
Abstract
The aim of this study was to examine the influences of internalized homophobia on Chinese gay and bisexual men’s quality of life and life satisfaction. Four hundred and eighty-three participants completed the Internalized Homophobia Scale, Chinese SF-12 Health Survey Version 2, and Satisfaction With Life Scale via the Internet. Scores for quality of life in several domains and life satisfaction were significantly lower than the heterosexuals’ norm scores. The present study revealed that internalized homophobia significantly negatively correlated with the mental component summary score and life satisfaction. The mental component summary score mediated the relationship between internalized homophobia and life satisfaction. Sexual orientation moderated the relationship between internalized homophobia and mental component score. Gay and bisexual men in China experience poorer quality of life and less satisfaction with life compared to heterosexuals, and internalized homophobia contributes to both.
The topic of sexual minorities has been a long-standing and important research issue. Researchers have revealed that, compared with heterosexual populations, sexual minorities are associated with increased negative outcomes, including mental health problems and bodily disorders, and they experience poorer health and lower life satisfaction and well-being (Cochran & Mays, 2007; Conlin, Douglass, & Ouch, 2019; Jackson, Hackett, Grabovac, Smith, & Steptoe, 2019; Newcomb & Mustanski, 2010; Powdthavee & Wooden, 2015; Vera-Villarroel, Valtierra, & Contreras, 2016). Psychologists have developed several theoretical explanations for this phenomenon. Some researchers have suggested that sexual minorities might experience cognitive and emotional conflicts because of their differences from heterosexuals as well as confusion about their sexual orientation (Feinstein, Meuwly, Davila, Eaton, & Yoneda, 2015). Meyer (2003) also developed a minority stress model and attempted to determine the proximal and distal risk factors that lead to health-related stress.
Furthermore, numerous studies have reported that sociodemographic (e.g., sexual orientation, sex role, education, income, religion, and race), psychological (e.g., gender role, self-esteem, social support, and violence), and social/cultural variables (discrimination, prejudice, and piety) are closely related to sexual minorities’ health status and life satisfaction (Lazarevic, Holman, Oswald, & Kramer, 2015; Lo, Kim, Small, & Chan, 2019; Mendoza-Perez & Ortiz-Hernandez, 2019; Meyer, 2003; Perales, 2018; Pollitt, Mallory, & Fish, 2018; Powdthavee & Wooden, 2015; Shangani, Gamarel, Ogunbajo, Cai, & Operario, 2019; Starr & Zurbriggen, 2017; Steward, Miege, & Choi, 2013; Wang et al., 2019). In particular, bisexuals are at double the risk of experiencing prejudices from both homosexuals and heterosexuals and have a higher likelihood to develop health problems than homosexuals and heterosexuals do (Balsam & Mohr, 2007). Additionally, masculine traits as well as homosexuals/bisexuals who identify themselves as tops and who behave and are perceived as masculine have been consistently linked with better mental health than feminine traits as well as those who identify themselves as bottoms and who behave and are perceived as feminine (Carlson & Steuer, 1985; Gonzalez, Bockting, Beckman, & Durán, 2012; Leung & Moore, 2003). African American and Latino sexual minorities and those with lower education or with less income have also been closely associated with lower mental health and well-being (Powdthavee & Wooden, 2015; Shangani et al., 2019).
Internalized Homophobia and Mental and Physical Health
Based on the minority stress model, previous studies have revealed that stigma, discrimination, and prejudice due to non-prototypical sexual orientation create “minority stress” and a hostile social environment as well as contribute to adverse health outcomes (Jackson et al., 2019; Meyer, 2003). Internalized homophobia (i.e., negative feelings about one’s own sexual orientation resulting from the internalization of antigay stigma and prejudice) is a key source of stress for sexual minorities that can lead to greater risk for mental health disorders and other negative outcomes (Herek, 2004; Meyer, 2003). For example, research has suggested a significant correlation between internalized homophobia and mental health such as anxiety, depression, and suicidal ideation (Newcomb & Mustanski, 2010; Vera-Villarroel, Valtierra, & Contreras, 2016; Xu, Zheng, Xu, & Zheng, 2017). Internalized homophobia contributed to physical health disorders including eating orders and sexual dysfunction (erectile dysfunction or premature ejaculation; Kuyper & Vanwesenbeeck, 2011; Newcomb & Mustanski, 2010). Sexual minorities are increasingly reporting higher rates of physical health problems such as HIV, sexually transmitted infections (STIs), and other physical health disparities (Cochran & Mays, 2007; Hatzenbuehler, Nolenhoeksema, & Erickson, 2008).
Internalized Homophobia and Health in Chinese Sexual Minority Men
Chinese gay and bisexual men have reported greater internalized homonegativity, compared to American gay men over the years (Mohr & Fassinger, 2000; Zheng & Zheng, 2016). The reasons are manifold; however, the leading cause of this phenomenon may be related to Chinese traditional culture and public opinions about sexual minorities (Choi, Steward, Miège, Hudes, & Gregorich, 2016; Xu et al., 2017). The dominant childbearing beliefs in China attach importance to male offspring and continuity of bloodlines, while sexual minorities are less likely to have children. This could induce psychological conflict between individual desires and social values. In China, as well as some other cultures around the world, homosexuality can be viewed as immoral and unacceptable, and the image of gay and bisexual men may be negative due to their sexuality being associated with HIV and other STIs (Xu et al., 2017). Sexual minority men may experience prejudice and discrimination, which could lead to feeling pressure from society and the experience of stress (Pyun et al., 2014).
Evidence has revealed that gay and bisexual men in China have a high level of internalized homophobia and individuals with high internalized homophobia are more likely to report psychological distress (e.g., anxiety, depression, and suicide attempts), unprotected sex, sexual compulsivity, and having female sexual partners (Boone, Cook, & Wilson, 2016; Xu et al., 2017). Internalized homophobia has been linked to high rates of STIs, because participants with high internalized homophobia are more reluctant to be tested for HIV despite their knowledge of the risks of unprotected sex (Pyun et al., 2014).
Internalized Homophobia and Quality of Life
Quality of life has been an increasing research focus in studies on sexual minority populations, and several studies have confirmed that lesbian, gay, and bisexual (LGB) individuals have a poorer quality of life (Cochran & Mays, 2009; Horowitz, Weis, & Laflin, 2001). For example, Træen, Martinussen, Vittersø, and Saini (2009) conducted an extensive investigation from several countries and suggested LGB individuals had a lower score on quality of life compared to heterosexuals.
According to World Health Organization guidelines, any reference to quality of life must include a person’s physical and mental state (including positive and negative feelings), social relationships, environment, religion, beliefs, and opinions (Kreis et al., 2015; Vera-Villarroel, Valtierra, & Contreras, 2016). Research has suggested that sexual minority individuals experienced negative events and had lower scores for mental health, physical health, and sociability (Cochran & Mays, 2007; Meyer, 2003). Internalized homophobia may play a crucial role in this process. Previous studies have demonstrated that participants with high internalized homophobia were at increased risk for internalizing mental health problems such as anxiety, depression, and substance use–related morbidity and suicide attempts compared to exclusively heterosexual women and men (Cochran & Mays, 2000; Hatzenbuehler, Mclaughlin, & Nolenhoeksema, 2008; Newcomb & Mustanski, 2010).
Research has revealed conflicting results regarding the relationship between internalized homophobia and physical health. Some studies demonstrated that sexual minority individuals suffered from poor physical health. For example, higher levels of internalized homophobia had a significant association with experiencing sexual problems (Szymanski & Carr, 2008). Many gay/bisexual men reported orgasmic disorder, erection difficulties, and rapid ejaculation (Bancroft, Carnes, Janssen, Goodrich, & Long, 2005). Research has also reported a relationship between internalized homophobia and substance use, eating disorders, high-risk sexual behaviors, and syndemic production (Hatzenbuehler, Nolenhoeksema, & Erickson, 2008; Kuyper & Vanwesenbeeck, 2011; Xu et al., 2017). Several studies suggested that the association between internalized homophobia and physical health was not significant (Frost, Lehavot, & Meyer, 2015). Forst and his colleagues revealed that individuals’ internalized homophobia was not associated with either externally rated physical health problems or lifetime physical health diagnoses, while it was closely related to one’s self-appraised physical health.
Internalized Homophobia and Life Satisfaction
Another domain that has attracted researchers’ attention is life satisfaction (and subjective well-being generally; Cummins, 2013). As a subjective assessment of the individuals’ overall well-being, evidence demonstrated that homosexuals were significantly less likely to report being “fairly or very happy” than heterosexuals in an Adult Psychiatric Morbidity Survey (Bachmann & Simon, 2014; Chakraborty, Babu, & Sarma, 2011). Other considerable research has provided evidence of sexual minorities as being at greater risk of low levels of well-being (Lazarevic et al., 2015; Luhtanen, 2003).
There is considerable research suggesting that internalized homophobia can affect the life satisfaction of LGB people in a variety of ways. Although research indicated that social support (e.g., close friendship, family acceptance) could effectively reduce minority stress and improve life satisfaction and psychological well-being, gay and bisexual individuals have few friends and lack support from peers (Domínguez-Fuentes, Hombrados-Mendieta, & García-Leiva, 2012; Gillespie, Frederick, Harari, & Grov, 2015; Lazarevic et al., 2015). Gay and bisexual individuals may conceal their sexual orientation to maintain face and harmony within the family, which can lead to greater stress and less life satisfaction (Hu, Wang, & Wu, 2013; Powdthavee & Wooden, 2015; Zang, Guida, Sun, & Liu, 2014). Good self-esteem is a prerequisite for a happy life, and individuals with high internalized homophobia experience more negative stereotypes and have relatively lower self-worth. Finally, this would affect one’s life satisfaction (Bachmann & Simon, 2014).
Several studies have endeavored to ascertain the relationship between health and life satisfaction. Past research has consistently reported strong relationship between health and life satisfaction (Carver, Scheier, & Segerstrom, 2010; Mannix, Feldman, & Moody, 2009). Research revealed that happier people and those who were more satisfied with their lives at baseline reported better health (self-rated health; an absence of limiting, long-term conditions; and physical health; Siahpush, Spittal, & Singh, 2008). As previously mentioned, internalized homophobia can reduce not only an individual’s quality of life and life satisfaction directly but also indirectly through other variables. Quality of life as an objective assessment of individuals’ survival system includes their mental, physical, and social state, which are related to their life satisfaction. It is essential to explore the relationships among these three variables and construct a path model.
The Present Study
Few studies have examined the quality of life of Chinese gay and bisexual men. Previous studies of Chinese gay and bisexual men on quality of life have tended to investigate special populations (e.g., individuals infected with HIV) rather than healthy individuals, while other studies investigated gay and bisexual men in specific states (south of China or one or two provinces; Hidru et al., 2016; Zhu, Liu, Qu, Hu, & Zhang, 2016). Neither of these types of studies examined the associations between internalized homophobia and quality of life. Internalized homophobia is a key component of sexual minority stress, and the effect that it has demands research attention. Thus, the present study was particularly concerned with the quality of life of Chinese gay/bisexual men, including basic health status and the influence of certain demographic variables on quality of life as well as the influences of internalized homophobia on Chinese gay and bisexual men’s quality of life and life satisfaction. In addition, life satisfaction has been defined as a cognitive evaluation of the quality of one’s overall life (Pavot & Diener, 1993). This study also examined the mediating effect of quality of life on the relationship between internalized homophobia and life satisfaction.
Method
Participants and Procedures
The present study used a network investigation and designed an electronic Web-based questionnaire using the professional survey website Wenjuanxing (www.sojump.com). Participants were recruited using advertisements on QQ (one of the most popular instant messaging softwares), Blued, Zank application software (two popular gay social software applications in China), and Baidu Tieba (the largest Chinese community online).
A total of 528 participants completed the questionnaire. The inclusion criteria used were male, age 18 years or older, and gay or bisexual (self-reported gay/bisexual). To ensure the validity and reliability of the data, a method similar to that used by Bauermeister et al. (2012) was adopted in this study. As a result, 45 participants were removed because of their age (younger than 18 years) or response time (less than 7 min). Subsequently, 483 participants were eligible for inclusion in this study. Out of these, 358 cases were identified as valid because they provided a unique and valid e-mail address (and without the same username) to receive the research results. The remaining 125 cases that seemed suspicious were also determined as valid after they passed a lie detector check. The mean age of the sample was 28.55 years (range 18–51).
Measures
Demographic characteristics
Participants were asked about their age, sexual orientation, sexual role, education, marital status, occupation, monthly salary, nation, religion, geographic location, and whether they were single children. The details of the social and demographic variables are provided in Table 1.
Scores for Each Dimension of QOL and LS According to the Demographic Characteristics.

Note. QOL = quality of life; PCS = physical component summary; MCS = mental component summary; LS = life satisfaction.
p < .05. **p < .01. ***p < .001.
Internalized homophobia
Internalized homophobia was assessed with the Revised Internalized Homophobia Scale (IHP-R) that assesses gay/bisexual individuals’ attitudes toward their sexual orientation (Herek, Cogan, Gillis, & Glunt, 1998; Meyer, 1995). The original version consists of nine items. The current study used a five-item version of the IHP-R that was better suited for administration to bisexuals and lesbians as well (Herek, Gillis, & Cogan, 2008). Sample items include “I wish I weren’t gay/bisexual” and “If someone offered me the chance to be completely heterosexual, I would accept the chance.” Participants responded to items on a 5-point Likert scale where 1 = strongly disagree and 5 = strongly agree. Higher scores indicated higher levels of internalized homophobia. In the present sample, internal consistency reliability for the five-item IHP-R scale was .86.
Quality of life
Quality of life was assessed with the Chinese SF-12 Health Survey Version 2 (SF-12v2; Lam, Wong, Lam, Lo, & Huang, 2010; Lam, Lam, Fong, & Huang, 2013). This scale was a short version of the SF-36 (The 36-Item Short Form Health Survey) and consisted of 12 items measuring eight quality of life domains, namely, physical functioning (PF), role-physical (RP), bodily pain (BP), general health (GH), vitality (VT), social functioning (SF), role-emotional (RE), and mental health (MH). The eight domains could be divided into two dimensions: the physical component summary (PCS) and the mental component summary (MCS; Maruish, 2012). The domain scores were calculated by summation of the relevant item responses and transformation into a standardized score ranging from 0 to 100 (with a mean score of 50 and a standard deviation of 10). Higher scale scores indicated higher levels of quality of life. The reliability of the Chinese (Hong Kong) version of the SF-12v2 was good in this study (Cronbach’s α = .76).
Life satisfaction
Life satisfaction was defined as a global measure of an individual’s contentment with life (Diener, Emmons, Larsen, & Griffin, 1985). The Satisfaction With Life Scale (SWLS) was used to assess participants’ general satisfaction with life (Pavot & Diener, 2009). The SWLS consisted of five items that are rated on a 7-point Likert scale where 1 = strongly disagree and 7 = strongly agree, with higher scores indicating greater life satisfaction. The Cronbach’s α in the present study was .84.
Data analysis
Data were analyzed using IBM SPSS 21.0 and Mplus 7.0. Descriptive statistics, t test, and one-way analysis of variance (ANOVA) were used to analyze the differences among participants on the study variables. Correlation analysis were used to analyze the relationships between internalized homophobia, life satisfaction, and quality of life using Pearson correlations. Regression analysis was used to explore the fitness of the hypothesized model in explaining the associations among internalized homophobia (as the independent variable), quality of life (as the mediator), and life satisfaction (as the dependent variable) as well as the sexual orientation and sex role (as the moderators).
Results
Table 2 presents the means and standard deviations of the health-related quality of life scores. The SF-12 v2 scores of the participants were compared with gender-adjusted population norms (Lam et al., 2010, 2013). Significant differences were found in role-physical, vitality, social functioning, social functioning, and mental health (p < .05 for all). There was no significant difference in the physical component summary score (p > .05), whereas the score for gay and bisexual men was significantly lower than the norm for the mental component summary (p < .001). The score for life satisfaction for gay and bisexual men was also significantly lower than the score for heterosexual adults (p < .001).
Comparison of Scores (M ± SD) of Dimensions of SF-12v2 and Life Satisfaction Between Subjects and Norm (Heterosexuals).
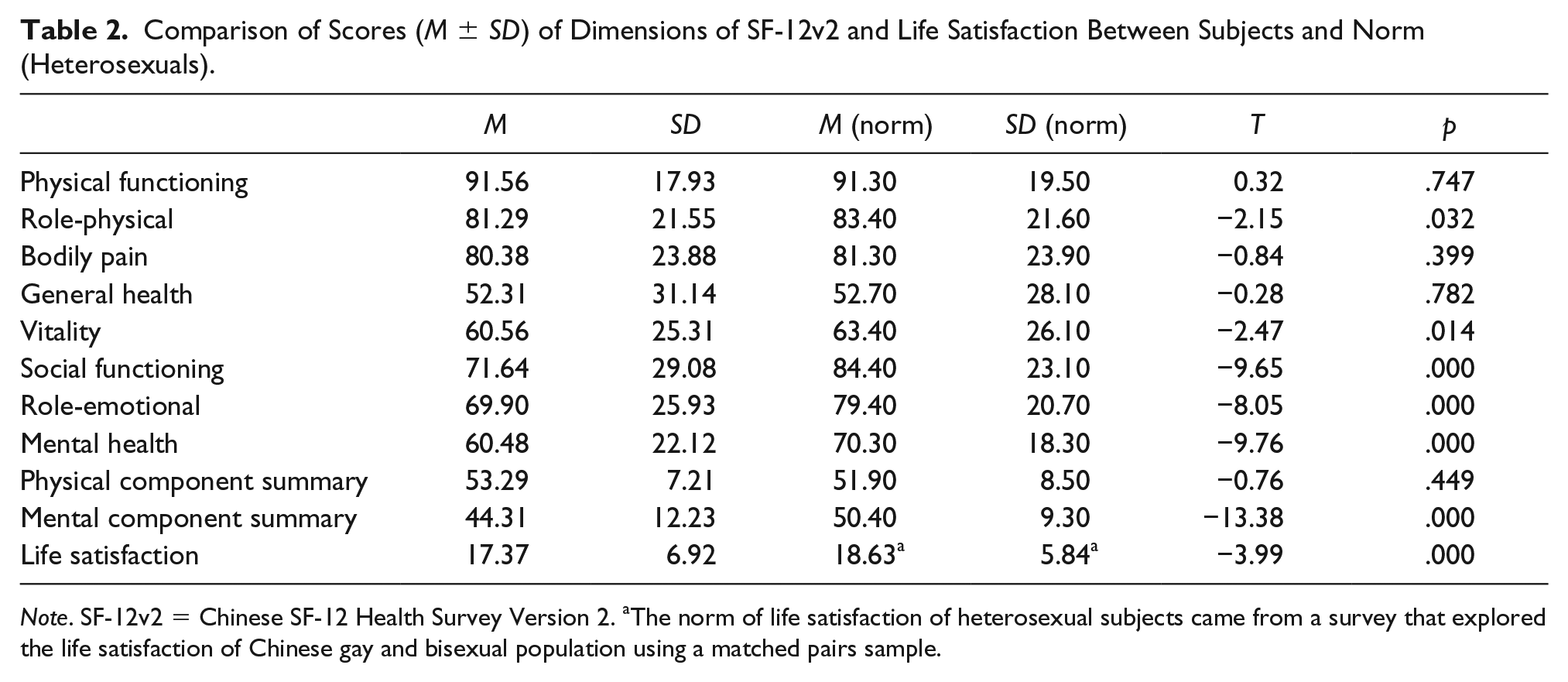
Note. SF-12v2 = Chinese SF-12 Health Survey Version 2. aThe norm of life satisfaction of heterosexual subjects came from a survey that explored the life satisfaction of Chinese gay and bisexual population using a matched pairs sample.
Grouped by demographic variables, the scores for physical health, mental health, and life satisfaction are presented in Table 1. There was a significant difference in mental health score based on age (p < .01). Participants who had at least a college degree had a higher mental component summary score and greater life satisfaction (p < .05 for both). There was a significant difference in mental component summary and life satisfaction among income subgroups (p < .01 for both); mental health and life satisfaction increased with increases in income. There were no significant differences with regard to sexual orientation, occupation, siblings, religion, ethnicity, and geographic location (p > .05 for all).
The correlation coefficients for the three variables of interest are presented in Table 3. Internalized homophobia was significantly negatively correlated with the quality of life domains (physical functioning, role-physical, vitality, social functioning, role-emotional, mental health, and physical component score; r = −0.1 ~ −0.15, p < .05 for all). Internalized homophobia significantly positively correlated with life satisfaction (r = −0.21, p < .001). In contrast to the domains of the physical component summary dimension, the scores of the mental component summary were significantly and positively correlated with life satisfaction (r = 0.31, p < .001).
Pearson Correlations Between Internalized Homophobia, Quality of Life, and Life Satisfaction.

Note. IHP = internalized homophobia; PF = physical functioning; RP = role-physical; BP = bodily pain; GH = general health; VT = vitality; sf = social functioning; RE = role-emotional; MH = mental health; PCS = physical component score; MCS = mental component score; LS = life satisfaction.
p < .05. **p < .01. ***p < .001.
To analyze the mediation effects of the mental component summary on the relationship between internalized homophobia and life satisfaction, bootstrapping procedure (5,000 bootstrap resamples) was used to test the hypothesized mediating effects (Figure 1). Because the physical component summary had no significant relationship with the other variables except for the mental component summary, it was not included in the analysis. The results of the different pathways are presented in Figure 1. These findings indicated that internalized homophobia and mental component summary significantly related to life satisfaction, and mental component summary had a significant mediation effect on the path between internalized homophobia and life satisfaction. The mediated effect of the mental component summary was −0.045 (SE = 0.012, 95% CI [−0.081, −0.018], p < .001).

The mediating effect of mental component summary on the relationship between internalized homophobia and life satisfaction.
Multiple-group analyses were used to investigate the moderating effects of sexual orientation and sex role on the relationship between internalized homophobia, mental component summary, and life satisfaction. The purpose of the multiple-group comparison test was to explore whether structural path coefficients and invariance of indirect effects were different among two sexual orientation subgroups and three different sex role subgroups. The restricted models were compared to the unrestricted models (df = 1) estimated in Mplus 7.0; the results of the χ2 test (Wald value) for differences are presented in Tables 4 and 5 (Wang & Wang, 2012; Wu & Chen, 2015). Based on the results of subgroup analysis, this study revealed that the effects of internalized homophobia on the mental component summary differ according to sexual orientation, while other path coefficients do not. Noninvariance across groups indicated that sexual orientation marginally but significantly moderated the effect of internalized homophobia on the mental component summary. For the relationship between internalized homophobia and mental component summary, the bisexual subgroup (β = −0.29, p < .001) had a negative and slightly higher path coefficient than the gay subgroup (β = −0.114, p < .05). As can be seen in Table 5, none of the moderating effect was observed among the subgroups with different sex roles. In other words, the effects of internalized homophobia and the mental component summary on life satisfaction did not vary among various sex roles. However, statistically speaking, the present study identified that the mediating effect of mental component summary existed only among people who self-identified as bottom.
The Results of the Multiple-Group Analysis Grouped by Sexual Orientation.

Note. IHP = internalized homophobia; MCS = mental component score; LS = life satisfaction.
p < .05. **p < .01. ***p < .001.
The Results of the Multiple-Group Analysis Grouped by Sex Role.

Note. T = top; V = versatile; B = bottom; IHP = internalized homophobia; MCS = mental component score; LS = life satisfaction.
p < .05. **p < .01. ***p < .001.
Discussion
The aim of the present study was to examine quality of life and life satisfaction among Chinese gay and bisexual men, as well as the relationship between internalized homophobia and the outcome variables. The findings revealed that in general, quality of life and life satisfaction were not optimal. More specifically, one domain of the physical component summary (role-physical) had a score that was lower than the norm, whereas all domains of the mental component summary were nearly 10 points lower than those of the population norm. Similarly, the study also identified that participants had lower satisfaction with life compared with heterosexuals.
The findings indicated that gay and bisexual men in China were experiencing comparatively poorer quality of life and life satisfaction, which was similar to other studies that have emphasized the importance of providing mental health care to the gay population (Bachmann & Simon, 2014; Horowitz, Weis, & Laflin, 2001; Williamson, 2000). Conversely, significant differences were not found in the other three physical health domains and the physical component summary, which was consistent with previous study (Herrick et al., 2013).
The present study revealed that there was a significant difference between sexual roles in relationship to mental component summary and life satisfaction. Bottoms had poorer mental health and lower life satisfaction than tops. Previous studies documented that bottoms showed a feminine profile in multiple domains, including self-reported masculinity/femininity, expressiveness, personality, gender nonconformity, and systemizing cognitive style, compared with tops or heterosexuals (Moskowitz & Hart, 2011; Zheng, Hart, & Zheng, 2013, 2015). Additionally, several stereotypes of sexual minorities also contribute to further widen the chasm of misunderstanding about them, such as sexual role stereotypes (i.e., tops are perceived as masculine and bottoms are perceived as feminine) and racial stereotypes (i.e., Black men are perceived as masculine and Asian men are perceived as feminine; Lick & Johnson, 2015). Previous studies have also found that men who self-reported as bottoms were far more likely to have a feminine gender identity than a masculine gender identity early in life (Lick & Johnson, 2015; Weinrich et al., 1992). Gay and bisexual individuals with gender nonconformity were perceived as violating gender norms and would experience more discrimination and prejudice and be rejected by others, which can lead to poor mental health (Collier, Van Beusekom, Bos, & Sandfort, 2013; Lo et al., 2019; Meyer, 2003; Newcomb & Mustanski, 2010). Bottoms are more likely to be perceived as challenging both heterosexual norms and traditional gender expectations; they may also experience more discrimination and prejudice than tops, resulting in poorer mental health (Starr & Zurbriggen, 2017). Finally, compared with tops, bottoms reported less sexual satisfaction, which, being an important index of life satisfaction and well-being, could also contribute to the lower life satisfaction of bottoms (Zheng & Zheng, 2016).
There were significant differences with regard to income and education; higher education and income were associated with better mental health and higher life satisfaction. The results in this study were consistent with previous findings (Powdthavee & Wooden, 2015). A better education received and more money earned by individuals meant a higher social status and better life; thus, better mental health. There were significant differences in life satisfaction according to marital status (Lazarevic et al., 2015; Powdthavee & Wooden, 2015). Single participants and those whose partners were female had the lowest scores, while those with same sex partners had the highest score. Individuals who hid their sexual orientation and/or who were single may have to endure emotional loneliness to some degree. Those who were in a heterosexual relationship against their will were in a worse situation, because of feelings of guilt or other complicated reasons.
The present study identified a negative association between internalized homophobia and quality of life, especially the mental component summary. This finding was similar to that of a previous study in which people who had a high level of internalized homophobia were more likely to have high levels of psychological distress compared to those who had lower levels of internalized homophobia (Cochran & Mays, 2000; Cochran & Mays, 2009; Xu et al., 2017). Internalized homophobia was a gay person’s negative social attitudes directed toward the self. Accordingly, the prejudice and discrimination in society and culture was internalized by individuals. This internalized social stigma could cause psychological conflict between self-perception and others’ perceptions, which leads to the instability and vulnerability of self-perception and triggers psychological stress. Research has also reported internalized homophobia can result in many negative outcomes (mental health problems, self-harm, HIV risk-taking behaviors, etc.; Herrick et al., 2013; Newcomb & Mustanski, 2010).
This study revealed that internalized homophobia was negatively related to physical functioning and role limitation due to physical problems, while its relationship to other physical health domains was not significant. Previous research suggested that the effect of internalized homophobia on physical health was complex. Some research identified LGB adults who experienced high rates of minority stress (i.e., reports of discrimination, rejection, internalized homophobia, and identity concealment) reported more total physical health problems (e.g., chronic diseases) and poorer overall health than those who experienced less minority stress (Frost, Lehavot, & Meyer, 2015). Other research has reported that the effect of internalized homophobia on physical health was decreased (Newcomb & Mustanski, 2010; Walch, Ngamake, Bovornusvakool, & Walker, 2016). This study indicated the path from internalized homophobia to physical health was not significant. One explanation could be that minority stress processes operated differentially on sexual minority mental and physical health, including internalized homophobia (Walch et al., 2016).
This study indicated internalized homophobia had a significant negative relationship with life satisfaction. As already mentioned, internalized homophobia was associated with mental health problems and less life satisfaction. Individuals with higher levels of internalized homophobia may be more inclined to hide their sexual orientation, particularly in China, and internalized homophobia has been suggested to correlate negatively with social support satisfaction and gay social support (Yadavaia & Hayes, 2012). Sexual minorities may believe mainstream society cannot provide the understanding and care they need and are dissatisfied with their interpersonal relationships, which reduces their initiative to seek social support (Szymanski & Carr, 2008). The end result is separation from others and feeling isolated from society, accompanied by the experience of emotional loneliness (Domínguez-Fuentes et al., 2012; Hu, Hu, Huang, & Zheng, 2016). For those with less social support as a resource, life satisfaction will undoubtedly decline further (Domínguez-Fuentes et al., 2012; Mendonça & Simoes, 2019). On the contrary, participants with low internalized homophobia adopted a much more proactive approach to communicate with the world, got support from others, and enjoyed higher life satisfaction (Domínguez-Fuentes et al., 2012). Research suggested that internalized homophobia correlated negatively with sexual satisfaction and intimacy (e.g., relationship stability and length; Balsam & Szymanski, 2005; Zheng & Zheng, 2016). Internalized homonegativity was significantly associated with sexual satisfaction among both Western and Chinese gay and bisexual men. The participants with high internalized homophobia were more likely to feel sexual dissatisfaction and a lack of intimacy.
The present study demonstrated that the relationship between internalized homophobia and life satisfaction was mediated by mental health. In other words, internalized homophobia could not only directly affect life satisfaction but also affect life satisfaction indirectly through quality of life. Previous research suggested that mental health had a strong relationship with life satisfaction (Bachmann & Simon, 2014; Chakraborty, Babu, & Sarma, 2011; Lazarevic et al., 2015). In the present study, participants with mental health problems were less likely to report being happy or satisfied with life, which further affected the relationship between internalized homophobia and life satisfaction. Life satisfaction was the subjective assessment of the individuals’ overall well-being. Internalized homophobia of the participants may make them more prone to experience less life satisfaction through having poor quality of life, especially with regard to mental health. Poor mental or physical health as a negative life event reduced life satisfaction even further. Participants with low internalized homophobia were less likely to have mental health issues and more likely to have an energetic and positive attitude toward life. Additionally, when internalized homophobia is low, life satisfaction is high because the person is less likely to have mental health problems.
Finally, a multiple-group analysis indicated that sexual orientation could moderate the influence of internalized homophobia on mental health. Previous studies have suggested that bisexuals reported significantly more discrimination from the heterosexual community as a result of rejection and marginalization from heterosexuals and lesbians/gay men, as compared to gay or lesbian individuals (Roberts, Horne, & Hoyt, 2015). Heterosexuals and lesbians/gay men expressed more negative attitudes toward bisexuals than toward lesbians/gay men (Eliason, 1997; Herek, 2000; Mulick & Wright, 2002) because of stereotypes about the illegitimacy and instability of bisexuality or negative perceptions of bisexuals as sexually irresponsible (sexually obsessed, diseased, promiscuous). This dual-source stigmatization (also named “binegativity”) intensified the stain and burden on the sexual identity development of bisexuals and led to higher internalized negativity (Berghe, Dewaele, Cox, & Vincke, 2010) as well as less connectedness to the LGB community (Friedman & Leaper, 2010) and a high level of psychological distress (Koh & Ross, 2006).
This study demonstrates that the path coefficients had no statistically significant differences among diverse sex role subgroups, and the mediating effect exists only for bottom-identified men. These findings are important as they help to identify sex role differences so that steps could be taken to keep them out of psychological problems. As mentioned earlier, bottoms acted with a feminine pattern that violated traditional gender roles and led to serious gender nonconformity or sexual identity problems, which seemed to result in critical mental health problems and low life satisfaction (Meyer, 2003; Moskowitz & Hart, 2011; Newcomb & Mustanski, 2010). Although mental health could not mediate the relationship between internalized homophobia and life satisfaction among top and versatile subgroups, it is important not to overlook the direct and negative effects of internalized homophobia on life satisfaction.
Conclusion
The present study was the first to investigate internalized homophobia, quality of life, and life satisfaction comprehensively and contributed to the literature by providing deep insight into the current situation of Chinese gay and bisexual men. In summary, this study revealed comparatively poorer health-related quality of life and less life satisfaction among Chinese gay and bisexual men. This study also suggested internalized homophobia to be significantly and negatively related to quality of life and life satisfaction. Moreover, mental health had a mediating effect on the relationship between internalized homophobia and life satisfaction, and sexual orientation moderated the relationship between internalized homophobia and mental health. The study therefore reminds us of the importance of paying more attention to the status of Chinese sexual minorities and the need to take efforts to buffer the negative effects of sexual minority stress and enhance individuals’ mental health to improve their life satisfaction.
Limitations
This study had several limitations. As this was an Internet survey, the accuracy of the questionnaires could not be ensured (e.g., potential bias of self-selection of network users). Chinese traditional cultural values (e.g., filial piety) played an essential significant role in individuals’ sexual identities, affecting their mental health and life satisfaction. Further study should incorporate other sexual minority stress factors related to the quality of life and life satisfaction of sexual minorities as well as Chinese traditional cultural-specific stress in order to capture the complex mechanism of this subject. In addition, the present study did not investigate lesbian and bisexual women. Thus, future studies should recruit female participants to explore how such stress-related factors influence women who are lesbian or bisexual, including sex role differences.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research is supported by the Fundamental Research Funds for the Central Universities (SWU1709244).
Ethical Approval
This study was approved by the Ethics Committee of Faculty of Psychology, Southwest University.
Informed Consent
Informed consent was obtained from all individual participants included in the study.