
Abstract
Homophobia and biphobia negatively impact the mental health of gay, bisexual, trans, Two-Spirit, and queer men and non-binary individuals (GBT2Q) and sexual and gender minority men, but little is known about the impact of gender-related oppression. The current study examines the impact of pressure to conform to masculine norms in Canada-based GBT2Q individuals. Specifically, the associations between (a) gender expression and pressure to be masculine and (b) pressure to be masculine and depression, anxiety, and self-rated mental health were investigated. Drawing from an online national cross-sectional survey of 8,977 GBT2Q individuals and sexual and gender minority men living in Canada aged 15 years or older, 56.4% (n = 5,067) of respondents reported experiencing pressure to conform to masculine norms. Respondents were more likely to report masculine pressure if they were younger than 30 years, described their gender expression as fluid, identified their sexuality as queer, were an ethnoracial minority, and were trans. Pressure to be masculine was associated with increased odds of depression, anxiety, and reporting poor or fair mental health. The current study provides evidence of the detrimental impact of pressure to conform to masculine norms on the mental health of gay, bisexual, trans, Two-Spirit, and queer men and non-binary peoples.
Introduction
Despite significant gains in the social and legal status of gay, bisexual, trans, Two-Spirit, and queer men and non-binary (GBT2Q) people over the past three decades in Canada, GBT2Q individuals continue to face multiple mental health disparities. GBT2Q individuals experience depression, anxiety, and problematic substance use at a prevalence two to five times greater than that estimated among their heterosexual/cisgender counterparts (King et al., 2008; Plöderl & Tremblay, 2015; Ross et al., 2018). Suicidal thoughts and behaviors are also elevated in this population (Ferlatte et al., 2018; Salway et al., 2019). Gay and bisexual men are four times more likely to attempt suicide at least once during their lifetime than heterosexual men (Hottes et al., 2016). Disparities are even higher among trans and non-binary people, who experience a prevalence of depression three times greater than that among cisgender sexual minority men (Ferlatte et al., 2019). Estimates from studies conducted in 2014 (Haas et al., 2014) and 2016 (Marshall et al., 2016) suggest that 30% to 40% of trans individuals have attempted suicide at least once in their lifetime (Haas et al., 2014; Marshall et al., 2016).
Mental health disparities faced by GBT2Q individuals are not inherent to their sexual or gender identities. Rather, they are attributed to stigma, discrimination, and alienation due to their sexual and/or gender identity (Ferlatte et al., 2015). Homophobia, biphobia, and transphobia or homo-bi-trans negativity have been reported to contribute significantly to these disparities (Meyer et al., 2021; Rogers et al., 2021; Salway et al., 2018; Walch et al., 2016). In addition, gender expression, such as masculinity or femininity, plays a vital role in the experience of sexual and gender minority men, defining social interactions both inside and outside of GBT2Q communities (Pachankis et al., 2018). Gender expression, in the context of their experiences, can be described as mannerisms, attributes, and/or physical appearance that could present as masculine, feminine, or androgynous.
However, gender expression outside of heteronormative masculinity can negatively impact how GBT2Q individuals are perceived or treated (Ramos et al., 2021). In a Western heteronormative context, traditional masculinity serves as a social construct and a social determinant of health (Evans et al., 2011). GBT2Q are often perceived as less masculine and are stereotyped with female gender roles (Hunt et al., 2016). Prejudice against GBT2Q individuals has been linked to perceived violations of traditional masculinity (Salvati et al., 2021). While masculinity is highly regarded by certain GBT2Q individuals, as indicated by Sánchez et al. (2009), there are some individuals who reject or hold negative attitudes toward GBT2Q individuals who do not conform to traditional gender norms or exhibit more feminine traits (Hunt et al., 2016). GBT2Q individuals may feel pressure to conform to traditional masculine behaviors to avoid stigma and fit in within and outside of their community (Sánchez et al., 2010). Despite the significant role that gender expression plays in the mental health experiences of GBT2Q individuals, there is a lack of research investigating the relationship between gender and mental health in this population.
Research on the relationship between gender, masculine norms, and mental health among the heterogenous GBT2Q community is relatively new and limited. However, research findings suggest that those whose gender expression does not conform to societal norms and expectations of masculinity are more likely to experience elevated rates of anxiety and depression due to additional stressors (Gordon & Meyer, 2007; Pachankis et al., 2020). Gendered microaggressions, such as societal pressure to conform to gender norms and policing of gender expression, are also prevalent among GBT2Q individuals and can lead to feelings of shame and anger, which are associated with depression and anxiety (Nadal et al., 2016). Discrimination was reported to mediate the relationship between gender expression and mental distress, and gender nonconformity is associated with higher rates of discriminatory experiences and depression (Baams et al., 2013; Sandfort et al., 2007; Toomey et al., 2013). These studies highlight the need for further exploration of the connections between gender, gender norms, and mental health in GBT2Q communities, considering the impact of gender expression and pressure to be masculine on mental health outcomes.
The present study aims to address gaps in the existing literature by investigating the pressure to conform to masculine norms and its relationship with the mental health outcomes of GBT2Q individuals. While previous research has highlighted the elevated rates of anxiety and depression among individuals whose gender expression and identity deviates from social norms, studies in this area have been limited by the use of different terminologies and constructs of masculinity, with GBT2Q individuals rarely being the primary focus. Using a large sample of GBT2Q individuals living in Canada, we asked the following questions: What is the prevalence of the pressure to be masculine among GBT2Q individuals? Who is affected by this pressure among GBT2Q individuals? And what association exists between the pressure to be masculine and mental health among GBT2Q individuals? By investigating the prevalence of pressure to be masculine, identifying the groups most affected by this pressure, and examining its association with mental health outcomes, this study aims to contribute and advance understandings of the social determinants of health within GBT2Q individuals. By addressing these gaps in the knowledge, the present study hopes to inform the development of effective interventions to address mental health disparities and promote overall wellbeing in GBT2Q populations.
Materials and Methods
Data for this study were derived from Sex Now, a serial cross-sectional survey of GBT2Q individuals in Canada conducted by the Community-Based Research Centre (CBRC). The present article is a secondary data analysis that reports data collected between November 2019 and February 2020. The survey was administered online, anonymously, and in Canada’s two official languages, English and French. Consent was documented at the start of the survey via a standard consent question in SurveyMonkey. Respondents were recruited from social media platforms (e.g., Facebook, Twitter), geolocating sexual/social networking apps targeted toward GBT2Q individuals (e.g., Scruff, Grindr), pornography sites (PornHub), GBT2Q-oriented media sites (i.e., Xtra, Fugues), community groups’ newsletters, and word of mouth.
To be eligible to complete the survey, respondents had to (a) self-identify as a man or as another gender besides women (e.g., non-binary, Two-Spirit, trans man); (b) live in Canada; (c) be 15 years old or older; (d) identify as gay, bisexual, queer, or any non-heterosexual sexual identity or report having had sex with a man in the last 5 years; and (e) be able to provide informed consent and complete the questionnaire in French or English. Sex Now does not include sexual minority women; thus, we cannot study the relation between gender expression and mental health outcomes in this particular sexual minority group. All respondents who completed the perceived masculinity question and at least one of the three mental health outcomes (see the following sections for details) were retained in a total of three analytic samples. A total of 14,587 individuals started the Sex Now 2019 survey. To examine the relationship between various outcomes and the key variables of interest, different subsets were created based on the outcome of the model. Thus, the data set was subsetted for masculine pressure (N = 8,977), depression (N = 6,268), anxiety (N = 6,258), and self-rated mental health (N = 6,296). This approach allowed us to focus our analyses on each specific outcome and explore the associations with the relevant variables.
Measures
Gender Expression
Gender expression was a four-level categorical variable derived from the following question: “What is your gender expression/presentation?,” where respondents could select “Mostly feminine,” “Mostly androgynous,” “Mostly masculine,” and “Fluidity between expression.”
Pressure to be Masculine
Pressure to be masculine was derived from the following question: “I feel pressure to be perceived as masculine . . .,” (check all that apply), where respondents could select “Pressure from gay, bi, or queer men,” “Pressure from friends or family members,” “Pressure from the general society,” or “No pressure.” Respondents could check more than one of the first three options. This question was added to the Sex Now 2019 survey based on community consultations and developed with input from community members. We created a binary variable that included respondents who felt pressure to be masculine versus those who did not feel any pressure to be masculine. We also created a count or continuous variable to look at the cumulative effect of multiple sources of pressure to be masculine. This count variable was created by adding all the sources of pressure to be masculine from the question, creating a score between 0 and 3.
Mental Health Outcomes
The following mental health outcomes were measured: depression, anxiety, and self-rated mental health.
Depression was measured using the validated Patient Health Questionnaire-2 (PHQ-2), a self-report scale including two major depressive symptoms specified in the Diagnostic and Statistical Manual of Mental Disorders (5th ed.; DSM-5; American Psychiatric Association, 2013; Kroenke et al., 2003). The two items included in the PHQ-2 are “feeling down, depressed or hopeless” and “having little interest or pleasure in doing things” over the last 2 weeks. For each item of the PHQ-2, respondents rated the occurrence of the item as follows: “Not at all = 0,” “Several days = 1,” “More than half the days = 2,” or “Nearly every day = 3,” with a cumulative score ranging from 0 to 6. A score of 3 and above indicates those who are likely to suffer from depression (Kroenke et al., 2003). We created a binary variable for depression with those who scored 3 and above on the PHQ-2. The PHQ-2 demonstrated acceptable internal consistency (Cronbach’s alpha) across the sample (64.1%; 95% confidence intervals [CI] [61.2, 66.7]) (Taber, 2018).
Anxiety was measured using the validated instrument, Generalized Anxiety Disorder 2-item (GAD-2), as a brief anxiety screening measure (Kroenke et al., 2007). The GAD-2 includes the following items: “Feeling nervous, anxious, or on the edge” and “Not being able to stop or control worrying” over the last 2 weeks. The GAD uses the same scoring scale as the PHQ-2, with a score of 3 and above used to identify probable cases of anxiety (Kroenke et al., 2007). We created a binary variable for anxiety with those who scored 3 and above on the GAD-2. The GAD-2 also demonstrated acceptable internal consistency (Cronbach’s alpha) across the sample (62.5%; 95% CI [59.7, 65.4]) (Taber, 2018).
Self-rated mental health was measured using a five-point scale question where respondents reported their overall mental health (Mawani & Gilmour, 2010) with the following question: “In general, how would you say your mental health is?” We created a binary variable to group “Fair; Poor” versus “Excellent; Very Good; Good.”
Sociodemographic Variables
Respondents self-reported the following social-demographic variables, which were treated as explanatory variables and as potential confounders for the analysis: age (in years), gender identity (“What is your gender identity?”), sexual orientation (“How do you identify sexually? [check all that apply]”), ethnoracial identity (“Which of these do you identify with? [check all that apply]”), income (“What was your income in the last year?”), education (“What is the highest level of education that you completed?”), trans experience (“Do you have trans experience? [i.e., your gender is different than the sex you were assigned at birth]”), disability identity (“Do you identify as a person with a disability?”), province (“What province or territory do you currently live in?”), and living environment (“What best describes the environment you live in?”). For sexual identity, respondents were given the option to select multiple sexual identities; owing to collinearity, respondents were categorized as those who were (a) only gay; (b) only bisexual; (c) only pansexual; (d) only queer; and (e) all others. Respondents were given the option to select multiple racial/ethnic identities for ethnicity. Identities were categorized again, owing to collinearity according to the following classification: Indigenous = any Indigenous identity, including those who are indigenous and identified with another ethnoracial category; ethnoracial minority = any identity other than indigenous and white, including those who identified with a minoritized ethnoracial identity and white, thus multiethnic; and only white.
Analyses
Analyses were conducted in three parts. (a) First, we examined the sociodemographic factors associated with pressure to be masculine. (b) Then, we examined the associations between pressure to be masculine and mental health outcomes and sociodemographic factors and mental health outcomes. (c) Finally, we hypothesized a compounding effect of pressure to be masculine from multiple sources and its relationship with mental health outcomes. To test this, we measured the associations between the count of pressure to be masculine indicators and mental health outcomes. Counts and percentages were reported to summarize demographic variables across the masculine pressure and three mental health outcome variables. We used bivariate logistic regression models to test relationships and calculated 95% CI for all odds ratios. Multivariable logistic regression models were estimated for each outcome, adjusted for potential confounders, including age, gender identity, gender expression, sexual identity, ethnoracial identity, annual income, living environment, trans experience, and disability. We ruled out multicollinearity by verifying variance inflation factors did not exceed four (E. Harrison & Riinu, 2020). The best-fitting model and inclusion of variables were selected based on the results of unadjusted analyses and the Akaike Information Criterion (AIC) (E. Harrison & Riinu, 2020). We interpreted results based on direction and magnitude of association. We used R Studio 1.3.1073 to conduct all analyses.
Ethics
The original Sex Now 2019 study was reviewed and approved by the research ethics board at the University of Victoria and University of British Columbia (BC17-487). This secondary analysis was reviewed and approved by the comité d’éthique de la recherche en sciences et en santé (CERSES) of the Université de Montréal (CERSES-2021-1164).
Results
The majority (56.4%, 95% CI [55.4, 57.4]) of respondents reported feeling pressure to be masculine from at least one category examined (i.e., society; friends and family; and the gay, bi, or queer community). Felt pressure to be masculine from the general society was the most common source of pressure to be masculine (49.1%, 95% CI [48.1, 50.1]), followed by friends and family (27.6%, 95%CI 26.7, 28.5) and then the GBT2Q community (24.1% (95% 23.3, 25.0).
Table 1 presents bivariate and multivariable associations between felt pressure to be masculine and demographic variables. Those who identified their gender as fluid had significantly higher odds of felt pressure to be masculine (adjusted odds ratio [AOR] 1.58; 95%CI [1.30, 1.91]) than those who identified as (mostly) masculine. Androgynous gender expression was also associated with higher odds of felt pressure to be masculine compared to selecting masculine gender expression (AOR 1.46; 95% CI [1.08, 2.00]). Queer respondents (AOR 2.70; 95% CI [2.28, 3.20]), those under 30 years of age (AOR 3.98; 95% CI [3.45, 4.58]), those being from an ethnoracial minority group (AOR 1.22; 95% CI [1.06, 1.41]), those with trans experience (AOR 1.64; 95% CI [1.27, 2.12]), and those who identified as disabled (AOR 1.24; 95% CI [1.05, 1.47]) had higher odds of felt pressure to be masculine. In contrast, those without a college or university degree had lower odds of felt pressure to be masculine than those with a degree (AOR 0.80; 95% CI [0.70, 0.92]).
Association Between Socio-Demographic Variables and Pressure to be Masculine

Note. Full models used the same analytic sample that was subsetted for the appropriate outcomes. AOR comparing outcome of masculine pressure to that of referent group. OR = odds ratio; CI = confidence interval; AOR =djusted odds ratio;; CAD = Canadian Dollars. Bold values indicate significant results (p<0.05).
Percentage calculated using column total as denominator.
Percentage calculated using row total as denominator.
Adjusted for age, gender identity, gender expression, sexual identity, ethnicity, annual income, residence, trans experience, and disability.
Models in Table 2 present the odds ratios for the association between felt pressure to be masculine and mental health outcomes, which include depression, anxiety, and poor/fair self-rated mental health. The bivariate models showed that those who felt pressure to be masculine had significantly higher odds of mental health outcomes (depression OR 2.04, 95% CI [1.79, 2.34]; anxiety OR 2.21, 95% CI [1.96, 2.50]; poor/fair self-rated mental health OR 2.24, 95% CI [1.99, 2.52]). Overall, after adjusting for sociodemographic confounders, respondents who had experienced pressure to be masculine still had an increased odds of negative mental health outcomes compared with those reporting no pressure (depression AOR 1.50, 95% CI [1.29, 1.76]; anxiety AOR 1.56, 95% CI [1.34, 1.79]; poor/fair self-rated mental health AOR 1.59, 95% CI [1.39, 1.83]).
Associations Between Pressure to be Masculine and Negative Health Outcomes and Health Behaviors

Note. Full models used same analytic sample that was subsetted for the appropriate outcomes. OR = odds ratio; CI = confidence interval; AOR = adjusted odds ratio. Bold values indicate significant results (p<0.05).
Percentage calculated using column total as denominator.
Adjusted for pressure to be masculine, age, gender identity, gender expression, sexual identity, ethnoracial identity, annual income, residence, trans experience, and disability.
Differences in negative mental health outcomes (depression, anxiety, poor/fair self-rated mental health) were similar in direction and statistical significance to one another (Supplemental Material Tables 1–3). However, there were some differences observed between the depression model and the anxiety model. None of the categories of gender expression had a significant association with anxiety. In addition, differences were noted in the comparison between the model with depression as an outcome and the model with poor/fair self-rated mental health. Respondents who expressed fluidity between expressions had higher odds of poor/fair self-rated mental health than those who identified as mostly masculine, and those whose sexual identity was pansexual, queer, or something other than gay, bisexual, pansexual, or queer had higher odds of poor/fair self-rated mental health than those who identified as gay.
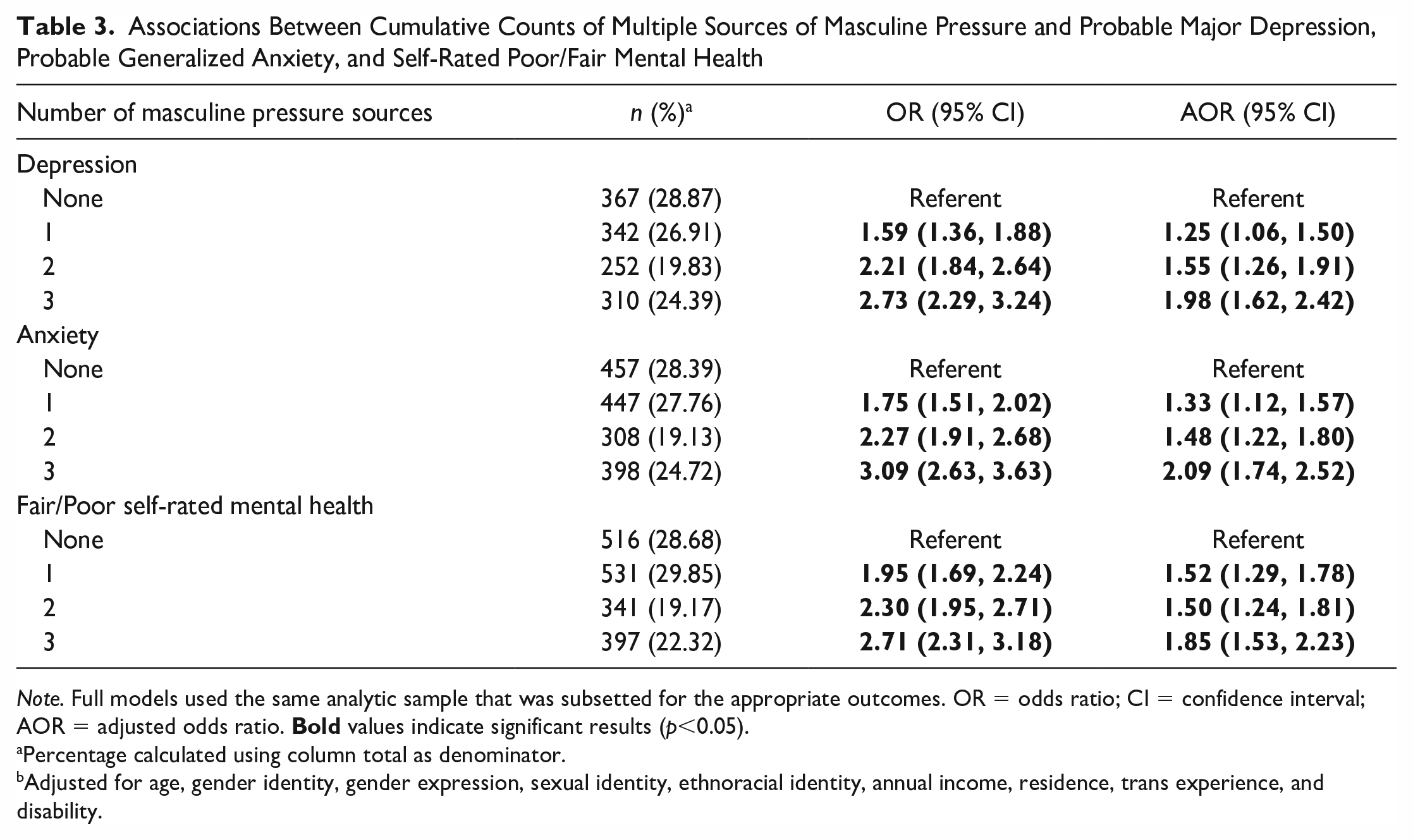
Table 3 shows the bivariate and multivariate relationships between multiple sources of felt pressure to be masculine on three mental health outcomes (depression, anxiety, and self-rated fair/poor mental health). The three multivariable models were adjusted for with the same sociodemographic variables used in the multivariable models in Table 2. Compared with respondents not reporting any felt pressure to be masculine, respondents reporting increasing numbers of forms of pressure to be masculine were at increased odds of depression (1 source of pressure AOR 1.25, 95% CI [1.06, 1.50]; 3 sources of pressure AOR 1.98, 95% CI [1.62, 2.42]), anxiety (1 source of pressure AOR 1.33, 95% CI [1.12, 1.57]; 3 sources of pressure AOR 2.09, 95% CI [1.74, 2.52]), and fair/poor self-rated mental health (1 source of pressure AOR 1.52, 95% CI [1.29, 1.78]; 3 sources of pressure AOR 1.85, 95% CI [1.53, 2.23]).
Associations Between Cumulative Counts of Multiple Sources of Masculine Pressure and Probable Major Depression, Probable Generalized Anxiety, and Self-Rated Poor/Fair Mental Health
Note. Full models used the same analytic sample that was subsetted for the appropriate outcomes. OR = odds ratio; CI = confidence interval; AOR = adjusted odds ratio. Bold values indicate significant results (p<0.05).
Percentage calculated using column total as denominator.
Adjusted for age, gender identity, gender expression, sexual identity, ethnoracial identity, annual income, residence, trans experience, and disability.
Discussion
This study demonstrates that three in five of GBT2Q individuals in a Canadian community-based survey have felt pressure to be masculine. General society was the most common source of felt pressure, followed by friends and family and other GBT2Q community members. Certain demographic factors were associated with higher odds of feeling this pressure, including identifying as gender fluid, having an androgynous gender expression, being queer, being under 30 years of age, being from an ethnoracial minority group, having trans experience, and identifying as disabled. GBT2Q individuals who felt pressure to act or be more masculine also had higher odds of depression, anxiety, and fair/poor (vs. good/excellent) self-reported mental health. Respondents who received pressure from multiple sources had a dose-response increasing odds of negative mental health outcomes compared with those who experienced no pressure. Of note, GBT2Q individuals who considered their gender presentation as androgynous or fluid (vs. masculine gender presentation) reported higher odds of experiencing pressure to be masculine and poorer mental health outcomes. Overall, the study findings highlight the significant impact of feeling pressure to conform to masculine norms on the mental health of individuals, underscoring the need for inclusive and supportive environments that challenge societal expectations and foster wellbeing among individuals with diverse gender identities/expressions.
The concept of “hegemonic masculinity” (Connell & Messerschmidt, 2005) offers a way to interpret our findings. Hegemonic masculinity is a dominant and socially prized form of masculinity that is idealized in most Western countries, including Canada. This cultural ideal emphasizes heterosexuality, competitiveness, strength, power, and control (McVittie et al., 2017), positioning men and masculine ideals as dominant over marginalized men and women and feminine practices (Connell & Messerschmidt, 2005; Staiger et al., 2020). GBT2Q individuals are subordinated by society within this hierarchy of masculinity, which can lead to increased pressure to pass as masculine and align with elements of hegemonic masculinity (McVittie et al., 2017). Our study shows that such pressures can manifest significant risks to mental health, including anxiety and depression. These findings align with previous research that has linked such pressure with substance use, resistance to help-seeking, concealment, and internalizing distress (Oliffe et al., 2020; Oliffe & Phillips, 2008; Seidler et al., 2016). While such gendered tensions have long been reported in mixed and straight male samples (Creighton & Oliffe, 2010; Fleming & Agnew-Brune, 2015; Fleming et al., 2014), the current study highlights the potential mental health risks specifically for GBT2Q.
This study is one of the few studies to measure the association of felt pressure to be masculine with mental health outcomes among GBT2Q individuals and demonstrates the importance of further research on the topic. Some authors have tried to explain the link between the expression of masculinity and mental health outcomes. For example, O’Neil et al. (1986) brought the gender role conflict (GRC) as a psychological state of mind in which men were socialized but could negatively impair their mental health. This concept occurs when “rigid, sexist, or restrictive gender roles result in personal restrictions, deviations, or violations of others or oneself” (O’Neil et al., 2017, p. 75). This could be particularly problematic in the case of GBT2Q individuals. Being part of a socially disadvantaged group brings significant challenges and stresses to heighten the risk of mental health issues (Schwartz & Meyer, 2010). Accordingly, our findings suggest the pressure to act/feel masculine should be examined as a determinant of GBT2Q individuals’ health and wellbeing alongside other stressors related to sexuality-based discrimination (Meyer, 2003).
Our findings reveal significant within-group differences, with some GBT2Q subgroups reporting elevated odds of pressure to be masculine, which varied by age, ethnicity, trans experience, disability status, and education level. This highlights the need to understand how masculinities intersect with other social determinants of health (Evans et al., 2011). Previous research reported that younger GBT2Q individuals face an elevated level of sexuality-based discrimination and prejudice (Ferlatte et al., 2014). Similarly, we reported that young GBT2Q individuals were more likely to report masculine pressure than older respondents. This could be due to GRC, which inhibits psychological development and results in tension for young GBT2Q individuals grappling with their gender identity(O’Neil, 2008; O’Neil & Renzulli, 2013; Pleck, 1981, 1995). In addition, younger GBT2Q individuals are especially prone to gender policing in their formative years, which can lead to increased pressure to conform to dominant masculine norms (Brake, 1999; Chambers et al., 2004; Mora, 2013; Payne & Smith, 2016). The developmental collision theory, a theory which posits that young GBT2Q individuals today experience greater visibility and inclusion, leading to some tensions related to developmental processes that all young people experience and GBT2Q identiy formation can somewhat explain their interpretation (Russell & Fish, 2019). The potential impact of coming out earlier in life is exposing GBT2Q individuals to a longer period of violence from masculine pressure.
Our results showed that trans respondents experienced more pressure to be masculine, likely due to gender minority stress caused by discrimination and microaggressions (Abbot et al., 2016). Trans individuals may face barriers to expressing their gender identity and often expect rejection in public spaces, leading to the concealment of their gender identity (Rood et al., 2016). Misgendering, or the misclassification of gender, is a significant minority stressor for transgender people and has been linked to psychological distress (McLemore, 2018). To claim masculinities, trans men often exhibit actions traditionally associated with being a man (Phillips & Rogers, 2021). The pressure to perform and pass as masculine may be a safety strategy to avoid trans-related violence and aggression (Abelson, 2014; B. F. Harrison & Michelson, 2019; Lee & Kwan, 2014) and may reflect a response to heightened anxiety caused by expected prejudiced events (Anzani et al., 2022). Thus, in our study, the pressure to perform and pass as typically masculine may reflect a safety strategy that reduced the potential for more lethal forms of masculinity—aggression and violence toward those deemed not masculine or, worse still, feminine. The theory of gender and health (Todd et al., 2022) can serve as a framework for understanding the unique experiences of transmasculine individuals in relation to gender identity and masculinity and can guide the development of interventions that promote health behaviors aligned with an individual’s gender identity.
Another important observation from our results was that respondents who reported their gender expression as androgynous were reported to have elevated rates of masculine pressures and negative mental health outcomes. It has been previously hypothesized that androgynous individuals are more psychologically adaptive because they aptly alternate between masculine and feminine gender roles (Juster et al., 2016; Prakash et al., 2010). However, our results suggest the opposite. Previously it was hypothesized that psychological androgyny is when individuals perceive the self to pose characteristics of both genders. It develops in people who experience little pressure to conform to gender stereotypes (Andersen & Bem, 1981). Another important observation to note is that respondents who reported their gender expression as androgynous seem more affected by the pressure to be masculine than those who reported their gender expression as feminine. There were very few respondents (1.83%) whose gender expressed as feminine. This could be potentially due to a potentially reverse relationship happening in that those respondents who felt pressure to be masculine then marked themselves down to be mostly masculine, even though they could be concealing some identity constructs that are outside the masculine norm.
Our study had limitations, including using a single item to measure felt masculine pressure and gender expression and not measuring enacted masculinity. Although, three different sources of pressure were evaluated. Our results cannot be used to infer whether respondents would act on this pressure. Moreover, the definition of pressure to be masculine remains still poorly understood and vaguely defined in the literature. This lack of clarity may impact the interpretation of our findings and limit their generalizability. In addition, important confounders such as religious affiliation were unmeasured and have been shown to influence gender norms and expression (Barnes & Meyer, 2012). Third, while this survey employed multiple recruitment strategies (e.g., social media, internet websites), the convenience sample limits the generalizability of the findings to the wider Canadian GBT2Q populations.
GBT2Q individuals commonly face pressure to conform to masculine gender norms, which can lead to negative mental health outcomes. To address this issue, several key recommendations should be implemented in future research, policies, and programs. First, further scholarship is needed to improve our understanding of how gender and masculinity affect the health of GBT2Q individuals. Second, longitudinal research should be conducted to explore the complex relationships between masculine pressure, homophobia/biphobia, femmephobia, and other forms of stigma, with a focus on vulnerable subgroups. Third, programs and services should be tailored to meet the unique needs of those affected by masculine pressure and associated mental health issues, such as trans people, GBT2Q youth, and individuals who express their gender as androgynous or fluid. Finally, more research is necessary to examine how masculine pressure functions as a social determinant of mental health among GBT2Q. This research should include an examination of hegemonic masculinity within the GBT2Q communities and should acknowledge and validate some masculine values in GBT2Q. By implementing these recommendations, we can promote the health and wellbeing of GBT2Q individuals affected by masculine pressure.
Conclusion
The current study provides evidence of a negative association between experiencing pressure to be masculine and mental health outcomes (depression, anxiety, self-rated mental health) among sexual and gender minority individuals living in Canada. Our study shows that a majority of GBT2Q individuals feel the pressure to be masculine. Our study also supports the further examination of the inclusion of masculine pressure as a social determinant of mental health among GBT2Q individuals. Findings could support the development of a possible intervention to alter norms and reduce pressure to improve the mental health outcomes of GBT2Q individuals. As masculine pressure remains poorly explored as a determinant of GBT2Q individuals’ mental health, more theoretical and empirical work is needed to advance scholarly understanding of the complexities that underline the trends identified in this article and the perception of masculine pressure.
Supplemental Material
sj-docx-1-jmh-10.1177_15579883231206618 – Supplemental material for Conformity to Masculinity Norms and Mental Health Outcomes Among Gay, Bisexual, Trans, Two-Spirit, and Queer Men and Non-Binary Individuals
Supplemental material, sj-docx-1-jmh-10.1177_15579883231206618 for Conformity to Masculinity Norms and Mental Health Outcomes Among Gay, Bisexual, Trans, Two-Spirit, and Queer Men and Non-Binary Individuals by Sarah Cooper, Tristan Péloquin, Nathan J. Lachowsky, Travis Salway, John L. Oliffe, Benjamin Klassen, David J. Brennan, Janie Houle and Olivier Ferlatte in American Journal of Men's Health
Footnotes
Acknowledgements
The authors are extremely grateful to the thousands of individuals who took the time to complete the survey and as such helped to strengthen GBT2Q health in Canada and beyond.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Sex Now 2019 received funding support from Canadian Blood Services MSM Research Fund, funded by the federal government (Health Canada) and the provincial and territorial ministries of health. The views herein do not necessarily reflect the views of Canadian Blood Services or the federal, provincial, or territorial governments of Canada. This secondary analysis was supported by a grant from the Pôle d’expertise et de recherche en santé et bien-être des hommes. Dr. Lachowsky was supported by a Michael Smith Foundation for Health Research Scholar Award (#16863). Dr. Oliffe is supported by a Tier 1 Canada Research Chair in Men’s Health Promotion. Dr. Ferlatte is supported by a Junior 1 research scholar award from the Fonds de Recherche du Québec—Santé.
Data Availability Statement
Partial Sex Now data are publicly available on the Our Stats dashboard (![]() ). The University of Victoria’s Human Research Ethics Board has only approved storage of our data on secure university servers since the data contain potentially sensitive information about study participants. Data are available on request through secure university servers only. Any requests to access the data can be made to the Sex Now Principal Investigator, Dr. Nathan Lachowsky (250-472-5739 or
). The University of Victoria’s Human Research Ethics Board has only approved storage of our data on secure university servers since the data contain potentially sensitive information about study participants. Data are available on request through secure university servers only. Any requests to access the data can be made to the Sex Now Principal Investigator, Dr. Nathan Lachowsky (250-472-5739 or
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.