
Abstract
Although men have greater societal and economic privileges, men have higher all-cause mortality rates than women, even after controlling for education. Further, racial/ethnic mortality disparities exist among men with varying levels of education. Few studies have explored the independent effects of education and all-cause mortality between non-Hispanic Black and non-Hispanic White men with the same level of education. Our purpose was to identify trends in racial differences in all-cause mortality between non-Hispanic White and non-Hispanic Black men with the same level of education. Data for the study came from the National Health Interview Surveys 2000–2011 linked to the 2000–2009 Mortality Files. The Student’s t and chi-square tests were used to assess the mean and proportional differences between non-Hispanic White and non-Hispanic Black men (≥18 years of age) across a range of demographic and health-related factors. Cox proportional hazard models were specified to examine the association between level of education and all-cause mortality adjusting for the demographic and health characteristics. Except for men who did not complete high school, statistically significant differences in all-cause mortality are present between non-Hispanic Black and non-Hispanic White men with the same level of education. The findings reveal the importance of understanding the level of education on differences in all-cause mortality between non-Hispanic Whites and non-Hispanic Blacks.
Keywords
There are societal and economic privileges associated with being male; however, women have significantly lower all-cause mortality rates than men, even after controlling for education (Hummer & Hernandez, 2013). While mortality has steadily declined in the United States, a body of evidence has confirmed racial disparities in mortality between Black and White men remain present (Beydoun et al., 2016; Cunningham et al., 2017; Freeman, Zonszein, Islam, Blank, & Strelnick, 2011; Hummer & Hernandez, 2013; Zajacova & Hummer, 2009). This is likely because there has been a paucity of research focusing on disentangling race and socioeconomic status (SES) in health disparities research (Beydoun et al., 2016; LaVeist 2005). There has been work on race, education, and mortality (Beydoun et al., 2016; Cunningham et al., 2017; Freeman et al., 2011; Hummer & Hernandez, 2013; Zajacova & Hummer, 2009). Yet, we are unaware of any studies that have focused exclusively on race differences in all-cause mortality among non-Hispanic Black and non-Hispanic White men. In addition, there is a need to advance our understanding of these race disparities in all-cause mortality among men by understanding race differences in mortality within levels of SES as measured by education.
Education has a critical role in determining one’s access to social and economic opportunities and ultimately affects life trajectory (Zajacova, 2006). Men with more education liver longer than their less educated peers (Sheehan, Montez, & Sasson, 2018). A vast body of literature has documented the strong inverse relationship between education and mortality (Hummer & Hernandez, 2013; Montez, Hayward, Brown, & Hummer, 2009; Montez, Hummer, Hayward, Wood, & Rogers, 2011; Sheehan et al., 2018; Zajacova, 2006; Zajacova & Hummer, 2009; Zajacova, Rogers, & Johnson-Lawrence, 2012). Substantial research has confirmed the education–mortality gradient; however, few studies have investigated racial differences in all-cause mortality between non-Hispanic White and non-Hispanic Black men with the same level of education.
The goal of this study was to determine whether all-cause mortality differs between non-Hispanic Black and non-Hispanic White men with the same level of education. This work will add to the growing body of men’s health disparities by examining the race differences in all-cause mortality between non-Hispanic Black and non-Hispanic Black men with the same level of education. This approach minimizes the potential confounding of race and SES, namely education.
Methods
Dataset
The National Health Interview Survey (NHIS) is a cross-sectional survey conducted annually by the National Center for Health Statistics via in-home interviews administered by U.S. Census Bureau. NHIS uses a nationally representative sample of the U.S. non-institutionalized civilian population from all 50 states and the District of Columbia. The NHIS includes individuals living in non-institutionalized populations of the United States, and oversamples non-Hispanic Blacks, Hispanics, non-Hispanic Asians, and persons aged 65 and older. The sampling follows a random, multistage area probability design that incorporates stratification and clustering (National Center for Health Statistics, 2006). Data from the 2000–2011 NHIS Sample Adult file were used for this study. Participants are surveyed regarding their demographic characteristics; health behaviors and conditions; functional limitations; cancer screening; and health-care access and utilization. Detailed information regarding NHIS can be found elsewhere (National Center for Health Statistics, 2006; Pleis & Lucas, 2009).
All-cause mortality data was ascertained through record matching with the National Death Index (NDI). Mortality follow-up for adults who participated in the 2000–2011 NHIS was obtained by linking records to NDI. The resulting data, The National Health Interview Survey – Linked Mortality File (NHIS-LMF), were used in this study (National Center for Health Statistics, 2013; Pleis & Lucas, 2009).
Study Sample
Data for the study came from the 2000–2009 NHIS-LMF. The NHIS-LMF is a probabilistic sample of non-Hispanic Blacks (n = 125,817, 18.7%), non-Hispanic Whites (n = 501,311, 74.5%), other adults (n = 43,782, 6.5%) aged ≥18 years. In this study, women (n = 461,858, 68.6%), those with Hispanic origin (n = 208,032, 30.9%), respondents who reported multiple races (n = 10,698, 1.6%), respondents whose race was neither only White nor only Black/African American (n = 33,084, 4.9%) were excluded. Those missing education data (n = 93,854, 1.4%) and mortality follow-up data (n = 311,960, 46.4%) were excluded. This resulted in an analytic sample size of 96,587 of which 15,591 (16.1%) are non-Hispanic Black men (referred to as Black men, hereafter) and 80,996 (83.9%) are non-Hispanic White men (referred to as White men, hereafter) with 9,211 (9.5%) deaths from any cause. Additional information on the sampling design and procedures of the NHIS-LMF is reported elsewhere (National Center for Health Statistics, 2013).
Measures
The primary outcome of this study is all-cause mortality. Mortality data w ascertained through record matching through the: National Death Index, Social Security Administration, Centers for Medicare and Medicaid Services, and death certificate matches. (National Center for Health Statistics Office of Analysis and Epidemiology, 2013). A binary variable for all-cause mortality was created to identify those men assumed alive versus those men assumed deceased from any cause (1 = assumed deceased, 0 = assumed alive). To determine the duration in this study, the derivation was based on National Center for Health Statistics use of the NHIS interview year and death year (Lochner et al., 2008). This has been used by other investigators (Borrell & Crawford, 2009).
The primary independent variables were race/ethnicity and education. Men reported their highest level of education, which was then categorized: less than high school; high school diploma or general equivalency diploma (GED); some college; associate degree and beyond. Men also reported their race as White or Black/African American and their ethnicity as Hispanic or not Hispanic. A variable was created to identify the racial/ethnic groups: non-Hispanic White and non-Hispanic Black.
Demographic variables included age (years), married (1 = yes, 0 = no), income level (<$34,999, $35,000–74,999, ≥$75,000). Health-related characteristics included having health insurance (1 = yes, 0 = no), smoking and drinking status (0 = never, 1 = current, 2 = former), obesity (1 = obese, 0 = not obese) as well as number of chronic conditions (none, one, two, three, or more).
Analytic Approach
The Student’s t and chi-square tests were used to assess the mean and proportional differences between White and Black men (≥18 years of age) across a range of demographic and health-related factors. Cox proportional hazard models were specified to examine the association between level of education and all-cause mortality adjusting for the measures described above. Survey procedures were used when specifying the statistical models to account for the complex survey sampling design of the NHIS. p values < .05 were considered statistically significant and all tests were two-sided. All analyses were conducted using STATA 14 software (Stata Corp., College Station, TX, USA).
Results
The distribution of characteristics of Black men and White are presented in Table 1. Black men were less likely to complete high school than Whites; 21% (n = 3,275) of Black men did not complete high school compared to only 12% (n = 9,720) of White men. Approximately one-third (33.8%, n = 5,270) of Black men report having a high school diploma or GED has their highest level of education, compared to 30% (n = 24,299) of Whites. For some college, the numbers are 21.3% (n = 3,321) and 19.4% (n = 15,713) respectively. Black men were less likely to report having an associate degree or beyond (23.9%, n = 3,726). Nearly half (47.6%, n = 7,421) of the Black men were married and 32.2% (n = 26,081) of White men indicate being married. Black men reported lower earning lower income over all than White men. Thirty-seven percent (n = 5,769) of Black men reported an annual household income of than $34,999, 28% (n = 4,365) reported an annual household income between $35,000 and $74,999, and 13.1% (n = 2,042) reported an annual household income above $75,000. For White men, the numbers are 23.6% (n = 19,115), 29.8% (n = 24,137), and 25.8% (n = 20,897), respectively. Men who chose not to report income or had missing income were similar among Blacks (21.9%, n = 3,414) and Whites (20.8%, n = 16,847). More White men (86.9%, n = 70,386) had health insurance coverage than Black men (77.3%, n = 12,052). More than half of Black men (56.7%, n = 8,840) reported never smoking and nearly one quarter (24.8%, n = 3,867) reported never drinking. Among White men, the numbers are 46.9% (n = 37,987) and 12.9% (n = 10,448), respectively. Approximately 26% (n = 4,085) of Black and 25% (n = 20,006) of White men reported currently smoking, and 59.2% (n = 9,230) of Blacks and 74.8% (n = 58,155) of White men reported currently drinking. White men were more likely to be former smokers (28.5%, n = 23,084 vs. 17.2%, n = 2,682). However, Black men were more likely to be former drinkers (16.1%, n = 2,510 vs. 15.3%, n = 12,392). Further, 30.8% (n = 4,802) of Black men and 26.3% (n = 21,302) of White men were obese; 57.6% (n = 8,981) of Black men reported having no chronic conditions, 28.3% (n = 4,413) reported having one chronic condition, 10.2% (n = 1,591) reported having two chronic conditions and 6.9% (n = 1,076) reported having three or more chronic conditions. For White men, the numbers are 55.1% (n = 44,629), 25.7% (n = 20,816), 10.8% (n = 8,748), and 8.3% (n = 6,723), respectively.
Distribution of Select Characteristics of Non-Hispanic Black and Non-Hispanic White Men Using 2000–2009 National Health Interview Survey Linked Mortality Files.

Table 2 outlines the hazard ratios resulting from the unadjusted Cox proportional hazard model. Analyses reveal all-cause mortality rates are notably different between White and Black men. Specifically, the unadjusted Cox proportional hazard model revealed that Black men were 1.13 times more likely to die than White men (Hazard Ratio [HR] 1.13, 95% confidence interval or CI [1.05, 1.22]). As expected, the risk of all-cause mortality decreases as level of education increases, when controlling for other race, demographic, and health factors. Men with associate degrees or above are 28% (HR: 0.72, CI [0.68, 0.76]) less likely to experience all-cause mortality than those who did not complete high school. For high school or GED and some college, the numbers are 13% (HR: 0.87, CI [0.81, 0.92]) and 15% (HR: 0.85, CI [0.79, 0.92]), respectively.
Association Between Race and Mortality Among Non-Hispanic Black and Non-Hispanic White Men in the 2000–2011 National Health Interview Survey Linked Mortality Files.

Note. aNon-Hispanic White men were the reference group.
The adjusted Cox proportional hazard model examined all-cause mortality between Black and White men with the same level of education. The hazard ratios resulting from the adjusted model are presented in Table 3. There was no statistically significant association between race and all-cause mortality for Blacks and men who did not complete high school. Statistically significant racial disparities in all-cause mortality are present for every other level of education. Black men with a high school diploma or GED are 1.15 (CI [1.02, 1.31]) times more likely to die from any cause than equally educated White men. Among Black and White men who attended some college but did not graduate, Black men are 1.29 (CI [1.06, 1.57]) times more likely to experience all-cause mortality than White men. Lastly, Black men who obtain post-secondary education have an associated hazard ratio of 1.24 (CI [1.01, 1.52]) compared to White men with the same level of education.
Association Between Race and Morality by Education Level in Non-Hispanic Black and Non-Hispanic White Men in the 2000–2011 National Health Interview Survey Linked Mortality Files.
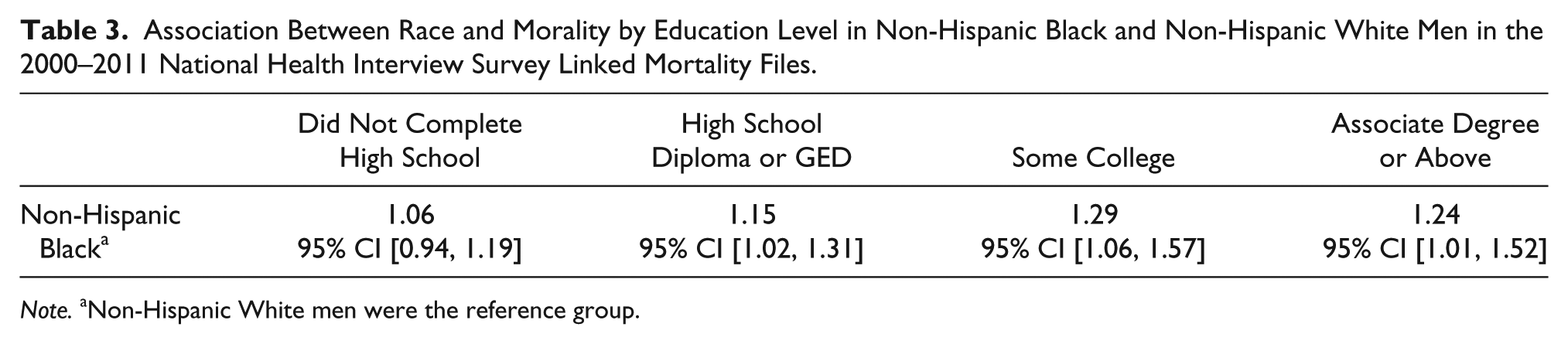
Note. aNon-Hispanic White men were the reference group.
Discussion
The goal of this study was to determine whether all-cause mortality among men with the same level of education vary by race/ethnicity. The key findings indicate racial disparities in all-cause mortality are present between men with the same levels of education. Compared to White men with the same level of education, Black men are 13% more likely to die from any cause, after controlling for age, marital status, income, insurance, drinking and smoking status, obesity and number of chronic conditions (HR: 1.13, CI [1.5, 1.22]). When looking at differences in all-cause mortality within levels of education between race/ethnicity, there are no statistically significant differences between Black men and White men who did not complete high school. At all other levels of education, Black men are more like to experience death from any cause than equally educated White men.
This study describes the association between education and all-cause mortality in Black and White men, where Black men are more likely to die from any cause than White men with the same level of education. Specifically, Black men have a higher risk of all-cause mortality than White men with the same level of education. The only exception is among men who did not complete high school. While Black men who do not complete high school still experienced an increased risk of all-cause mortality compared to White men who did not complete high school, this was not statistically significant. These findings are consistent with prior research indicating the socioeconomic benefits of education (Hummer & Hernandez, 2013; Montez et al., 2009; Montez et al., 2011; Zajacova, 2006; Zajacova & Hummer, 2009; Zajacova et al., 2012). This study implies race or ethnicity may play a larger role in all-cause mortality than previously thought, especially between Black and White men. These results confirm race differences in all-cause mortality, even when substantially reducing the potential confounding of race and education by stratifying for education. The remaining observed race difference might be a result of structural or institutional forces such as segregation, job discrimination, income inequality, wealth inequality, and differential access to housing (Hummer & Hernandez, 2013; Williams, 2015). Prior work has shown that the social and environmental conditions in which Black and White men dwell is important to consider when examining disparities in health behaviors and chronic conditions (Thorpe, Kennedy-Hendricks, et al., 2015; Thorpe, Bell, et al., 2015). An enhanced understanding of the social determinants of health may provide insight into where concerted efforts can be made to develop interventions and health-promoting strategies within specific racial/ethnic groups for the purposes of minimizing morbidity and mortality.
This study is not without its limitations. First, NHIS is a cross-sectional survey; consequently, neither causality nor temporality can be established. Further, NHIS data are self-reported and may be subject to bias. Additionally, the small sample of non-Hispanic Black men with advanced college degrees prohibited the ability to create additional strata to conduct more specific analyses. Lastly, the primary outcome is all-cause mortality. It is not possible to stratify the effects of education level on specific causes of death. Homicide, motor vehicle accidents, and suicide, among others may have different mortality rates across Black and White populations.
Despite these limitations, there are several strengths associated with this study. First, to the authors’ knowledge, this is the first study to examine all-cause mortality between Black and White men within same levels of education. Additionally, the study includes 12 years of NHIS data, which allows for a sufficiently large and diverse sample to provide reliable estimates as it relates to all-cause mortality and race by education level. Lastly, the inclusion of the covariates allows the analyses to account for confounding factors, such as health status or income, which may impact mortality.
The results of the study revealed Black men have increased risk of all-cause mortality than White men, even after controlling for potential confounders and stratifying by education level. These findings reveal socioeconomic returns to education and the societal protective mechanisms associated with education vary greatly between White and Black men. Future studies should investigate how race/ethnicity and gender relates to one’s socioeconomic position; this may help explain why differences in mortality persist even after stratifying for education.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Research conducted was supported by the National Institute on Minority Health and Health Disparities (U54MD000214) and the National Institute on Aging (K02AG059140 and R01AG054363).