
Abstract
Dyslipidemia is linked to various health complications, including cardiovascular disease and inflammation. This study aimed to assess the association between smoking and lipid profile in the Tabari cohort population. Data from the Tabari Cohort Study involving 4,149 men were analyzed. A standardized questionnaire collected smoking history, while blood samples measured lipid levels and anthropometric measurements were recorded. Statistical analysis utilized chi-square tests and logistic regression, adjusting for potential confounders. The prevalence of smoking was 893 (21.52%; urban: 20.6%, mountainous: 23.8%, significant level: .024). The adjusted odds ratio (OR) of low high-density lipoprotein (HDL) among smokers 1.48 (95% confidence interval [CI]: 1.25–1.77, p < .001) was the same as non-smokers. The adjusted OR of high low-density lipoprotein (LDL) in men with 1 to 10, 11 to 20, and more than 20 cigarettes per day was 0.95 (95% CI: 0.73–1.25), 1.30 (95% CI: 0.99–1.71), and 2.64 (95% CI: 1.32–5.27) and low HDL was equal to 1.34 (95% CI: 1.06–1.68), 1.61 (95% CI: 1.26–2.05), and 2.24 (95% CI: 1.13–4.42) compared with non-smokers, respectively. The study findings indicate that smoking is associated with lower HDL levels, even after adjusting for potential confounders. The odds of low HDL and high LDL increases with higher smoking intensity. The low HDL and high LDL levels in individuals smoking over 20 cigarettes/day, respectively, show a 2.24-fold and a 2.64-fold increased odds compared to non-smokers. These findings highlight the importance of smoking cessation in relation to lipid profiles and related health risks.
Introduction
The human serum contains a variety of lipid subclasses that can exert diverse impacts on the individual’s physiological state. The maintenance of optimal levels of each subclass is crucial for the promotion and preservation of overall health and well-being (Ambroży et al., 2022).
The presence of dyslipidemia in the male population can heighten the susceptibility to a range of health complications, such as cardiovascular disease, metabolic syndrome, and atherosclerosis (Ambroży et al., 2022; Grandys et al., 2021; Ostovar et al., 2017; Parikh et al., 2022).
Elevated levels of triglycerides (TG) have been demonstrated to increase the likelihood of developing cardiovascular disease (Folin & Contiero, 1994). Similarly, high levels of total cholesterol (TC) have been linked to an augmented risk of cardiovascular disease (Mills & Wilkinson, 1966). On the other hand, high-density lipoprotein (HDL), commonly referred to as “good cholesterol”, has been associated with a reduced risk of cardiovascular disease (Folin & Contiero, 1994). Conversely, low-density lipoprotein (LDL), or “bad cholesterol”, has been associated with an increased risk of cardiovascular disease (Folin & Contiero, 1994). The adoption of lifestyle modifications to maintain optimal levels of these serum lipids can help mitigate the risk of developing cardiovascular disease. In certain instances, pharmacological interventions may also be necessary to manage high serum lipid levels. Ongoing monitoring of serum lipid levels through regular consultations with a health care provider can aid in the early detection and management of potential issues (Folin & Contiero, 1994; Grandys et al., 2021; Mills & Wilkinson, 1966).
In men, smoking has been associated with dyslipidemia, characterized by elevated levels of TC, TG, and LDL-cholesterol, as well as decreased levels of HDL-cholesterol. The severity of dyslipidemia has been observed to increase with the extent of smoking (Jeong, 2022). A study involving healthy middle-aged men revealed that heavy smokers exhibited significantly lower levels of serum HDL, LDL, and TC, while their TG levels were significantly higher compared to non-smokers (Wakabayashi, 2008). Several studies have indicated a potential link between smoking and aging, with a noteworthy prevalence of smoking, particularly cigarette smoking, observed among the elderly population in Iran (Huang et al., 2022; Vatankhah et al., 2020). Notably, a research has demonstrated a significant association between the prevalence of smoking, including waterpipe tobacco smoking, and age, as well as the presence of cardiovascular disease, among Iranian adults aged 35 to 70 (Moghadam et al., 2023; Zahirian Moghadam et al., 2021).
Some findings suggest that smoking can have implications in relation to aging, and that the prevalence of smoking, particularly cigarette smoking, is notable among the elderly in Iran.
It is considerable that smoking is frequently linked to other lifestyle factors that can influence serum lipid levels, which can complicate the isolation of the precise effects of smoking on these levels. Numerous studies have consistently reported an association between smoking and elevated levels of TC, TG, and LDL-cholesterol, as well as reduced levels of HDL-cholesterol, all of which are established risk factors for cardiovascular disease (Linna et al., 2008; Wakabayashi, 2008; Yamamoto et al., 2003).
However, further research is required to comprehensively elucidate the dissimilarities in the impact of smoking on serum lipid. In the present study, we aimed to determine the association between smoking and lipid profile in the male population aged 35 to 70 years old based on cohort study.
Method
Design
The present study is a cross-sectional study conducted within the data collected in the enrolment phase of the Tabari Cohort Study (TCS). TCS is a part of the Prospective Epidemiological Research Studies in Iran (PERSIAN), a national cohort study, that confirmed by the Mazandaran University of Medical Science ethical committee (IR.MAZUMS.REC.95.2524). In the first phase of TCS, which took place from June 2015 to November 2017, 10,255 individuals aged 35 to 70 years old, from two urban (Sari) and mountainous (Kiasar) regions were enrolled. Details and methods of both TCS and PERSIAN have been published in previous articles (Eghtesad et al., 2017; Kheradmand et al., 2019; Poustchi et al., 2018).
For the present study, we have utilized data of all men who have participated in TCS (4,149 individuals). In total, 2,946 individuals from the urban and 1,203 individuals from the mountainous regions were analyzed.
Data Collection
Data collection methods consist of questionnaires, anthropometric measurements, and laboratory examination. A standardized questionnaire with established reliability and validity, approved by the central team of the PERSIAN cohort, was used to collect data. The questionnaire included multiple items related to general information, socioeconomic status, employment history, physical activity, and smoking history. In this study, individuals classified as smokers were defined as those who reported a consistent smoking habit of at least one cigarette per day for a minimum duration of 1 month or those who had recently quit smoking, specifically within a month prior to their participation in the research (Moghadam et al., 2023).
After a 12-h fasting, blood samples were taken from all participants in TCS for laboratory tests. TC, TG, LDL-cholesterol, and HDL-cholesterol levels were measured using a BT 1500 analyzer (Biotecnica, Italy).
Then, trained personnel measured anthropometric indices, including waist circumference (WC) and hip circumference, according to the standard protocol (Poustchi et al., 2018).
Covariates
Selected covariates included age (categorized 35–39/40–49/50–59/60–69 years), residency (urban/mountainous), marital status (single/widow/divorced/married), social economic status (from the first quintile as poorest to the fifth quintile as richest groups), education years (no schooling/1–5/6–8/9–12 years/university or college academic degree), metabolic equivalent of task (MET; ≥median/), WC (<102/≥102), waist to hip ratio (WHR; ≤0.9/>0.9), and waist to height ratio (WHtR; <0.05/≥0.05) as previously defined (Poustchi et al., 2018).
Statistical Analysis
The following criteria were considered as normal levels of lipid profile: TC ≤ 200, TG ≤ 150, LDL-cholesterol ≤ 130, and HDL-cholesterol ≥ 40 (male) (Fulks et al., 2009; Luxia et al., 2021).
In the present study, SPSS version 26 was used for data analysis. Variables were described in terms of percentage and number. Comparison of categorical variables between the groups was performed using the chi-square test. Logistic regression analysis was used to investigate the relationship between smoking and lipid profile by adjusting the effect of variables suspected to be confounder. It should be noted that in addition to presenting the results and comparison according to current daily smoking (yes/no), analysis with the dose–response approach and p for the trend of smoking intensity and the pack-year have also been presented.
Results
In this study, 4,149 (40.45%) of the 10,255 cohort population were men aged 35 to 70 years old, all of whom were included in the study. Of the total studied population, 2,946 (71%) resided in urban areas, while 1,203 (29%) were mountain dwellers. The majority of the studied population (1,360 [32.77%]) belonged to the age group of 50 to 59.
Smoking Status According to Participants’ Demographic Variables
Among the male participants, a total of 893 (21.52%) were found to be smokers. The prevalence of the rate of smoking in the urban and mountain populations was 607 (20.6%) and 286 (23.8%), respectively (p = .027; Table 1)
Demographic and Smoking Status of Study Participants

Note. MET = metabolic equivalent of task; BMI = body mass index; WC = waist circumference; WHR = waist to hip ratio; WHtR = waist to height ratio.
Table 1 demonstrates a significant association between participants’ age and smoking prevalence. Notably, the prevalence of smoking increased with advancing age, with rates of 148 (25.3%), 317 (24.7%), 295 (21.7%), and 133 (14.4%) observed among smokers aged 35 to 39, 40 to 49, 50 to 59, and 60 to 70, respectively, compared to non-smokers in the same age groups (p < .001). In addition, a significant relationship was found between years of education and smoking behavior. The prevalence of smoking among individuals with different levels of education was as follows: 229 (17.2%), 335 (25.2%), 128 (25.4%), 161 (23.9%), and 40 (12.9%) for those with university/college degrees, 9 to 12 years of education, 6 to 8 years of education, 1 to 5 years of education, and no schooling, respectively, compared to non-smokers with the same educational backgrounds (p < .001).
Our findings also revealed positive correlation between smoking and the MET index, with rates of 404 (20.1%) and 489 (22.9%) observed among smokers below and above the median, respectively, compared to non-smokers below and above the median (p = .031).
Conversely, an inverse relationship was observed between smoking and BMI (391 [27.9%], 357 [18.8%], and 145 [17.0%] were observed for BMI categories <25, 25–29.9, and ≥30 kg/m2, respectively, compared to non-smokers in the same categories, p < .001), WC (751 [22.3%] and 142 [18.3%] were observed for smokers with WC measurements <102 and ≥102 cm, respectively, compared to non-smokers, p = .014), WHR (430 [26.5%] and 463 [18.3%] were observed among smokers with ratios ≤0.9 and >0.9, respectively, compared to non-smokers, p < .001), and WHtR (277 [32.1%] and 616 [18.8%] were observed among smokers with WHtR <0.05 and ≥0.05, respectively, compared to non-smokers, p < .001; Table 1).
Lipid Profile According to Participants’ Demographic Variables
Regarding abnormal lipid profile levels, the study identified 959 (23.1%) cases of abnormal HDL, 741 (17.9%) cases of abnormal LDL, 1,303 (31.4%) cases of abnormal TC, and 1,921 (46.3%) cases of abnormal TG among the 4,149 male individuals from the Tabari cohort.
The analysis revealed that high level of LDL, TG, and TC as well as low level of HDL were significantly different in different age group and socioeconomic status. Abnormal lipid profile levels were significantly higher in urban residents compared to other areas, with rates of 569 (19.3%), 724 (24.6%), 1,540 (52.3%), and 1,010 (34.3%) for LDL, HDL, TG, and TC, respectively (p < .001). However, no significant differences were observed in abnormal lipid profiles based on marital status. Additional demographic and clinical variables are detailed in Table 2.
Demographic and Clinical Variables of Study Participants

Note. MET = metabolic equivalent of task; BMI = body mass index; WC = waist circumference; WHR = waist to hip ratio; WHtR = waist to height ratio; LDL = low-density lipoprotein; HDL = high-density lipoprotein; TC = total cholesterol; TG = triglycerides.
There was a significant relationship between demographic variables such as age, socioeconomic status, and education level, and abnormally high levels of LDL, TG, and TC. Place of residence, MET index, BMI, WHR, and WHtR were significantly associated with abnormal levels of all four lipid profile factors (LDL, HDL, TG, and TC). However, only WC showed a significant relationship with abnormal HDL and TG. No significant relationship was found between marital status and lipid profile levels. These demographic variables were examined to determine the role of confounding factors in the study (Table 2).
Analysis of Lipid Profiles Based on Smoking Status
Among total men participated in TCS, 893 individuals (21.52%) were smokers. Among the smokers, 27.8% (248 individuals) had abnormal HDL levels, while among non-smokers, 21.8% (711 individuals) had abnormal HDL levels (p = .000). As Table 3 shows, TC, LDL, and TG levels were not significantly different between smokers and non-smokers (p = .594, p = .578, p = .089, respectively), whereas HDL level (p < .001) was significantly different between the two groups.
The Comparison of Smoking and Non-Smoking Group Based on Their Lipid Profiles

Note. LDL = low-density lipoprotein; HDL = high-density lipoprotein; TC = total cholesterol; TG = triglycerides
Logistic Regression Analysis of Smoking and Lipid Profile
Results of multivariate regression analysis showed that odds of low-level HDL in smoker participant was 1.48 (1.25–1.77) higher than non-smoker participant (p < .001; Table 5). Our finding showed after adjusting for possible confounding variables including age, BMI, MET index, residency, marital status, social economic level, educational level, and WHR, only the frequency of people with low HDL was significantly higher in smokers, 38% (odds ratio [OR]: 1.38) more than in non-smokers (Table 4).
Association Between Current Smoking and Lipid Profile Using Univariate and Multivariate Regression

Adjusted variables: age, body mass index, metabolic equivalent of task, residency, marital status, social economic status, education years, waist circumference, waist to hip ratio, and waist to height ratio. LDL = low-density lipoprotein; HDL = high-density lipoprotein; TC = total cholesterol; TG = triglycerides; OR = odds ratio; CI = confidence interval.
In addition, we analyzed the association between severity of smoking with lipid profile in smoker participants. Results showed a significant relationship between pack-year smoking with HDL and LDL level, based on the result analysis of p for trend with multivariate logistic regression (Table 5). When examining the severity of smoking in relation to non-normal lipid profile levels, a significant direct relationship was observed for LDL (p for trend = .015) and HDL (p for trend < .001) after adjusting for confounder variables (Table 5). The adjusted OR of high LDL in men with 1 to 10, 11 to 20, and more than 20 cigarettes per day was 0.96 (95% CI: 0.73–1.25), 1.30 (95% CI: 0.99–1.71), and 2.64 (95% CI: 1.32–5.27) and low HDL was 1.34 (95% CI: 1.06–1.68), 1.61 (95% CI: 1.26–2.05), and 2.24 (95% CI: 1.13–4.42) compared with non-smokers, respectively. In other words, the OR of LDL and HDL disorders has significantly increased with the increase in the number of cigarettes smoked per day (Table 6).
The Number of Pack-Year Smoking Groups Based on Lipid Profile (Chi-Square and p for Trend With Multivariate Logistic Regression)

Adjusted variables: age, body mass index, metabolic equivalent of task, residency, marital status, social economic status, education years, waist circumference, waist to hip ratio, and waist to height ratio. LDL = low-density lipoprotein; HDL = high-density lipoprotein; TC = total cholesterol; TG = triglycerides.
Association Between Severity of Smoking and Lipid Profile Using Univariate and Multivariate Logistic Regression
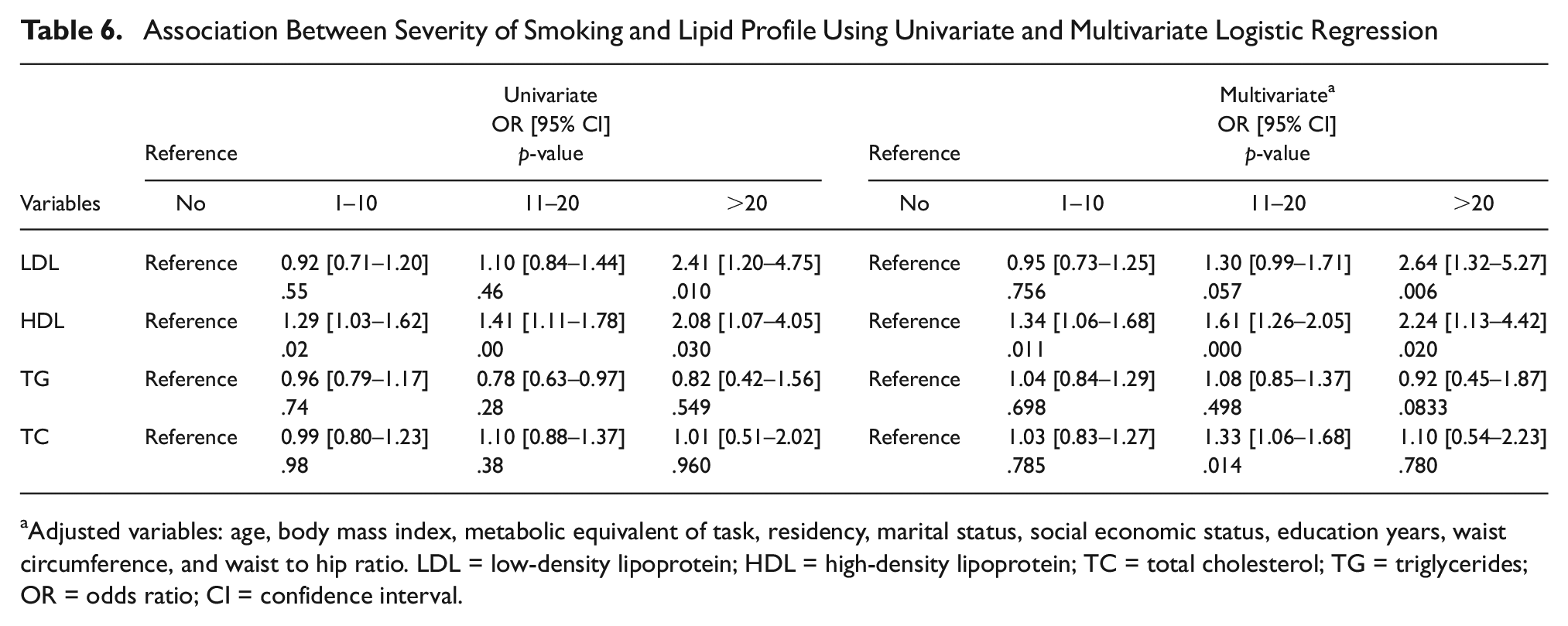
Adjusted variables: age, body mass index, metabolic equivalent of task, residency, marital status, social economic status, education years, waist circumference, and waist to hip ratio. LDL = low-density lipoprotein; HDL = high-density lipoprotein; TC = total cholesterol; TG = triglycerides; OR = odds ratio; CI = confidence interval.
Discussion
Association Between Smoking and Lipid Profile
The present study aimed to investigate the association between smoking and lipid profile in a population-based cohort study aged between 35 and 70 years old conducted within the TCS. The results of the present study showed that smoker participants had low level of HDL and this finding remained consistent after adjusting for possible confounding variables. The severity of dyslipidemia was observed to increase with the extent of smoking, indicating a dose–response relationship between smoking and its impact on lipid profile. The dose–response analysis showed that the chance of abnormal level of LDL and HDL in participants who smoked more than 20 pack-years, respectively, is 2.64 and 2.24 times more than participants who smoked less than 10 pack-years.
Previous research has already concluded that smoking is linked to unfavorable changes in lipid profile, including elevated TC, LDL, and TG, as well as decreased HDL levels, all of which are indicators of cardiovascular risk (Girish & Harish, 2018). Hence, based on our findings, it can be concluded that smoking has a significant negative impact on HDL-cholesterol levels, even after accounting for other factors.
Smoking can affect HDL-cholesterol levels and function through various mechanisms, such as altering lipid transport enzymes, causing oxidative modifications, and reducing HDL-cholesterol levels (Assmann et al., 1984). In summary, smoking-induced changes in cholesterol metabolism involve alterations in lipid transport enzymes, oxidative modifications of lipoproteins, and changes in serum cholesterol levels. These effects can impact HDL metabolism, contribute to changes in lipid profile, and potentially increase the risk of cardiovascular disease (He et al., 2013).
Association Between Smoking Intensity and Lipid Profile
Considering our findings, as smoking intensity increases, there is a tendency for TC and TG, while LDL and HDL levels significantly disturb. Such alterations in lipid profile may contribute to the development of dyslipidemia and elevate the risk of cardiovascular disease (Girish & Harish, 2018). Previous researches inferred that smoking has the potential to influence abnormal blood LDL levels by affecting oxidative stress (Ho et al., 2021). Further investigation is required to gain a comprehensive understanding of the underlying mechanisms. Our study did not find significant differences in TC, LDL-cholesterol, and TG levels between smokers and non-smokers and this finding contrasts with some previous research. However, it is important to note that smoking is often associated with other lifestyle factors that can influence lipid levels, making it challenging to isolate the precise effects of smoking alone. Further research is needed to comprehensively elucidate the disparities in the impact of smoking on different lipid subclasses.
Association Between Demographic and Smoking Status of Study Participants
In the present study, the prevalence of smoking was found to be higher in mountainous areas compared to urban areas. This finding is consistent with numerous other studies that have shown a higher likelihood of smoking among rural residents compared to their urban counterparts. This association can be attributed to various factors, including socioeconomic conditions, cultural norms, and limited access to health care facilities. Consequently, there is a clear link between rural residency and smoking, with higher smoking rates observed in rural communities (Axelson et al., 1988; Gergianaki et al., 2019).
Furthermore, our study aligns with several other investigations that highlight a distinct connection between lower education levels and a higher prevalence of smoking. Collectively, these studies indicate that this association is likely influenced by a combination of factors, such as limited access to information regarding the health risks associated with smoking and fewer resources to effectively manage stress (Menvielle, Franck, Radoï, et al., 2016; Menvielle, Franck, Stücker, & Luce, 2016; Yu et al., 2018). In addition, our findings reveal a direct relationship between smoking and MET index, while indicating a negative relationship between smoking and BMI, WC, WHR, and WHtR indices.
Certain studies have suggested two potential reasons for the lower weight indices observed in smokers: an increase in the rate of metabolism and a decrease in appetite. The exact cause of the heightened metabolic rate in smokers remains uncertain, although it is hypothesized that nicotine in cigarettes may stimulate the sympathetic nervous system, or that smoking could enhance the production of adrenaline (Warwick et al., 1987).
Association Between Lipid Profile and Demographic Variables in Smokers
There is no clear evidence regarding demographic characteristics and its relationship with smoking and lipid profile. The present study revealed a significant relationship between the age of smokers and high levels of LDL, TC, and TG. This finding aligns with previous research indicating that middle-aged individuals (45–64 years) who smoke are more susceptible to health disorders (Dube et al., 2019).
Our study established a direct relationship between MET index, BMI, WHR, WHtR, and all four lipid profile factors. This was expected since these indices are commonly associated with obesity, consistent with previous findings (Stępień et al., 2014).
It is crucial to highlight that quitting smoking has the potential to improve serum lipid levels and reduce the risk of cardiovascular disease in some individuals (He et al., 2013). In addition to smoking cessation, there are several lifestyle modifications that can be beneficial in improving the lipid profile of smokers. These include adopting a healthy diet, engaging in regular physical activity, maintaining a healthy weight, and effectively managing stress (Joshi et al., 2013).
It is advisable to seek guidance from a health care professional for personalized advice on improving lipid profile as a smoker. They can offer tailored recommendations and closely monitor progress over time. Consulting with a health care professional ensures that the interventions are suitable for individual circumstances and can maximize the effectiveness of the efforts to enhance lipid profile. Overall, this study emphasizes the need for comprehensive smoking cessation interventions and highlights the role of HDL as a crucial biomarker for assessing cardiovascular risks in individuals who smoke. By prioritizing efforts to reduce smoking prevalence and promote healthier lifestyles, we can empower individuals to make informed decisions for their cardiovascular well-being and ultimately strive for a healthier, smoke-free future.
Strengths and Limitations
Significant strength of this study lies in its large sample size, the use of a standardized questionnaire with established reliability and validity, and the inclusion of comprehensive laboratory measurements for lipid profile assessment. However, there are some limitations to consider. One of the limitations of the current study is its cross-sectional design, which introduces a potential distortion in establishing a causal relationship between lipid profile and smoking. To overcome this limitation, we performed a dose–response analysis (cigarettes per day). It is recommended that future research will explore this relationship using prospective studies. Longitudinal studies would provide more robust evidence in this regard. Second, the study population consisted of Iranian men aged 35 to 70 years old, which may limit the generalizability of the findings to other populations. Future research should aim to replicate these findings in diverse populations.
Further research is needed to gain a deeper understanding of the underlying mechanisms linking smoking and lipid metabolism and to explore the impact of smoking cessation on lipid profile improvement. Longitudinal studies involving diverse populations would provide valuable insights into the long-term effects of smoking on lipid profile and cardiovascular health.
Conclusion
In conclusion, this study provides compelling evidence that smoking is associated with low levels of HDL in men, and this correlation remains even after accounting for potential confounding variables. The dose–response analysis further elucidates the impact of smoking intensity on LDL and HDL levels. Participants with a smoking history surpassing 20 pack-years exhibited an abnormal amount of lipid that was more than twice that of those with a smoking history of less than 10 pack-years. These findings highlight the need for comprehensive smoking cessation interventions and emphasize the role of HDL as a crucial biomarker for assessing cardiovascular risks in individuals who smoke. By prioritizing efforts to reduce smoking prevalence and promote healthier lifestyles, we can empower individuals to make informed decisions for their cardiovascular well-being and ultimately strive for a healthier, smoke-free future.
Footnotes
Acknowledgements
The authors would like to thank all the members of the PERSIAN cohort study (Ministry of Health and Medical Education and Mazandaran University of Medical Sciences).
Authors’ Contributions
Mahmood Moosazadeh and Mona Modanloo acquired data, performed the statistical analyses, interpreted data, drafted and revised the manuscript for important intellectual content, and approved the final version. Motahareh Kheradmand, Pedram Ebrahimnejad, Mehrasa Rostamian, Shamim Mahboobi, Fatemeh Mardanshah, Marzieh Dehghanzadegan, Fatemeh kianmehr, and Aysa Safajoo interpreted data, reviewed the analyses, and approved the final version. All authors have read and approved the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the research deputy of Mazandaran University of Medical Science (grant no. 2524). The funding body played no role in the design of the study and collection, analysis, and interpretation of data and in writing or decision to publish this manuscript.
Ethics Approval and Consent to Participate
TCS was confirmed by the Mazandaran University of Medical Science ethical committee (IR.MAZUMS.REC.95.2524). All ethical principles of the Helsinki ethical declaration have been met and written informed consent was obtained from all the participants.
Consent for Publication
Not applicable.
Availability of Data and Materials
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.