
Abstract
About 1 in 10 men experiences sexual assault, resulting in various difficulties most frequently associated with post-traumatic stress disorder. However, trauma-focused cognitive behavioral therapies (TF-CBT) seem less effective for men who experienced sexual assault compared to women. Efficacy of TF-CBT could be improved by adapting interventions according to the empirical data detailing men’s preferences regarding psychological services. This scoping review aimed to document preferences of men who experienced sexual assault regarding psychological services, and to explore barriers and motivators to help-seeking for this population. A systematic approach was used to gather literature describing preferences regarding psychological services, and barriers and motivators to help-seeking. Thirty-five peer-reviewed studies and two non-peer reviewed reports met inclusion criteria. Data from included articles were extracted using a systematic extraction grid. A thematic content analysis was conducted to synthesize and present the results from the 37 studies. The number of empirical studies on preferences regarding psychological services was limited as only five documented preferences, all related to the clinician’s characteristics (e.g., clinician’s gender) and the type of intervention (e.g., action-oriented). Most studies reviewed barriers to help-seeking. The barriers most frequently identified were adherence to masculine norms and to myths about male sexual assault. Injury or substance abuse following sexual assault often act as motivators to help-seeking for men. To adapt TF-CBT to men who experienced sexual assault, researchers and clinicians should accommodate and further study these men’s preferences, consider their motivators regarding help-seeking and alleviate barriers to help-seeking, notably by deconstructing masculine norms.
Sexual assault, defined as a sexual conduct perpetrated without consent, such as an unwanted sexual intercourse, sexual touching, or kissing, is a public health issue affecting the health and well-being of millions of people worldwide (S. Khan et al., 2020). Although women report having experienced sexual assault more often than men, a growing body of literature provides evidence on the prevalence and consequences of having experienced sexual assault among men (for a review, see Peterson et al., 2011). In North America, about 1 in 10 men will experience sexual assault in their lifetime (Tourigny et al., 2008) and face physical and psychological consequences, such as the development of anxiety, depression or, more frequently, post-traumatic stress disorder (PTSD; Heidt et al., 2005; Morris et al., 2014; Tewksbury, 2007).
Although studies have identified that male victims of sexual assault experience PTSD symptoms as severe as female victims (Elliott et al., 2004; Guina et al., 2019), there is also evidence of consequences to sexual assault that are more common among men than women. Notably, in a national study comparing the symptomatology of both genders who had experienced sexual assault, Elliott and colleagues (2004) reported that men had higher levels of sexual concerns and dysfunctional sexual behaviors than women and engaged more often in self-destructive or health-damaging behaviors (e.g., unsafe sexuality, smoking, substance abuse).
Psychological interventions have proven effective in reducing PTSD symptoms and psychological distress for victims of sexual assault, regardless of gender. According to expert consensus guidelines, trauma-focused cognitive behavioral therapies (TF-CBT) represent the gold standard for the treatment of PTSD (e.g., Bisson et al., 2013; Forman-Hoffman et al., 2018). More specifically, prolonged exposure therapy (PE), which consists of exposing a patient to reminders of the traumatic event to promote the emotional and cognitive processing of the trauma, has demonstrated effectiveness in reducing PTSD symptoms and improving the quality of life of sexual assault victims (Cusack et al., 2016; Ehring et al., 2014). Cognitive processing therapy (CPT), which targets trauma-related dysfunctional beliefs, has also been validated among victims of sexual assault. Effectiveness studies have reported significant reduction in PTSD and depression symptoms for both genders (Chard, 2005; Resick & Schnicke, 1992; Schnurr et al., 2022; see Schnyder and Cloitre [2022] for further details on TF-CBT). Eye Movement Desensitization Reprocessing (EMDR), which involves desensitizing an individual to trauma using a series of eye movements, is another TF-CBT that appears effective in reducing PTSD symptoms, but its efficacy in early interventions for PTSD has yet to be fully established (Covers et al., 2021).
Studies have demonstrated that only a small proportion of men seek psychological help (AL-Asadi, 2021; Gallegos et al., 2015; Masho & Alvanzo, 2010). As of 2021 in Canada, for every seven women who sought psychological services, only one man did likewise (AL-Asadi, 2021). For men who do seek help, TF-CBT appears to be effective, but to a lesser extent than for women. Felmingham and Bryant’s (2012) randomized controlled trial reported a similar significant reduction in PTSD symptoms between male and female victims of sexual assault immediately after attending PE or CPT combined with PE. However, reduced maintenance of treatment gains was observed at 6-month follow-up for men who completed PE only compared to women. Another study investigated the impact of gender on response to PE and CPT (A. J. Khan et al., 2020). Following CPT, women demonstrated a significantly greater reduction in PTSD symptom severity than men, whereas no gender difference in treatment response was observed after PE. In addition, Békés and colleagues (2016) have reported greater secondary gains (e.g., quality of life, support-seeking, supportive interactions) in women attending a TF-CBT for PTSD compared to men. However, no statistically significant gender difference was observed on PTSD symptoms.
A way to improve the efficacy of TF-CBT for male victims of sexual assault could be to adapt interventions according to their preferences. Indeed, a meta-analysis including 53 studies and more than 16,000 clients reported that preference accommodation is related to better treatment outcomes (Swift et al., 2018). To achieve adequate treatment adaptations for men who experienced sexual assault, there is a need to better understand their preferences regarding psychological services. Therefore, a scoping review was conducted to document the preferences regarding psychological services identified in the literature for men who experienced sexual assault. Other aspects that may influence the uptake of psychological services by men who experienced sexual assault are barriers and motivators to help-seeking. Thus, the secondary objective of this scoping review was to explore the specific barriers and motivators to help-seeking among men who experienced sexual assault.
Method
The Ethics Committee of the Institution in which the research was conducted waived the need for ethical approval for this research project as it was based exclusively on the secondary use of published anonymous information. Preferences regarding psychological services being dispersed across multiple disciplines and methodologies, a scoping review approach, which aims to map available literature in a number of fields (Munn et al., 2022) and allow for the inclusion of multiple types of evidence, was chosen. A scoping review of the literature was thus performed to identify empirical studies documenting preferences regarding psychological services, as well as barriers and motivators to help-seeking, in men who experienced sexual assault. Preferences regarding psychological services were defined as options that are considered most appropriate by an individual under given circumstances. Psychological services included any psychological help provided by a trained provider in a variety of settings (e.g., psychotherapy, crisis, or community intervention) or modalities (e.g., face-to-face, telephone, video conferencing, online platform). Barriers to help-seeking referred to reasons reported by men who experienced sexual assault for not wanting or being able to obtain psychological services. Motivators to help-seeking were operationalized as elements identified as causing or encouraging a person to consult services.
Search Strategy
A systematic approach based on the extension for scoping reviews of the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA-ScR; Tricco et al., 2018) and the recommendations of the Joanna Briggs Institute (JBI) scoping review methodology group (Munn et al., 2022) was used to search for relevant literature. To gain a multidisciplinary view of service preferences, three databases (PsycNet, PubMed and Eric) were searched. In total, 23 search equations (see Appendix) were created based on keywords related to the topic of interest. Keywords addressed men and gender differences (i.e., “men,” “male,” “women,” “gender,” “sex,” and “differences”), psychological treatments (i.e., “treatment,” “intervention,” “therapy,” “efficacy,” and “cognitive behavioral”), psychological treatment preferences (i.e., “preferences”), traumatic events (i.e., “PTSD,” “sexual assault,” and “sexual abuse”), and others (i.e., “symptoms” and “experiences”). When a search equation yielded more than 1,000 results, an advanced search was performed using the “Keywords” filter on PsycNet. “MeSH terms” on PubMed and “Descriptor” on Eric were added to each keyword in the equation. Searches were conducted in May 2021.
Screening Process
Figure 1 presents the outcomes of the data selection process. Initial searches identified 4,056 articles, which were reviewed for eligibility based on the title and abstract. The articles had to be published over a 15-year span, between 2006 (a year marked by a notable surge in studies on male sexual assault indexed on PubMed) and May 2021 (year when the search was conducted), address sexual violence and men or gender differences. Peer-reviewed articles, theses, and dissertations, and government reports and non-peer reviewed commentary articles were included to widen the search. Reviews were included as they provided valuable recommendations and insights that complemented the primary research findings. Only case studies were excluded given their limited generalizability. Articles that targeted juvenile population were also excluded. The eligibility of the studies was assessed by two trained graduate students. Disagreements were resolved by discussion, until full inter-rater agreement was achieved. A total of 64 articles were eligible based on title and abstract.

Flowchart of the Selection of Articles
Eligible full articles had to specifically address preferences regarding psychological services, barriers to help-seeking, or motivators to help-seeking in their results or recommendations. Forty-two studies were excluded on this basis after reading the articles. Data from 22 articles were extracted by the first two authors with a systematic extraction grid detailing sample characteristics, study design, objectives, and hypotheses, and relevant results and discussion elements. Inter-rater agreement was realized. Disagreements were resolved by discussion. Selected articles were cross-referenced, resulting in 15 additional articles. A total of 37 articles, of which 35 are peer-reviewed and two are non-peer reviewed reports, were included in the scoping review. See Table 1 for a description of the studies.
Description of Included Studies (N = 37)
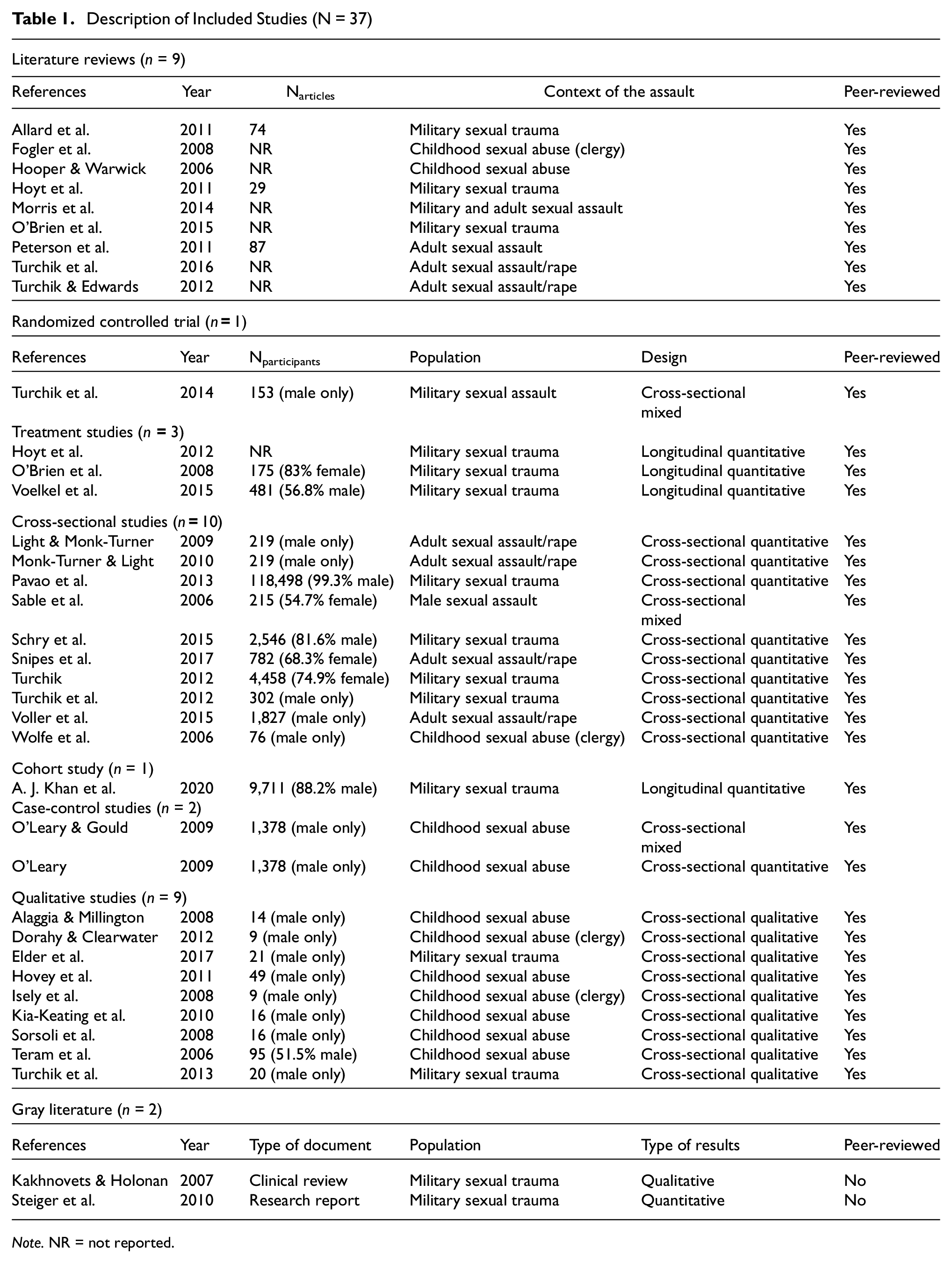
Note. NR = not reported.
Data Synthesis
To guide the presentation of the results, a thematic analysis was conducted with the main findings and recommendations of the studies. The analysis followed an iterative process, as a codebook was created and then refined as the thematic analysis progressed, using the NVivo software. The first two authors of the article conducted the analysis separately, which resulted in an excellent inter-judge agreement (K= 0.94), and then reached consensus on disagreements through discussion.
Results
Overview of Identified Literature
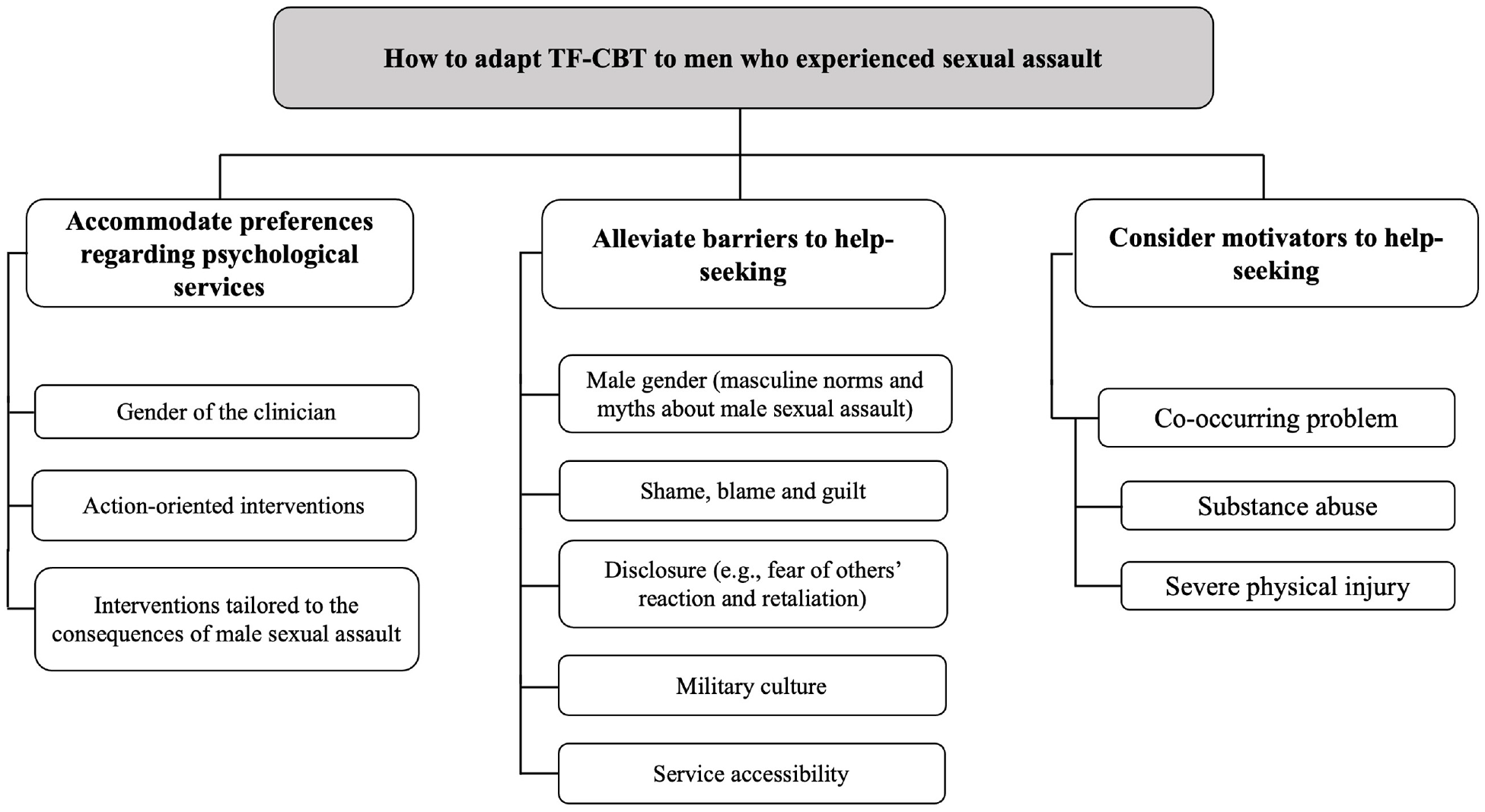
This scoping review collated literature on preferences regarding psychological services, as well as barriers and motivators to help-seeking from 35 peer-reviewed articles and two non-peer-reviewed manuscripts published between January 2006 and May 2021. The 35 peer-reviewed articles included nine literature reviews delving into other themes while addressing barriers to help-seeking in their results and 26 clinical studies using quantitative (n = 14), qualitative (n = 9), or mixed methods (n = 3). The majority of the studies were conducted in the United States and focused on a population of men who had experienced sexual assault in childhood, adulthood, or military settings. Most articles were published within the first half of the eligible timeframe (2006–2013). Table 2 presents the main relevant findings and recommendations. The literature predominantly documented barriers to help-seeking, while findings on preferences for psychological services and motivators to help-seeking were more limited. See Figure 2 for an overview of the main topics of the thematic content analysis.
Main Relevant Findings According to the Objectives of the Scoping Review

Note. MST = military sexual trauma; SA = sexual assault.
Overview of Reviewed Findings on Adaptations of TF-CBT to Men Who Experienced Sexual Assault
Preferences Regarding Psychological Services
Five studies identified preferences regarding psychological services. These articles documented that men who experienced sexual assault show preferences pertaining both to the clinician and the psychological service (see Table 2).
Preferences Related to Clinician Characteristics
Three qualitative studies (Sorsoli et al., 2008; Teram et al., 2006; Turchik et al., 2013) reported that men who experienced sexual assault may express a preference for the gender of the clinician who will provide them with services. Some men may prefer to be assisted by a male clinician because they perceive that issues related to masculinity may be better understood or to avoid being vulnerable in front of a woman (Turchik et al., 2013). Other men appeared to find it easier to share sensitive information to a female clinician, whom they perceived as compassionate and less likely to have homophobic reactions (Sorsoli et al., 2008; Teram et al., 2006; Turchik et al., 2013).
In addition, four articles (three qualitative studies and one literature review) made specific recommendations to clinicians to adopt a supportive and accepting attitude when working with men who experienced sexual assault to enhance their sense of being understood and their receptivity to psychological help (Alaggia & Millington, 2008; Fogler et al., 2008; Hovey et al., 2011; Isely et al., 2008).
Preferences Related to the Type of Intervention
One retrospective cohort study (A. J. Khan et al., 2020) demonstrated that PE was more effective than CPT among men who experienced sexual assault in a military setting. Thus, the authors suggested that PE may be more suitable for male victims of military sexual assault due to its action-oriented and concrete nature.
In terms of intervention content, a randomized controlled trial (Turchik et al., 2014) reported that men who experienced sexual assault in a military context preferred to receive information about male-specific consequences to sexual assault than general information about sexual assault. Several studies (e.g., Elder et al., 2017; Kia-Keating et al., 2010; Monk-Turner & Light, 2010) extended these findings with recommendations (in discussion or in implications for practice) for developing and providing interventions that target the specific consequences and needs of men who have been sexually assaulted.
Barriers to Help-Seeking
Several of the reviewed studies reported findings and recommendations regarding barriers to help-seeking in men who experienced sexual assault. Barriers fell into five categories, that is, related to male gender, to negative emotions (shame, blame, and guilt), to disclosure of sexual assault, to military context, and to accessibility of services (see Figure 2).
Barriers Related to Male Gender
The barriers to help-seeking most strongly supported by the reviewed literature were those related to male gender. A total of 14 studies addressing male sexual assault experienced in a variety of contexts (childhood, adulthood, and military service) identified adherence to traditional masculine norms as a barrier to help-seeking. Six of the studies were literature reviews, five were qualitative studies, one was a treatment study, and two were cross-sectional studies. The findings revealed that masculine identity may be an important issue to men who experienced sexual assault, who may feel the need to reassert their strength (O’Brien et al., 2015), self-reliance (e.g., Fogler et al., 2008; Hooper & Warwick, 2006), or emotional toughness (e.g., Hoyt et al., 2011; Turchik, 2012), in accordance with traditional masculine norms. Disclosing the assault and seeking help could therefore be viewed as signs of weakness (e.g., Hovey et al., 2011; Hoyt et al., 2011; Turchik, 2012).
The majority of studies that addressed masculine norms also identified myths about sexual assault (e.g., men cannot be sexually assaulted, men who are sexually assaulted are homosexual) as a barrier to disclosing sexual assault and to help-seeking. These myths were addressed in 12 studies (six literature reviews, four qualitative studies, and two cross-sectional studies). Men who experienced sexual assault reported fearing being labeled with unfounded or blunt stereotypes, such as they must have desired the assault, they are homosexual, they are not able to defend themselves, etc. (e.g., O’Brien et al., 2015; Teram et al., 2006; Turchik & Edwards, 2012). According to Turchik and Edwards’ (2012) literature review, these myths about sexual assault could invalidate the experience of sexually assaulted men and contradict their masculine identity. Several authors have therefore recommended integrating an educational component into interventions to deconstruct the impact of traditional masculine norms and myths about male sexual assault (e.g., Kakhnovets & Holohan, 2007; O’Brien et al., 2015).
Shame, Blame, and Guilt
Shame, self-blame, and guilt themselves act as a barrier to help-seeking. Six studies (two literature reviews, two qualitative studies, and two cross-sectional studies) have identified that feelings of shame, guilt, or self-blame for causing or failing to prevent the sexual assault were a barrier to disclosing sexual assault. The qualitative studies of Dorahy and Clearwater (2012) and of Isely and colleagues (2008) illustrated that overwhelming shame and guilt following childhood sexual abuse led to a number of other obstacles hampering help-seeking, such as a sense of inferiority and incompetence, low self-esteem, excessive anger or rage, and denial. Furthermore, O’Brien and colleagues’ (2015) literature review documented that men who did seek help often offered an incomplete trauma narrative (e.g., physical reaction) at the beginning of treatment, due to shame and guilt.
Disclosure
Ten studies identified various considerations about disclosing sexual assault to receive help as a barrier to help-seeking. Seven studies (e.g., Dorahy & Clearwater, 2012; Elder et al., 2017; Turchik et al., 2013) noted that men could fear or anticipate negative reaction (e.g., anger, laughter, denial) from relatives and health service providers on disclosure of the sexual assault, often related to myths about male sexual assault. One qualitative study (Dorahy & Clearwater, 2012) and one research report (Steiger et al., 2010) described a fear of retaliation (e.g., loss of relationships or social status, punishment for an unperformed violation) upon disclosure. Moreover, three studies identified confidentiality concerns among male victims of sexual assault when disclosing and seeking psychological help (Sable et al., 2006; Steiger et al., 2010; Turchik et al., 2013), and two studies highlighted issues of distrust and negative experiences with the justice system among this population (Sable et al., 2006; Steiger et al., 2010).
Military Culture
Five peer-reviewed articles (four literature reviews and one treatment study) and a research report (Steiger et al., 2010) identified that military culture generates unique barriers to disclosure for veterans who are victims of sexual assault, or exacerbates other existing barriers (e.g., myths about male sexual assault). The reviewed studies documented that men who are sexually assaulted in military service may be compelled to remain silent. They may feel the need to conform to the values and rules of military culture (e.g., unit cohesion) or fear that disclosing an assault by a fellow service member will be perceived as a betrayal and lead to negative consequences (e.g., Morris et al., 2014; O’Brien et al., 2015; Steiger et al., 2010).
Accessibility of Services
Perceived and actual accessibility of services was another barrier to help-seeking. Three studies (O’Brien et al., 2015; Pavao et al., 2013; Voelkel et al., 2015) indicated that more female than male victims of military sexual trauma received psychological services, notably because greater resources were allocated to women in specialized sexual assault services. Other barriers (i.e., financial concerns, lack of knowledge about available services, cultural barriers, lack of sensitivity, and awareness regarding religious beliefs) were also identified across four other studies (e.g., Light & Monk-Turner, 2009; Sorsoli et al., 2008; Turchik et al., 2013; Wolfe et al., 2006).
Motivators to Help-Seeking
The reviewed studies reported motivators to help-seeking for men who experienced sexual assault, documented in one cross-sectional study (Light & Monk-Turner, 2009) and one qualitative study (Elder et al., 2017). Both studies identified that male victims of sexual assault may be more likely to seek services for a co-occurring problem (see Figure 2). Light and Monk-Turner (2009) suggested that physical injuries resulting from the sexual assault could legitimize help-seeking for some men. In addition, Elder et al.’s (2017) study revealed that male victims of sexual assault who use alcohol or drugs excessively may be more inclined to seek help when their substance use reaches a severity requiring medical or addiction services.
Discussion
The objective of this scoping review was to document preferences of men who experienced sexual assault regarding psychological services, and to explore barriers and motivators to help-seeking. To optimize TF-CBT, researchers and clinicians could accommodate preferences regarding psychological services, alleviate barriers to help-seeking, and consider motivators to help-seeking for men who experienced sexual assault. This scoping review could contribute to guide adaptation of TF-CBT to men who experienced sexual assault.
The gender of the clinician was the preference that was most documented in the literature, although there was no consensus toward one specific gender (e.g., Turchik et al., 2013). Female clinicians were perceived as more compassionate and less likely to have homophobic reactions while male clinicians were perceived as more understanding of masculine issues (Sorsoli et al., 2008; Teram et al., 2006; Turchik et al., 2013). Thus, the opportunity to select the gender of the clinician should be given to men who experienced sexual assault, whenever possible. In addition, preferences leaned toward active and sensitive interventions tailored to male sexual assault and its consequences (A. J. Khan et al., 2020; Turchik et al., 2014). As PE is a more concrete and action-oriented, problem-solving approach than other therapeutic options (such as CPT), it may respond more adequately to the needs of men who experienced sexual assault.
Nearly half of the reviewed articles identified masculine norms and myths about male sexual assault as barriers to help-seeking, underlining the need to address these. Clinicians and other professionals should be educated about masculine norms and myths about male sexual assault. Indeed, it would enable them to adapt TF-CBT to male victims of sexual assault by adding an important psychoeducational component to deconstruct these myths and norms, as recommended by several studies in this scoping review (e.g., Kakhnovets & Holohan, 2007; O’Brien et al., 2015). This adaptation requires special attention when TF-CBT is offered in the military population since the values and rules of military culture create and reinforce traditional masculine norms (e.g., strength) and myths about sexual assault (such as the belief that men cannot be victim of the sexual assault; e.g., Morris et al., 2014; O’Brien et al., 2015).
This scoping review identified that shame, self-blame, and guilt can inhibit disclosure of sexual assault among men, hindering help-seeking behavior and often leading to the concealment of crucial details during trauma narrative (e.g., Dorahy & Clearwater, 2012; O’Brien et al., 2015). Considering this particular need, one way to adapt TF-CBT to male sexual assault victims is to proactively validate sexual assault experience and normalize the emotions and consequences associated with male sexual assault. This means that the therapist will also need to show extra sensitivity when enquiring about the assault and to avoid forcing disclosure or putting men in an unnecessary vulnerability position that may exacerbate negative emotions (e.g., shame for not defending themselves) and confront masculine identity.
Some studies documented the limited accessibility of psychological services for men who experienced sexual assault (e.g., O’Brien et al., 2015; Voelkel et al., 2015). One way to alleviate this barrier could be to develop online TF-CBT dedicated specifically to men, as it may allow men who experienced sexual assault to self-manage their difficulties, to protect their confidentiality, to reduce the risk of stigmatization, and to facilitate access to evidence-based strategies to alleviate symptoms. Randomized controlled trials have demonstrated that online TF-CBT can be effective in reducing PTSD, depression, anxiety, and insomnia symptoms (e.g., Belleville et al., 2023; Littleton et al., 2016; Spence et al., 2011).
The reviewed studies offered avenues on what motivates men who experienced sexual assault to seek help. Men appear more likely to seek help in the presence of a co-occurring problem (substance abuse, severe physical injury; Elder et al., 2017; Light & Monk-Turner, 2009). Thus, history of sexual assault could be systematically assessed in a non-confronting way in medical (e.g., hospitals, private medical clinics) or addiction settings (e.g., rehabilitation centers, men’s support organizations). Moreover, specialized sexual assault services such as TF-CBT could be promoted within these services for reference purposes.
Limitations
Although this scoping review provided useful insights about preferences regarding psychological services, as well as barriers and motivators to help-seeking for men who experienced sexual assault, the results should be interpreted in light of some limitations. First, the search strategy was based on uncontrolled vocabulary and restricted to three databases. Therefore, some studies may have been missed. However, the method was standardized and based on the best practice guidelines for conducting scoping reviews (Munn et al., 2022; Tricco et al., 2018), and the use of 23 data equations across three databases from the disciplines of medicine (PubMed), psychology (PsycNet), and education (Eric) enabled a thorough mapping of literature. Furthermore, the quality of the included studies was not assessed, which even if in line with the best practice guidelines for scoping reviews (Tricco et al., 2018), limits confidence about the robustness of the reported findings. Another caveat comes from the limited availability of empirical data on the preferences regarding psychological services from men who experienced sexual assault. Although several authors offered recommendations on this topic, as documented in Table 2, the lack of supportive evidence underscored the need for further empirical investigation. Including barriers and motivators as variables of interest may offer additional evidence-based recommendations to further adapt TF-CBT. Despite these limitations, this scoping review was the first to have a primary aim of exploring preferences regarding psychological services among men who experienced sexual assault. It provided rich results on different components of help-seeking (preferences, barriers, and motivators). The use of a thematic content analysis helped to organize the available literature to offer pragmatic ideas to target the necessary adaptations to TF-CBT for men who experienced sexual assault.
Conclusion
In conclusion, men who experienced sexual assault have preferences toward psychological services but also face barriers to seeking psychological help. Despite a substantial body of peer-reviewed literature documented barriers to help-seeking, empirical data on preferences regarding psychological services are scarce, indicating a notable knowledge gap. Moreover, existing literature predominantly focuses on very specific preferences regarding psychological services, often using qualitative methodologies, and primarily among men who have been sexually assaulted in the military. To address this gap, further research is needed to comprehensively document preferences regarding psychological services across various clinical and demographic contexts. Potential research avenues could involve distinguishing preferences for psychological services among men who experienced sexual assault according to the context of the assault (e.g., childhood, adulthood, in the military) and according to identity factors (e.g., ethnicity, ability status, sexual orientation). In light of findings of this scoping review regarding PE, further treatment studies focusing on this therapy are necessary to demonstrate whether it aligns with the preferences of men who experienced sexual assault, and whether this alignment enhances treatment response. This research could provide valuable guidance for clinicians and researchers in adapting TF-CBT treatment plans for men who experienced sexual assault. Such studies could provide further insight on how to mobilize men toward psychological services and to maximize the efficacy of TF-CBT according to their preferences and needs.
Footnotes
Appendix
Acknowledgements
The first author thanks the Canadian Institutes of Health Research and the Fonds de recherche Québec—Santé for providing the training award opportunities during the completion of this scoping review. The authors thank Nohad Majani for help in screening articles.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: L.G. holds a doctoral scholarship from the Canadian Institutes of Health Research (grant no. 493564) and held master-level awards from Fonds de recherche Québec—Santé (grant no. 302194) and the Canadian Institutes of Health Research (Frederick Banting and Charles Best Canada Graduate Scholarships, grant no. 499299).