
Abstract
During the postpartum period, fathers may be at risk of increased stress and loneliness, which may be offset or buffered by the provision of social support. This study aimed to explore fathers’ postpartum experiences of loneliness, perceived stress, and social support. A constructivist grounded theory approach was used to inform study design and analysis. Semistructured interviews were conducted to collect data from 12 fathers, living in the Republic of Ireland, who had an infant aged 6 months or younger. A grounded theory entitled “support for the supporter,” describing fathers’ experiences with social support, and loneliness during the postpartum period, was derived. Participants described experiencing increased financial pressure and having difficulty balancing the role of “breadwinner” with fatherhood. Participants described feeling excluded from maternity care and lacked avenues for information within the Irish health care system. Participants linked their experiences of loneliness to the lack of social support in the postpartum period. This study offers a novel insight into Irish fathers’ experiences with maternity care during the COVID-19 pandemic. This study is the first to qualitatively explore paternal postpartum loneliness and provides a good foundation for future research and intervention in this area. Findings suggest that it would be wise to promote social support from other experienced fathers, friends, family, and from partners to reduce paternal postpartum loneliness.
The peripartum period, defined as the period from pregnancy (prepartum) to 1 year post birth (postpartum), is a joyful time for many parents (Salonen et al., 2010). It is a period of transition for parents, marked by changes in relationships and family dynamics, as well as increased stressors such as those associated with infant care and balancing responsibilities.
Although research has examined maternal social support and loneliness during the postpartum period, fathers’ experiences have received less attention, particularly within an Irish context. Changes in social perceptions around gender roles have led to increased recognition of the need to support fathers during the postpartum period in the Republic of Ireland. While Irish fathers have traditionally been viewed as providers with limited engagement in child care, there is now societal consensus that fathers should have greater involvement with child care and household responsibilities (Ralph, 2016). However, fathers’ involvement in child care varies across different household structures and socio-economic groups, with fathers from single income households often being less involved in child care (Ralph, 2016). This indicates that current policies and support systems within The Republic of Ireland may not address the needs of Irish fathers. At present, there remains a significant gap in the support available for Irish fathers as existing services are generally oriented toward mothers (Connolly & Devaney, 2018).
Few studies have explored fathers’ experiences with social support, while, to the best of our knowledge, no study has focused specifically on fathers’ experiences of postpartum loneliness. With rates of maternal loneliness increasing as a result of the COVID-19 pandemic (Dib et al., 2020; Farewell et al., 2020; Kent-Marvick et al., 2021), compared to rates of 32% to 42% before the pandemic (Kent-Marvick et al., 2021), it is likely that fathers have also experienced increases in loneliness during this time.
Postpartum social support may include informal support (from partners, family members and friends) and formal support (from health care professionals, and support groups) aimed at helping parents navigate the challenges which occur during the postpartum period. Formal support offered to fathers during the postpartum period may include informational/emotional support provided by health care professionals such as midwives (Leahy-Warren et al., 2023). Educational workshops and antenatal classes are another source of formal support which offer information on child care, parenthood, and the emotional aspects of fatherhood (J. Y. Lee et al., 2018). Fatherhood support groups provide an avenue for fathers to share experiences, offer advice and provide mutual support related to parenting and fatherhood (Nash, 2018a, 2018b; Wells et al., 2021).
Fathers may have limited access to support during the postpartum period. Even without considering the additional stress of the COVID-19 pandemic, the peripartum period brings about significant life transitions for both mothers and fathers, which can disrupt previously fulfilling relationships (Heinrich & Gullone, 2006). Like mothers, fathers experience disruptions and changes in their relationships during this time (Darwin et al., 2017; Keizer et al., 2010; Parfitt & Ayers, 2014). Social isolation and exclusion have many causes in the peripartum period; for instance, fathers feel excluded by health professionals (Entsieh & Hallström, 2016; Fletcher et al., 2006; Gervais et al., 2016; Smyth et al., 2015; Steen et al., 2012). Fathers may also be reluctant to seek support due to the stigma associated with violating “traditional masculine gender norms” (Rominov et al., 2018).
Issues with accessing social support before the COVID-19 pandemic are likely to have been exacerbated during it. Practicing social distancing during COVID-19 has been of particular importance for pregnant women, considered a vulnerable group. In many Irish maternity hospitals, partners were prohibited from attending peripartum appointments (e.g., check-ups & scans) alongside their partner, and policies of restricted visitation in hospital wards and neonatal intensive care units (e.g., only one selected person permitted to visit) were introduced (Renfrew et al., 2020; Smith et al., 2021). Parent education classes, which connect parents socially, were postponed and offered online (Sheil & McAuliffe, 2021).
Many women were alone during the early stages of labor while fathers waited in hospital car parks (Panda et al., 2021). Although the pandemic resulted in a number of restrictions across the population, these experiences may have been particularly difficult for new parents, given the heightened needs for social support during the peripartum period. Moltrecht et al. (2022) qualitatively explored parents’ experiences during the COVID-19 pandemic. Parents experienced COVID-19-related stressors, including feelings of distress and uncertainty surrounding the pandemic (Moltrecht et al., 2022). Parents felt that their peripartum care was disrupted by the pandemic, and they described feeling alone both at home and during antenatal appointments. Parents highlighted the absence of support as a major area of concern (Moltrecht et al., 2022). Fathers felt excluded from maternity care, and they lacked information about their partner’s pregnancy (Moltrecht et al., 2022).
Loneliness occurs when an individual’s social network or relationships are less satisfying than desired (Peplau & Perlman, 1979). Given the changes which occur during the peripartum period, and the additional challenges introduced by social distancing, fathers may be vulnerable to experiencing situational loneliness during this time. Situational loneliness refers to loneliness experienced by individuals who previously had satisfying relationships but are now confronted with a specific crisis/life transition (e.g., the arrival of an infant/social distancing measures) that disrupts these relationships (Heinrich & Gullone, 2006). While more is known about risk factors for peripartum loneliness among mothers (e.g., age, metal health issues, poor relationship quality, poor marital satisfaction; Geller 2004; K. Lee et al., 2019), some studies provide information about risk factors which place fathers at risk of developing loneliness. Recently married fathers may experience increased loneliness due to the shift in focus to the new family unit, resulting in isolation from family and friends (Keizer et al., 2010). Mental health issues also play a role, as stress (Kent-Marvick et al., 2021), depressive symptoms, and social phobia (Johansson et al., 2020; Junttila et al., 2015) have been associated with paternal peripartum loneliness. Mental health issues can affect the couple relationship, potentially leading to feelings of loneliness (Johansson et al., 2020). In a qualitative study exploring maternal depression, fathers expressed feeling lonely as they did not have another adult to talk to (Valdez & Martinez, 2019). In this study, fathers felt lonely as they could not speak with extended family, friends, or work colleagues (due to stigma around mental health and help seeking) and while their children were aware of their mothers’ depression, fathers felt it was inappropriate to seek emotional support from their children. For other fathers in this study, loneliness resulted from not knowing whether their attempts to support their partner were working. Research indicates that a lack of peer support, from other fathers may be a risk factor for paternal postpartum loneliness, as these fatherhood support groups facilitate social connection and reduce feelings of loneliness (Wells et al., 2021).
Very little research has examined the trajectory of loneliness during the COVID-19 pandemic in peripartum populations. Research which has examined peripartum loneliness indicated the prevalence of maternal loneliness increased during the pandemic, with rates ranging between 40% and 59% (Dib et al., 2020; Farewell et al., 2020; Kent-Marvick et al., 2021), compared with rates between 32% and 42% prepandemic (Kent-Marvick et al., 2021). No research had explored fathers’ loneliness during the COVID-19 pandemic at the time of the study. Further research is required to explore fathers’ loneliness, particularly in the context of the COVID-19 pandemic and its impact upon social relationships. As such, the aim of this study was to explore the experiences of loneliness and social support among fathers during the postpartum period, which coincided for them with the COVID-19 pandemic and related restrictions.
Method
Study Design
The study used a qualitative research design. Data were collected between April 2021 and July 2022. Some interviews were conducted when COVID-19 public health measures were in effect, and some were conducted afterwards following the ease of restrictions in The Republic of Ireland (January/February 2022). This may have influenced the results of this study. Fathers’ experiences with social support and loneliness may have differed depending on the level of COVID-19 social distancing measures in place at the time of interview. During periods of restriction, limited in-person interactions may have exacerbated fathers’ feelings of loneliness. As restrictions eased, fathers likely had increased access to in-person support, potentially leading to lower levels of loneliness and improved perceptions of support.
Interview data were collected and analyzed according to constructivist ground theory guidelines outlined by Charmaz (2006). Such an approach is suitable when researchers are aiming to understand how individuals react and cope in a challenging context. In line with constructivist grounded theory guidelines, initial codes were generated. This involved coding line-by-line segments of data. Next, focused coding was conducted. This involved evaluating and using the most significant/frequent codes which provided the most accurate categorization of the data. Next, axial coding was conducted which involved comparing codes to one another and reassembling codes to develop categories. Finally, categories were finalized to arrive at a grounded theory of “support for the supporter” and a thematic map was created to provide a visual overview of themes. Results are reported using the COREQ guidelines (Tong et al., 2007). In line with COREQ guidelines, when reporting results, the study presented participant quotes to support themes, ensured intercoder reliability for data consistency and outlined both major and minor themes which emerged from the data.
Participants
This study used convenience and snowball sampling. Participants were recruited from a larger mixed-methods study which examined paternal peripartum mental health. Participants completed an online questionnaire. At the end of this questionnaire, participants were asked whether they would like to engage in a one-on-one interview with the researcher, with the option to select “yes” or “no.” The researcher contacted those who selected yes to participate in the interview. Information about this study was shared on the researcher’s social media accounts, on the study website, and with online fatherhood discussion groups, such as Reddit. Information was shared with antenatal clinics in The Republic of Ireland, advocacy organizations such as The Blue Skies Initiative and Children and Young People Services Committees (CYPSC) and support groups via email such as From Lads to Dads. Posters outlining the nature of the study were placed within the mental health outpatient department at a large maternity hospital in The Republic of Ireland. Inclusion criteria were fathers over the age of 18, who had an infant 6 months old or younger. Both first-time and experienced fathers were recruited. Exclusion criteria were individuals with diminished ability to provide informed consent (by self-report), fathers who were under the age of 18, and fathers living outside of the Republic of Ireland.
Malterud’s informational power approach to sample size estimation in qualitative research was used to guide recruitment (Malterud et al., 2016). The study aimed to recruit 10 to 15 participants. Twelve fathers participated in this study (see Table 1). Before commencing, the study received ethics approval from Maynooth University research ethics committee (study approval reference—2424266) as well as The Rotunda Hospital Research Ethics Committee to recruit participants via the mental health outpatient’s department (study approval reference—REC-2020-016). All participants provided verbal informed consent to participate in the study prior to interview. Informed consent was recorded using a Dictaphone.
Sample Characteristics of (n = 12 Fathers With a Child Aged 6 Months or Younger).
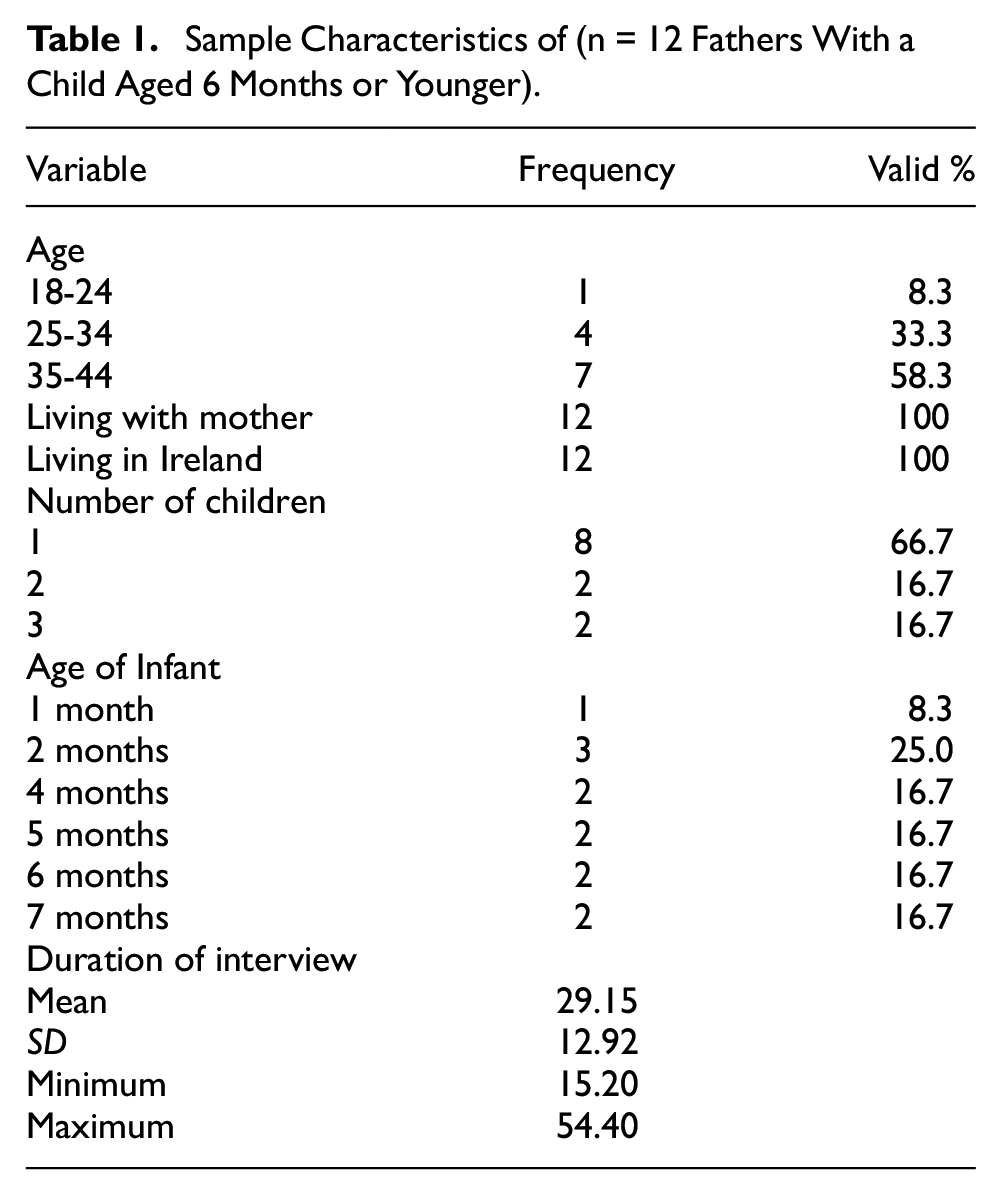
Demographic information for the sample (n = 12) is presented (Table 1). The majority of participants were between 35 and 44 years old (58.3%; n = 7), had 1 child (66.7%; n = 8) and had an infant aged 2 months (25.0%; n = 3) at the time of interview. All participants were living in The Republic of Ireland at the time of the interview. All participants were living with the mother of their child at the time of interview.
Data Collection
One-to-one semistructured interviews were conducted to assess fathers’ experiences with social support and loneliness during the peripartum period. An interview schedule was used to guide the researcher during the interview process. The schedule was developed following guidelines (Charmaz, 2006) and refined during an initial pilot phase (see Supplemental Appendix A). As is advised in constructivist grounded theory, the interview schedule was dynamic and changed with each subsequent interview if the research team felt that questions were either missing, redundant, or needed refinement. During each interview, participants were asked open-ended questions. Participants were asked to speak about their experiences with postpartum stressors/challenges, for example, “What new challenges emerged for you during the postpartum period?,” “What have you felt that you need support with during this time?” Participants were asked to speak about their experiences with postpartum social support, for example, “Who did you receive support from to help you with new challenges during the postpartum period?” Finally, participants were asked to speak about their experiences with postpartum loneliness, for example, “What do you think may have contributed to your increased feeling of loneliness during this time?”
As this study used a constructivist grounded theory approach, data collection and analysis occurred concurrently. In line with the constant comparative method (Glaser, 1965), data were compared and categorized consecutively. Further data collection was shaped by what had been previously analyzed. Probing questions were also used to encourage participants to expand their answers.
Interviews were conducted and transcribed by one member of the research team (an early career researcher SMC), who had no previous relationship with participants. The early career researcher was also involved in data analysis. The early career researcher was a (female) Psychology graduate and postgraduate student. Authors AM and JMcHP (both female) have experience conducting qualitative research using interviews and provided training for the early career researcher prior to the interviews, and JMcHP was also involved in data analysis.
Interviews were conducted by phone (due to COVID-19 social distancing measures and for health and safety considerations) and were recorded using an offline Dictaphone. Audio recordings were transcribed verbatim following each interview, and transcripts were pseudonymised using Microsoft word. Interviews ranged in duration from 15 to 56 minutes.
Data Analysis
Interview transcripts were read and reread in full, following each interview, during the coding process by both SMC and JMcHP to increase familiarity with the data. The coding process was conducted collaboratively by both researchers to ensure intercoder reliability. Interview data were analyzed according to constructivist ground theory guidelines outlined by Charmaz (2006). First, initial codes were generated. This involved coding line-by-line segments of data (See Supplemental Appendix B for an example of codes applied to short segments of data). Next, focused coding was conducted. This involved evaluating and using the most significant/frequent codes which provided the most accurate categorization of the data. Next, axial coding was conducted which involved comparing codes to one another and reassembling codes to develop categories. Finally, categories were finalized to arrive at a grounded theory, to be described using a thematic map (Figure 1). The researchers met regularly to discuss their interpretations of the data, codes, and emerging themes. These meetings occurred bi-weekly over the course of the data analysis phase.
Thematic Map.
Results
The mean duration of interviews was 29.15 minutes. The interviews ranged in duration from 15.20 to 54.40 minutes.
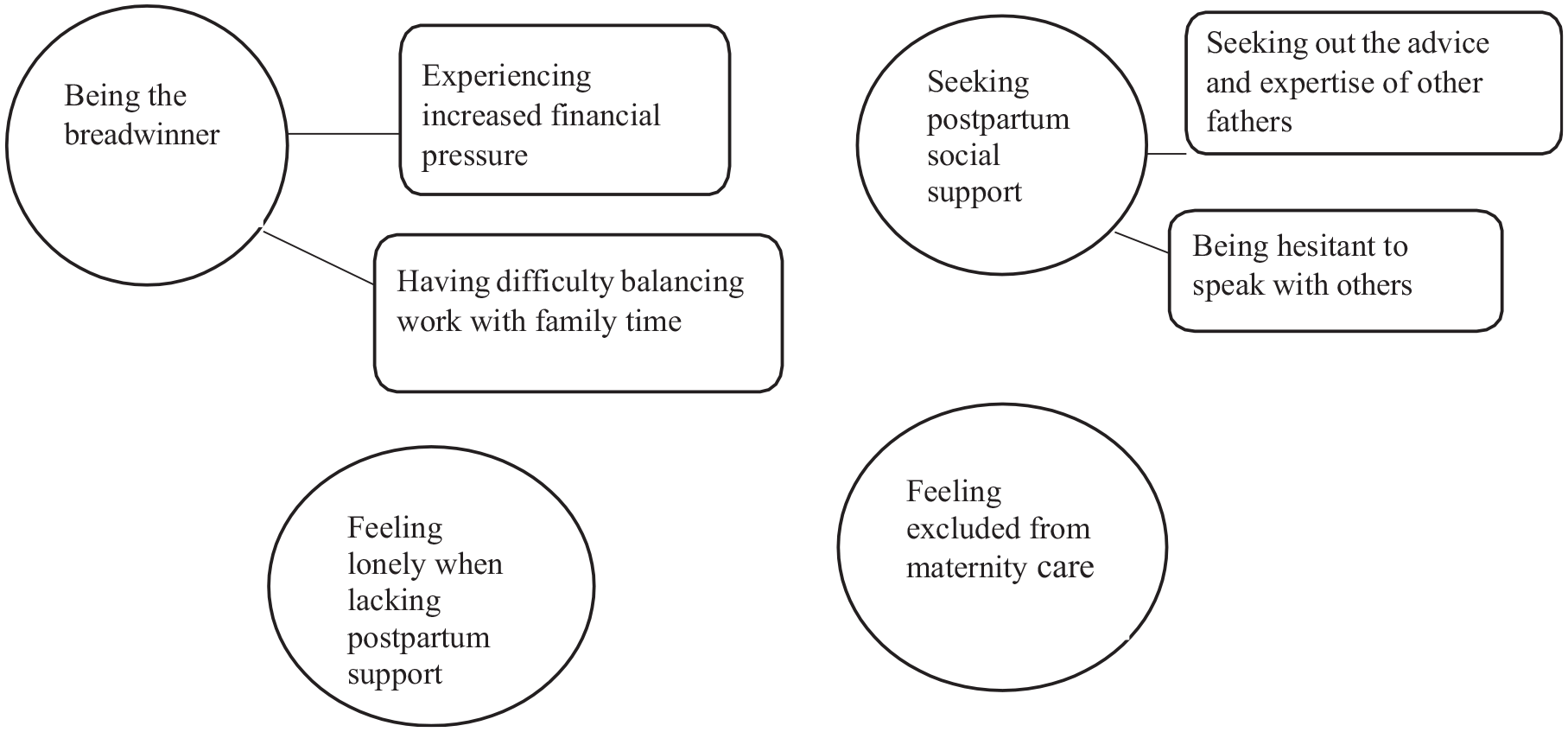
A grounded theory is presented, entitled “support for the supporter” (see Figure 1). During the analysis of the interview transcripts, four key themes emerged from the data, which fell under the broader grounded theory title: (a) being the breadwinner, (b) seeking postpartum social support, (c) feeling excluded from maternity care, and (d) feeling lonely when lacking postpartum support (See Table 2 for a full description of themes and subthemes with sample quotations).
Presentation of Themes, Subthemes, and Sample Quotations From n = 12 Interviews.

Theme 1: Being the Breadwinner
Participants discussed experiencing increased financial pressure during the postpartum period. Many participants spoke about their perceived responsibility to provide for their families during this time and how this was the most challenging aspect of the postpartum period: And of course, when you have a baby, you have to make ends meet, and look after everyone at home. So, for me, that has been the main responsibility or the challenging part of it. (p6)
One participant felt their partner did not have the same financial concerns as they did during the postpartum period. This participant felt hesitant to share their financial concerns with their partner: The financial pressure, I need to talk with my partner about . . . not to control spending but to talk about that as a couple and say you know look we need to hold back a bit here. The concerns that I have, maybe she doesn’t see as much. (p8).
Participants spoke about having difficulty balancing work with family time during the postpartum period. Participants expressed how it was challenging to fulfill the role of “the breadwinner” and father: Yeah that’s the one that comes to mind I’d say at the moment, especially with my wife. She’s off work at the moment and that’s probably the biggest one at the moment, being the breadwinner . . . and, being a father at the same time, you know? (p8)
Some participants felt that balancing work with child care was “tiring” and “tough.” Participants found it difficult to allocate enough time to both work and child care: It can be hard to give time, so I feel like sometimes it can be hard to give time to everything equally or where you want it and then personally, I suppose I just feel stressed a little bit. (p8)
Participants wanted to be more available at home to spend time bonding with their infant and wanted to be more available to support their partner with child care. Participants valued having flexibility with work so they could spend more time with their infant. One participant discussed using holidays to extend their paternity leave: I’ve had to use some of my own holidays to take time off, to be there for my children and their mother you know. Even though there’s a good allowance for time off, it’s still not as much as I would like. (p9)
Theme 2: Receiving and Seeking Social Support
Many participants discussed seeking out the advice and expertise of other fathers during the postpartum period. Participants described how other fathers reached out to them and offered support during this time. Some participants actively searched for and used online or text-based fatherhood discussion groups or connected with others by phone during periods of COVID-19 isolation.
Participants discussed how they shared advice, exchanged stories, photographs, and shared their frustrations with other fathers both online and in-person. Participants valued speaking with individuals in a similar situation and discussed the normalizing effect that this form of support had for them: It helps to see that you’re not the only one struggling with things a bit or thinking about things in a certain way, it’s completely normal. (p1)
Although many participants sought the advice of other fathers, some participants discussed feeling hesitant to speak with others about their feelings with others, particularly with other men. This seemed to emerge from perceptions surrounding the masculine norm of men not discussing feelings with one another. Participants described speaking indirectly about their feelings. One participant discussed how they tried to “soldier on” and “keep things going” rather than discuss their feelings during this time: I suppose the typical Irish male thing you soldier on until past the point where you should have done…there were certainly some days in the early weeks where I was running on fumes if you know what I mean, trying to do too much, trying to keep things going until eventually my partner said, basically said go upstairs and go into the spare room and turn the lock in the door and sleep until you wake up but look again that was more or less trying to burn the candle at both ends. (p12)
Theme 3: Feeling Excluded From Maternity Care
Participants described feeling excluded from maternity care during COVID-19. A number of participants discussed advocating for fathers to be included in maternity care, although ultimately felt like they could not do anything to change their circumstances. Participants lacked information about and were not involved in discussions regarding pregnancy, birth, or infant care. This exclusion was paired with concerns about the well-being of their partner and infant. Participants described feeling frustrated, angry, and upset about being excluded from maternity care: The worry and everything there was no need for it. I am sitting outside waiting in the car park while my partner is alone in the room. It is sickening how fathers don’t have rights in this . . . It breaks my heart. (p7)
Participants described feeling frustrated as Irish maternity hospitals had different policies in place for fathers, and they were unsure about attending the birth: The most frustrating part was the continued unknown as to whether or where I would be allowed in for the birth. Some maternity hospitals opened up but then down here it was totally different. In certain hospitals, you were allowed in for as long as you want afterwards but in others you were only allowed in for two hours a day. (p3)
When participants did attend peripartum appointments, some described feeling uninvolved or feeling like a “secondary caregiver”: I’m just sort of standing in the background like I’m not getting questions about the child or anything like that their patient is the mother and child and I’m just sort of like, a supporting character in it or not the secondary caregiver, that sounds very cold, but ultimately they don’t have an interest in my wellbeing. (p11)
Participants discussed how COVID-19 restrictions have highlighted a disparity in care for fathers and expressed how they lacked resources and avenues for information within the Irish health care system: I didn’t even realise that this was an issue. I honestly didn’t. I realised that this actually is an issue, and you know for example you have your six-week check-up and that goes through the baby’s health and also the mother’s health and mental health such as postnatal depression. There actually isn’t an avenue for fathers for that. So where do you have a conversation about this? (p3)
Theme 4: Feeling Lonely When Lacking Support
Participants discussed feeling lonely during the postpartum period, in the absence of or when lacking social support. Many participants were isolated from family and friends during COVID-19 restrictions and for some participants this resulted in feelings of loneliness.
A lack of partner support contributed to feelings of loneliness during the postpartum period. One father discussed how they experienced a decline in partner support, closeness, and intimacy during this time and how this contributed to loneliness: There’s not the same level of closeness or anything . . . I do probably feel the most sort of lonely or kind of out on my own that I have in years, you know what I mean? . . . your relationship with your partner changes, and her focus is on something else. So what used to be a very reliable source of support that you had, not that it’s not reliable anymore. (p9)
Participants discussed the role that social support played in relation to reducing or preventing feelings of loneliness during the postpartum period. Those who stayed in touch with friends and family throughout COVID-19 restrictions felt less lonely. Having a good support structure in place, meeting with family and friends and engaging with social outlets was preventive of postpartum loneliness: . . . No to be honest, because we’ve had, we knew had this great support structure in place with our families, our friends, and our neighbours who we love by the way, so we have a really good relationship with them. (p1).
Partner support and communication seemed to play an important role in reducing/ preventing participant’s feelings of loneliness. Despite being isolated from family and friends, participants did not feel lonely as they received support from their partner: I’m very lucky that my wife and I have lived together for years . . . we’re a newly married couple and we still have things that we like to talk about you know, we enjoy each other’s company hahaha. So, loneliness is not something that I have ever struggled with because we’re quite good communicators. (p10)
Discussion
A grounded theory entitled “supporting the supporter” is presented, which explains fathers’ experiences of postpartum loneliness and social support in the context of the COVID-19 pandemic. The theory emphasizes the need for identifying social support requirements for fathers during this time. The qualitative theme “Being the breadwinner” provides an insight into the sources of stress or challenges fathers experienced during the peripartum period—“Experiencing increased financial pressure” and “Having difficulty balancing work with family time.” The subtheme “Experiencing increased financial pressure” is consistent with research suggesting financial pressure is a common source of paternal peripartum stress (Seah & Morawska, 2016; Yu et al., 2011). Philpott et al. (2017) investigated the prevalence of paternal postpartum depression in Ireland and its associated factors. Fathers who were struggling financially had a greater risk of postpartum depression than those who were financially secure.
In this study, fathers perceived themselves as “breadwinners” or aligned themselves with this role. In a review of 30 studies Valiquette-Tessier et al. (2019) reported fathers were stereotyped as financial providers or primary breadwinners for the family across all racial and ethnic groups. If a father’s perception of a “good father” is to be a provider, peripartum stress may be worsened (Darwin et al., 2017), and fathers may experience depressed mood (Chhabra et al., 2022; Morse et al., 2000).
The subtheme “Having difficulty balancing work with family time” highlights the challenge of balancing the role of “breadwinner” with the role of fatherhood. Participants felt balancing work with child care was “tiring” and “tough.” Participants wanted to be more available at home to spend time with their infant and help with child care. As fathers have responsibilities to fulfill both within the home and within the workplace, work-family conflict may arise due to the incompatibility of the roles (Huffman et al., 2014). Although mothers and fathers report having similar levels of work-family conflict (Young & Schieman, 2018), much of the research to date has focused on work–family conflict among mothers. There is a need for increased research focusing on fathers’ experiences with work-family conflict. Fathers in this study valued having flexibility with work so they could spend more time with their infant, which highlights the importance of flexibility within the workplace for fathers during the peripartum period. Work–family conflict has been associated with paternal peripartum anxiety and depression (Koh et al., 2014, 2015).
The theme “Being the breadwinner” may be explained by parenting schemas. Parenting schemas refer to beliefs about the parenting role, how to behave in that role, beliefs about children in general (e.g., how children should develop) and beliefs about one’s own child (Azar et al., 2005). Fathers may hold inflexible schemas about how they should behave within the family unit or fatherhood role, for example, holding a “breadwinner” schema, believing that a father should be a provider. Schemas can change when an individual is faced with new information or variations to their core beliefs (Azar et al., 2005). It is therefore essential that fathers are provided with enough information and support surrounding fatherhood to promote the development of new fatherhood schemas which are more flexible and adaptive.
The theme “Seeking postpartum social support” provides information about the support that participants sought during the postpartum period. The subtheme “Seeking the advice and expertise of other fathers” describes how participants sought and valued the support of other experienced fathers. Participants discussed the normalizing effect this support had for them. The benefits of speaking with other fathers has been identified in previous research. In Carlson et al. (2014) and Shorey et al.’s (2017) studies, fathers recommended groups with other fathers to learn from and support one another as they were going through the same experiences. In Wells et al.’s (2021) study, fathers felt fatherhood support groups positively benefited their relationship with their family, enhanced their self-confidence, improved their family equality and decreased loneliness. The benefits of using online fatherhood forums has also been noted in previous research (White et al., 2018).
Despite seeking the support of other experienced fathers, some participants felt hesitant to speak with others about their feelings, particularly with other men. This hesitation appeared to emerge from perceptions surrounding the masculine norm of men being nonemotional or not discussing feelings with one another. Previous research suggests fathers are reluctant to speak about their mental health and are influenced by “perceived expectations of masculinity” (Darwin et al., 2017) or “traditional masculine gender norms” (Rominov et al., 2018). The violation of these “expectations” or “norms” may lead to negative appraisal from others, making fathers reluctant to speak about their feelings or seek help (Rominov et al., 2018). Further research into seeking support and adherence to masculine norms is necessary to reduce the stigma surrounding men’s mental health, particularly within an Irish context as participants felt this was common among Irish men. A potential way to reduce hesitancy to seek support, may be offering fatherhood support groups in relaxed or informal settings such as pubs, cafes, sport centers, or community centers. These community settings often serve as hubs which facilitate connection. They are familiar spaces, where fathers could connect with one another share experiences, and advice in a less formal environment. Nash (2018a, 2018b), reported fathers were less favorable toward male-based group discussions in health settings and toward groups which focused on sharing feelings. Fathers were hesitant to engage in activities that suggested femininity/weakness, feeling more comfortable in relaxed, environments such as pubs or using peer-support phone lines (Nash, 2018a, 2018b). Fathers felt more comfortable when groups focused on “facts” related to pregnancy/birth (Dolan et al., 2011; Nash, 2018a).
The theme “Feeling excluded from maternity and infant care” highlights the challenges that participants experienced when excluded from maternity care during COVID-19. Participants lacked information about and were excluded from discussions about pregnancy, birth, or infant care. Similarly a study conducted in 2022 indicated that fathers felt excluded from maternity care and lacked information about their partner’s pregnancy during COVID-19 (Moltrecht et al., 2022). When participants did attend peripartum appointments, some described feeling uninvolved or feeling like a “secondary caregiver.” In line with this, research has reported fathers felt ignored and side-lined in maternity settings and reported being treated like “a visitor” (Hodgson et al., 2021). Participants also described feeling frustrated, angry, and upset. Participants described their efforts to advocate for fathers to be included in maternity care, although ultimately felt like they could not do anything to change their circumstances. Participants discussed how COVID-19 restrictions have highlighted a disparity in care for fathers and expressed how they lacked resources and avenues for information within the Irish health care system. This finding offers a novel insight into Irish fathers’ experiences with maternity care during the COVID-19 pandemic.
“Feeling lonely when lacking postpartum support” provides an insight into the sources of support that prevented or alleviated paternal loneliness. To our knowledge, this is the first study to suggest that a lack of support from partners, friends, and from family may contribute to paternal postpartum loneliness. As well as feeling lonely for this reason, participants felt lonely because they were isolated from friends and family during COVID-19. Similarly, although in a pre-COVID-19 context, previous research indicated that reduced social contact is associated with postpartum loneliness in mothers (K. Lee et al., 2019).
Despite being isolated from family and friends, many participants in this study did not feel lonely as they received support from their partner. In line with previous research (Junttila et al., 2015), a decline in relationship satisfaction and intimacy seemed to result in feelings of loneliness. In terms of changes in relationship intimacy during the postpartum period, previous research reported that fathers may experience feelings of distance, a loss of closeness (Darwin et al., 2017) and changes in the sexual relationship (Parfitt & Ayers, 2014). Findings in this study contribute to previous literature finding such relationship changes contributed to fathers’ loneliness during the postpartum period. One participant attributed his feelings of loneliness to a loss of previous closeness, intimacy, and a shift in his partners focus from the relationship to the new infant. In addition, another participant discussed how they have not felt lonely as they enjoyed their partner’s company and conversations throughout the postpartum period. This theme offers a novel insight into how aspects of the partner relationship, can affect fathers’ well-being and contribute to loneliness during the postpartum period.
Strengths and Limitations
Rather than focusing on mothers’ experiences during the postpartum period, a unique strength of this study was highlighting fathers’ experiences. Paternal mental health is uniquely associated with infant well-being and development (Fisher et al., 2021) although fathers tend to be under-recognized with respect to peripartum mental health issues. This study contributes to a growing body of research suggesting paternal peripartum well-being is an important issue among new fathers.
It is important to note that interviews were conducted both during the implementation of COVID-19 public health measures and following the ease of restrictions in The Republic of Ireland (January/February 2022). This may have influenced the results of this study, particularly in relation to experiences with social support and loneliness. While similarities were evident between these interviews, it’s important to recognize that differences also existed among them.
Regarding similarities between the interviews, both groups (those who completed interviews during the implementation of COVID-19 public health measures and those who completed interviews during the easing of restrictions) expressed feeling excluded from maternity care. Both groups discussed experiencing limitations on attending appointments and scans as well as feeling uninvolved in peripartum appointments. In addition, both groups discussed having reduced social contact with extended family and friends due to COVID-19. Fathers interviewed during the implementation of restrictions were unable to socialize with family and friends in person, while some fathers who were interviewed during the ease of restrictions, chose to continue social distancing to protect their infant’s health.
In terms of differences between the groups, some fathers interviewed during the ease of restrictions reported participating in more in-person social activities compared to fathers interviewed during enforced social distancing. In addition, it is important to note that fathers interviewed during the implementation of Covid-19 restrictions reported feeling lonelier more so than those interviewed during periods of eased restriction, and this was attributed to having a lack of available in-person support from family and friends.
Overall, fathers interviewed during restrictions expressed greater loneliness than fathers interviewed during the ease of restrictions, and they received less in-person support. Social support played a key role in preventing/reducing loneliness, both during times of restriction and afterwards.
The sample within this study consisted of fathers who were living in the Republic of Ireland and who were living with the mother of their child. In addition, the majority of the sample were aged 35 to 44 and were first-time parents. This may limit the generalization of findings to more diverse groups. Future research would benefit from using a more diverse sample. In addition, future research may benefit from collecting further demographic information from participants. This study focused on social support and loneliness among fathers who had an infant 6 months old or younger. This may limit the generalization of findings to other time points during the peripartum period. Future research could explore social support and loneliness at different time points during the peripartum period, for example, up to 12 months postpartum. While this study employed a constructivist grounded theory research design with two raters, it is feasible that other researchers may have approached the data with alternative analytical frameworks leading to the identification of different themes. The themes which emerged in this study should be considered as one possible interpretation of the data.
Implications for Future Research
Findings in this study have important theoretical implications. Future research could explore how to change schemas related to the fatherhood role, for example, how providing information and support to fathers might promote the development of more adaptive schemas about fatherhood. This study was the first to qualitatively explore paternal postpartum social support and loneliness and provides a good foundation for future research. At present, there remain many unanswered questions about fathers’ peripartum loneliness. For example, how does loneliness differ between fathers from different sociodemographic groups. What are the risk factors associated with paternal loneliness? What are the psychosocial consequences of loneliness for fathers, the infant and the family? Further quantitative and qualitative research is required to answer these questions. More research is also required to examine the experiences of fathers regarding their postpartum social support needs, the ideal timing of postpartum support, barriers to receiving support and how support/support interventions might reduce postpartum loneliness.
Clinical Implications
Findings highlight the need for fathers to have a role not only within the workplace but also within the home and with child care. Modern fathers are encouraged to engage with child care; however, inflexible workplace policies may make it difficult for fathers to be involved at home. Government or workplace policies may facilitate fathers’ involvement with child care and lessen financial burden during this time.
Findings regarding fathers’ feelings of exclusion during the COVID-19 pandemic in Irish health care settings, have long-term implications which extend beyond the pandemic. Findings highlight the need for ongoing improvements in Irish maternity care. Postpandemic maternity care should be focused on establishing environments which are supportive and inclusive of both mothers and fathers during the peripartum period. Findings can inform health care practitioners of modifiable factors which may prevent or alleviate loneliness during the postpartum period. Interventions to target low partner support, and low support from friends/family during the postpartum period may be helpful in preventing/alleviating postpartum loneliness. By focusing on paternal social support and aspects of the partner relationship such as communication, intimacy and closeness, interventions can foster more supportive family environments. In addition, fathers require avenues to access information and have discussions about peripartum care. Developing social support interventions designed specifically for fathers, aimed at sharing information around pregnancy/birth, and facilitating discussions around fatherhood may improve well-being and reduce feelings of loneliness. Fathers discussed the normalizing effect such discussions had for them, highlighting the benefits of creating spaces where fathers can share their experiences with peers. However, some fathers were hesitant to seek support from others, particularly from other fathers. Previous research suggests a potential way to reduce this hesitancy is to offer fatherhood support groups in relaxed environments, with a focus on facts related to pregnancy/birth (Nash, 2018a, 2018b). Offering support groups in relaxed, informal settings such as pubs, cafes, sport centers or community centers may provide fathers with a space to connect and learn about pregnancy, birth and fatherhood in a relaxing, less formal environment.
If parents are isolated or cannot be physically present to engage with others, connecting via technology e.g., (web-based platforms) may offer a way to form connections. This may apply to contexts outside of COVID-19 if parents are isolated for another reason. Although communicating online cannot always replace face-to-face contact, it is clearly beneficial in times of isolation or crisis and can act as a temporary substitute for face-to-face support. Some fathers may also prefer seeking support online. For example (Ammari, & Schoenebeck, 2015) suggest fathers may prefer seeking support in anonymous online settings as they can do so without the judgment and stigma that is often experienced in offline contexts.
Conclusion
This study was the first to qualitatively explore paternal postpartum social support and loneliness and provides a good foundation for future research. This study contributes to a growing body of research suggesting paternal peripartum well-being is an important consideration for those who identify as fathers. Further research that targets interventions to address the unique challenges and needs of fathers during the postpartum period is warranted. To reduce financial pressure and work-family conflict, there is a need for increased support for fathers in relation to policy and within the workplace following the arrival of their infant. Most importantly, findings signpost the importance of targeting low partner support, low support from family, friends and from other fathers as potentially modifiable factors for postpartum loneliness interventions. Findings offer a unique insight into how aspects of the partner relationship, including communication, closeness, and intimacy, play an important role in fathers’ feelings of postpartum loneliness.
Supplemental Material
sj-docx-1-jmh-10.1177_15579883241249921 – Supplemental material for Support for the Supporter: Paternal Postpartum Loneliness and Social Support During the COVID-19 Pandemic
Supplemental material, sj-docx-1-jmh-10.1177_15579883241249921 for Support for the Supporter: Paternal Postpartum Loneliness and Social Support During the COVID-19 Pandemic by Sarah Murray Cunningham, Joanna McHugh Power, Philip Hyland and Anne-Marie Casey in American Journal of Men's Health
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
The participants of this study did not give written consent for their data to be shared publicly so due to the sensitive nature of the research, supporting data are not available.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.