
Abstract
We evaluated depression-related health care resource utilization and antidepressant prescription medication utilization among commercially insured men in the United States who underwent inflatable penile prosthesis (IPP) implantation between January 1, 2007 and December 31, 2020, and who received a depression diagnosis in the year preceding the IPP procedure. A total of 11,177 patients received an IPP during the index period, 808 of whom were diagnosed with depression. A statistically significant reduction in overall depression-related health care visits occurred from pre- to post-IPP, decreasing from 4.9 to 3.8, p < .001. In addition, there was a significant reduction in depression-related inpatient visits (0.07 vs. 0.03, p = .02) and office visits (4.25 vs. 3.29, p < .001) from pre- to post-IPP. Of the 678 men who received an antidepressant medication within 1 year prior to their IPP date, 15% stopped antidepressant medication use entirely post-IPP. Among patients with continued antidepressant medication use post-IPP (n = 574), there was a significant decrease in the number of prescriptions (7.55 vs. 8.09, p < .0001) and refills (7.52 vs. 8.11, p = .0015), with a higher likelihood of discontinuation (17.6% vs. 10.5%, p < .0001) and a lower proportion of days covered (0.79 vs. 0.83, p = .0004) post-IPP compared with pre-IPP. In conclusion, IPP was associated with reduced depression-related health care utilization and antidepressant medication use among recipients. This suggests potential mental health benefits for IPP recipients beyond restoration of erectile function. Comprehensive insurance coverage for IPP, especially for men with depression, may be beneficial to both patients and insurers.
Introduction
Erectile dysfunction (ED) is a prevalent and often an emotionally distressing condition that affects men’s sexual health and overall well-being. Beyond the physical impairment it presents, ED can also have a profound impact on mental health and overall quality of life (DiMeo, 2006). Many men with ED suffer from other comorbidities, such as depression, diabetes, and Peyronie’s disease, amplifying the adverse consequences of ED on their daily life (Li et al., 2022). Penile implants, including inflatable penile protheses (IPP), offer a potential solution to restore erectile function and improve the overall quality of life of men suffering from ED and its comorbidities (Chung & Mulhall, 2021; Kohn et al., 2022; La Croce et al., 2022). While it is difficult to determine the true coverage rate for ED treatment (and specifically for IPP) among all men in the United States, a substantial number of men either do not have health insurance coverage for ED therapy or have coverage exclusions for treatment with IPP (Burnett et al., 2021; Kohn et al., 2022; Masterson et al., 2019; Mazur et al., 2018).
Previous research has observed improvements in depressive symptoms following treatment of ED, including treatment with IPP (Khera et al., 2018; Nackeeran et al., 2021). Limited evidence is available to quantify the association of IPP with subsequent depression-related health care utilization. This study aimed to evaluate health care utilization associated with depression among commercially insured men in the United States who received an IPP to test a hypothesis that the utilization of total health care resources, including emergency department, inpatient, outpatient, and office visits, as well as antidepressant medication use, would be reduced following IPP implantation.
Method
A retrospective claims-based analysis was conducted using the Merative MarketScan Commercial Claims Database. Men aged 18 and older who underwent IPP implantation (identified via Current Procedural Terminology [CPT] code 54405) between January 1, 2007 and December 31, 2020, and who had a diagnosis of depression (identified using the Centers for Medicare and Medicaid Services Chronic Conditions Warehouse depression codes; Services, 2020) in the year preceding the IPP implantation date, were identified. Eligible patients were required to have at least 1 year of continuous enrollment in the database both before and after the date of the IPP implantation. Patients were excluded if they received an IPP procedure during the 1-year pre-index period. For inclusion in the analysis of antidepression medication utilization, patients were required to have received an antidepressant medication prescription (including selective serotonin reuptake inhibitors, serotonin/norepinephrine reuptake inhibitors, tricyclic antidepressants, monoamine oxidase inhibitors, phenylpiperazine antidepressants, tetracyclic antidepressants, and miscellaneous antidepressants, vortioxetine, and bupropion) within 1 year prior to their IPP implantation date.
The study assessed both health care utilization and antidepressant medication utilization. Health care utilization was assessed by counting the number of emergency department visits, inpatient visits, outpatient visits, office visits, and total health care visits within 1 year pre- and 1 year post-index IPP, where total health care visits included all sites of service for depression. Antidepressant medication utilization was evaluated based on the proportion of days covered (PDC), the number of prescriptions and refills, and instances of discontinuation (defined as a gap of 90 or more days between refills) before and after IPP implantation.
Statistical analysis was performed using paired t-tests to assess the differences in both antidepressant and health care utilization before and after IPP implantation. Data analysis was conducted using Instant Health Data software (Panalgo, Boston, MA, USA) and R, version 3.2.1 (R Foundation for Statistical Computing, Vienna, Austria).
Results
Health Care Utilization
Among the 11,177 total patients who received an IPP during the index period, 808 patients had a diagnosis for depression. The average age was 55.3 years (±6.8) and the average Charlson comorbidity index (CCI) score was 1.6 (±0.9) (Table 1). Compared with the pre-IPP period, patients experienced a reduction in the mean number of total depression-related health care visits (4.9 pre-IPP vs. 3.8 post-IPP, p < .0001), inpatient visits (0.07 vs. 0.03, p = .02), and office visits (4.25 vs. 3.29, p < .0001) post-IPP (Table 2).
Patient Characteristics
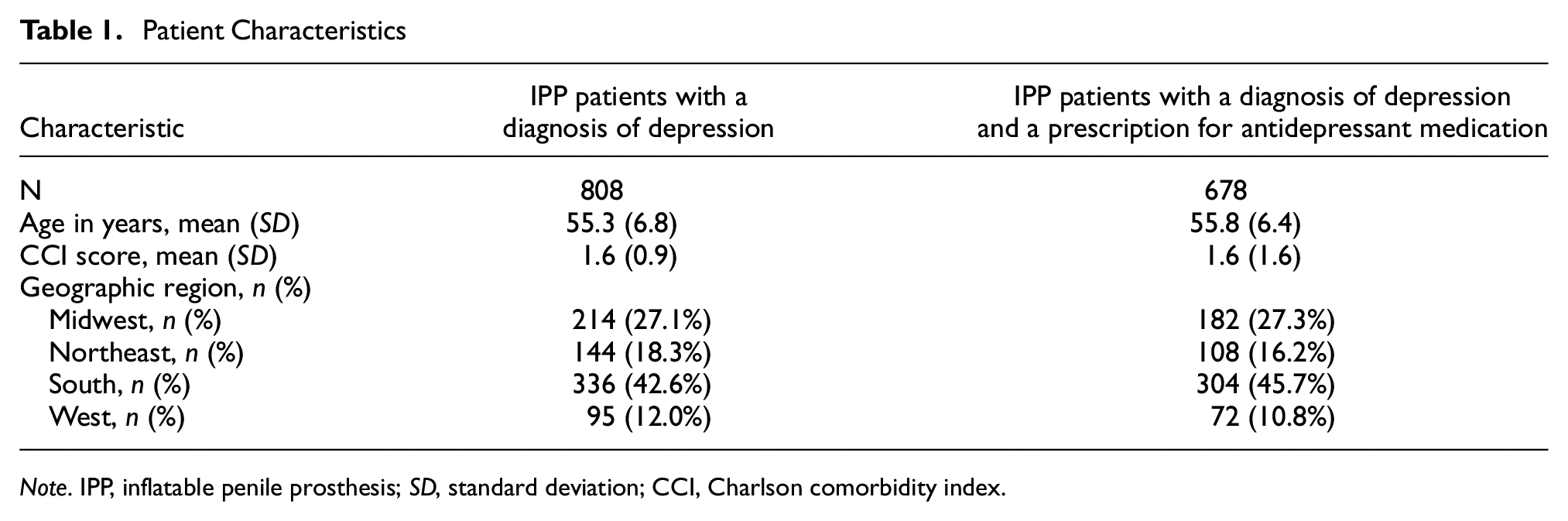
Note. IPP, inflatable penile prosthesis; SD, standard deviation; CCI, Charlson comorbidity index.
Comparison of Health Care Utilization Associated With a Primary Diagnosis of Depression Pre- and Post-IPP
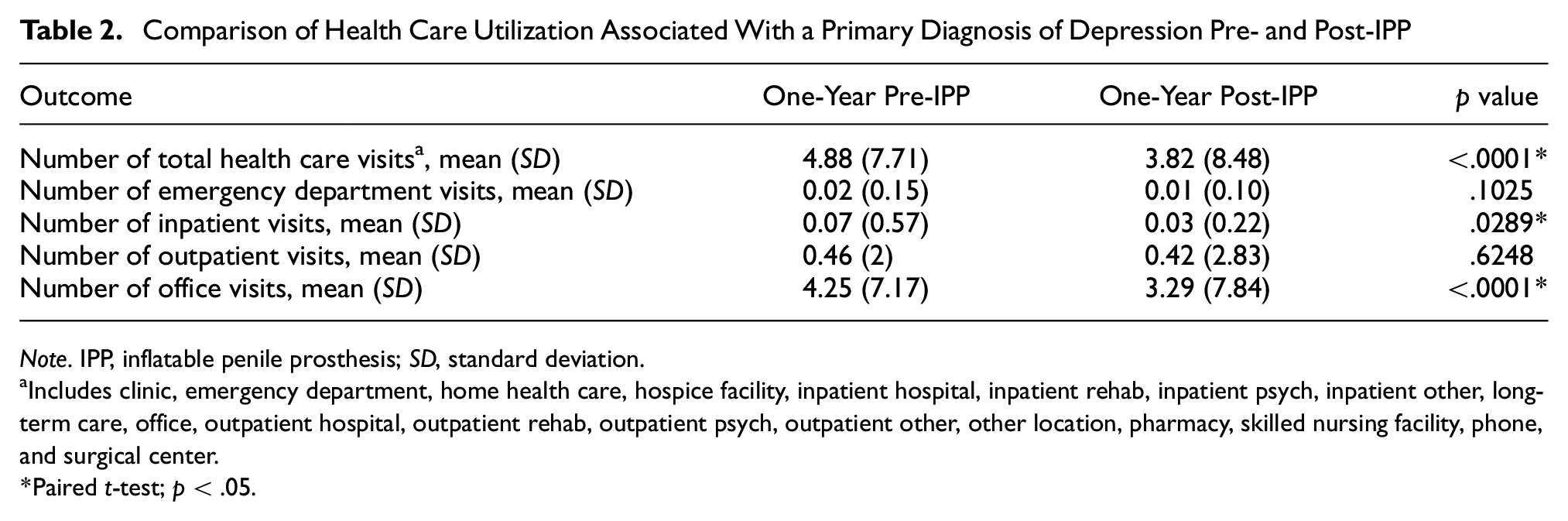
Note. IPP, inflatable penile prosthesis; SD, standard deviation.
Includes clinic, emergency department, home health care, hospice facility, inpatient hospital, inpatient rehab, inpatient psych, inpatient other, long-term care, office, outpatient hospital, outpatient rehab, outpatient psych, outpatient other, other location, pharmacy, skilled nursing facility, phone, and surgical center.
Paired t-test; p < .05.
Antidepressant Medication Utilization
A total of 678 men diagnosed with depression who underwent IPP and who had an antidepressant medication prescription during the 1-year pre-IPP period were identified. The average age was 55.8 (±6.4) and the mean CCI score was 1.6 (±1.6) pre-IPP (Table 1). Of these patients, 104 (15%) had no antidepressant prescriptions in the post-IPP follow-up period, representing a complete stop of antidepressant medication treatment. The remaining 574 men who did not completely stop their antidepressant medication usage post-IPP (Table 3) received significantly fewer antidepressant prescriptions (7.55 vs. 8.09, p < .0001) and refills (7.52 vs. 8.11, p = .0015) in the 1-year post-IPP period. These patients were also significantly more likely to discontinue their antidepressant medications, defined as a gap of 90 or more days between refills (17.63% vs. 10.45% of patients; p < .0001) and had a lower mean PDC (0.79 vs. 0.83, p = .0004) post-IPP versus pre-IPP (Table 3).
Utilization Among Patients With an Antidepressant Prescription Post-IPP (n = 574)
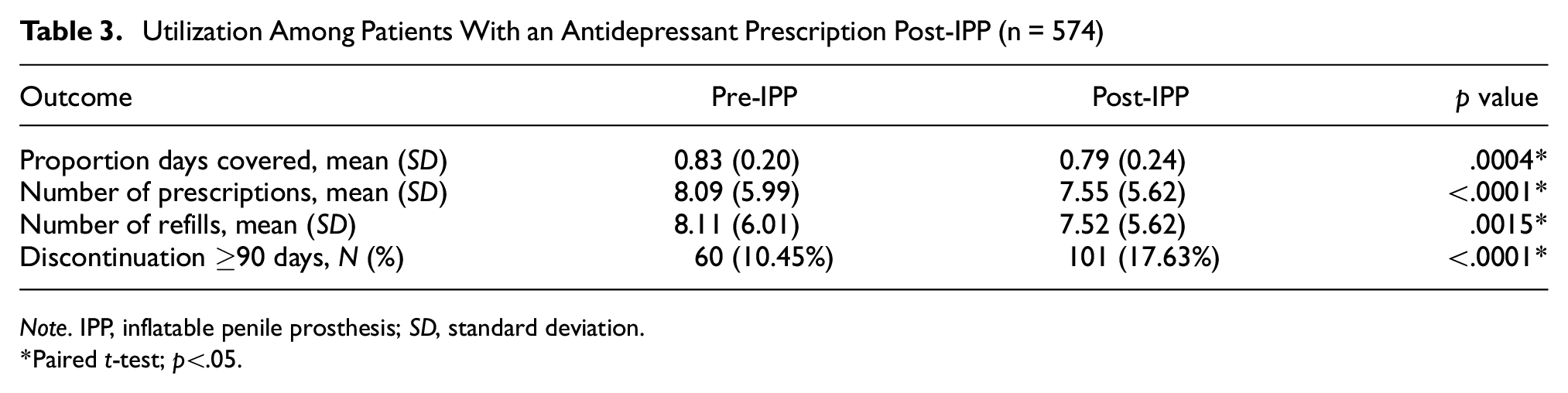
Note. IPP, inflatable penile prosthesis; SD, standard deviation.
Paired t-test; p<.05.
Discussion
The association between ED and depression has been extensively studied (Calzo et al., 2021; Manalo et al., 2022; Ozkent et al., 2021). Depression can be both a precursor and a consequence of ED, creating a cycle that affects both the mental and physical health of the patient. IPP placement can restore sexual function, enhance self-esteem, and improve the overall quality of life for these individuals (Barton et al., 2018). By providing a solution for men with chronic, organic ED, IPPs can also foster emotional well-being and intimacy within relationships and reduce the psychological stress and strain ED can place on both partners. This study explored a fundamental area where research appears to be limited: the association of IPP placement with subsequent depression-related health care utilization and antidepressant medication use. It is important to clarify this study’s intention is not to assert that seeking health care for depression is problematic. Instead, the study posits that health care utilization can be a proxy for the overall burden a person’s depression may impose, and observed reductions reflect a decreased burden.
The study’s findings demonstrate IPP implantation was associated with decreased antidepressant medication usage and fewer overall health care visits, including inpatient visits and office visits. There may be several potential explanations for these findings. First, restoration of erectile function, through interventions such as IPP implantation, may improve sexual function and quality of life while decreasing depressive symptoms (Khera et al., 2018; Nackeeran et al., 2021; Pillay et al., 2017). Consequently, this could reduce the frequency of mental health–related consultations within this population, as suggested in previously published studies (La Croce et al., 2022; Li et al., 2022). Second, the comorbidity burden among men with ED is well-documented (García-Cruz et al., 2018; Hackett, 2009). Therefore, addressing ED may thereby confer beneficial effects on several of the commonly associated conditions. Finally, previous research has demonstrated a relationship between ED and loss of productivity and increased absenteeism (Rojanasarot et al., 2022). Successfully treating ED with an IPP, as this study reflects, may therefore improve work-related aspects, thereby improving individuals’ overall mental health and well-being.
The results of this study are consistent with findings in the existing literature. Nackeeran et al. (2021) elucidated that men who underwent medical or surgical treatments for ED, namely penile prosthesis implantation or phosphodiesterase type 5 inhibitor medication use, were less likely to develop major depressive disorder within the subsequent 3 years. Similarly, Khera et al. (2018) reported that among patients grappling with ED and concurrent Peyronie’s disease, there was a marked improvement in their depression scores post-IPP implantation. Nonetheless, a more cautious perspective was offered by Pillay et al. (2017). Despite discerning certain significant associations between penile prosthesis use and depression symptom reduction, the authors hypothesized this linkage might be tenuous and, perhaps, ephemeral (Pillay et al., 2017). Additional investigation is warranted given the prevalence of ED and the significant burden of depression to individuals and society.
In addition to alleviating depressive symptoms, IPP and other ED treatments have demonstrated potential in mitigating the possible economic burden and improving the quality of life of those affected. Beyond the physical and emotional toll it exacts, ED profoundly influences quality of life, intimate relationships, and workplace productivity (Elterman et al., 2021; Goldstein et al., 2019). From an economic perspective, Rojanasarot et al. (2022) identified an overwhelming annual incremental cost of $7,270 due to the additional 282.7 work hours of impairment in U.S. privately insured men with ED compared with those without ED. Furthermore, the potential exclusion of penile prosthesis implantation benefits from employer-sponsored health plans in the United States could result in a staggering $9.3 billion in lost productivity due to ED (Rojanasarot et al., 2022). In addition, a previously published study identified that depression had one of the highest annual burdens of lost work productivity compared with other priority conditions, including cardiometabolic or chronic lung diseases (Rojanasarot et al., 2023). Given this study addressed patients with depression and ED conditions, the implications of the results could be used to communicate the values of IPP to health care stakeholders.
This study offers real-world insights into the benefits of IPP through analysis of a large commercial claims database. The Merative MarketScan Commercial Claims Database consists of medical and drug data for several million individuals covered by employer-sponsored private health insurance in the United States annually, encompassing employees, their spouses, and dependents (Merative, 2023). In addition, the total health care visits analyzed included all sites of service for depression.
This study is subject to certain limitations inherent to all retrospective claims data analyses. The validity of medical claims data depends on coding accuracy and may lack information from health encounters, including disease severity and patient-reported depression outcomes. Etiology of a patient’s ED cannot be discerned from claims. Changes in patterns of depression-related claims do not necessarily imply a change in the number or severity of depressive symptoms. Encounters with providers not covered by commercial insurance will not appear in these claims. In addition, prescriptions filled and paid for by means other than commercial health insurance, such as cash/self-pay, are not accounted for in claims data. Estimates of antidepressant medication utilization are sensitive to the proportion of patients not using their commercial insurance to fill their prescriptions. Claims data also do not allow one to determine why someone stopped filling their prescription; therefore, we cannot infer that all patients who stopped taking antidepressant medication did so because they experienced a reduction in depressive symptoms. It is not possible to distinguish between patients who take their medications as prescribed and those who fill their prescription medications but do not carry through with taking them. Finally, this study involved patients with commercial insurance; thus, the results may not be generalizable to those with public insurance (Medicare, Medicaid) or those who lack insurance.
This study reported a significant reduction in depression-related health care visits and antidepressant medication utilization post-IPP implantation, emphasizing IPP’s potential role in not only restoring erectile function, but also impacting mental health outcomes. Further research may evaluate the causative factors and implications of these findings on patient care and treatment approaches. To maximize patient benefits, comprehensive coverage of medically necessary IPP among commercially insured patients is crucial, along with broader systemic changes, patient education on ED and its association with depression, consistent follow-up care, and societal acceptance for the treatment of both ED and depression.
Footnotes
Acknowledgements
The authors would like to thank Craig Solid for assistance in preparing this manuscript and Rutugandha Paranjpe for assistance in the early analysis of the study.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: A.M.M. and S.R. are full-time employees of, and shareholders in, Boston Scientific. Y.E.S. is a graduate student who is working on a Global Health Economics and Market Access project with Boston Scientific. R.R. is a consultant for and grant recipient of Boston Scientific. T.K., R.G., S.N., and F.P. have no relevant disclosures to report.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by Boston Scientific.
Ethical Approval and Informed Consent Statements
Because this study involved a retrospective analysis of billing claims of de-identified beneficiaries, no informed consent or review board approval was required.
Data Availability Statement
The data that support the findings of this study are available from the Merative MarketScan Commercial Claims Database but restrictions apply to the availability of these data, which were used under license for the current study, and so are not publicly available. Data are, however, available from the authors upon reasonable request and with permission of Merative.