
Abstract
Appendicular mucocele (AM) is a rare and potentially malignant entity linked to obstructive dilatation of the appendix with an intraluminal accumulation of mucoid material. Most AM is asymptomatic or simulates acute appendicitis. We report an exceptional case of AM discovered in the face of hypokalemia and aggravation of chronic kidney disease (CKD) without diarrhea in an old man. Investigations led to the diagnosis of AM in its malignant form complicated by gelatinous ascites. We retained mucinous hypersecretion as the cause of hypokalemia and acute renal failure. Aggressive surgery and intraperitoneal chemotherapy corrected hydroelectrolyte imbalance.
Keywords
Introduction
In patients with chronic kidney disease (CKD), hypokalemia is uncommon. Instead, there is usually hyperkalemia whose major risk factors include lower estimated glomerular filtration rate, use of renin-angiotensin-aldosterone system inhibitors, diabetes, older age, and male gender (Seliger, 2019). Hypokalemia among CKD patients is often due to extrarenal, mainly digestive, loss of potassium.
We report the case of a diabetic, old man with advanced chronic renal failure, who presented with hypokalemia due to gastrointestinal leakage secondary to appendicular mucocele (AM). AM is a rare and potentially malignant entity linked to dilation of the appendix and the abnormal accumulation of mucus in its lumen. Its revelation by hypokalemia as reported herein has never been previously reported to the best of our knowledge.
Case Report
A 66-year-old man with a history of hypertension, type 2 diabetes mellitus, coronary, and CKD was admitted into nephrology for hypokalemia despite worsening renal insufficiency. The interrogation revealed the notion of abdominal pain dating back a few months without episodes of diarrhea.
On physical examination, the blood pressure was normal and the patient’s abdomen was soft, non-tender, and non-distended, with no palpable masses. The diuresis was 1.5 L/24 h.
Results of laboratory testing demonstrated a worsening of the patient’s CKD, with the rate of creatinine clearance going from 25 to 15 mL/min. They also showed a serum potassium (K+) level of 2.8 mmol/L, with collapsed kaliuresis, and metabolic acidosis, with bicarbonates at 14 mmol/L.
These findings suggested a lower digestive leak of K+. An abdominopelvic ultrasound was therefore requested, revealing a thickened aspect of the last ileal loops at the level of the right iliac fossa.
For further exploration, the patient underwent a computed tomographic scan of the abdomen and pelvis showing an aspect in favor of AM complicated by gelatinous disease of the peritoneum (Figure 1 and 2).

Abdominal-Pelvic Scanner: Aspect of Appendicular Mucocele Complicated by Gelatinous Disease of the Peritoneum 
After K+ supplementation, the kalemia corrected quickly and the patient was entrusted to the surgeons. The exploration of the abdominal cavity found an important effusion of gelatinous material, which also involved other abdominal organs and an appendicular neoplasm.
A right hemicolectomy with peritoneal cleansing was performed followed by intraperitoneal chemotherapy based on 5-fluorouracil since histology showed appendicular mucinous neoplasm of low grade, extensive tissue, and serous.
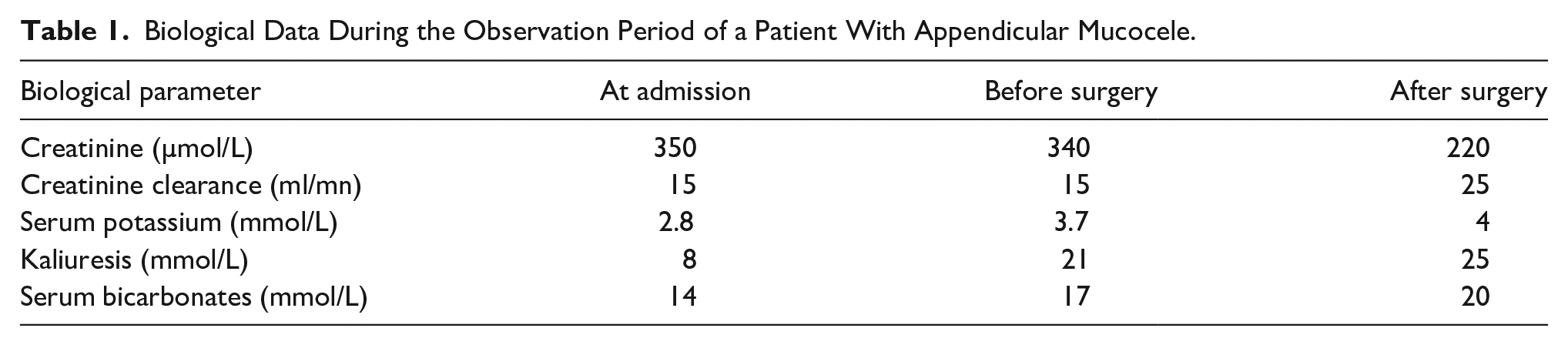
During the follow-up, serum potassium remained normal, and the patient regained his previous renal function. The evolution of the biological data during the observation period is represented in Table 1.
Biological Data During the Observation Period of a Patient With Appendicular Mucocele.
Discussion
The classification of AM or mucinous tumors of the vermiform appendix includes a spectrum of neoplastic lesions ranging from benign proliferation, intraluminal, to invasive adenocarcinomas (Anania et al., 2015). It is a rare disease that occurs in 0.2% to 0.3% of appendectomies (Caspi et al., 2004).
The AM is asymptomatic in 20% to 25% of cases and the diagnosis is accidental (Bronzino et al., 2006). In 50% to 65% of cases, there are signs of acute inflammation of the appendix and in 10% to 20% of cases, intestinal obstruction or palpable mass in the right lower abdominal quadrant are present (Cerame et al., 1988; Ito et al., 2004). Melena (Wolff & Ahmed, 1976), intussusception (Ohno et al., 2000), infiltration of the bladder (Tripodi et al., 1995), vaginal penetration with colporragia (Didolkar & Fanous, 1977), and pyonephrosis by compression of the right ureter (Deture et al., 1976) are rarer occurrences.
The discovery of AM in our patient was made during the assessment of hypokalemia. This is an exceptional mode of revelation for such neoplasm. Indeed, AM can be, as in this case, complicated by gelatinous disease of the peritoneum, the « pseudomyxoma peritonei », a condition caused by cancerous cells (mucinous adenocarcinoma) that produce abundant mucin or gelatinous ascites. The AM would therefore have been responsible in our patient for an equivalent of the electrolyte depletion syndrome (Mckittrick-Wheelock syndrome). This latter is a rare and life-threatening disease characterized by the triad of (1) chronic mucous diarrhea, (2) renal function impairment with hydroelectrolyte imbalance, and (3) a giant colorectal tumor (Villanueva et al., 2022). The mechanism behind severe electrolyte and body fluid depletion in Mckittrick-Wheelock syndrome is suggested to involve cyclic adenosine monophosphate (AMP) and prostaglandin E2 acting as mediators, which increase the loss of fluid and electrolytes from the plasma to the intestinal lumen (Steven et al., 1981). Our patient didn’t present diarrhea, but the abundant mucosecretion would be responsible for hypokalemia due to digestive loss.
Most of the reported cases of pseudomyxoma peritonei involve women of reproductive age (with a history of endometriosis, abdominal surgery, or pelvic inflammatory disease) (Anania et al., 2015). Its occurrence in an old man, as reported herein, constitutes another particularity of this observation.
As recommended by most authors in the case of pseudomyxoma peritonei, our patient underwent a surgical aggressive attitude and intraperitoneal chemotherapy with good evolution (Anania et al., 2015).
Conclusion
AM complicated by gelatinous ascites can cause profound hypokalemia even without diarrhea. Abundant mucosecretion would even be responsible for severe electrolyte and body fluid depletion with acute renal failure similar to those observed in Mckittrick-Wheelock syndrome. Aggressive surgery and intraperitoneal chemotherapy correct these life-threatening abnormalities.
Footnotes
Author Contributions
All authors have contributed to the manuscript in significant ways, reviewed, and agreed upon the manuscript.
S.M. and Y.C. defined the research theme. S.M. and Y.C. designed the methods and experiments, carried out the laboratory experiments, analyzed data, and interpreted the results. S.M., Y.C., and M.B.H. discussed the interpretation and presentation.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
Written informed consent was obtained from the patient for publication of this case and accompanying images. A copy of the written consent is available for review by the Editor-in-Chief of this journal on request.
Patient Consent
Written informed consent was obtained for the publication of the patient’s information and images.