
Abstract
Being a man has been recognized as a salient risk factor for suicide. Adopting uncompromised masculine perceptions (i.e., conforming to the masculine gender role norms) may restrict emotional expressiveness in men, which, in turn, may contribute to depression and somatization symptoms. We examined the moderating role of psychological flexibility and alexithymia in the relationship of masculinity with depression and somatization symptoms. A sample of 119 men completed measures of masculinity, alexithymia (difficulty identifying and delivering subjective feelings), psychological flexibility, depression, and somatization symptoms in a cross-sectional design study. Psychological flexibility levels moderated the relationship between masculinity and depression symptoms: Masculinity contributed as positively associated with depression symptoms when psychological flexibility was low, but no such association was found at moderate or high levels of psychological flexibility. As a cognitive factor promoting adaptive emotional regulation, psychological flexibility might reduce depression symptoms among inflexible masculine men. Clinical implications relate to diagnosing at-risk subgroups and their treatment.
Keywords
Introduction
Gender has been recognized as a high-risk factor for depression (Mann et al., 2021) and suicide (Cleary, 2019). Suicide is four times as frequent among men than women in most Western countries (World Health Organization, 2021), whereas depression is lower for men than women (Kessler & Bromet, 2013; Simon et al., 2002). Many studies have sought to explain this gap. Some men find it difficult to seek help and express distress, an inclination manifested in their underreporting of distress (Chandler, 2022; Fields & Cochran, 2011; King et al., 2020). Upon considering gender differences in psychophysiology, neurobiological and hormone differences across the life span have been identified as associated with depression prevalence (e.g., pregnancy; Eid et al., 2019), and emotion regulation was reported as affected by social gender role norms, such as norms of masculinity (Hammond, 2012; Rochlen et al., 2010; Seidler et al., 2016). However, the role of gender perception, detailed below, has remained unexamined.
Depression is closely associated with mental health problems such as somatization symptoms (Lieb et al., 2007), alexithymia (Hemming et al., 2019), suicidality (Mann et al., 2021), and post-traumatic stress disorder (PTSD; O’Donnell et al., 2004). Depression also plays a critical role in health problems (e.g., back pain; Pinheiro et al., 2016). Extensive professional literature has sought to identify internal and external factors that increase depression symptoms.
Several conditions have been recognized as risk factors for depression. Among these are comorbid psychiatric disorders and stressful life events (e.g., PTSD; O’Donnell et al., 2004), genetic inclinations, neurobiological deficits, and social alienation (Avenevoli et al., 2015; Burcusa & Iacono, 2007). From the perspective of gender roles in some Western cultures, social expectations for men, relative to women, have been linked to a lower inclination for help-seeking and a higher prevalence of aggressive behavior and substance abuse (Harding & Fox, 2015; Reidy et al., 2009), resulting in some masculine expectations comprising facilitators of men’s mental health problems. Several studies have reported a consistent trend of associations between problematic extroverted behaviors, such as aggressive behavior and substance abuse, and depression symptoms in men (McDermott et al., 2016; Rice et al., 2013).
Masculinity is a complex construct often associated with socialization processes beginning in childhood (Addis et al., 2010). The experience of masculinity is dynamic and context-dependent and tends to be influenced by social structures and power dynamics (Robertson et al., 2016). Over the years, several conceptual models of the masculine construct have been introduced. The traditional masculinity model, based on norms of stoicism, self-reliance, and power (Addis & Cohane, 2005), is perceived by many as primitive, negative, and patriarchal (Everitt-Penhale & Ratele, 2015). The hegemonic masculinity model, which has won wide recognition, refers to a socially ideal masculine behavioral pattern, presenting the most respectable way of being a man in a given society (Connell & Messerschmidt, 2005). The hegemonic relational pattern includes eschewing behaviors socially defined as feminine (e.g., complaining or asking for help), denial of weakness, emotional self-control, physical dominance, and aggressive behavior (Cole & Davidson, 2019; Mahalik et al., 2003). These masculine gender role perceptions have been thought to be responsible for some men to embrace negative beliefs and negative health behaviors (Harper & Harris, 2010). These negative beliefs and behaviors can provide fertile ground for the development of mental health symptoms, including depression and suicide risk (Bennett et al., 2023; Möller-Leimkühler, 2002).
Whereas no formal social prohibitions constrain unconventional expressions of masculinity, men who do so will invariably cross gender role boundaries and thus risk social sanctions (Courtenay, 2000; O’Neil, 2008). Some men may experience internal contradictions, often feeling denied the option of expressing themselves more freely due to their stiff perceptions regarding masculine demands such as stoicism and self-reliance (Connell & Messerschmidt, 2005). These internal conflicts may promote a maladaptive coping style, especially among those who stiffly adopt the masculine gender role, frequently manifested in a restrained approach toward emotional situations (e.g., self-enclosure; Addis & Mahalik, 2003). This restricted attitude may explain some men’s reluctance to seek mental treatment even during severe crises (Cleary, 2017; Nam et al., 2010; Seidler et al., 2016). In response to the reluctance of some men to seek assistance following events such as divorce, they may experience an aggravation of mental distress, often exacerbating helplessness and misery. Consequently, they may resort to maladaptive and masculine socially endorsed behaviors, such as aggression and substance abuse, as immediate means to alleviate their psychological distress (Hasin et al., 2007; Magovcevic & Addis, 2008; Rice et al., 2013; Seidler et al., 2016). Internal contradictions and self-stigma regarding how a man presents his gender role seem to contribute critically to mental health problems among some men, including depression symptoms (Mahalik & Di Bianca, 2021).
Following assumptions of the deficit model of masculinity, high conformity to the masculine gender role as a whole construct has been associated with problematic characteristics and mental health symptoms (Bennett et al., 2023; Milner et al., 2018; O’Neil, 2012). However, the dynamic nature of how masculinity is perceived and manifested in different contexts and social environments encouraged the coining of the term “masculinities,” which facilitated a broader perspective regarding the presentations of masculinity (Messerschmidt & Messner, 2018; Robertson et al., 2016). Masculinities are not solely individual characteristics but are also shaped by institutions and societal norms such that they are both the producers and products of social structures and human agency. Notions such as caring masculinities reflect the dynamic nature of masculinity by emphasizing how masculinity can change and adapt within the masculine-framed norms. Refiguring masculinity by eschewing the domination components while adopting values such as caring and interdependence may hint at how some men can change values within the masculine-framed norms, adopt positive values, and attain positive health and well-being outcomes (Elliott, 2016; Messerschmidt & Messner, 2018; Tang et al., 2014).
Individual differences in the implications of some masculine norms on men’s mental health have also been reported (Hammer & Good, 2010; Wong et al., 2017), suggesting potential protective moderators that might function as a buffer between masculinity and mental health symptoms. An explanation for these findings may stem from the multiple sub-dimensions (e.g., self-reliance) composing the hegemonic masculinity construct, some of which have been associated with positive mental health outcomes (Iwamoto et al., 2018; Kaya et al., 2019). Adopting the primacy of work and ambitiousness, considered part of the masculine construct (Mahalik et al., 2003), has been associated with healthy psychological well-being (Kaya et al., 2019). Given the dynamic nature of the masculinity construct as reflected in the literature (Robertson et al., 2016), men’s ability to espouse a flexible masculine image, adopting some sub-dimensions while eschewing others, may protect them from mental symptoms.
Psychological flexibility is “the tendency to respond to situations in ways that facilitate valued goal pursuit” (Doorley et al., 2020, p. 2). Research has identified this trait as an important psychological asset that enhances mental health (Doorley et al., 2020; S. C. Hayes et al., 2004). This capacity to be flexible correlates negatively with depression, anxiety, stress, substance abuse, chronic pain, thought suppression, and job burnout (Bond et al., 2011; de Boer et al., 2014; Lloyd et al., 2013; Luoma et al., 2011). The masculine ideal reflected in the hegemonic model of masculinity includes features such as showing strength, emotional control, and diminished self-disclosure (Mahalik et al., 2003). A combination of a high degree of masculine gender role adoption and psychological inflexibility may contribute to mental health problems. However, psychological flexibility may mitigate the relationship between the degree of masculine gender role adoption and depression and somatization symptoms. Aspects of psychological flexibility, such as values-driven conduct and cognitive diffusion, offer potential assistance to some men experiencing depression. Psychological flexibility may mitigate cognitive contagion associated with gender-based self-image and contradictions surrounding help-seeking, such as by being liberated from their thoughts and perceptions regarding masculine norm expectations and utilizing values-guided behavior to seek help.
Another facet may be reflected by alexithymia, indicating difficulty identifying and expressing feelings to oneself and others. Men have consistently been characterized as having higher alexithymia levels than women (Levant et al., 2009; Li et al., 2015). Alexithymia is associated with mental health problems such as anxiety, aggression, suicidality, and depression (Berardis et al., 2008; Fietz et al., 2018; Hornsveld & Kraaimaat, 2012; Li et al., 2015; Osimo et al., 2021). Whereas alexithymia is closely related to these mental health difficulties, especially depression, it has been identified as a distinct construct (Gilanifar & Delavar, 2016; Hemming et al., 2019). The capacity to identify and express feelings may be an independent construct associated with depression symptoms, especially in men. Therefore, alexithymia might moderate the relationship between masculinity, depression, and somatization symptoms.
The current study seeks to shed light on the nature of the association between masculinity and mental health problems, specifically depression and somatization symptoms, which are closely related but distinct constructs (Kroenke et al., 2010; Rief et al., 2010). In the present study, we considered the masculinity construct to be complex and multidimensional and explored its relationship with men’s depression and somatization symptoms. We examined psychological flexibility and alexithymia as possible protective moderators mitigating this relationship. To our knowledge, no study has addressed psychological flexibility and alexithymia directly as protective factors for depression and somatization symptoms while considering men’s masculinity level. Three main hypotheses were examined:
Methods
Participants
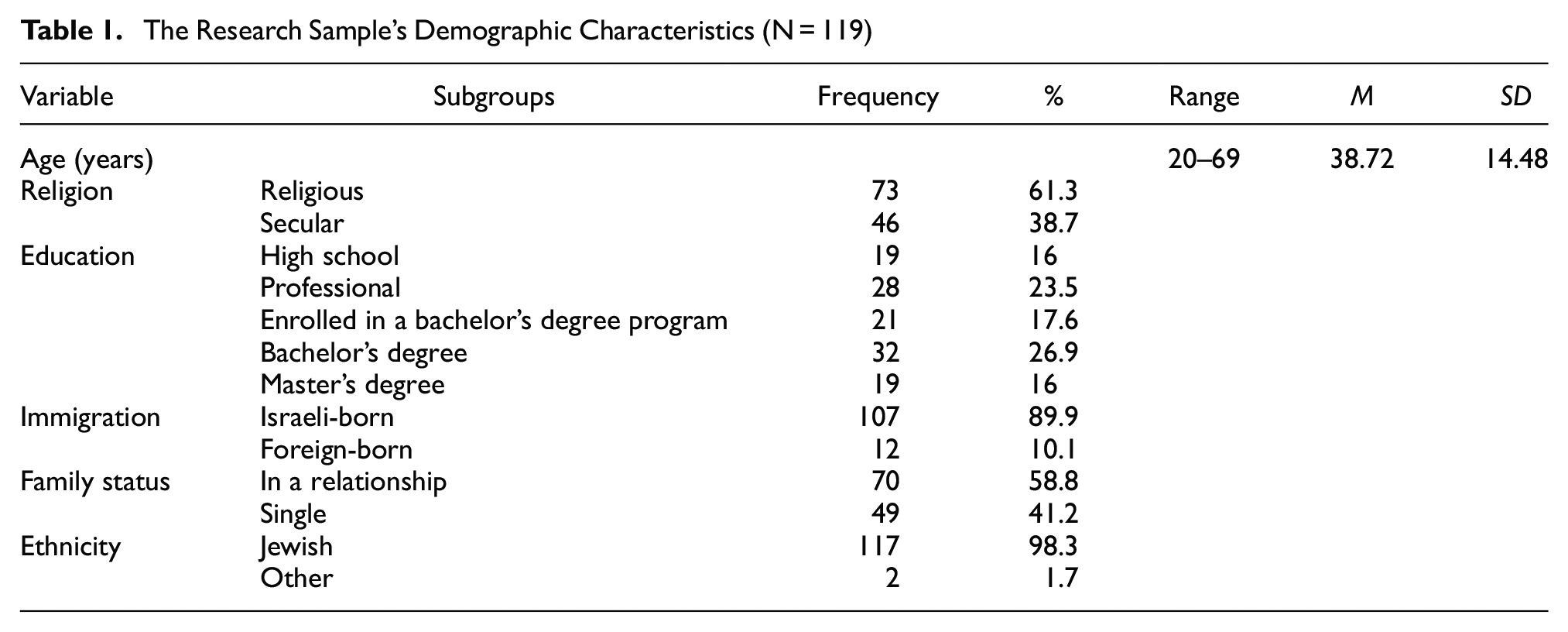
The study sample comprised 119 (all male) adult participants who completed all study questionnaires. Participants were recruited voluntarily from the community responding to an invitation on social media or students who volunteered to accumulate research hours for an Introduction to Psychology course at Ruppin Academic Center in Israel. The sample’s demographics are presented in Table 1. Participants’ mean age was 38.72 (SD = 14.48) years. Participants’ education levels varied: 16% (n = 19) completed high school, 23.5% (n = 28) had acquired professional non-academic training, 17.6% (n = 21) were enrolled in a bachelor’s degree program, 26.9% (n = 32) held a bachelor’s degree, and 16% (n = 19) held a master’s degree and above. Moreover, 58.8% (n = 70) were in some relationship, and 41.2% (n = 49) were single. Among the participants, almost all (98.3%, n = 117) were Jewish; 61.3% (n = 73) identified themselves as religiously observant and 38.7% (n = 46) as secular. Regarding place of birth, 89.9% (n = 107) were Israeli-born, and 10.1% (n = 12) were foreign-born.
The Research Sample’s Demographic Characteristics (N = 119)
Measures
Conformity to the Masculine Gender Role
The Conformity to Masculine Norms Inventory-46 (Parent & Moradi, 2009) was designed to measure conformity to the masculine gender role, originally through nine scales. For the present study, we adopted items from seven scales relating to the study’s aim: winning, emotional control, violence, power over women, playboy, self-reliance, and heterosexual self-presentation. Each of the seven scales comprised four to six items regarding masculine perceptions, resulting in 37 total items. Items were presented on a 4-point Likert-type scale (e.g., “I never share my feelings”), ranging from 1 (Strongly disagree) to 4 (Strongly agree). We calculated a total mean score of the questionnaire, with higher scores indicating greater adherence to the masculine gender role. For the present sample, the questionnaire’s internal consistency was α = .80.
Alexithymia
The Toronto Alexithymia Scale (TAS; Bagby et al., 1994) measures the ability to recognize emotions using three scales: difficulty recognizing emotions, difficulty describing emotions, and external thinking. The TAS comprises 20 statements concerning the identification of emotions (e.g., “I have feelings that I can’t quite identify”), with each item presented on a 5-point Likert-type scale, ranging from 1 (Strongly disagree) to 5 (Strongly agree). A total sum score was calculated, with higher values representing a higher degree of difficulty with emotional recognition. For the current study, we used the Hebrew version of the TAS (Zohar & Cloninger, 2011). The TAS’s internal consistency for the current sample was α = .80.
Psychological Flexibility
The Acceptance and Action Questionnaire – version 2 (AAQ-II; Bond et al., 2011) measures the degree of psychological flexibility. The AAQ-II comprises seven statements regarding psychological flexibility (e.g., “I’m afraid of my feelings”), presented on a 7-point Likert-type scale, ranging from 1 (Never true) to 7 (Always true). The responses were summed to a total score, with higher values indicating greater psychological flexibility. For the present sample, the internal consistency was α = .87.
To examine the degree of psychological and physical distress symptoms, two questionnaires assessing depression and somatization were used.
Depression
The widely used Patient Health Questionnaire-9 (Kroenke et al., 2001) examined the respondents’ depression symptoms in the last 2 weeks. The nine statements regarding symptoms of depression (e.g., “Little interest or pleasure in doing things”) were presented on a 4-point Likert-type scale ranging from 0 (Not at all) to 3 (Nearly every day), with higher ratings indicating more frequent depression symptoms. These nine items were summed for a total score of depression severity. In the present study, the internal consistency was α = .79.
Somatization
The somatization subscale of the Brief Symptom Inventory (BSI; Derogatis & Spencer, 1982) was used to examine somatic symptoms. The measure elicits to what extent the problem distresses or bothers the respondent over the last month (e.g., “How much were you distressed by feeling weak in parts of your body”; Mohammadkhani et al., 2010). The BSI comprises seven statements describing somatic symptoms, presented on a 5-point Likert-type scale ranging from 0 (Not at all) to 5 (Very much). The somatization subscale’s seven ratings were averaged to determine its score, with higher scores indicating more somatic symptoms. For the present sample, the internal consistency was α = .84.
Socio-Demographic Characteristics
We assessed socio-demographic characteristics, including age, education, family status, immigration, ethnicity, and religion.
Procedure
Participants received an online link with self-report questionnaires distributed via Qualtrics software on social networks in a non-random convenience sample using the snowball method. The participants were required to affirm their willingness to participate in the study and provide informed consent after reading the explanation of the study’s aims. Those agreeing were asked to complete the questionnaire, comprising closed questions regarding their demographics, mental and physical health, and gender role beliefs. The ethics committee of Ruppin Academic Center approved this study.
Data Analysis
Pearson intercorrelations between the study variables and demographics were calculated, followed by two four-step hierarchical regression analyses, one for depression and one for somatization. All independent variables were centered before entering the regression models. To statistically control age, education, family status, and religion, these were inserted into the equation in Step 1. Masculinity was entered in Step 2. After controlling for all other variables, alexithymia and psychological flexibility levels were entered in Step 3 to examine their contributions. To examine the combined contribution of masculinity–psychological flexibility and masculinity–alexithymia, these hypothesized two two-way interactions were entered in the final step. The same procedure was then carried out with somatization as a dependent variable. Following the regression, simple slopes post hoc analysis was performed using the PROCESS macro for SPSS (Model 1; A. F. Hayes, 2013) to examine the nature of the interactions within a regression framework. The statistical significance of the coefficients was confirmed by constructing 95% confidence intervals using a bootstrap procedure (see Efron & Tibshirani, 1986) with 1,000 resamples. SPSS (v26.0 for Windows) was used for all analyses. The level of statistical significance was set at p = .05.
Results
Preliminary Analysis
In a preliminary analysis, the correlations between the study variables and demographics were calculated. The means, standard deviations, and intercorrelations are presented in Table 2. Alexithymia correlated positively with somatization symptoms (r117 = .24, p < .01) and depression symptoms (r117 = .34, p < .001). Psychological flexibility correlated negatively with somatization symptoms (r117 = −.38, p < .001) and depression symptoms (r117 = −.55, p < .001). In addition, depression symptoms revealed a strong positive correlation with somatization symptoms (r117 = .60, p < .001).
Intercorrelations Between the Study Variables and Demographics (N = 119)
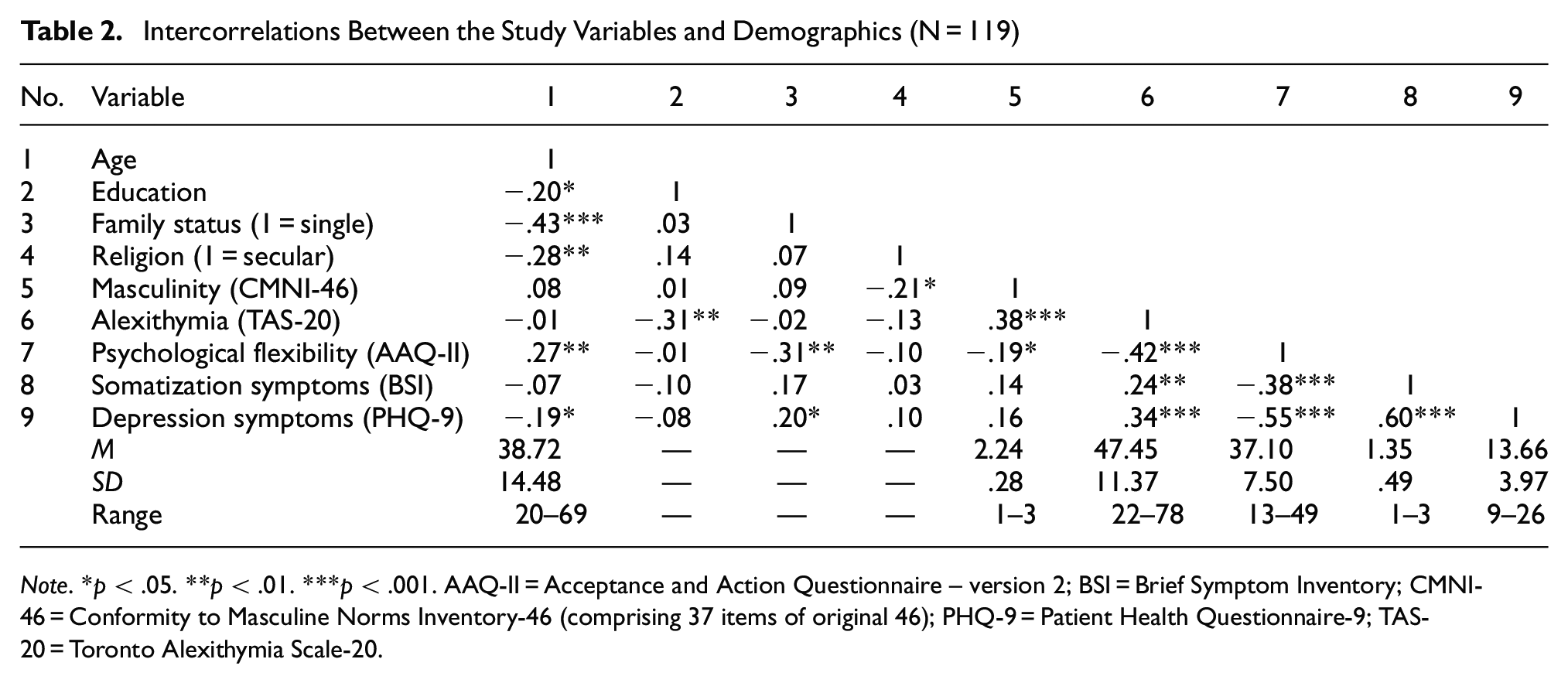
Note. *p < .05. **p < .01. ***p < .001. AAQ-II = Acceptance and Action Questionnaire – version 2; BSI = Brief Symptom Inventory; CMNI-46 = Conformity to Masculine Norms Inventory-46 (comprising 37 items of original 46); PHQ-9 = Patient Health Questionnaire-9; TAS-20 = Toronto Alexithymia Scale-20.
Hierarchical Regression Analysis for Depression Symptoms
To examine the moderating role of psychological flexibility on the relationship between masculinity and depression symptoms, beyond demographics and study variables, a four-step hierarchical regression analysis (Cohen et al., 2013) was conducted with depression symptoms as the dependent variable.
Overall, the whole model was found significant (Fmodel(9, 109) = 6.91, p < .001) with 36.3% of the depression symptoms variance explained by the predictors (adjusted R2 = .311). Step 1 did not contribute significantly to the depression symptoms, as seen in Table 3. In Step 2, masculinity was entered into the model and was found significant (Fchange-Step2(1, 113) = 4.31, p < .05), contributing an increase of 3.4% to the explained variance for depression symptoms. In Step 3, alexithymia and psychological flexibility were entered into the model and were found significant (Fchange-Step3(2, 111) = 18.68, p < .001), contributing an increase of 22.6% to the explained variance for depression symptoms. In Step 4, the masculinity–alexithymia interaction and the masculinity–psychological flexibility interaction were entered into the model. The addition of the interactions yielded only marginal significance (F(2, 109) = 2.87, p = .061). However, the masculinity–psychological flexibility interaction contributed a unique negative contribution to the prediction of depression symptoms (b = −.80, t109 = −2.18, p < .05).
Hierarchical Regression Model Summary to Predict Depression Symptoms (N = 119)

Note. *p < .05. ***p < .001. AAQ-II = Acceptance and Action Questionnaire – version 2; CMNI-46 = Conformity to Masculine Norms Inventory-46 using 37 statements out of 46; PHQ-9 = Patient Health Questionnaire-9; TAS-20 = Toronto Alexithymia Scale-20.
Moderation Analysis for Depression Symptoms
To examine the nature of the interaction between masculinity and psychological flexibility on depression symptom levels, we performed a moderation analysis using PROCESS macro (Model 1; A. F. Hayes, 2017). In this analysis, masculinity was the independent variable, and psychological flexibility was the moderator. The interaction was found significant (F(1, 109) = 4.75, p < .05). At low levels of psychological flexibility, the relationship between masculinity and depression symptoms was positive and significant (β = .29, t(109) = 2.13, p < .05) as shown in Figure 1. However, at moderate psychological flexibility levels, this relationship diminished, becoming non-significant (β = .09, t(109) = .98, p = .327). At high levels of psychological flexibility, the relationship between masculinity and depression symptoms further changes direction, becoming negative though non-significant (β = −.12, t(109) = −.98, p = .330).
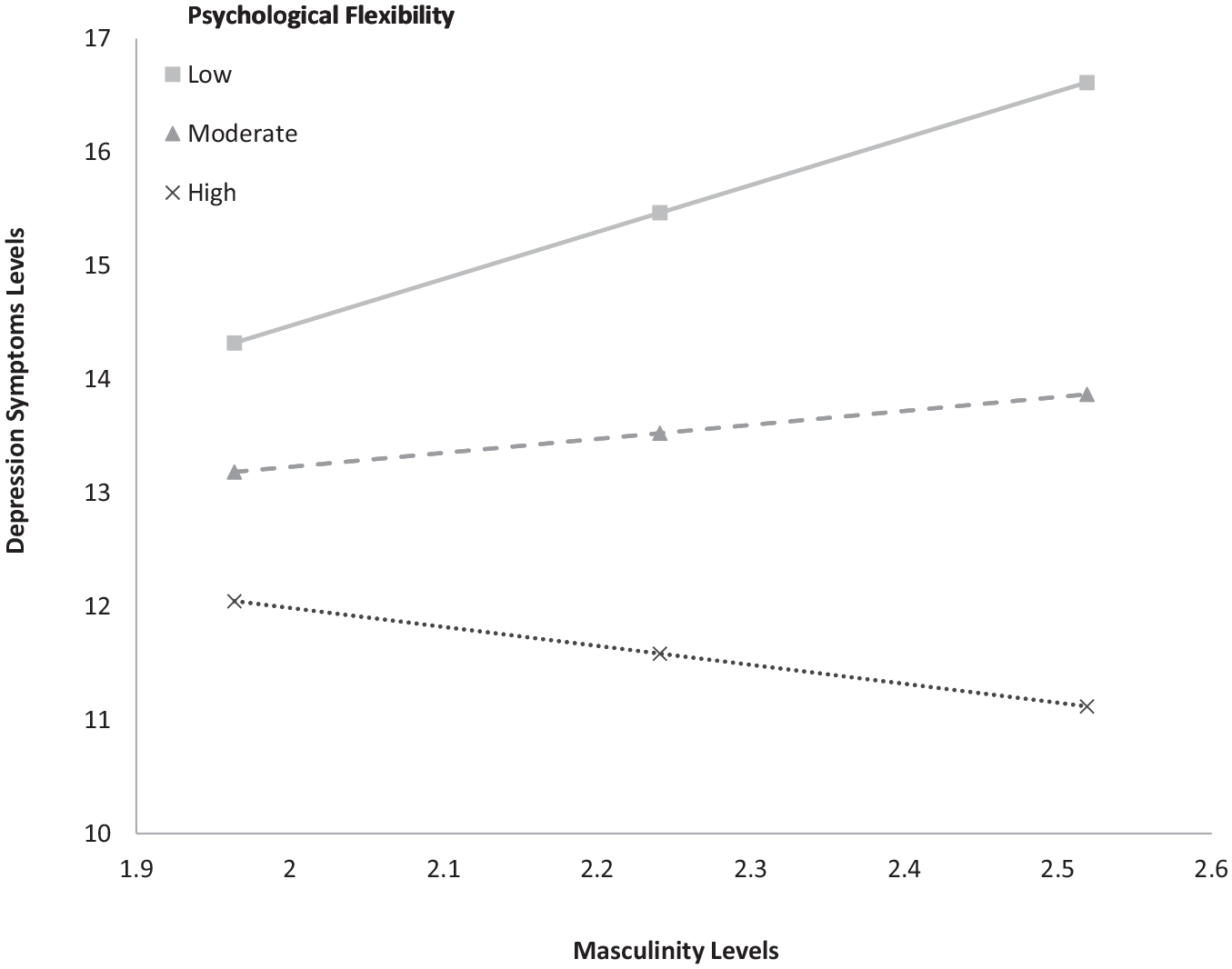
Depression Symptoms as a Function of Masculinity and Psychological Flexibility Levels (N = 119)
Hierarchical Regression Analysis for Somatization Symptoms
To examine the moderating role of psychological flexibility on the relationship between masculinity and somatization symptoms, beyond demographics and study variables, a four-step hierarchical regression analysis (Cohen et al., 2013) was conducted with somatization symptoms as the dependent variable.
Overall, the whole model was found significant (Fmodel(9, 109) = 2.50, p < .05) with 17.1% of the variance in somatization symptoms explained by the predictors (adjusted R2 = .103). Step 1 did not significantly contribute to the somatization symptoms. In Step 2, masculinity was entered into the model and was found non-significant (Fchange-Step2(1, 113) = 2.43, p = .122) yielding an increase of 2% in the explained variance for somatization symptoms. In Step 3, alexithymia and psychological flexibility were entered into the model and were found significant (Fchange-Step2(2, 111) = 7.22, p < .001) increasing the explained variance for somatization symptoms by 10.8%. In Step 4, the masculinity–alexithymia interaction and the masculinity–psychological flexibility interaction were entered into the model. The addition of the interactions was found non-significant (Fchange-Step4(2, 109) = 0.02, p = .982) as well as the contribution of each interaction discretely. Thus, we discontinued the moderation analyses of somatic symptoms as the dependent variable.
It is important to note that the moderation effect between masculinity and psychological flexibility was mainly observed for the total score and not for the subscales. This aligns with our understanding that for high flexibility, there is less impact for one subscale over another which emphasizes the dynamic nature of masculinity construct, and allows men to overcome challenging contradictions and perceptions. Hence, we presented the masculinity construct based on the total score.
Discussion
The masculine gender role construct has been associated with a wide range of problematic behaviors and mental health symptoms, including depression and somatization (Hasin et al., 2007; Mahalik & Di Bianca, 2021; Milner et al., 2018; O’Neil, 2012). Whereas these reported findings have been consistent and widespread, recent research has pointed to the dynamic nature of masculinities (Elliott, 2016; Robertson et al., 2016), including identifying differential effects, positive and negative, subject to different masculine gender role dimensions (Wong et al., 2017). Thus, we treated the masculinity construct as a complex rather than a single coherent construct by investigating psychological flexibility and alexithymia as possible moderators of the relationship of masculinity with both depression and somatization symptoms.
Our first hypothesis (Hypothesis 1) was partially confirmed. Men reporting relatively high masculine gender role adoption levels also reported significantly higher depression symptoms beyond the contribution of age, education, family status, and religion. However, this effect was not evident for somatization symptoms. The contribution of masculinity to depression symptoms beyond demographic variables aligns with the hegemonic theoretical model of masculinity (Connell & Messerschmidt, 2005) and with previous studies highlighting the critical role of sociocultural contexts when examining masculine gender role perceptions and mental health symptoms relationships (Canetto, 2008, 2017; Robertson et al., 2016). Our second hypothesis (Hypothesis 2) was confirmed, predicting that psychological flexibility will negatively contribute to depression and that somatization and alexithymia will positively contribute to depression and somatization. Critically, aligning with our third hypothesis (Hypothesis 3a), psychological flexibility moderated the relationship between masculinity and depression symptoms: Masculinity was associated with depression symptoms only at low psychological flexibility levels.
The Moderating Role of Psychological Flexibility
Psychological flexibility’s moderating role in our study is consistent with recent research reporting a similar moderating effect in decreasing mental health problems, including depression symptoms (Fonseca et al., 2020). This finding also expands the empirical and theoretical support for acceptance and commitment therapy (ACT)’s hypothesis regarding the negative implications of psychological inflexibility (S. C. Hayes et al., 2004) in the context of gender role perceptions. Men reporting a higher degree of masculinity and psychological inflexibility are more likely to experience depression symptoms. The degree of psychological inflexibility may be expressed by rigid adherence to harmful health behaviors and perceptions, such as substance abuse and an aggressive attitude. Subsumed under the prevailing masculine gender role norms, this rigidity and inflexibility will likely affect one’s coping style, especially following emotion-laden situations (Seidler et al., 2016).
One explanation for these findings may lie in the mutual influence of internal and external factors. Some scholars have suggested that external socialization processes promote internal schemas of gendered behaviors and perceptions conforming to social masculine expectations (Mahalik et al., 2007; McCusker & Galupo, 2011; Robertson et al., 2016). Previous research has shown that due to the critical role of the social environment in masculine gender role perceptions, some men who experience the environment as uncompromised regarding masculine perceptions are more concerned with their masculine self-representation and are more likely to adopt a narrow and stiff masculine gender role norms schema (Gibbs et al., 2011; Gould et al., 2010; Milner et al., 2018). As a result, they may manifest more negative extroverted behaviors and perceptions aligned with the hegemonic masculine gender role, such as aggression and self-enclosure (Magovcevic & Addis, 2008; Seidler et al., 2016). These negative extroverted behaviors and perceptions have been recognized as facilitators for severe psychiatric conditions (e.g., suicide risk; Bennett et al., 2023; Cleary, 2017; Gvion & Levi-Belz, 2018; Levi-Belz et al., 2014) and a leading cause for masked depression symptoms in some men (e.g., Martin et al., 2013).
Internally, men with high levels of psychological inflexibility may be more likely to adopt a rigid masculine gender role schema about themselves and others (Cole & Davidson, 2019). While men who have adopted a rigid masculine schema may experience internal gender conflict that contradicts their harsh masculine schema, they may also be more likely to express intense feelings such as guilt and shame (Cohn & Zeichner, 2006; Stolorow et al., 2014). These feelings of guilt and shame may, in turn, facilitate maladaptive coping styles such as self-reliance and emotional control rather than help-seeking (Mahalik & Di Bianca, 2021). Open and flexibly minded men, especially with regard to masculine gender role norms, may be more liberated from social expectations, which, in turn, may lead to their being less subject to internal gender conflict, a condition consistently reported as associated with depression (Addis, 2008; Mahalik et al., 2003; Martin et al., 2013; Rice et al., 2013). These relatively open men may prioritize their valued personal goals and adapt their masculine schema accordingly without being troubled over their “damaged” masculine self-representation (Tang et al., 2014). Notably, even after controlling for alexithymia and age, factors reported as salient contributors to depression symptoms (Levant et al., 2009), this moderating effect was preserved.
Interestingly, the moderation role of psychological flexibility was evident only in the relationship between masculinity and depression symptoms. Psychological flexibility was not shown to moderate the masculinity–somatization relationship despite depression and somatization having been recognized as closely associated constructs (Bener et al., 2013). This finding may be understood by considering the theoretical basis of each construct. Depression is understood as enhanced by a cognitive rehearsal of “automatic negative thoughts,” as asserted in Aaron Beck’s work on the cognitive triad (Beck, 1979) and reinforced by substantial research demonstrating a strong effect of cognitive behavioral therapy (Clark et al., 2000). Depression’s cognitive component (cognitive bias) seems very impactful and, therefore, more affected by the degree of psychological flexibility manifesting in one’s inclination to think, behave, and feel without being subject to cognitive contagion (Luoma et al., 2007).
Aligned with previous studies, we found alexithymia to be strongly associated with the degree of masculine gender role adoption and depression symptoms (Li et al., 2015). However, alexithymia did not moderate the masculine gender role’s relationship with depression or somatization symptoms. Thus, alexithymia may not be an independent construct but a confounding factor in the masculine gender role construct. Alexithymia may emerge and be maintained by prolonged avoidance of self-disclosure, considered a significant component of masculine gender role norms (Addis & Mahalik, 2003; Stolorow et al., 2014), which, in turn, can facilitate mental health problems such as depression (e.g., Li et al., 2015).
Our findings should be interpreted in the context of several limitations. First, the study’s cross-sectional design and the correlational nature of our findings constrain deriving causal inferences. We assumed that the construct of masculine gender role adoption would function as a catalyzer of mental health outcomes; however, the reverse can be true. Future studies should examine these associations in a longitudinal design to confirm the examined phenomena’s direction.
A second limitation stems from the elusive nature of the masculinity construct. As established in the literature on socialization processes, the masculine gender role is a consequence of prolonged interactions between the external environment and internal perceptions (Robertson et al., 2016). The construct of masculine gender role adoption seems subject to various interpretations by the depressed male. Negative mood symptoms of depression at the time of the study may have influenced the participants’ perceptions about themselves, the world, and the future and, consequently, may have confounded their self-reports of their masculine gender role perceptions. Follow-up prospective studies should seek causal inferences regarding the associations between masculine gender role norms and depression symptoms and clarify the direction of this association.
A third salient limitation derives from our sampling procedure, the sample size, and the sample’s characteristics. We used a volunteer sampling method and provided an online link via social media and online academic facilities. Our volunteer sample was small and thus may represent a range restriction in the men’s population: Relative to women, men tend to be less cooperative with mental health practitioners (Call & Shafer, 2018; Cleary, 2017) and are generally far less self-disclosing of their feelings, thoughts, and beliefs (Schaub & Williams, 2007). As our study suffered from substantial dropout—more than one-third of the participants who began the questionnaire did not complete it—we suggest that several of those agreeing to participate were offended or taken aback by the questionnaires’ content, choosing to discontinue their responding. Following this scenario, participants completing our questionnaires may have been more moderate, open, and flexible in their masculine perceptions and, thus, may not adequately represent the entire population of men. Thus, the nature of our final sample may underestimate the implications of the masculine gender role’s impact on mental health status, reflecting a more positive picture than that characterizing the general male population. In addition, although we examined masculinity perceptions among men, we did not collect information on sexual orientations, which could interact with individuals’ flexibility regarding the masculine image. Future research could explore the relationship between sexual orientation, masculine perceptions, and psychological flexibility.
Clinical Implications and Conclusions
Several implications of our study are noteworthy. Regarding diagnostic implications, our findings reveal psychological flexibility to be a significant buffering factor in the relationship between masculine gender role adoption and depression symptoms, expanding our understanding of how some men develop and experience depression symptoms. Our findings underscore the critical implications of psychological flexibility in some men’s emotional status. Mental health practitioners and social workers interacting with men should evaluate their patients’ psychological inflexibility as a potential facilitator of depression symptoms and extroverted problematic behaviors associated with depression in men (McDermott et al., 2016; Rice et al., 2013). From a therapeutic perspective, ACT, which promotes psychological flexibility, may offer a beneficial therapeutical approach for men adopting the stereotypic male gender role. ACT may help these male patients acquire skills to reduce their likelihood of contagion with the gendered contradictions they may experience. Furthermore, ACT may assist in enhancing being in time, thought diffusion, and values-guided behavior. In conclusion, the buffering effect of psychological flexibility should be a salient consideration when inquiring about diagnosing and promoting men’s mental health. In some men, psychological flexibility could moderate the relationship between conformity to masculine norms and depression symptoms, as masculinity adherence is positively associated with depression symptoms when psychological flexibility levels are low. As a cognitive factor promoting adaptive emotional regulation, psychological flexibility might assist in reducing depression symptoms among some inflexible masculine men.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.