
Abstract
Microsurgical subinguinal varicocelectomy (MSV) is the gold standard for treating varicoceles. Preservation of the internal spermatic arteries (ISAs) during MSV is important for sperm production. This study aimed to evaluate the safety and efficacy of elevating systolic blood pressure (SBP) using MSV. Data from 252 consecutive adult male patients were retrospectively reviewed. The patients were divided into two groups: a traditional group that underwent conventional MSV (n = 134) and a modified group that underwent MSV with a transiently elevated SBP of 140–160 mm Hg (n = 118). Arterial identification time, unilateral operative time, number of ISAs, arterial injury rate, and other postoperative indicators, including postoperative complications and sperm parameters, were compared between the groups. All the procedures were successful. The arterial identification and unilateral operative times were significantly shorter in the modified group (31.34 ± 10.44 vs. 42.94 ± 12.39 min and 61.48 ± 8.78 vs. 76.35 ± 12.33 min, p < .01, respectively). Intraoperatively, the number of preserved ISAs was significantly higher in the modified group (1.92 ± 0.53 vs. 1.45 ± 0.32, p < .01). The arterial injury rate did not differ significantly between the groups (2.74% vs. 0%, respectively). Compared with preoperative values, sperm parameters improved significantly 6 months postoperatively. Significant differences in semen parameters or postoperative complications were not observed between the groups. Elevated intraoperative SBP can be used to rapidly, safely, and effectively identify ISAs, increase the number of retained spermatic arteries, and markedly reduce the operative time for MSV.
Introduction
Varicocele is the most common surgically correctable cause of male infertility (Kilciler et al., 2011). Potential mediators of varicocele pathogenesis include scrotal hyperthermia, backflow of toxic metabolites, testicular hypoperfusion, hypoxia, and hormonal disturbances (Cardoso & Cocuzza, 2019). This condition is commonly associated with the production of low-quality semen, testicular pain, and atrophy. Varicocele treatment aims to prevent retrograde flow into the internal sperm vein (ISV; Lomboy & Coward, 2016). The ideal technique aims to ligate all internal and external spermatic veins while preserving the spermatic arteries and lymphatics (Cayan et al., 2008). Several methods have been used for this purpose, including open surgical ligation of the spermatic vein, laparoscopic varicocelectomy, and microsurgical varicocelectomy. Microsurgical subinguinal varicocelectomy (MSV) is considered the gold standard treatment (Baazeem et al., 2011; Owen et al., 2017; Silveri et al., 2003), but its primary disadvantage is a longer operative time (Al-Kandari et al., 2007), a factor that correlates significantly with challenges in separating the internal spermatic artery (ISA) from the ISV (Park et al., 2011). Although dissection and conservation of the ISA is time-consuming, it is vital in MSV. Papaverine irrigation and micro-Doppler are the most widely adopted techniques for arterial identification and preservation of MSV (Cho et al., 2019). Such methods are sometimes effective but does not always work. Identifying and preserving the ISA rapidly and accurately is the greatest challenge when shortening the operative time.
At our institute, we attempted to visualize arterial pulsations during MSV. In this retrospective, controlled study, we aimed to evaluate the effectiveness of elevating systolic blood pressure (SBP) for rapid and safe intraoperative identification of ISAs during MSV and to compare its clinical utility with that of traditional MSV using papaverine solution.
Materials and Methods
This study involved consecutive patients treated at a single institution. In total, 252 adult men aged ≥18 years (mean age, 27.92 ± 6.82 years) who underwent 279 MSVs at the Zhejiang Provincial People’s Hospital between January 2018 and December 2021 were enrolled. In this cohort, 32 of the patients had offspring. None of the patients had prior exposure to harmful radiation, chemicals, urinary genital tract infections, or physical trauma that could have impaired their reproductive function. Patients who had received chemotherapy, radiotherapy, steroids, antiviral treatments, or other medications known to affect fertility were excluded. Comprehensive semen analyses were performed for all patients 1 week before and 6 months after the surgery. Each patient underwent chromosomal assessments, reproductive hormone evaluations, and ultrasound examinations of the male reproductive organs. Patients with karyotype anomalies, Y chromosome microdeletions, leukocytospermia, or a history of parotitis or cryptorchidism were excluded. The procedures were performed over two different time periods by the same surgical team specialized in MSV. The first 134 (53.2%) patients who underwent 146 classical MSV procedures were classified into a traditional group, and the 118 (46.8%) remaining patients who underwent 133 MSVs with the addition of elevated SBP during surgery were classified into a modified group. All patients signed an informed written consent agreement. This study was approved by the hospital’s Medical Ethics Committee (QT2022351). The guidelines of the Declaration of Helsinki were followed. The same chief surgeon (KB.Y) who had performed >300 varicocelectomies prior to the study commencement had performed both types of operations on all patients. The inclusion criteria comprised the following: (a) patients with a diagnosis of varicocele according to American Society of Reproductive Medicine and American Urological Society diagnostic criteria, with Clinical Grades 1–3 as described by Dubin and Amelar (Shridharani et al., 2016); (b) patients with a scrotal Doppler ultrasound indicating an ISV diameter of ≥2 mm and venous reflux with or without the Valsalva maneuver; (c) patients with a normal preoperative electrocardiograph, pulse, and blood pressure; and (d) patients with a tolerable norepinephrine (NE)-induced blood pressure elevation, as evaluated by anesthesiologists. Exclusion criteria comprised the presence of subclinical and secondary varicoceles or complications and patients with severe heart, brain, liver, kidney, or other organ diseases.
Semen analyses were performed 1 week before and 6 months after the surgery. The collection and evaluation of semen samples were conducted within an andrology laboratory, where an experienced technician, in strict compliance with the World Health Organization’s laboratory manual guidelines, conducted assessments. Following 2−7 days of sexual abstinence, the patients provided samples via masturbation in sterile containers. At 30 min after liquefaction, the semen volume was measured in a laminar flow room. Sperm concentration and motility were assessed using a computer-assisted sperm analysis system. All procedures were performed under general anesthesia, and the same surgical team did not use intraoperative Doppler ultrasonography in either group.
In the traditional group, MSV was performed using conventional techniques. Intraoperative blood pressure management strategy involves targeting an SBP within 10% of the patient’s baseline resting value (Futier et al., 2017), with a maximum upper limit of 140 mm Hg. In accordance with Goldstein et al.’s (1992) approach, a 2- to 4-cm incision was made below the external inguinal ring, Camper’s and Scarpa’s fasciae were incised, the spermatic cord was grasped with an Ellis clamp, the testis was delivered into the incision, and the external spermatic and gubernacular veins were ligated using 4-0 silk ties. The testis was then returned to the scrotum, and the spermatic cord was placed over a Penrose drain. Dissection was performed using a Zeiss OPMI Vario/S88 surgical microscope at 6−18× magnification. The cremasteric fibers were then divided into 2 groups. The vasal compartment, including the vasal and associated vasculature, in addition to the lymphatic system, was separated and preserved with a second Penrose drain after opening the internal spermatic fascia. The arteries were first identified and subsequently separated via subtle pulsation. Upon identification, an ISA was encircled with a blue loop. The compartment was irrigated multiple times with a 1% papaverine solution to identify the arteries when pulsation was faint. All the identified lymphatics were preserved. The ISVs were ligated after all arteries and lymphatics were identified and preserved. The cremaster muscle was closed using a 5-0 monofilament absorbable suture, and the spermatic cord was repositioned. Finally, the fascia and skin of the scarpa were closed using a 5-0 absorbable monofilament suture.
In the modified group, some modifications were made as described below. Dilutions of 2 mg of norepinephrine (NE) in a 5% dextrose solution were prepared in 50-mL syringes. The NE injection was initiated when the rest of the spermatic cord was separated from the vasal structures. The NE infusion rate was limited to 0.03–0.15 μg·kg−1·min−1. The patient’s SBP gradually increased and remained within 140–160 mm Hg for approximately 10–15 min. Once the ISA was identified on the basis of its pulsatile appearance under an operating microscope, a blue loop was placed around it. NE infusion was stopped to return the SBP to normal when all ISAs were confirmed and preserved. The subsequent procedure was the same as that described above.
Evaluations
In this study, arterial identification time was defined as the time from opening the internal spermatic fascia to exposing the ISA under a microscope. Unilateral operative time was measured from the initial incision to skin closure. All the identified ISAs separated from the surrounding veins and lymphatics were preserved and counted. The rate of arterial injury, including arterial wall injury and accidental arterial ligation, was also recorded. Semen parameters were analyzed 1 week before and 6 months after the surgery. Complications up to 6 months after the surgery, including clinical hydrocele, testicular atrophy, and varicocele recurrence, were compared between the two groups. Varicocele recurrence was diagnosed on physical examination and scrotal Doppler ultrasonography (postoperative ISV diameter, ≥2 mm). All adverse reactions that developed during hospitalization were recorded.
Statistical Analysis
Statistical analyses were performed using SPSS software (IBM, SPSS statistics version 26). Power calculation was performed using JMP Trial 17 (JMP Statistical Discovery LLC). Data are presented as mean ± standard deviation. Independent and paired-sample t-tests were used for intergroup and intragroup comparisons, respectively. Count data are presented as n (%), and between-group comparisons were performed using a χ2 test. Statistical significance was set at p < .05.
Results
Comparison of Baseline Characteristics
The preoperative patient characteristics of the two groups are presented in Table 1. The traditional group comprised 134 patients with varicoceles, of whom 122 (91.04%) had unilateral varicocele and 12 (8.96%) had bilateral varicoceles. The modified group included 118 patients with varicocele, including 103 (87.29%) with unilateral and 15 (7.7%) with bilateral varicoceles. No significant differences in age, blood pressure, position, clinical grade, or ISV diameter were observed between the two patient groups.
Comparison of Preoperative Patient Characteristics in the Two Groups
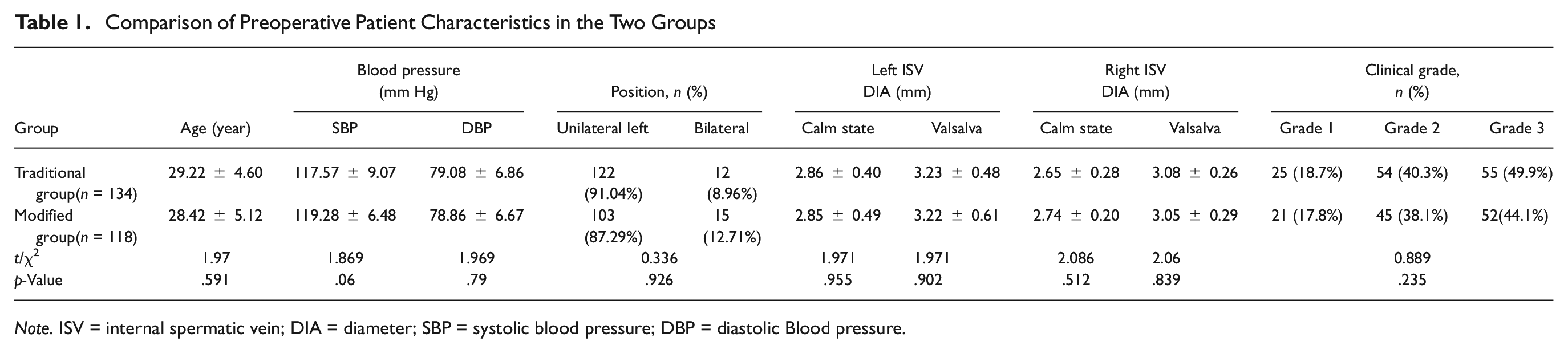
Note. ISV = internal spermatic vein; DIA = diameter; SBP = systolic blood pressure; DBP = diastolic Blood pressure.
Comparison of the Intraoperative and Postoperative Results
A summary of the intraoperative and postoperative results for both patient groups is presented in Table 2. In total, 134 patients in the traditional group underwent 146 MSVs, whereas 118 patients in the modified group underwent 133 MSVs following the same method with the addition of intraoperative SBP elevation. In the modified group, the ISAs of all patients demonstrated visible pulsations with an elevated SBP of 140–160 mm Hg (Figure 1). The arterial identification time and unilateral operative time were significantly shorter in the modified group than that in the traditional group (31.34 ± 10.44 vs. 42.94 ± 12.39 min and 61.48 ± 8.78 vs. 76.35 ± 12.33 min, p < .01, respectively). Intraoperatively, the number of preserved ISAs was significantly higher in the modified group than that in the traditional group (1.92 ± 0.53 vs. 1.45 ± 0.32, p < .01). Power analysis was performed on the mean arterial identification time, unilateral operative time, and number of ISAs across the two groups. The analysis revealed that the statistical power, considering the current sample size, significantly surpassed the 80% threshold, indicating robustness in detecting true effects. Four (2.74%) patients in the traditional group had arterial injuries identified using microscopy, including one arterial wall injury and three accidental arterial ligations; no repair was required. The arterial injury rate did not differ significantly between the two groups (χ2 = 3.697; p > .05). One (0.85%) patient in the modified group presented with a transient headache on Postoperative Day 1. Similar adverse effects were not observed in the traditional treatment group, and adverse reactions did not differ significantly between the two groups. Six months after the surgery, significant differences in complications, including clinical hydrocele, testicular atrophy, or varicocele recurrence, were not observed between the two groups.
Comparison of the Intraoperative and Postoperative Results in the Two Groups

Note. ISA = internal spermatic arteries
The number of ISAs and the arterial injury rate for each side were analyzed in one patient with bilateral varicocele.

Intraoperative Images of the ISA During Microsurgical Subinguinal Varicocelectomy. (A) ISA view before the elevation of the SBP; (B) ISA vasodilatation and pulsatility demonstrated clearly after the elevation of the SBP within 140–160 mm Hg
Comparison of Preoperative and Postoperative Semen Parameters
The semen parameters were compared between the two groups 1 week before and 6 months after surgery. Tables 3 and 4 present the primary data. Six months after surgery, the total sperm count, sperm concentration, and forward-moving sperm rate were significantly higher than those at 1 week prior to surgery. The semen parameters did not differ significantly between the two groups.
Comparison of the Preoperative and Postoperative Semen Parameters in the Two Groups

Number of Patients With Different Types of Sperm Abnormalities in the Two Groups

Discussion
The American Urological Association recommends that varicocelectomy be performed under optical magnification to maximize ISA preservation (Sharlip et al., 2002). In this study, we adopted a modified visualize technique involving SBP elevation during MSV and assessed its clinical usefulness. In a prior study, Jarow et al. (1992) reported a mean of 2 arteries during varicocelectomy and of 2.4 arteries in adult spermatic cords after autopsy. Using intraoperative Doppler ultrasonography, Guo et al. (2015) and Lv et al. (2017) reported the numbers of preserved ISAs to be 1.9 and 1.96, respectively. In our study, the average number of ISAs in the traditional group treated with papaverine solution was 1.45, which was similar to the results of previous studies (Mirilas & Mentessidou, 2011; Wang et al., 2012; Zhang et al., 2014; average number, 1.4–1.6). Conversely, in the modified group, the average number of ISAs preserved intraoperatively was 1.92, which was significantly higher than that in the traditional group (χ2 = 8.643; p < .05). This intergroup difference can be explained by two factors. First, the density of the veins surrounding the artery in the subinguinal spermatic cord may have influenced the effect of the papaverine solution. Second, arterial spasm of the dissected vessels may have rendered identification of arterial pulsation difficult, while elevation of SBP enabled a more precise determination of vascular structures and helped distinguish between the veins and arteries. Our study results suggest that more ISAs were identified and preserved to visualize technological improvements in MSV.
A meta-analysis on surgical procedure reported that the operative time was longer in an MSV group than that in laparoscopic and open surgery groups (Yuan et al., 2017). According to Park et al. (2011), a longer operative time is generally associated with more components of the venous system in the spermatic cord. Kirac et al. (2013) reported that differences in the operative time depend on the surgeon’s capability. Lee et al. (2016) considered that the ISA type and the difficulty in separating ISA from ISVs affected the operative time. Özkaptan et al. (2020) reported that the use of equipment such as an intraoperative Doppler could shorten the operative time. Our study indicated that the average arterial identification and operative times were 31 and 61 min, respectively, in patients undergoing MSV with elevated intraoperative SBP. The operative time in the modified group was significantly reduced by an average of 15 min compared with that in the traditional group (t = 10.890; p < .05).
Chan et al. (2005) and Cocuzza et al. (2010) identified three reasons as to why ISAs are not easily discernible. First, detection of pulsations is challenging in small arteries. Second, aggressive dissection can cause vasospasms, thereby preventing arterial pulse identification. Third, complex branches of veins surround or obscure the arteries. In this study, the arterial injury rate in the traditional group was 2.74%, which was higher than that reported by Chan et al. (2005) and Cocuzza et al. (2010) (average arterial injury rate: 1%–1.1%). No arterial injury was observed in the modified group. Our results indicated that SBP was elevated and maintained within 140–160 mm Hg, and that the arterial injury rate in the modified group was lower than that in the traditional group, although the p-value was not significant. Elevating intraoperative SBP with intravenous infusion of NE may contribute to the precise identification of ISAs during dissection of the spermatic cord. Small arteries located within the complexes of adjacent veins prevent accidental ligation as well.
NE is the first-line treatment for maintaining end-organ perfusion pressure, particularly in critically ill patients with low systemic vascular resistance (Chen et al., 2020), as it can effectively elevate arterial blood pressure through exerting pharmacological effects on α1 adrenoceptors (Zhou et al., 2022). Davis (1992) reported that when blood pressure was increased to 140 mm Hg, NE did not significantly affect the lumen cross-sectional area and cause any vasoconstriction. Davis suggested that a hypertensive blood pressure of ≥140 mm Hg may cause progressive vasodilation and accelerate the blood flow. During the procedures in this study, we further confirmed that vasodilation and pulsation of the arteries remained evident with an elevated SBP of ≥140 mm Hg. NE exerts weak β-adrenergic receptor agonist activity and may be more suitable for maintaining blood pressure, with fewer negative effects on heart rate and cardiac output (Elnabtity & Selim, 2018). To adjust for safety, we controlled the SBP within 140–160 mm Hg for approximately 10–15 min at a low dose (0.03–0.15 μg·kg−1·min−1). In the modified group, one (0.85%) patient presented with a transient headache, but no serious adverse effects, such as arrhythmia, extreme hypertension, nausea, or omission, were otherwise observed. The adverse reactions did not differ significantly between the two groups.
Similar to Guo et al.’s (2015) findings, improvements in semen parameters were observed 6–12 months after surgery. Our study demonstrated that the sperm count (t = 10.731, p < .001 in traditional group; t = 5.945, p < .001 in modified group), sperm concentration (t = 10.051, p < .001 in traditional group; t = 6.551, p < .001 in modified group), and sperm forward-moving rate (t = 22.173, p < .001 in traditional group; t = 17.151, p < .001 in modified group) were significantly increased after MSV, which accords with the results of previous studies (Baazeem et al., 2011; Cayan et al., 2008; Schauer et al., 2012). Significant differences in postoperative semen parameters were not observed between the two groups, including the sperm count (t = 0.262; p > .05), sperm concentration (t = 1.305; p > .05), and sperm forward-moving rate (t = 1.701; p > .05). These results indicated that the elevated SBP in the MSV group did not affect the degree of improvement in semen parameters between the two groups 6 months after surgery. In terms of complications, three varicocele recurrences were recorded in the traditional group, with an incidence of 2.24%, with no significant differences between the two groups (χ2 = 2.654; p > .05). Other complications such as clinical hydrocele or testicular atrophy were not observed in either group. These results indicated that elevated intraoperative SBP did not influence postoperative data in either group.
Strengths and Limitations
The strength of this study was that ISAs with constant pulsatile distension and contraction were easily identified during MSV when the SBP was maintained at 140–160 mm Hg. Few specific cohort studies have investigated SBP elevation during MSV. This visualize technique is inexpensive and convenient and results in fewer adverse reactions. In particular, this technology can be beneficial for medical units that do not equip intraoperative Doppler imaging.
This study had some limitations. This was a non-randomized retrospective study. While the same team of surgeons was involved, their proficiencies varied at different stages of observation, and a subjective bias cannot be avoided. Intraoperative ultrasound was not employed in the traditional group. The extent of SBP change and intraoperative effects did not show any dose-effect relationship. The sample size was small, and only a 6-month follow-up period was covered. Further studies with larger sample sizes, utilization of intraoperative ultrasound, and longer follow-up periods are required to confirm our findings.
Conclusion
Overall, elevating the intraoperative SBP to 140–160 mm Hg can lead to the rapid, safe, and effective identification of ISAs, increase the number of retained ISAs, and significantly reduce the operative time. Moreover, the modified technique did not adversely influence the postoperative sperm parameters or varicocele recurrence rates. We strongly recommend that this method be applied during microsurgery in patients with varicoceles.
Supplemental Material
sj-pdf-1-jmh-10.1177_15579883241265071 – Supplemental material for Effects of Systolic Blood Pressure Elevation on Internal Sperm Artery Identification During Microsurgical Subinguinal Varicocelectomy
Supplemental material, sj-pdf-1-jmh-10.1177_15579883241265071 for Effects of Systolic Blood Pressure Elevation on Internal Sperm Artery Identification During Microsurgical Subinguinal Varicocelectomy by Yang Kebing, Wang Chenglu, Xu Xiaobo, Aikeremu Tiliwalidi and Zhang Liao in American Journal of Men's Health
Footnotes
Acknowledgements
We would like to thank Professor Xu Zhihui for guidance for the scientific research. We thank Dr. Lu Wanpeng for his assistance with the statistical analysis of the data.
Authors’ Contributions
Yang Kebing conceived of the study and drafted the manuscript. Wang Chenglu and Xu Xiaobo participated in the procedure. Xu Xiaobo carried out data curation. Wang Chenglu performed the statistical analysis. Aikeremu Tiliwalidi and Zhang Liao participated in its design and coordination. All authors read and approved the final manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Statement
The research meets ethical guidelines, and approval was provided by the institutional review board.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.