
Abstract
Incarceration can lead to different risk behaviors often due to increased distress and disruption of social networks. It is not well known, however, how these associations may differ by age. In this study, we measure age differences in longitudinal associations between incarceration and substance use, sex risk, and sexually transmitted infection (STI) among Black sexual minority men and Black transgender women (BSMM/BTW). We recruited BSMM/BTW from 2009 to 2011 that were part of the HIV Prevention Trials Network 061 study. We compared those less than 30 years old (n = 375) to those 30 years old or greater (n = 794) examining substance use, sex risk, and STI infection stratified by age. Logistic regression with inverse probability weighting was used for the statistical analysis. Approximately 59% of the sample reported incarceration history. In adjusted analysis, incarceration was more strongly associated with alcohol use and stimulant use among older individuals as was sexual risk behaviors including buying and selling sex. Concurrent partnerships were associated with the younger age groups. STI incidence was associated with younger individuals while associations with HIV infection were similar for the two age groups. Understanding differences in substance use and STI risk among age cohorts is imperative to the design and implementation of re-entry programs. Younger BSMM/BTW participating in re-entry support programs may benefit in particular from HIV/STI prevention and care efforts, while post-release substance abuse treatment and harm reduction programs should target older individuals with continued substance abuse.
Introduction
Black men bear a disproportionate burden of HIV and sexually transmitted infections (STIs), with Black sexual minority men (BSMM) and Black transgender women (BTW) experiencing the highest STI/HIV rates (Centers for Disease Control and Prevention, 2023). Sexual risk behaviors are proximate determinants of STI/HIV acquisition, and substance use is an underlying determinant of both sexual risk-taking and STI/HIV acquisition (Chamberlain et al., 2017). Specifically, younger BSMM/BTW are more likely than their older counterparts (i.e., those over 30 years of age) to seek sexual partners via social media, and those who find sexual partners online are more likely to have condomless anal intercourse (Bauermeister et al., 2011; Broaddus et al., 2015; Witkovic et al., 2022). Although STI/HIV incidence rates are highest in younger adult groups, risk-taking can fuel outbreaks in older age cohorts, and age mixing between younger and older groups can result in STI/HIV exposure across age groups. Risk-taking behaviors such as the use of alcohol and/or certain drugs, important health outcomes in themselves, may be greater in different age groups (Schulenberg et al., 2021; Vasilenko et al., 2017), highlighting the importance of understanding drivers of such outcomes across all ages. There is a need to clarify factors that drive STI/HIV incidence and underlying behavioral determinants including sexual risk-taking and drug use in both older and younger groups.
A structural determinant of adverse health and well-being of Black men, including BSMM/BTW, is criminal justice involvement (CJI), including contact with the police and incarceration. In BSMM/BTW of all ages, CJI is associated with methamphetamine use, condomless sex, crack cocaine use, drug and alcohol use, risk behavior, and STI/HIV infection (Harawa et al., 2018; Khan et al., 2019). The specific mechanisms that drive these relationships are unclear, but it is well-documented that incarceration is a disruptive life event that can damage social and sexual networks (Khan et al., 2011; Volker et al., 2016), which may lead to social isolation and distress, and in turn may increase sexual risk-taking behaviors and illicit drug use (Feelemyer et al., 2020). Mental illness, homelessness, and unemployment disproportionally affect those who have been incarcerated, exacerbating poverty risk while creating barriers to the uptake of HIV, STI, and drug treatment (Wildeman & Wang, 2017). The public health significance of CJI of BSMM/BTW is underscored by the persistent, alarming race disparity in exposure to CJI and differential application of drug laws and unfair targeting by law enforcement. Black men have more than five times greater the rate of incarceration compared with white individuals (Nellis, 2016) and BSMM/BTW have twice the incarceration risk compared with their non-minority men who have sex with men (MSM) counterparts (Meyer et al., 2017; Millett et al., 2012).
Although several studies have explored adverse STI, sexual, and drug-related outcomes among BSMM/BTW under 30 years old (Jeffries et al., 2018; Newcomb, 2013; Robbins et al., 2020), few have examined the degree to which interactions between incarceration’s influence on substance use, sexual risk behavior, and STI/HIV may vary with age. Measuring the effects of incarceration on these outcomes by age will ensure that STI/HIV-related drug and sexual risk-taking prevention approaches for people affected by incarceration can be tailored for age cohorts, if appropriate.
The purpose of the current study was to estimate age differences in the influence of incarceration on substance use, sexual risk-taking, and STI. Specifically, we examined the longitudinal associations between recent incarceration and subsequent 6-month alcohol and drug use; sexual risk behaviors including multiple partnerships and sex trade (selling sex, buying sex); and biologically confirmed chlamydia, gonorrhea, and syphilis in BSMM/BTW aged younger than 30 years and BSMM/BTW aged 30 years and older who participated in the HIV Prevention Trials Network (HPTN) 061 study.
Method
This secondary analysis used the HPTN 061 dataset. The data collection methods have been described elsewhere (Brewer et al., 2014). To summarize, 1553 BSMM/BTW who reported condomless anal intercourse were enrolled from six cities (New York, San Francisco, Washington DC, Atlanta, Boston, and Los Angeles) and followed for 1 year. Participants eligible for the study were individuals at least 18 years of age who self-identified as a man or were assigned male at birth, who self-identified as Black, African American, Caribbean Black, or multiethnic Black, and reported at least one condomless anal intercourse event with a male partner in the past 6 months.
Exposure: Incarceration
At the 6-month interview, participants reported the number of times that they had spent one or more nights in jail or prison in the past 6 months; those who reported they had spent at least one night incarcerated were defined as having experienced recent incarceration.
Outcomes: Drug Use and HIV Sexual Risk Indicators
Outcomes of interest included substance use, sexual risk behavior, and incident STI measured at the 12-month follow-up visit. The Alcohol-Use Disorders Identification Test (AUDIT) score (Saunders et al., 1993) identified unhealthy alcohol use in the past 6 months with a score ≥8. We collected information on use of marijuana, opiates, stimulants, and a composite variable of any hard drug use (defined as use of heroin, crack, cocaine, methamphetamine, or unprescribed prescription drugs [Vicodin, Oxycontin, and Xanax], or other drugs [e.g., Ketamine and hallucinogens]).
We included information on engagement in HIV-related sexual risk behavior (which included selling sex, buying sex, concurrent and multiple partnerships). Finally, we included information on incident STI infection (which included chlamydia, gonorrhea, syphilis, and HIV). For HIV, a rapid HIV antibody test was conducted after participants received HIV/STI risk-reduction counseling. If the rapid HIV test was reactive, HIV infection was confirmed at study sites by Western blot testing. STI infections were confirmed with laboratory testing on all participants.
Covariates
We collected several variables at baseline for participants included in the analysis, which were based on the 6 months prior to the baseline interview (unless otherwise noted). Self-reported measures included age, transgender identity, unstable housing (yes/no), high school education or less (yes/no), insufficient income (defined as defined as not having enough money in the household for rent, food, or utilities in the past 6 months), hard drug use (defined as any use of either crack, cocaine, methamphetamine, heroin, unprescribed prescription drugs, or miscellaneous hard drugs), weekly marijuana use, health coverage/health insurance (yes/no), prior lifetime incarceration, AUDIT score ≥8, depressive symptoms based on Centers for Epidemiologic Studies—Depression scale score (Radloff, 1977), experience of physical and/or threatened violence due to race and/or sexuality (yes/no), any reported perceived racism (yes/no), any perceived homophobia based on the Racism and Life Experiences Scale (Harrell et al., 1997) (yes/no), any reported internalized homophobia based on items adapted from Herek and Glunt (1993) (yes/no), any reported sex with female partners (yes/no); having ever received HIV testing (yes/no), transactional sex (defined as sex for money or drugs), multiple partnership (defined as having higher than the median number [≥3] of partners), concurrent partnerships (defined as partners in addition to their primary partner and currently cohabiting with primary partner).
Statistical Analysis
R version 3.6.2 was used for all analyses. Our analytic sample included HPTN 061 participants who returned for the 12-month follow-up interview who had non-missing data on recent incarceration history (N = 1,169 participants). For individuals with missing values for one or more covariates, multiple imputation was used to reduce bias and increase power in the analyses by imputing data using predictive mean matching in the “mice” package (Zhang, 2016). Out of the 1,133 subjects present at the 12-month visit, 416 (36.7%) were missing information on at least one covariate resulting in 40 imputed datasets using predictive mean matching. Quality of the imputations was assessed via visual inspection of density plots of the imputed variables. Values of the imputed variables were checked to make sure that only plausible values were imputed.
We used inverse probability weighting (IPW; Cole & Hernán, 2008) with stabilized weights in fully adjusted analysis to adjust for baseline confounding. The list of covariates described above was used to construct the weights used in the adjusted models. Predicted probabilities, also known as propensity scores, of recent incarceration at 6 months (the main exposure) were extracted and converted into inverse probability weights, which were stabilized in regard to the probability of the observed exposure (Hernán et al., 2006). Logistic regression with the Ridge penalty was conducted for each of the 40 imputed datasets, to create 40 sets of propensity scores, which were used to create 40 sets of inverse probability weights.
We divided men into two age groups, 18 to 29 and 30 and older, in line with the methods used in other studies (Bocour et al., 2011; Jeffries et al., 2018; Tieu et al., 2015; Weber et al., 2001) and based on the distribution of ages of participants included in the study. To assess whether the influence of incarceration on outcomes at 12 months varied by participants’ age, we tested the significance of incarceration by age.
The IPW weights were used in the final adjust analysis, where we estimated unadjusted risk ratios (RR) and adjusted risk ratios (aRRs) and 95% confidence intervals (CIs) for associations between recent incarceration and each of the outcomes at 12 months follow-up, using modified Poisson regressions with robust standard errors to estimate RRs in each of the imputed datasets. Parameter estimates and variances were extracted from each model and were pooled following Rubin’s rules. Unadjusted and aRRss and standard errors via the Delta Method for each age group were obtained using the “margins” package from R.
Informed Consent
Informed consent was obtained from all participants prior to participation in the research study.
Ethical Approval
This secondary data analysis of de-identified data is deemed non-human subjects research and does not require institutional review board (IRB) review.
Results
A total of 1,169 BSMM/BTW were included in this analysis. Table 1 provides demographic information of the cohort participants as well as stratified by age group at baseline. Overall, 375 (32.1%) were aged 18 to 29, and 794 (67.9%) were 30 and older; 601 (51.4%) had less than a high school education, 655 (56%) reported insufficient income, 113 (9.7%) reported being unstably housed, and 712 (60.9%) had current health coverage. A total of 686 (59%) participants had ever been incarcerated at baseline. By age group, 144 (38.4%) of those under 30 reported recent incarceration, compared with 542 (68.3%) among those that were 30 or older (χ2: 96.86, p < .001).
Participant Characteristics at Baseline for Overall Cohort and Stratified by Age Group (N = 1,169)

Note. AUDIT = Alcohol-Use Disorders Identification Test; SD = standard deviation; MSMO = Men who have sex with men only; MSMW = Men who have sex with men and women. a Hard drug use includes the use of: heroin, crack, cocaine, methamphetamine, or unprescribed prescription drugs (Vicodin, Oxycontin, and Xanax), or miscellaneous drugs (e.g., Ketamine, hallucinogens).
p-value for the association between each characteristic and the age group.
At the 6-month follow-up visit 14.1% reported recent incarceration. By age group, 13.1% of those under 30 reported recent incarceration, compared with 14.6% among those that were 30 or older (χ2: 0.381, p = .54).
Alcohol and Drug Use
Table 2 presents the results on incarceration status and associations with different substance use outcomes. Incarceration was associated with a nearly 50% increase in the risk of having an AUDIT score of 8 or greater in those 30 and over (aRR 30 and older = 1.50; 95% CI = [1.11, 2.02]); but this association was not observed in those under 30 (aRR <30 = 0.92; 95% CI = [0.46, 1.81]). There was no evidence that incarceration was associated with increases in marijuana use in either age group. However, incarceration was more strongly associated with hard drug use, particularly among those in the older (30 years or older: aRR = 1.30; 95% CI = [1.03, 1.66]) versus younger age group (<30 years: aRR = 0.82, 95% CI = [0.43, 1.54]). The age difference in the incarceration-hard drug use association appears to be driven by incarceration-related increases in stimulant use in the older age group (30 years or older: aRR = 1.37, 95% CI = [1.06, 1.76]) versus the younger group (<30 years: aRR = 0.93, 95% CI = [0.47, 1.88]). There were no statistically significant differences with respect to opiate use, mainly due to the small number of participants reporting use of this drug.
Risk Ratios and 95% Confidence Intervals for the Association Between Recent Incarceration and Drug Use and Sexual Risk Behaviors and Black Sexual Minority Men/Black Transgender Women, Stratified by Age Group (HIV Prevention Trials Network 061)

Note. RR = risk ratios; CI = confidence interval; AUDIT = Alcohol-Use Disorders Identification Test.
Sexual Risk-Taking
Table 2 presents the associations between incarceration and sexual risk behaviors including sexual partnerships. In those under age 30, the aRR for the association between incarceration and selling sex was 2.65 (95% CI = [0.96, 7.37]) and with buying sex was 2.58 (95% CI = [0.80, 8.30]), which were slightly higher than the aRR for those who were 30 years old or older (selling sex: 1.87; 95% CI = [1.14, 3.07]) and buying sex: 1.68; 95% CI = [0.91, 3.11]). Unadjusted analyses suggested modest associations between incarceration and multiple partnerships and incarceration and concurrency in both age groups, but covariate adjustment attenuated these relationships.
Sexually Transmitted Infections
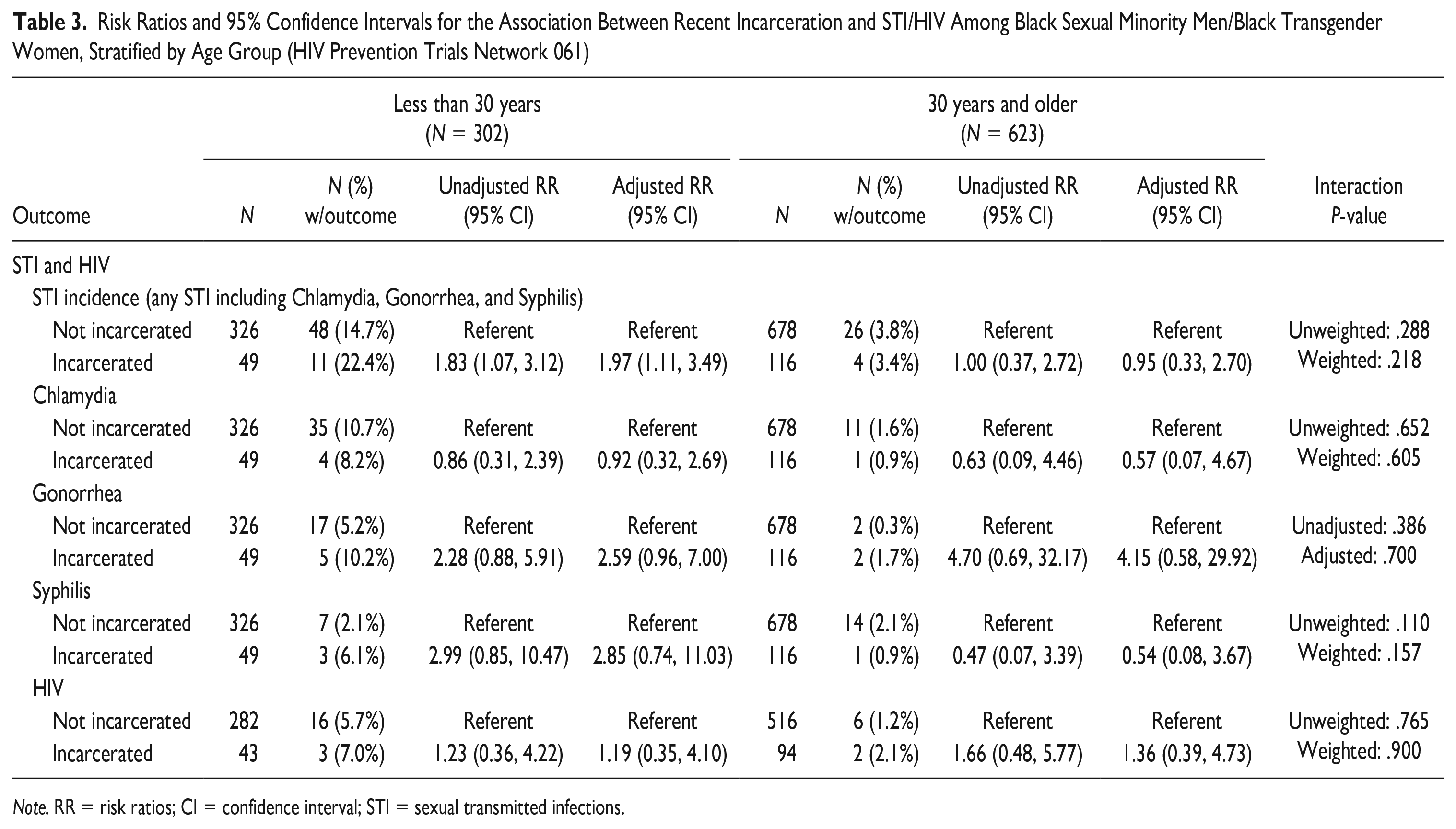
Table 3 provides the associations between incarceration and STI/HIV. Incarceration was associated with increased risk of any STI in the younger cohort (aRR <30 = 1.83; 95% CI = [1.07, 3.12]), but did not appear to be as associated with any STI in the older age group (aRR = 0.95; 95% CI = [0.33, 2.70]). This relationship between incarceration and any STI appears to be driven by incarceration-related increases in gonorrhea in the younger cohort (aRR <30 = 2.59; 95% CI = [0.96, 7.00]). No relationship was found when examining incarceration and HIV.
Risk Ratios and 95% Confidence Intervals for the Association Between Recent Incarceration and STI/HIV Among Black Sexual Minority Men/Black Transgender Women, Stratified by Age Group (HIV Prevention Trials Network 061)
Note. RR = risk ratios; CI = confidence interval; STI = sexual transmitted infections.
Discussion
We analyzed differences in incarceration-related outcomes by age (i.e., younger than 30 years old; 30 years old or older) among a cohort of BSMM/BTW. We observed evidence of variation in the relationship between incarceration and outcomes related to drug and alcohol abuse, sexual risk behavior and STI among the different age groups. Incarceration appeared to be more strongly associated with incident STI acquisition in men younger than 30 years old yet was associated with increased substance use risk in men 30 years old or older, in particular stimulant use (which has continued to increase in use among this population in the last 5–10 years; Arrington-Sanders et al., 2022; Dangerfield II et al., 2020). Furthermore, incarceration-related increases in sexual risk-taking in both groups highlight the potential for incarceration-related HIV/STI transmission should these be present in the networks of all BSMM/BTW regardless of age. Our findings suggest relevant differences between age groups that are pertinent to the design of re-entry support programs.
We observed an association between incarceration and sex trade in BSMM/BTW 30 years old or older, and sex trade was associated with increased STI risk; these were parallel to associations observed between incarceration and STI in both age groups. STI is more prevalent among younger populations regardless of gender, race, or incarceration status (Bocour et al., 2011). Young BSMM/BTW are more likely to experience stressors such as homelessness, a lack of stable relationships, and no health insurance compared with their older counterparts (Vagenas et al., 2016); it is possible that these stressors coupled with a lack of access to treatment may play a role in previously incarcerated young BSMM/BTW’s increased STI risk. It is also possible that sexual network factors explain the elevated risk of STI in younger BSMM/BTW; even if incarceration increases sexual risk-taking in both age groups, if contact with a partner with an STI or HIV is higher in younger versus older networks, this would translate to higher level of STI/HIV in younger age groups.
We observed an association between incarceration and sex trade among BSMM/BTW 30 years old or older, highlighting the potential for HIV/STI transmission in this group as well. A recent study by Yang et al. reported an association between incarceration and transactional sex, as well as independent associations between older age (40 and older) and drug use (Yang et al., 2020). These findings were replicated in the present work; both sex trade and drug use were correlated with incarceration history in the BSMM/BTW 30 years old or older. It is possible that the relationship between incarceration and transactional sex is mediated by drug use, given the well-documented correlation between drug use and transactional sex (Bauermeister et al., 2017; Bobashev et al., 2009). Further investigation of possible mechanisms to explain the observed relationship is warranted.
Previous research has indicated relationships between incarceration and adverse sexual and drug-related outcomes among BSMM/BTW younger than 30 years old, including greater numbers of male anal sex partners, drug use (excluding marijuana), limited access to HIV care, intimate partner violence, methamphetamine use, and survival sex work (Jeffries et al., 2018; Schneider et al., 2017; Vagenas et al., 2016). Most of these studies, however, did not directly compare younger BSMM/BTW to older BSMM/BTW, suggesting an avenue for future research. Literature exploring adverse sexual health outcomes among older BSMM/BTW is limited, and few studies explore the impact of race and incarceration on these measures. In addition, existing studies of older BSMM/BTW often use age 40 or 50 to define age groups (Jacobs et al., 2013; Mutchler et al., 2019; Tobin et al., 2018) which has left a gap in the literature about sexual health outcomes among BSMM/BTW in their 30s and 40s. The present work and others that use 30 as an age cutoff may not entirely capture risks among older or mature BSMM/BTW.
There are important implications from the findings with respect to tailoring harm reduction and interventions for BSMM/BTW with CJI. For younger individuals, efforts should be made to increase STI testing and treatment along with increased access to interventions aimed at reducing risky sexual risk behaviors. For older BSMM/BTW, the focus should be on increasing access to substance use treatment, particularly for alcohol and stimulant use and support services for employment that may help reduce participation in sex-trading behaviors. The period immediately following release from incarceration could present an opportunity to integrate these services into existing programs tailored to individuals recently released from incarceration to maximize participation and access to these services. It is important, however, that treatment services are tailored to the individual need of each BSMM/BTW post-release.
Limitations
Limitations of the current research include modest sample sizes, which has resulted in low power to detect significant differences by age despite our observation that point estimates are different for younger and older BSMM/BTW in which in RRs were at different sides of the null in multiple instances. We did not have information on length of stay for incarceration events reported by our participants. Results may not be generalizable to all BSMM/BTW as the HPTN 061 cohort recruited men from specific cities and their sexual network partners, resulting in a sample that is not representative of the larger BSMM/BTW population. Similarly, our sample is subject to social desirability bias and may miss the perspectives and experiences of BSMM/BTW who are less comfortable reporting their sexual orientation or other stigmatized behaviors such as substance use.
Conclusion
This research presents a further step toward understanding how incarceration affects sexual and racial minorities. Incarceration’s long-term detrimental impact on BSMM/BTW of all ages is clear. Our findings suggest that BSMM/BTW younger than 30 years old participating in re-entry support programs may benefit in particular from HIV/STI prevention and care efforts while older men may value additional resources from post-release substance use treatment.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by the following grants: National Institute on Drug Abuse (P30 DA011041); the National Center for Chronic Disease Prevention and Health Promotion (U48 DP005008); Centers for Disease Control and Prevention (U48 DP006382); National Institute on Drug Abuse (P30DA027828-08S1); and National Institute on Drug Abuse (R01DA044037).