
Abstract
In South Africa, HIV prevalence for gay, bisexual, and men who have sex with men (GBMSM) is as high as 49.5%, yet only 25.7% are taking treatment, resulting in transmission risk between partners and the need for dyadic interventions for men in relationships. Through our preliminary research, we identified the evidence-based intervention Healthy Relationships (HR)—an HIV risk assessment and status disclosure intervention for those in relationships—to be tailored into videoconference format for partnered HIV-positive GBMSM in South Africa. The HR adaptation, called SOAR (Speaking Out & Allying Relationships), applied a human-centered design approach. In-depth interviews were conducted with HIV-positive GBMSM (N = 15) to refine intervention preferences with results used to establish a beta SOAR. A trained interventionist conducted SOAR functionality (n = 6) and usability (n = 7) tests with separate invited groups composed of the original participants interviewed. Field logs, focus group discussions, and a study-specific preference survey were administered. Thematic analysis and descriptive statistics were completed with a convergent analytical approach used to understand usability. Overall experience of GBMSM in SOAR was good (69%) or excellent (31%). More than half of the participants (61%) rated using videoconferencing for SOAR as good, with 38% rating it as fair. All participants stated that SOAR was understandable and satisfactory with willingness to recommend it to other GBMSM. This adaptation approach was effective, and the resultant SOAR intervention has the potential to improve individual coping and HIV communication skills with partners to engage with biomedical prevention and in turn support GBMSM couples.
Keywords
Introduction
In South Africa, HIV prevalence among gay, bisexual, and other men who have sex with men (GBMSM; Duby et al., 2018; Lane et al., 2014; Lippman, 2017) ranges from 13.2% to 49.5%, some of the highest rates for sexual and gender minorities globally. Although much of what we know about HIV risk, prevention, and treatment outcomes comes from research with individual GBMSM, there is an expanding focus on GBMSM couples (Essack et al., 2020; Stephenson et al., 2021). In the Global North, one third to two thirds of new HIV infections among GBMSM occur between primary partner relationships (Bazzi et al., 2016; Dunkle et al., 2013; Stephenson et al., 2017). Despite limited research with South African GBMSM couples, studies demonstrate similar relationship dynamics as in the Global North that influence HIV risks (Essack et al., 2020; Stephenson et al., 2021). For instance, decisions to forgo condom use for anal intercourse among primary partners often reflect desires for trust and intimacy (Arnold et al., 2013; Bazzi et al., 2016; Daniels, Maleke, et al., 2017; Daniels, Struthers, et al., 2019; Goodreau et al., 2012; Stephenson et al., 2017; Sullivan et al., 2009). Although HIV research with male couples in South Africa remains at a nascent stage, to date research has focused almost exclusively on prevention, with a lack of attention on HIV-positive GBMSM in relationships.
Among HIV-positive, partnered South African GBMSM, there is a high rate of HIV transmission. GBMSM may limit or pause antiretroviral therapy (ART) use when staying with their romantic partner and often do not disclose HIV status to partners (Daniels et al., 2018; Lane et al., 2016; Sandfort et al., 2019). Evidence suggests that GBMSM often lack skills in communicating their HIV status and treatment programs to existing and new partners (Charurat et al., 2015; Lane et al., 2016; Lima et al., 2017; Magidson et al., 2016; Rees et al., 2017; Zhang et al., 2018). There is a lack of understanding of pre-exposure prophylaxis (PrEP) and the role of ART adherence in transmission (undetectability and untransmittability [U=U]) and how this knowledge can be communicated and leveraged to support a relationship in South Africa (Daniels et al., 2018; Daniels, Maleke, et al., 2017; Graham et al., 2015; Kalichman et al., 2009; Magidson et al., 2016). As a result, South African HIV-positive GBMSM report unprotected sex with partners after diagnosis without being on treatment (Daniels, Maleke, et al., 2017). In fact, only 25.7% of GBMSM in South Africa are on antiretroviral therapy, and of that, 84.0% are virologically suppressed (Scheibe et al., 2018). These trends demonstrate the need to integrate GBMSM couple dynamics into HIV prevention and treatment interventions in South Africa, and there have been increased calls for dyadic interventions (Daniels, Struthers, et al., 2019; Stephenson et al., 2017). Therefore, based on our preliminary research (Daniels et al., 2022), we selected the Healthy Relationships (HR) intervention to adapt for South African GBMSM in relationships.
HR is a five-session, group-based HIV prevention intervention developed for HIV-positive heterosexual men and women and GBMSM in the United States (Kalichman et al., 2007). In its original iteration, HR is designed to improve individual HIV disclosure risk assessments and safer sexual behavior skills with partners in particular as well as family and friends for support, demonstrating efficacy in these outcomes in various settings (Marhefka et al., 2013, 2014). Based upon the Social Cognitive Theory framework (Merlin et al., 2018), HR uses role-play and discussion for participants to develop coping skills in assessing and managing HIV-related stress, including disclosure and sexual behaviors (Marhefka et al., 2013, 2014). Conducted with HIV-positive GBMSM and women, HR resulted in a significant decrease in unprotected sex and lower risk of HIV transmission at 6 months (Kalichman et al., 2001). Subsequent adaptations of HR include videoconference delivery that also demonstrated high feasibility with 84% satisfaction and few unprotected sex incidences compared with participants in the control (Marhefka et al., 2014; Turner et al., 2019).
We built upon established HR videoconference design and efficacy to adapt HR by utilizing a human-centered design (HCD) approach for GBMSM in Eastern Cape, South Africa. As a multistep, iterative process, HCD gathers perspectives and experiences from key stakeholders and end users for intervention development and adaptation with a particular strength in technology integration (Lyon et al., 2019): a collaborative approach between researchers and users to create a more viable, usable final product that aligns with the preferences of the study populations (Beres et al., 2019; Harte et al., 2017). Although used to adapt and develop multiple mHealth and in-person interventions for HIV prevention and education globally (Mukherjee et al., 2022), HCD is only emerging as a framework in African contexts despite the well-established community-driven HIV response, IT infrastructure, and smartphone usage (Beres et al., 2019). A few studies using HCD have worked with both patients and providers to improve HIV outcomes across African settings. To guide the development of Coach Mpilo, a peer support intervention for HIV treatment with South African men, end-user feedback reported a high level of acceptability among the target population as demonstrated with a 95% ART retention rate at 6 months after intervention initiation (Bautista-Arredondo et al., 2018; Bruns, 2021; Catalani et al., 2014; Ramos, 2017). To design the National Digital Health Platform for Rwandan youth, an HCD approach was deployed by working with youth from design through prototyping and pilot-testing (Ippoliti et al., 2021). Results identified increased need for more user touchpoints with cyber-pharmacists, expanded access to resources like tablets and sensitization training in schools, and improved user confidentiality and expanded content like a job readiness resource (Ippoliti et al., 2021). In Kenya, a clinical decision-making support system for tuberculosis (TB) and HIV care was designed with providers and IT specialists (Catalani et al., 2014). The HCD results demonstrated high understandability, importance, helpfulness, and practicality with lower actionability due to limited TB-related clinical education (Catalani et al., 2014). Across all HCD-driven studies, mixed methodologies ensured an iterative intervention or tool development process to tailor to the end-user of patients and providers.
Our HR adaptation, called SOAR (Speaking Out & Allying Relationships), follows the HCD approach. Initial intervention identification and tailoring were based on our preliminary findings of low rates of HIV-related discussions within GBMSM partnerships and of interest in and desire for mHealth HIV programs to improve their stress, disclosure, and treatment management while in relationships (Daniels et al., 2018; Daniels, Struthers, et al., 2019; Gilmore et al., 2013). Results from the current study demonstrate that HCD is an effective, efficient model for intervention tailoring, especially when preliminary research has been established and mHealth or eHealth tools are the mode of intervention delivery.
Method
Our intervention adaptation utilized mixed methodological approaches over three phases to (1) assess GBMSM preferences and confirm their relationship dynamics around HIV to inform the development of a beta SOAR, (2) determine intervention functionality in the videoconference format (Zoom), and (3) evaluate usability in that participants considered SOAR understandable and satisfactory.
Inclusion Criteria and Recruitment
The study was conducted in Buffalo City Municipality health district in the Eastern Cape province of South Africa. The municipality comprises rural areas, informal settlements, and townships with limited HIV research focused on gender and sexuality minority communities when compared with large urban areas like Cape Town and Johannesburg (Daniels, Maleke, et al., 2017; Daniels, Glockner, et al. 2019; Daniels, Struthers, et al., 2019; Medina-Marino et al., 2021). Participants were recruited through GBMSM community events and HIV testing outreach activities. Potential participants had the opportunity to speak with the study manager in private during the activity, or they were able to contact the study manager via phone. Interested participants went through screening and consent activities. All recruited participants were GBMSM, above 18 years old, HIV positive by self-report, in a romantic relationship with a man for at least a month, prescribed ART, and living in the rural setting of Eastern Cape, South Africa. All participants had to own or have access to a smartphone. Participants completed written informed consent and received R150 (~US$14) as travel reimbursement for completing the study activities and a R150 (~US$14) data plan to support their session attendance. Study procedures were conducted in the local language, isiXhosa.
GBMSM Preferences Identification and Beta SOAR Development
We conducted fifteen (N = 15) individual interviews with GBMSM to gather their experiences and preferences in two broad domains: (1) HIV disclosure with partners and (2) interests in and considerations for participating in an intervention to develop HIV disclosure and treatment management skills over videoconference in a group setting. Interview guides were developed to examine these domains using preliminary research conducted by the research team. Interviews were designed to be 45 min in length, conducted in isiXhosa over Zoom or in person, and audio-recorded for translation and transcription.
Identified preferences combined with preliminary research and the original HR manual were used by the research team to develop an initial SOAR (beta version). Afterward, SOAR was manualized, and an interventionist training program was developed and implemented. Didactic training content included skills in GBMSM health competency, group facilitation, resource and referral, and SOAR delivery and presentation. A trained social worker specializing in HIV care and support was recruited and hired to lead SOAR sessions. The social worker grew up and worked in Eastern Cape and was an isiXhosa native speaker. After completing the didactic training, a series of sequential simulations were conducted such that the social worker first completed SOAR as a participant, then co-facilitated with a research team member, and finally facilitated SOAR as lead. Each simulation was video-recorded and reviewed by the entire team to discuss SOAR delivery until fidelity was achieved (i.e., 95% of the intervention content was consistently administered).
SOAR Functionality
Due to the diverse set of intervention content and its videoconference delivery to GBMSM in rural settings, a functionality test was conducted with participants (n = 6) who were selected from those who completed the preference interviews. Participants were invited to ensure that the group represented an age range between 18 and 45 years. Before beginning the functionality test, each participant provided their mobile number to receive session reminders and the confidential videoconference (Zoom link) meeting invite. After participants completed each of the five SOAR sessions, the program interventionist completed a field log for functionality. The field log was used to document any technical issues related to the SOAR sessions and participant questions that arose, including any preliminary understanding of content, to include domains (Beukes et al., 2016): (1) participant attendance and device use with camera, (2) reported disconnections and image or sound loss, (3) length of each session, and (4) summary of general participant interactions and engagement with session content. Findings were used to adjust any technical delivery considerations for SOAR in this setting.
SOAR Usability
The usability test was designed to determine the extent to which the intervention content was understandable and satisfactory (Gbadamosi et al., 2018; Harte et al., 2017; Wray et al., 2017). The intervention was tested over 5 weeks with a 2-hr session per week. Participants (n = 7) were selected from those who had completed the initial interview but had not completed the functionality test.
All participants completed the five intervention sessions on Zoom. During the sessions, the interventionist monitored participant engagement. Similar session reminders and Zoom access link were used as conducted in the functionality test. All intervention sessions were video- and audio-recorded for review by investigators to provide feedback to the research interventionist for training purposes. All participants received SMS reminders for each session and a data plan to complete the testing.
After the usability test, a focus group discussion was conducted per session to evaluate six intervention usability domains: (1) satisfaction with the sessions, (2) timeliness and appropriateness of sessions, (3) clarity of session content delivery, (4) clarity and management of self-assessments and action plans, (5) incomplete sessions, and (6) the technical transition between sessions. In addition, using findings from the focus group discussions, a study-specific survey was developed to assess GBMSM understanding and satisfaction with the intervention.
In addition, a study-specific usability survey was administered to all functionality and usability test participants. The survey was designed to assess GBMSM experience during SOAR sessions and valued content in their lives. Results were integrated into the final intervention with the manual updated accordingly.
Data Analysis
All functionality field logs were collated and then reviewed by the team to provide input on intervention delivery by staff and any technical adjustments needed. To understand preferences and usability, interviews and focus group discussions were audio-recorded, translated, and transcribed. Transcripts were cleaned and confirmed for accuracy before being uploaded into analytical software Dedoose to be ordered into codes and categories (Braun & Clarke, 2014; Scorgie et al., 2021). First, the research team separately analyzed each transcript using predefined codes and open coding, and then the team discussed coding to confirm alignment and coding distinctions to clarify codes (Poteat et al., 2020). Second, using a thematic approach (Fereday, 2006), researchers analyzed the coded transcripts to identify SOAR preferences and usability themes as an iterative process. An additional comparative analysis based on age was conducted to identify any distinctions (Braun & Clarke, 2006; Fereday, 2006; Mitchell et al., 2016). Theme discrepancies were resolved by agreement during research team discussions. The usability survey was analyzed in STATA using descriptive statistics (Medina-Marino et al., 2022). A convergent analytical approach was applied to compare results from the focus group and survey to finalize intervention components and delivery considerations (Poteat et al., 2020; Teo et al., 2020). Finally, results from the adaptation process were presented to a research advisory board for review and recommendation for intervention design and delivery. The research advisory board consists of five GBMSM HIV service providers and research scientists in South Africa.
Ethics Statement
All participants interested were screened, and then those eligible were invited to complete a written informed consent process that was approved by a local institutional review board.
Results
There were 15 Black, HIV-positive, and partnered GBMSM recruited at HIV outreach activities led by a local collaborating organization. The participants ranged in age from 25 to 45 years old, with an average age of 28, and all had been living with HIV for at least 5 years (range = 5–11 years). Among them, all reported being prescribed ART, with 14 (93%) currently on ART, while four (29%) of the 14 participants reported a missed ART dose in the previous 2 weeks. All participants completed an interview with subgroups completing either a functionality or usability test (Supplemental Table 1).
GBMSM Intervention Preference Identification and Beta SOAR Development
Interviews provided additional contextual understanding of GBMSM relationship dynamics, HIV education and communication skills needed, and preferences for intervention delivery.
Participants described their experiences and considerations for disclosing their HIV status to their family, friends, and partners (Table 1). Some described the desire to disclose out of love and need for honesty in hopes of mutual support. In the process of disclosing to partners, a few reported that their partner also disclosed their HIV-positive status afterward, improving openness and communication about treatment in their relationship. Participants noted that family members could act as a support system for them when deciding to disclose or not, serving as brokers or mediators. However, instances were also reported of family members not being supportive such that they disclosed HIV status without permission as an act of demeaning or belittling that reinforced HIV and sexuality stigma. Overall, participants indicated that HIV disclosure was dependent on them having a clear understanding of HIV disease for treatment and prevention so they could effectively communicate to others like partners to dispel concerns and stigma, increasing the likelihood of support. Findings revealed the important relationship between disclosing to family and partners: Several participants expressed that partner disclosure is risky in that it can result in loss and that a trusted family member can serve as a key supporter to help them navigate these situations. We used these findings to select video content and conceptualize role-plays for SOAR sessions (Supplement 2). The two main role-play scenarios were created to cover disclosure with associated stressors and questions for GBMSM to apply skills learned in each session. Specific scenarios of note were navigating risk of dual HIV and sexuality disclosure and identifying ideal HIV treatment support from partners.
SOAR Theme Preferences
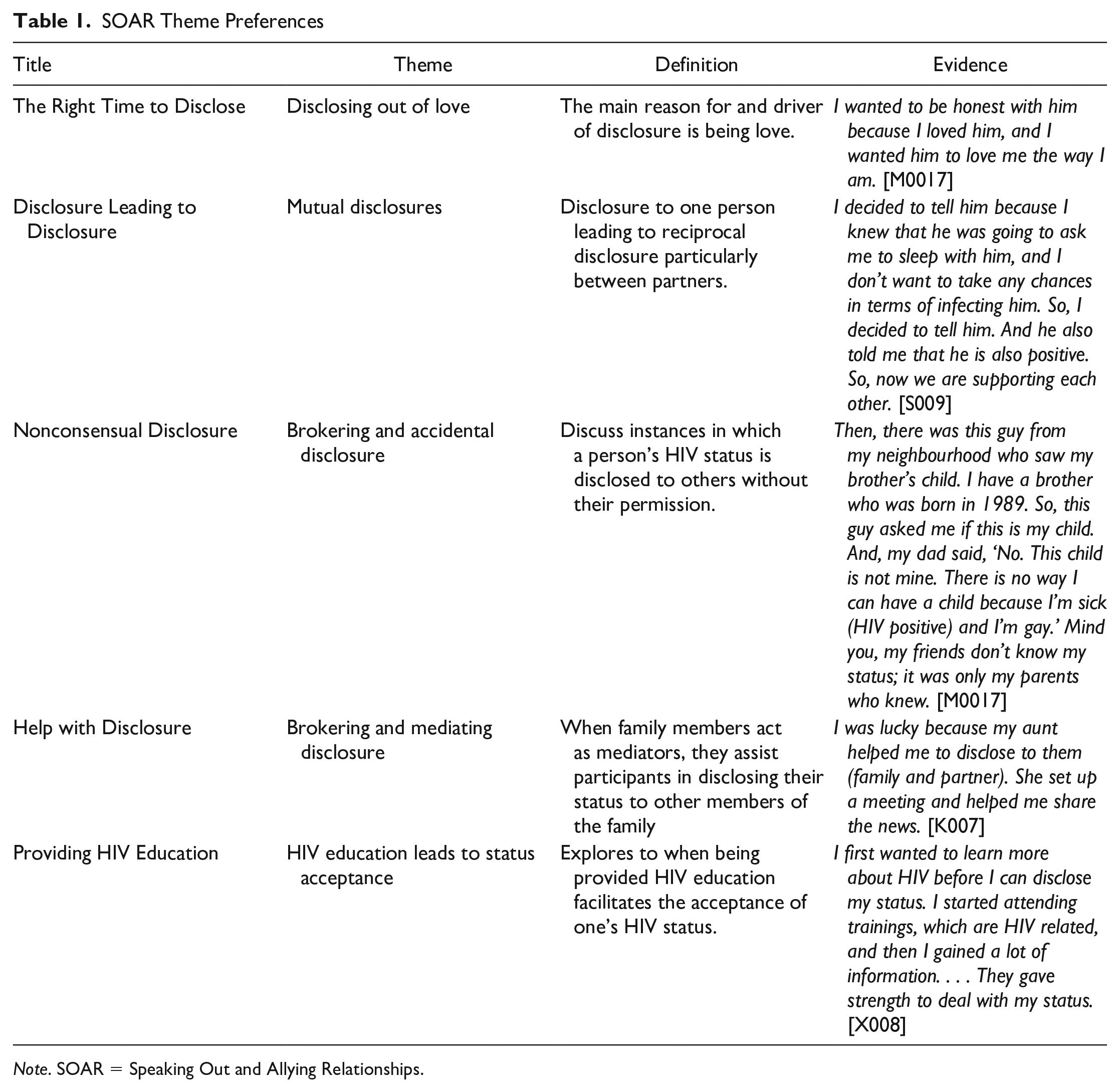
Note. SOAR = Speaking Out and Allying Relationships.
In Table 2, we show the HR intervention with the added and refined SOAR content. Core elements from each session in the original intervention were retained with modifications to contextualize skill-building in the South African context (Table 1). Based on interviews and preliminary research, we integrated GBMSM intervention preferences and needed coping skills into SOAR. Educational activities for PrEP and undetectability and untransmittability (U=U) were added to Session 1, including how these can work together to support a relationship like in the case of sero-discordancy or unknown HIV status of a partner. For Sessions 2 and 3, coping and disclosure skills were discussed. Role-plays (Supplement 1) were used to practice applying risk assessment in disclosing HIV and sexuality to friends and family and HIV status to intimate partners and to identify and practice communicating support needs with both groups. In Sessions 4 and 5, added content from previous sessions were reviewed with role-plays.
SOAR Content Integrated Into HR
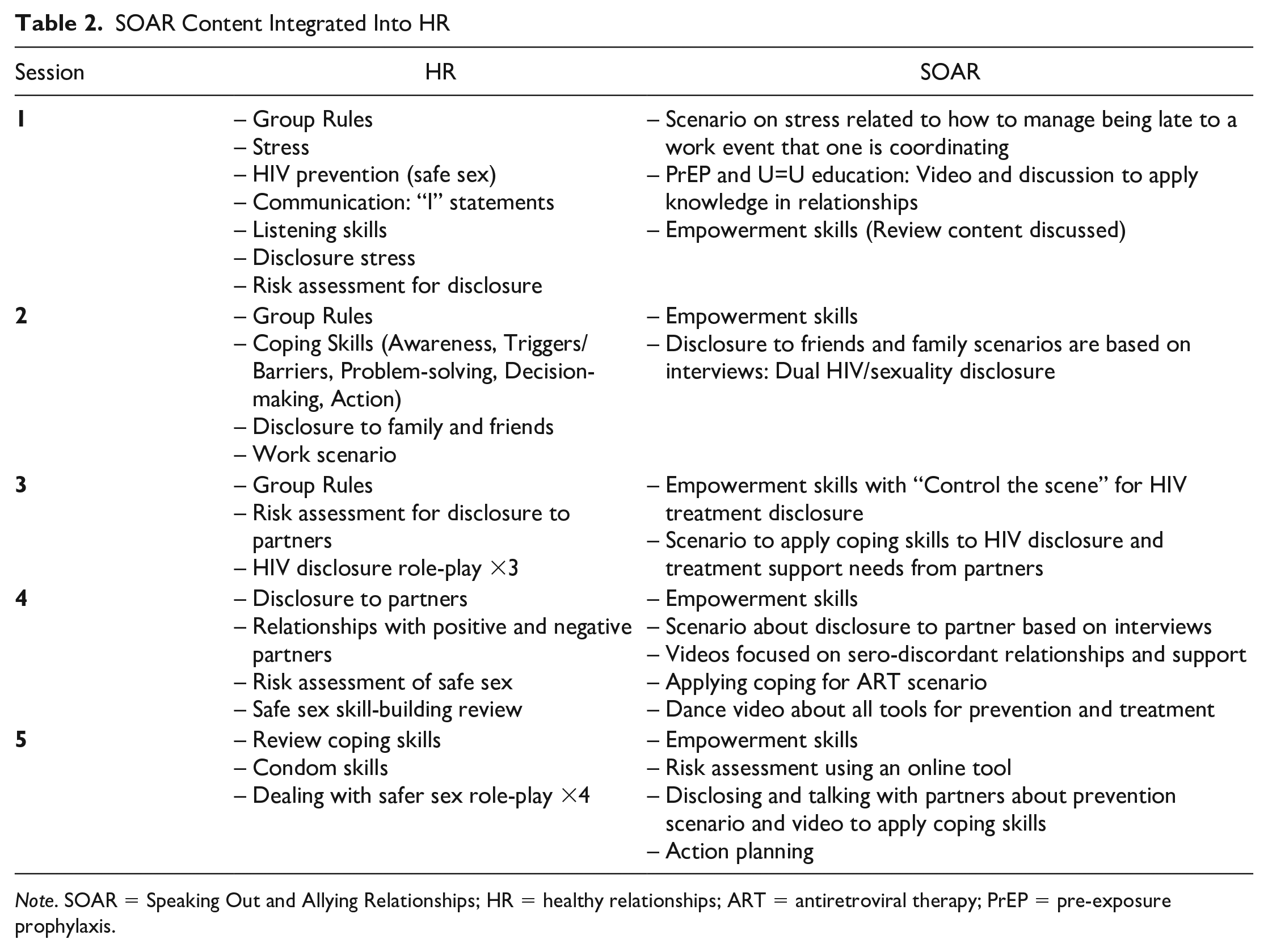
Note. SOAR = Speaking Out and Allying Relationships; HR = healthy relationships; ART = antiretroviral therapy; PrEP = pre-exposure prophylaxis.
One key element of the HR intervention is to start every session with “Empowerment Skills,” where participants review previous learning and discuss how they applied new skills in their daily lives. The original intervention uses movie clips to support skill-building, so the adapted SOAR included South African and Black GBMSM voices about living with HIV in the form of short films and YouTube episodes that were 4 to 12 min in length. Integrated videos covered the South African GBMSM context for HIV disclosure and relationship dynamics, including sero-discordancy, and these aligned with content for each session.
The original HR also uses personal feedback forms, but the research team determined that this may present administrative burden for participants, so it was decided to leverage the effectiveness of action planning in HIV prevention and treatment to empower participants to make their own plan to apply new skills based on risk assessments for HIV disclosure and treatment. When creating personal action plans, participants formulated a plan to disclose or not disclose their HIV status to their partners and a plan for treatment. This action plan was shared with the interventionist via SMS and discussed in the three subsequent check-in meetings, which were conducted with each group for 30 min after the last SOAR session and 1 month apart.
All sessions and meetings were designed to be delivered on Zoom with active video cameras to facilitate group conversation. A PowerPoint slide deck was developed for each session, and these were used to guide conversation about SOAR content using contextually relevant and empowering images, videos, and role-plays. Each session was built to cover content under 2 hr, which was preferred by participants as well as preference for a mix of isiXhosa and English for intervention delivery. These adaptations established the Beta SOAR that was used for functionality and usability testing. The primary focus for testing was on the five sessions. The check-in meetings were not conducted as part of this testing process but are part of the subsequent feasibility test of the SOAR intervention.
SOAR Functionality
After each of the five sessions, the interventionist completed a field log to assess functionality of the SOAR session (Table 3). Of the seven GBMSM invited, four GBMSM participated in the first two sessions, and six participated in the last three sessions. All participants attended the session using a smartphone and noted no impact of load-shedding (government-planned power outages) on intervention engagement. Over the five sessions, only one user reported technical issues related to using their smartphone for the Zoom session. During the first session, one participant was uncomfortable with having their camera on, but midway through the first session, this participant became more at ease with the session and turned on his camera. All other participants kept their cameras on during the sessions. No other technical issues were reported, with no reported difficulty seeing or hearing the videos or slides presented by the interventionist. Participants also noted no difficulty with lost connections or dropped video signals.
Functionality Outcomes

SOAR Usability
The goal of the usability test was to determine whether participants were satisfied with the intervention and the degree to which the session content was relatable and understandable to inform any refinements to SOAR (Table 4). Data for the usability test were collected via postsession focus group discussions and a survey. All GBMSM participated (n = 7), and results indicated that the participants thought each concept or skill taught was clear and the role-plays were relatable and understandable. Participants could identify all concepts and information presented in each session and noted that the videos used were informative, educational, and relevant. Many participants stated they would recommend all five of the SOAR sessions to others based on what they learned. The key concepts the participants took away from each session centered around the importance of trust and communication when thinking about disclosing HIV status to partners, peers, and family members. When asked about what words the session content suggested, participants stated that the content was exciting and that they wanted to have access to the PowerPoint slides to share with others in their networks.
Usability Outcomes

Note. ART = antiretroviral therapy; PrEP = pre-exposure prophylaxis.
One participant noted that the sessions made them want to make good decisions because every decision mattered. Along these lines, the most discussed focus group topics were information and skills gained for disclosure, relationships with men, and HIV education. In addition, approximately half of the participants noted the importance of other SOAR topics: listening skills, risk assessments, and gaining support from family and peers. The least discussed topics involved information regarding coping skills and triggers.
Survey results aligned with qualitative findings. Participants were asked to rate the importance of elements of the SOAR intervention (Table 5). Nearly all the participants (92%) saw the most crucial part of participation in SOAR sessions as the ability to interact with other HIV-positive GBMSM. The majority of participants also noted the importance of sharing stories and experiences with other GBMSM (76%), learning new information regarding HIV treatment (76%), and learning about the disclosure process and coping skills (69%). Less critical elements of the intervention were watching videos of shared experiences (46%), participating in role-play (46%), and learning about triggers (23%). Participants were also asked to identify the most discussed topics during the SOAR sessions (Table 6) and identified these as information regarding disclosure, relationships with men, and HIV education. In addition, approximately half of the participants noted the information regarding listening skills, risk assessments, and gaining support from family and peers. The least discussed topics involved information regarding coping skills and triggers.
Most Important SOAR Content

Note. SOAR = Speaking Out and Allying Relationships; GBMSM = gay, bisexual, and men who have sex with men; PrEP = pre-exposure prophylaxis.
Most Reported SOAR Topics Discussed
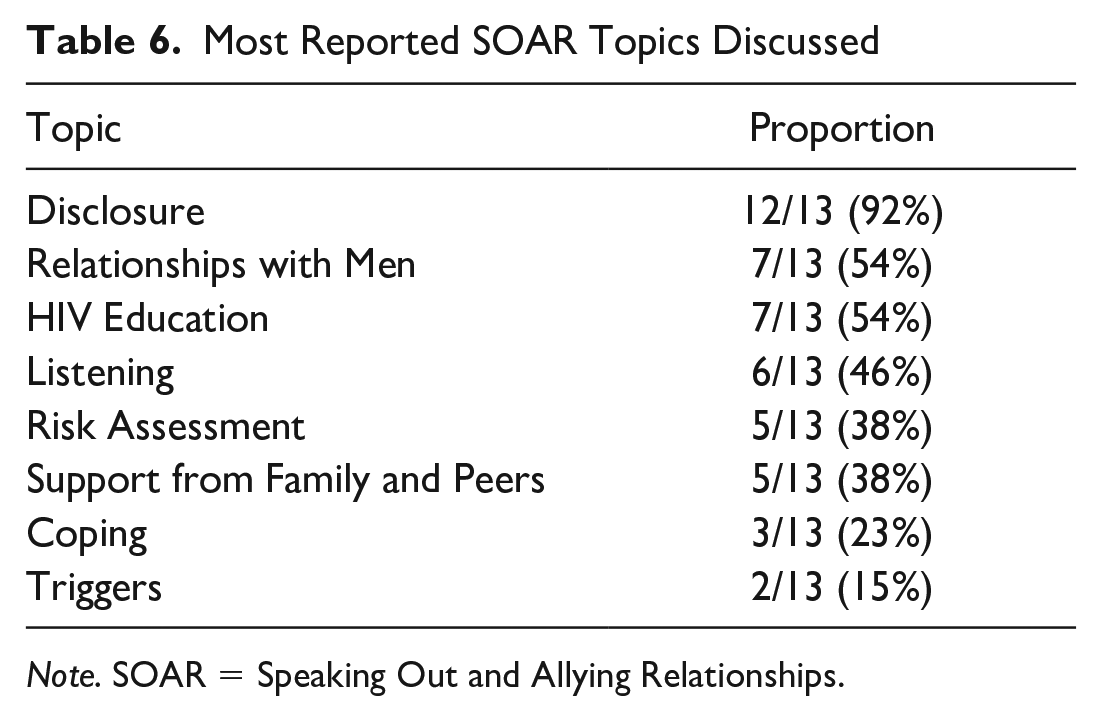
Note. SOAR = Speaking Out and Allying Relationships.
The overall experience of GBMSM in SOAR was good (69%, n = 9) or excellent (31%, n = 4). Over half of the participants (61%, n = 8) rated using videoconferencing (Zoom) for SOAR as good, with 38% (n = 5) rating it as fair. All participants reported that they would be willing to recommend SOAR to other GBMSM in their communities.
Discussion
By utilizing an HCD approach (Harte et al., 2017; Ramos, 2017), we successfully adapted HR into a beta SOAR for GBMSM in South Africa. The beta SOAR required minimal changes after conducting feasibility and usability tests as participants found the HIV education and skill content were appealing and interesting along with all role-play scenarios and most of the videos. After testing, we replaced a video that did not depict a GBMSM individual and added more time for participants to explain and develop their action plans. The final adaptations, including role-play scenarios, are outlined in Tables 1 and 2 and will be carried over into the final version of SOAR that will be tested for feasibility in a pilot randomized controlled trial with the aim to eventually test the intervention in a fully powered efficacy trial.
Our use of HCD to guide our intervention adaptation process was efficient but dependent on the extensive preliminary research that was conducted prior (Daniels et al., 2018; Daniels, Lane, et al., 2017; Daniels, Struthers, et al., 2019). Such research facilitated identification of the intervention, HR, that aligned with GBMSM preferences for HIV treatment support and disclosure to partners. Also, the research provided us data to develop an interview protocol to refine GBMSM intervention preferences in this study. Given the multiple intervention delivery components like videos, videoconferencing, and PowerPoint slides for each of the five sessions, functionality and usability were tested separately and for all sessions to ensure content from each were understandable and satisfactory. Alternatively, functionality could have been tested with just one or two sessions in one day, but this would not allow us to understand changes in participant access over time such as the potential impact of load-shedding or changes in smartphone access. Although other models for intervention adaptation map out a step-by-step process from intervention identification to feasibility or efficacy testing, and may be used in conjunction with HCD (Wingood & DiClemente, 2008; Woolf-King et al., 2022), we found our HCD approach may be well suited for studies with established preliminary research that did not apply such models originally—especially with findings identifying the need to tailor an evidence-based intervention to address health disparities in a new setting or population.
While some HIV treatment behavioral interventions for GBMSM have been developed in African settings, there is a noted gap in relationship- or couples-based interventions, and few have harnessed mHealth tools, including videoconferencing, in settings where smartphone usage is significant (Dworkin et al., 2019; Fan et al., 2020; Hightow-Weidman et al., 2018; Horvath et al., 2019; Lewis et al., 2013; Tanner et al., 2018; Turner et al., 2019). With increased innovations, including smartphone technology and cellular data, delivering interventions via video platforms is feasible (Ntinga et al., 2022). These platforms expand access to those in more rural settings, those with difficult work or school schedules, and those who otherwise may not be able to travel to a common space for sessions. Furthermore, they allow participants to control their confidentiality and develop skills in a personal space. Given the intersectional stigma of HIV and sexuality along with the related discrimination for GBMSM in South Africa (Abubakari et al., 2021; Bergman et al., 2022), videoconference delivery can facilitate participant decisions to manage any associated risks with these at times joint disclosures (Daniels, Struthers, et al., 2019). Our usability findings suggest that videoconference delivery of SOAR aligns with GBMSM preferences in this area as it allows them to control and discuss HIV and sexuality disclosure and related skill-building in a safe space prior to considering these conversations with family, friends, and partners.
Social Cognitive Theory Is Sustained in SOAR
The interactions between cognition, behavior, and environment that comprise Social Cognitive Theory are well supported by the SOAR intervention design as in HR (Marhefka et al., 2014; Merlin et al., 2018). SOAR creates an online, supportive environment for small groups of four to seven GBMSM living with HIV who are navigating similar HIV disclosure and treatment stresses, like risks of disclosure and transmission. Our participants valued meeting other GBMSM living with HIV and learning together and grew more comfortable with the group, as demonstrated by the participants who were hesitant to use their video cameras during the first two sessions but turned on their cameras after the second session. Scenarios and role-plays were contextually grounded, allowing participants to apply self-regulation skills like coping, and these skills were reinforced through conversations about videos related to their experience, such as stories of GBMSM with partners who have an unknown HIV status. Action planning and check-in meetings are intended to facilitate self-management of HIV disclosure, communication, and treatment so as to empower GBMSM to apply new skills gained in real life (Khumsaen & Stephenson, 2019). In turn, SOAR may improve partner communication about HIV prevention and treatment, lowering risk of transmission within relationships already severely affected by stigma and discrimination (Curtis et al., 2022; Metheny et al., 2022; Stephenson et al., 2021). Specifically, the SOAR intervention is designed to empower GBMSM in relationships by improving individual coping skills and communication with partners about HIV testing and how PrEP and ART (U=U) work in concert for prevention and wellness.
Strengths and Limitations
Our SOAR intervention adaptation process using HCD has two key strengths. First, findings from our preliminary research identified GBMSM preferences for an intervention to improve their HIV treatment adherence. Because such preferences aligned with HR outcomes, we were able to efficiently tailor this evidence-based intervention for GBMSM in South Africa rather than develop and test a new intervention and thus inform intervention adaptation methods in cross-cultural settings (Movsisyan et al., 2019, 2021; Sullivan et al., 2014). Although most of our participants had been living with HIV for at least 5 years, which may not represent all GBMSM like those newly diagnosed, interviews identified ongoing influences of HIV stigma on disclosure and relationships that are commonly shared. Second, our research has shown that GBMSM are willing to participate in video groups as a means of HIV intervention (Daniels, Lane, et al., 2017), and HR has been delivered in this mode effectively with a U.S. population (Marhefka et al., 2014; Turner et al., 2019). In this study, the positive feedback on such delivery showed that SOAR could be successful for GBMSM in South Africa. The use of virtual sessions viewed by participants using personal smartphones allowed for greater access to the program in a comfortable setting. However, this strength may be compromised by a key limitation, if not managed effectively: South Africa is facing an energy crisis, which results in load-shedding, when there are periods of scheduled blackouts at different times and locations in the country. When scheduling technology-based mHealth interventions, managing session times around blackout times and discussing such planning with participants are critical. In our experience, load-shedding was not identified as a barrier for participant engagement but may become an issue in a larger pilot study or fully powered efficacy trial. Overall, while this study was confined to beta testing the adaptation of HR into SOAR, the success of the original HR intervention and the acceptability of our adaptation indicate that SOAR has potential to create significant behavioral changes in the HIV disclosure and treatment outcomes among partnered, HIV-positive GBMSM in South Africa.
Supplemental Material
sj-docx-1-jmh-10.1177_15579883231197355 – Supplemental material for Developing the Speaking Out and Allying Relationships Intervention on Videoconference for HIV-Positive GBMSM in Eastern Cape, South Africa
Supplemental material, sj-docx-1-jmh-10.1177_15579883231197355 for Developing the Speaking Out and Allying Relationships Intervention on Videoconference for HIV-Positive GBMSM in Eastern Cape, South Africa by Joseph Daniels, Remco P. H. Peters, Sarah Portle, Ntokozo Mashabela, Helen Struthers, Oscar Radebe, Dawie Nel, Andrew Medina-Marino, Cikizwa Bongo and Rob Stephenson in American Journal of Men's Health
Footnotes
Acknowledgements
We would like to thank all the participants who agreed to share their perspectives and experiences during this study and greatly appreciate the support from community partners and the Eastern Cape District of Health.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The research was funded by a grant from the National Institues of Health, NIMH R34MH125790, Daniels (Contact Principal Investigator).
Ethical Statement
All participants interested were screened, and then those eligible were invited to complete a written informed consent process that was approved by South African and international institutional review boards. This study has been reviewed and approved by the University of Cape Town Review Board (FWA00001938) with reliance by Institutional Review Boards at Arizona State University (STUDY00014539) and the University of Michigan (HUM00208997).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.