individual needs of the patient. It is also worth noting the effectiveness of monotherapy with iPDE-5 in the short term (p = .05); however, upon observation after 6 months, a negative trend in the obtained IIEF scores was noted, likely associated with the persistence of a high level of stress, which will be further discussed.
Significant differences were identified between both treatment conditions regarding the improvement in stress level indicators, as reflected in Table 4. Despite these differences, both treatment conditions, both combined and monotherapy, proved effective in reducing distress levels to a moderate-to-mild degree. It is worth noting a significant percentage of patients experiencing a high level of distress, possibly associated with both personal factors and socio-economic circumstances, influencing overall well-being.
Received Scores of the Perceived Stress Scale

Source. Created by the author.
These factors could also be included in the list of potential risk factors for the development of psychogenic SDs. However, the combined therapy with the inclusion of psychocorrection was significantly more effective, with a high likelihood of reducing distress levels in Group 1 compared to the control group. This is because CBST focuses on replacing maladaptive cognitive patterns of thinking and behavior.
Among other things, a crucial element of CBST was exercises focused on sensory awareness and the “stop-start” method. These components were complemented by psychosexual education and training in the use of adaptive sexual responses. Some men reported difficulties in using the “stop-start” technique when attempting to delay sexual intercourse. Despite these occasional difficulties, CBST is considered a promising method of treatment, especially in countries where sexual education is a taboo subject, and the number of men seeking professional psychological help is low (Figure 1).
As it is seen from the results, the therapeutic properties of iPDE-5 contribute to the maintenance of erection but do not reduce feelings of anxiety among men taking these drugs. This is evident from the presented data, where the distress level, although decreased after pharmacological monotherapy, rose again during a follow-up examination after 6 months. This increase is likely associated with a decrease in scores of erectile function, further intensifying negative emotions and experiences for the man.
The effective role of psychocorrection in the treatment of psychogenic ED establishes it as a primary approach to therapy. The values, socialization, cultural, and gender norms among Ukrainian men can have a significant impact on sexual health and the formation of maladaptive behavioral patterns. Psychosexual education, debunking sexual myths, and restructuring beliefs about sexual life are essential components of interventions for SDs.
The modern discovery of the effectiveness of CBST in alleviating symptoms of psychogenic SDs underscores the role of a biopsychosocial approach in patient management. This demonstrates that non-organic factors also play a crucial role in the development and maintenance of ED, and psychocorrection can be introduced into the treatment scheme in combination with other therapeutic methods, such as pharmacological treatment with iPDE-5.
In accordance with the presented data and their interpretation, the following recommendations can be formulated:
In childhood and adolescence, males should receive mandatory sexual education appropriate to their age so that young individuals can develop adaptive sexual attitudes toward their bodies and intimate relationships from an early age.
Urologists and andrologists dealing with male sexual health should undergo training in the basics of psychocorrection or at least be cautious about the presence of psychogenic risk factors. This ensures that men with SDs can easily access psychocorrection interventions.
CBST should be prescribed to men with psychogenic dysfunctions for at least 8 weeks following the scheme proposed in this study. However, the duration and therapy plan can be adjusted according to the severity of symptoms and individual preferences.
Men with SDs should undergo screening for symptoms of anxiety, depression, and distress, and the IIEF and PSS-10 scales can be applied to monitor the progress of therapy.
Discussion
According to the latest European Association of Urology Guidelines (Salonia et al., 2021) for 2021 on SDs, after identifying a specific type of SD, it is recommended to discuss patient expectations carefully and consider pharmacotherapy as the primary method of treatment for patients with SDs throughout their lives. At the same time, for patients with acquired SDs, treating the underlying cause is indicated as the main goal in the initial stages.
In their study, Nimbi et al. (2021), citing organizations such as WHO and the World Association for Sexual Health, define sexual health as a human right and a key goal for improving the quality of life. It is asserted that sexual health extends beyond reproductive and sexually transmitted infection issues, encompassing positive aspects such as satisfaction from intimate relationships, diversity in sexual experiences, and aspects of sexual orientation. Cultural factors have been identified as crucial in analyzing sexual stimuli, and relationship satisfaction can be a significant predictor of sexual satisfaction, depending on gender and adherence to gender stereotypes. Several studies confirm that men with stress disorders, especially post-traumatic stress disorder (PTSD), may be more prone to developing ED compared to those without this disorder (Castillo et al., 2022; Perepeliuk, 2023). The interaction of PTSD’s stress impact on the nervous system, hormonal balance, and its effect on mental well-being can influence sexual function. Fear, anxiety, and depression often accompanying PTSD can also contribute to the development of ED.
Wittmann and Bober (2021), in their research, emphasize the importance of psychocorrection in urological practice. They point out that urological diseases and their treatment can significantly affect patients’ sexual functioning and sexual health. However, discussions about sexual health rarely occur and are limited to physiological aspects of sexual function. The authors argue that urologists are not obligated to conduct psychological therapy, but can improve the sexual well-being of their patients by providing informational resources and referring them to colleagues with additional experience in sexual health.
The results of a systematic literature analysis conducted by Atallah et al. (2021), covering 13 articles, indicate that the combination of psychotherapy and iPDE-5 is more effective in treating psychogenic ED compared to the use of these methods separately. In half of all studies described, it was found that combined interventions and psychotherapy significantly outperformed pharmacological treatment, and in one study, only individual psychotherapy. However, the authors state that no conclusions can be drawn about which type of psychocorrection is more promising, requiring further comparative research.
The study by Boddi et al. (2015) examines the effectiveness of treating ED with a combination of vardenafil and CBST compared to pharmacotherapy alone. The research confirms that ED is a multifactorial condition where both organic and psychological aspects play a crucial role. Only combined treatment demonstrated significant improvement in sexual satisfaction for both the partner and the woman, with the effect being more stable at the final stage. This is an important predictor of efficacy and requires further investigation. Dewitte et al. (2021), in their review, also highlight the importance of involving the partner in the assessment and treatment of SDs, emphasizing the significance of joint decision-making and agreement between partners regarding potential treatment options.
Over the recent years, significant progress has been made in the treatment of ED, including the development of more complex and reliable methods such as penile prostheses, injections, vacuum devices, intraurethral suppositories, and shockwave therapy (Bird et al., 2021). However, according to Althof (2023), despite this technological progress in treatment, there is an adverse psychological impact of ED on the patient, his partner, and the couple as a whole. This impact often goes unnoticed or underestimated, and existing treatment methods may merely mask the negative psychological or relational effects of ED rather than address them. As a result, a considerable number of cases (from 31% to 57%) prematurely terminate effective interventions for ED without achieving the desired outcome, and the psychological consequences of ED persist or worsen.
In the study by Han et al. (2023), the effectiveness of online cognitive-behavioral therapy (CBT) during the COVID-19 pandemic for treating psychogenic ED was assessed. The IIEF, Rosenberg’s self-esteem scale, Nine-item Patient Health Questionnaire, and Seven-item Generalized Anxiety Disorder scale were used to evaluate erectile function, self-esteem, depression, and anxiety, respectively. Interestingly, CBT showed significantly better scores on the self-esteem, anxiety, and health scales but not on the IIEF, which contradicts the findings of this study. However, the use of online methods is a promising direction that requires further investigation. Similar conclusions were drawn by Andersson et al. (2011), but their study focused on the effectiveness of online group CBT therapy, with a follow-up assessment after 6 months.
Researchers Bilal and Abbasi (2020) conducted a study among 28 men in Pakistan and showed that age influences ED symptoms and depression. However, the duration of psychotherapy did not show a significant difference in severity with the use of the IIEF and the depression, anxiety, and stress scale-21. It is important to note that the selected pharmacotherapy was 50 mg of sildenafil citrate, emphasizing the need to specify and compare with various alternative options. The study by Khan et al. (2019) involved a 15- to 18-month follow-up assessment of a subset of 20 men receiving either monotherapy with iPDE-5 or combination therapy. The results were similar to those described earlier, but after 15 to 18 months, the obtained effects were not associated with changes in relationship satisfaction or mental health indicators, emphasizing the need for dynamic and long-term monitoring.
The study by Nobre (2010) confirms that depression, dysfunctional beliefs, negative cognitive schemas, and automatic thoughts have a significant impact on male erectile function. The author points out the limited number of conceptual models attempting to integrate the interplay of these psychological factors in the context of ED. The use of different indicators, such as the IIEF, cognitive schema activation questionnaire, sexual dysfunctional beliefs’ questionnaire, and sexual analysis scale, allows for a comprehensive understanding of the factors influencing ED (Papucha, 2023).
Pieramico et al. (2023) provided evidence that psychotherapeutic interventions can effectively contribute to the mental and sexual health of men who have undergone prostate cancer. However, further research covering larger and more diverse population groups is needed. Future studies should focus on understanding the mechanisms of change through CBT interventions to ensure the mental and sexual health of men with psychogenic or organic SDs.
The article by Lafortune et al. (2023) provides predominantly sociological data, but it is worth mentioning: according to the results of an online survey of patients receiving sexual psychotherapy, over a third of those seeking professional help for SDs reported a lack of access to services, and almost 60% cited at least one barrier to receiving help. The study also emphasizes that more than half of the respondents claim a high level of psychological stress, correlating with the results of the conducted research.
The research by Seitz et al. (2020) highlights the prevalence of SDs among patients and underscores the importance of integrating sexual health issues into the treatment of psychiatric patients. With the participation of 100 psychiatrists, it was found that only a third of doctors actively address sexual health issues in their daily practice. Over 60% of doctors do not discuss these issues for various reasons, such as a lack of time or the judgment that other problems are more important. Therefore, the authors conclude that there is currently a high need for the creation of an informational network for the treatment of sexual problems, as well as the necessity to enhance the qualifications of psychiatrists in the field of sexual medicine, emphasizing the importance of collaboration among medical specialists for the effective integration of sexual health issues into practice.
Thus, the relationship between SDs and the psychological health of men is undeniable, regardless of the etiological factors of these disorders. Psychocorrection itself can serve as a quality candidate for conducting combined therapy for patients with SDs to overcome symptoms of anxiety, distress, and cognitive biases.
Conclusions
ED is a condition where a man experiences difficulties in achieving or maintaining the erection necessary for sexual intercourse. This problem may have physical, psychological, or combined causes, such as cardiovascular diseases, diabetes, stress, depression, or certain medications. The role of psychogenic ED in men’s health is significant, as it can affect the quality of life and interpersonal relationships. This condition is also an important indicator of overall men’s health and may signal the need for further medical examination, including mental health assessments.
Treatment for ED may include pharmacological methods, such as the use of iPDE-5, or non-medical approaches, such as lifestyle changes and psychotherapy. Psychotherapy plays a crucial role in the treatment of SDs, especially in cases where psychological aspects of a man’s life are identified as key factors in the development of the condition. SDs are often associated with emotional states, stress, anxiety, or depression.
Psychotherapy allows patients to identify and understand maladaptive emotional or psychological factors that may affect their sexual ability. Specialists using CBST techniques help patients manage stress, improve well-being, develop healthy sexual attitudes, and enhance communication with partners. Furthermore, psychotherapy can uncover sexual traumas or negative beliefs influencing sexual functioning and help overcome these issues. Psychotherapy can complement other methods of treating SDs, particularly in situations where psychological aspects play a leading role in the occurrence and fixation of the problem.
Prospects for future research include conducting factorial analysis of various environmental and individual factors, involving patients’ partners in studies, and extending the observation period.
Footnotes
Author Contributions
Liana Spytska contributed to conceptualization, methodology, investigation, writing—original draft, visualization, supervision, project administration, funding acquisition, and writing—reviewing and editing. The author read and approved the final version of the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval and Informed Consent
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. Informed consent was obtained from all individuals included in this study. A study was approved by Ethics Commission of the Kyiv International University, No. 84512.
Data Availability
The data that support the findings of this study are available on request from the corresponding author.