
Abstract
The objective of this study is to evaluate the prognostic value of lymphocyte-to-monocyte ratio (LMR) in patients with prostate cancer (PCa) by a method of meta-analysis. China National Knowledge Infrastructure (CNKI), Wanfang Data, PubMed, Web of Science, Cochrane Library, and Embase were searched to collect relevant literature until March 2023. The Newcastle-Ottawa Scale was used to assess the bias risk of the literature included. Hazard ratios (HRs) and 95% confidence intervals (CIs) were used to evaluate the prognostic value of LMR in PCa. Stata 15.0 statistical software was used for data analysis. A total of six published articles were included in this meta-analysis, containing 1,104 patients with PCa. The results of the meta-analysis indicated better overall survival (OS; HR = 1.73, 95% CI: 1.73, p = .001) and progression-free survival (PFS; HR = 2.63, 95% CI: 1.58~4.38, p < .001) in patients with PCa with low LMR compared with high LMR. In conclusion, compared with low LMR, PCa patients with high LMR have a better prognosis. LMR is an independent risk factor affecting the long-term prognosis of patients with PCa. The detection of LMR before treatment is of certain significance in judging the clinical prognosis of patients with PCa.
Introduction
Prostate cancer (PCa), a common malignant tumor of the urinary system, is second only to lung cancer in the incidence of male tumors. According to the latest data, the number of new cases of PCa in 2022 is expected to exceed 268,000 in the United States, surpassing lung cancer and ranking first among male tumors (Siegel et al., 2022). PCa usually has three clinical stages in the diagnosis and treatment process, which first begins with the prostate limitation stage, then progresses to prostate-specific antigen (PSA) increasing stage, and then the castration metastasis stage, known as metastatic castration-resistant prostate cancer (mCRPC; Achard et al., 2022). PCa in the localized stage was asymptomatic, being in the advanced stage of metastasis when symptoms appeared. It is of great clinical significance to identify prognostic markers of PCa.
The inflammatory state and internal environment changes of patients with malignant tumors affect their prognosis and outcome to some extent, and the inflammatory state is correlated with the malignancy of tumors and the prognosis of patients (Diakos et al., 2014). The relationship between inflammation, tumor occurrence and development, and tumor microenvironment has been widely recognized (Murata, 2018). Several studies have explored and confirmed the potential mechanism of inflammation affecting tumors through animal models and clinical models (Iyengar et al., 2016; Mohammed et al., 2021; Nøst et al., 2021; Song et al., 2022). A large number of studies reported that immune inflammatory cells in peripheral blood, such as neutrophils, platelets, and lymphocytes, can promote the proliferation, invasion, and migration of tumor cells (Jin et al., 2021; Wei et al., 2020; Yoon et al., 2021). Hematological indicators established based on these immunoinflammatory cells, such as neutrophil-to-lymphocyte ratio (NLR), platelet-to-lymphocyte ratio (PLR), lymphocyte-to-monocyte ratio (LMR), and so on, are thought to reflect the levels of systemic immune and inflammatory responses. It has been reported in several studies that these hematological indicators can be used to predict the therapeutic effect or prognosis of patients with various malignant tumors, including non-small-cell lung carcinoma, PCa (Guan et al., 2020; Guo et al., 2018; Liu et al., 2022), and so on. These hematological indicators are simple, economical, and easy to detect, so they become a hot spot in clinical research related to tumor prognosis.
There is no systematic review to investigate the association between LMR and PCa prognosis at present. Therefore, the method of meta-analysis was applied in this study to investigate the relationship between LMR and the prognosis of PCa and to provide evidence-based medical evidence for the prognostic value of LMR in the treatment of PCa.
Method
Literature Retrieval
This meta-analysis was conducted according to the guiding principles of the Preferred Reporting Items For Systematic Reviews and Meta-Analyses (PRISMA; Moher et al., 2010; Supplementary Table 1). China National Knowledge Infrastructure (CNKI), Wanfang Data, PubMed, Web of Science, Cochrane Library, and Embase databases were searched to collect literature on the prognostic value of LMR in PCa from inception to March 2023. The search strategy was as follows: (“prostate cancer” OR “prostate carcinoma” OR “prostate tumor”) AND (“Lymphocyte to monocyte ratio” OR “Lymphocyte to monocyte” OR “LMR”). There were no restrictions on language. Relevant records in each database were retrieved independently by two researchers and finally cross-checked. If there was any inconsistency in the process of retrieval, the two researchers reached an agreement through discussion.
Inclusion and Exclusion Criteria
Inclusion criteria: (a) subjects were pathologically diagnosed patients with PCa; (b) the relationship between LMR and overall survival (OS) or progression-free survival (PFS) of patients with PCa was reported; (c) the complete hazard ratio (HR) and 95% confidence interval (CI) could be obtained, or calculated according to the data in the paper identified.
Exclusion criteria: (a) conference abstracts, reviews, case reports, letters, or unpublished studies; (b) the research data in the original literature were incomplete; (c) duplicate data; (d) only abstracts existed and full texts could not be obtained.
Literature Screening and Data Extraction
Data screening, extraction, and cross-checking of literature were conducted independently by two researchers. In case of disputes, the two researchers reached an agreement through discussion. Data extraction included first author, year of publication, ages, country, number of PCa, follow-up period, tumor node metastasis (TNM) stage, treatments, cut-off value of LMR, HR, and 95% CI for OS and PFS.
Quality Assessment of the Included Records
The Newcastle-Ottawa Scale (NOS) was applied to assess the qualities of the included studies (Stang, 2010), evaluated from three aspects: (a) selectivity (0–4 points); (b) Comparability (0–2 points); (c) Outcome evaluation (0–3 points). The total NOS score is nine. Studies with NOS scores ≥6 were rated as high quality.
Statistical Analysis
Stata 15.0 statistical software was used for data analysis. We directly obtained the HR values from the literature, or used Engauge Digitizer 11.3 software to extract effective data from the Kaplan–Meier survival curve, and then calculated HR and 95% CI as measurement indexes. Heterogeneity was tested by Cochran’s Q statistic test. I2 statistics and P values were selected to judge the magnitude of heterogeneity. If heterogeneity was significant (I2≥ 50%, or P≤ 0.05), a random-effects model was chosen for meta-analysis. Otherwise (I2 < 50%, and P > 0.05), a fixed-effects model was utilized. If obvious heterogeneity existed, the sources of heterogeneity were investigated according to ethnicity. The sensitivity analysis was performed with the method of one-by-one exclusion to explore the influence of a single study on the combination effect. Egger’s test was used to evaluate the publication bias. p < .05 was considered statistically significant.
Results
Results of the Literature Search
According to strict screening criteria, a total of six articles were finally entered into this meta-analysis (Bauckneht et al., 2020, 2022; Huszno et al., 2022; Li et al., 2021; Liang et al., 2022; Shigeta et al., 2016; Figure 1), including 1,104 patients with PCa. One paper contained two studies (Shigeta et al., 2016). The basic characteristics of the included studies are presented in Table 1. As seen from Table 1, the NOS scores of all the included studies were higher than 6 points, indicating that they were all high-quality studies.

Flowchart of Literature Screening
Basic Characteristics of the Included Studies
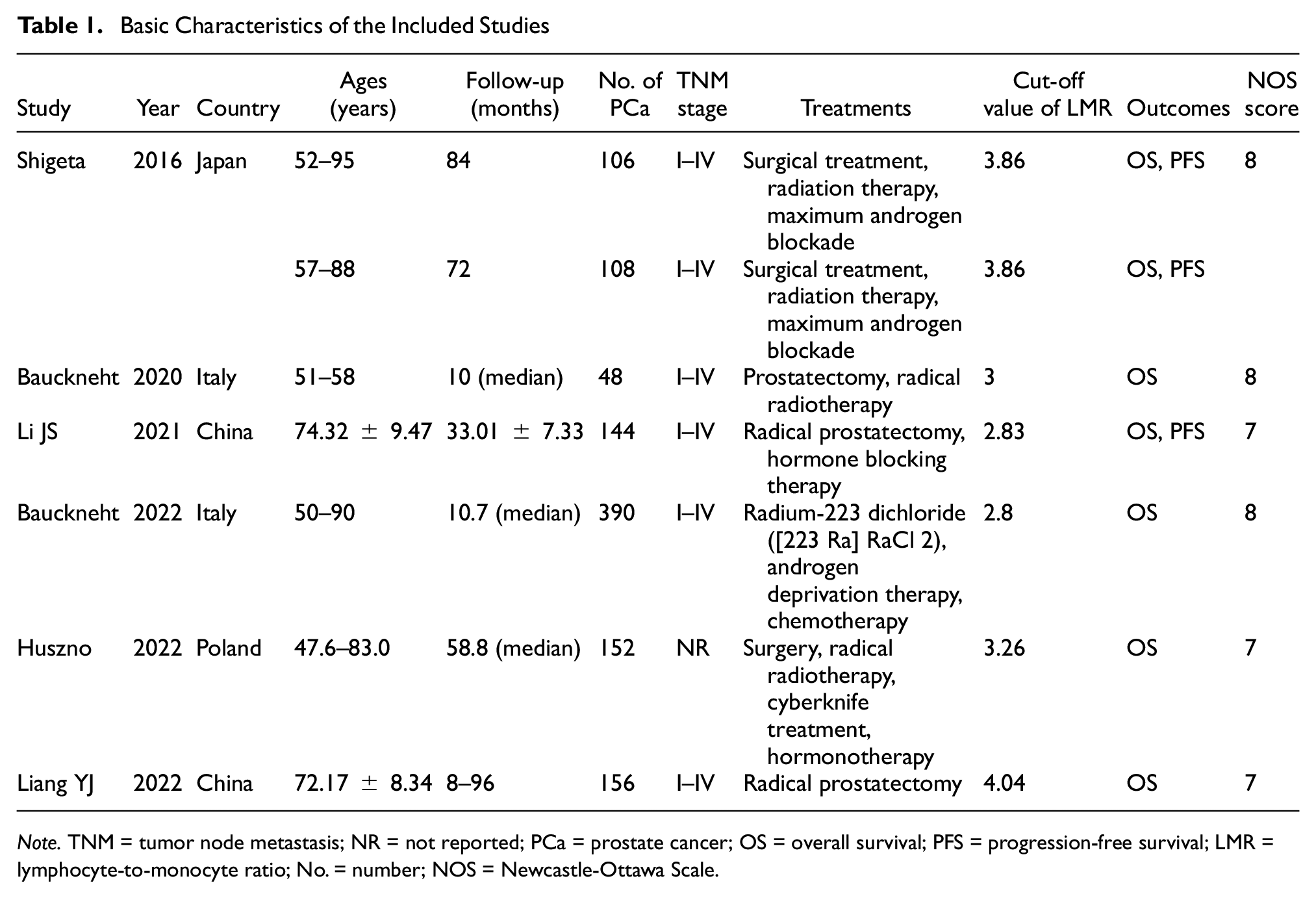
Note. TNM = tumor node metastasis; NR = not reported; PCa = prostate cancer; OS = overall survival; PFS = progression-free survival; LMR = lymphocyte-to-monocyte ratio; No. = number; NOS = Newcastle-Ottawa Scale.
Results of Meta-Analysis
Relationship Between LMR and OS in PCa Patients
A total of six articles, including seven studies, were included in the meta-analysis of LMR influencing OS in PCa patients. There was significant heterogeneity among eligible studies (I2 = 84.5%, p < .001). Therefore, the random-effects model was used. The results of the meta-analysis (Figure 2) indicated that the OS of PCa patients with low LMR was significantly shorter than those with high LMR (HR = 1.73, 95% CI: 1.25–2.39; Z = 3.276, p = .001). The subgroup analysis based on ethnicity suggested no significant reduction in heterogeneity among either Asians (I2 = 90.2%, p < .001) or Caucasians (I2 = 75.2%, p = .018).

Forest Plot of LMR Associated With OS of PCa Patients
Relationship Between LMR and PFS in PCa Patients
There were two articles (Li et al., 2021; Shigeta et al., 2016), including three studies included in the meta-analysis of LMR associated with PFS in patients with PCa. Significant heterogeneity across identified studies existed (I2 = 55.0%, p = .108). Therefore, the random-effects model was adopted for the combined analysis. The pooled results (Figure 3) displayed that the PFS of PCa patients with low LMR were significantly shorter than those with high LMR (HR = 2.63, 95% CI: 1.58–4.38; Z = 3.725, p < .001).

Forest Plot of LMR Associated With PFS of PCa Patients
Publication Bias Detection
Egger’s Test was conducted to detect publication bias in terms of LMR related to the OS of patients with PCa. Egger’s Test showed a p value of .056 (t = 2.48), which was larger than .05, indicating no obvious publication bias in this meta-analysis.
Sensitivity Analysis
Sensitivity analysis was performed on the results of the combined analysis of LMR associated with OS of PCa patients. The results showed (Figure 4) that no significant change was observed between the conclusions of the combined analysis again after omitting each study and the conclusions before the elimination. Therefore, the findings of this study have good robustness.
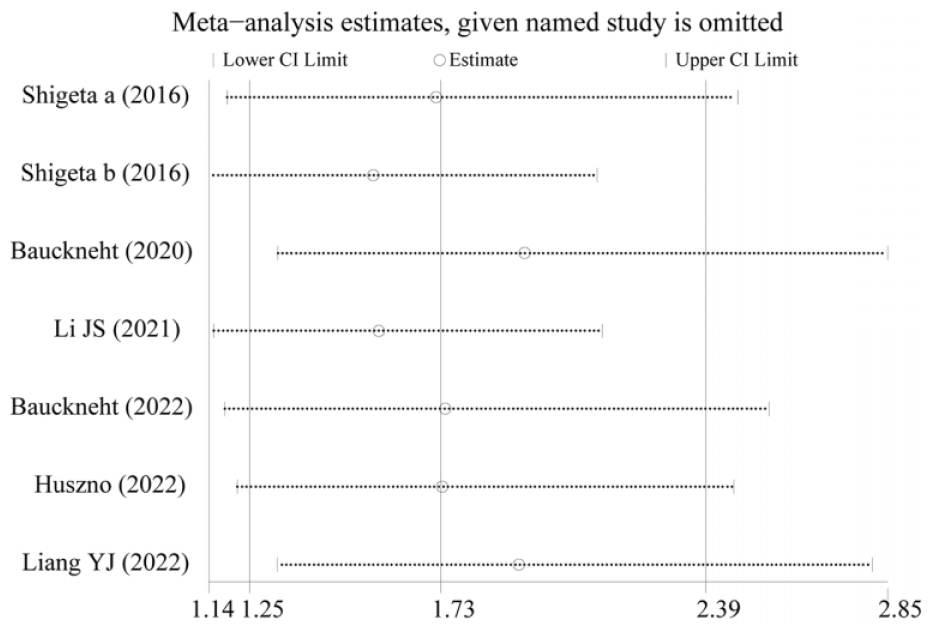
Sensitivity Analysis of LMR Associated With OS of PCa Patients
Discussion
Studies identified that inflammation not only increases the risk of cancer but also promotes the progression and metastasis of cancer (Coussens &Werb, 2002; Neufert et al., 2021; Zhang & Xu, 2023). Inflammation plays an essential role in the occurrence, development, and metastasis of tumors by promoting angiogenesis, proliferation, and anti-apoptosis (Coussens &Werb, 2002). Neutrophils, monocytes, platelets, and lymphocytes in peripheral blood all play a key role in systemic inflammatory responses. Guo et al.’s meta-analysis (Guo et al., 2018) in 2018 reported that elevated NLR and PLR was associated with poor OS and PFS. As a marker of systemic inflammatory response, LMR has potential value in the diagnosis and prognosis of tumors.
One of the most common immune cells in the tumor microenvironment is tumor-associated macrophages, which are partially derived from the local proliferation of macrophages and mostly from monocytes in peripheral blood circulation. Chemokines produced by tumors are considered to be important factors in introducing monocytes into tumors (Balkwill et al., 2005). In addition, lymphocytes play a crucial role in regulating immune antitumor activity (Bai et al., 2021; Goff & Danforth, 2021), and tumor-infiltrating differentiation clusters CD8+ and CD4+ lymphocytes have been proven to play a significant role in antitumor activity (Sznurkowski et al., 2011). This means that a decrease in the number of lymphocytes can indicate tumor cells escaping the normal immune system, which could affect a patient’s survival prognosis.
Owing to the controversy over the results of LMR associated with survival analysis in previous studies, this article systematically reviews the relationship between LMR, a systemic inflammatory response indicator, and prognosis in PCa patients. A total of six articles were included in our study. Although there was obvious heterogeneity among the included studies, we still obtained several meaningful conclusions. This study is the first meta-analysis on the correlation between LMR and the prognostic value of patients with PCa, possessing essential clinical significance. By combining HR and 95% CI, the overall results showed that LMR was a risk factor for OS and PFS in PCa patients. PCa patients with high LMR had better OS and PFS than those with low LMR. The publication bias detection of OS detected by Egger’s Test showed that the p value was greater than .05, indicating no obvious publication bias in this study. Sensitivity analysis of OS showed that there was no significant difference between the conclusion of recombination after the removal of any study and that before the removal, indicating that the conclusion obtained in this study had good robustness.
The modified Glasgow Prognostic Score (mGPS) is based on serum albumin and C-reactive protein levels to evaluate the nutritional status of patients (McMillan et al., 2007). The mGPS can predict the prognosis of PCa (Goktas Aydin et al., 2024; Neuberger et al., 2023). Neuberger identified that baseline mGPS could predict radiologic response and OS in metastatic hormone-sensitive PCa treated with docetaxel chemotherapy (Neuberger et al., 2022). Therefore, the prognostic value of LMR, NLR, or PLR for PCa after stratification based on mGPS is essential for clinical decision-making in PCa treatment, which is also a key topic for future research.
There were several limitations in our meta-analysis. First, only six articles were included in this review, with a small sample size, which might have a certain influence on the robustness of the conclusions. LMR is a dynamic process, and due to limited sample size, comparative analysis before and after treatment cannot be conducted. Second, significant heterogeneity existed in both OS and PFS analyses. Heterogeneity was not reduced even after subgroup analysis based on ethnicity. There might be other sources of heterogeneity. For instance, the unequal truncation values of LMR may affect the clinical application of LMR, and more credible evidence is needed to determine the optimal cut-off values. Third, LMR comes from peripheral blood, easily affected by patients’ basic conditions, such as age, tumor burden, histological features, disease stage, inflammatory disease, chronic disease, and so on. Fourth, the research population of the six included articles were concentrated in China, Japan, Italy, and Poland, and the scope of the research subjects is relatively limited. Therefore, more studies are needed to verify whether the findings of this meta-analysis can be extrapolated to other ethnic groups.
Conclusion
Compared with low LMR, PCa patients with high LMR have a better prognosis. LMR is a risk factor affecting the prognosis of patients with PCa and can predict the biological behavior of cancer to a certain extent. However, due to the limitations of this study, the results should be treated with caution. Compared with other prognostic markers, systemic inflammatory response indicators have the advantages of low cost, repeatability, and simplicity, which are expected to be popularized in clinical practice, helping clinicians to provide a certain reference basis for individual treatment of patients. More large-scale, prospective studies are warranted to verify the value of LMR for prognosis in patients with PCa in the future.
Supplemental Material
sj-docx-1-jmh-10.1177_15579883241234747 – Supplemental material for Prognostic Value of Lymphocyte-to-Monocyte Ratio (LMR) in Patients With Prostate Cancer: A Systematic Review and Meta-Analysis
Supplemental material, sj-docx-1-jmh-10.1177_15579883241234747 for Prognostic Value of Lymphocyte-to-Monocyte Ratio (LMR) in Patients With Prostate Cancer: A Systematic Review and Meta-Analysis by Qin Xiang, Yueguang Liu, Junwen Xiao, Longhua Ou and Jianhui Du in American Journal of Men’s Health
Footnotes
Acknowledgment and Credits
None.
Authors’ Contributions
Made a substantial contribution to the concept or design of the work (Q.X., Y.L., J.D.); drafted the article or revised it critically for important intellectual content (Q.X., Y.L., J.X., L.O., and J.D.); acquisition, analysis or interpretation of data (Q.X., Y.L., and J.X.); critical revision of the manuscript (Q.X., L.O., J.D.); approved the version to be published (Q.X., Y.L., J.X., L.O., J.D.). All the authors have participated sufficiently in the work to take public responsibility for appropriate portions of the content.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This paper is supported by the Medical youth innovation research project of Sichuan province (grant no. Q22051), Research project of Sichuan Medical Hygiene and Health Promotion Association (grant no. KY2022QN0139), and the Fund for promoting high-quality hospital development of Guang’an People’s Hospital of Sichuan Province (grant no. 21FZ013).
Ethics Approval and Consent to Participate
Ethics approval and consent to participate are not applicable because this is a meta-analysis.
Consent for Publication
There is not applicable.
Availability of Data and Material
The datasets adopted during the meta-analysis are available on reasonable request from the corresponding author.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.