
Abstract
Patients with lean nonalcoholic fatty liver disease (NAFLD) may have different metabolic profiles than those with NAFLD. Estrogenic activity is associated with NAFLD pathogenesis. We evaluated the production ability of equol, which has estrogenic activity, in lean NAFLD and assessed their gut microbiota in relation to their equol-producing ability. Among 684 adult participants, 276 (40%) had NAFLD and 293 (43%) were equol producers. The rates of equol producers in the normal and NAFLD groups were 43% and 42%, respectively. Among the patients with NAFLD, 55 (20%) had lean NAFLD of which 18 (33%) were equol producers. The rate of equol production in men with lean NAFLD was 8%, which was the lowest, while the corresponding rate in the other participants was approximately 40%. The gut microbiota composition of equol producers and nonproducers showed many significant differences. The gut microbiota of men with lean NAFLD showed increased abundance of Caulobacter and decreased abundances of Slackia and Terrisporobacter. Thus, almost all men with lean NAFLD lacked equol-producing ability, and their gut microbiota showed a reduced abundance of Slackia, which is related to equol production. The pathology of lean NAFLD in men may be strongly associated with equol-producing ability and gut microbiota.
Introduction
Nonalcoholic fatty liver disease (NAFLD) is one of the most common cause of chronic liver disease worldwide because of the increased rates of obesity and metabolic syndrome associated with lifestyle changes (Loomba & Sanyal, 2013; Younossi et al., 2016). Various pharmacological therapies for NAFLD have been currently examined at several phases of clinical trials (Negi et al., 2022). However, the current practice guidelines recommend only pioglitazone and vitamin E for clinical use (Marchesini et al., 2016). Although obesity and NAFLD are strongly associated, not all patients with NAFLD are obese, especially in Asia (Albhaisi et al., 2019; Seto & Yuen, 2017). This subset of NAFLD is usually referred to as lean NAFLD. Patients with lean NAFLD may have different metabolic profiles than those with NAFLD (Seto & Yuen, 2017). The long-term prognosis of lean NAFLD is even less well-known; some data suggest that these patients may even have worse outcomes than obese individuals with NAFLD (Cruz et al., 2014) and show an increased risk of developing severe liver disease (Hagstrom et al., 2018; Younes et al., 2021). This has led to considerable debate about whether lean NAFLD represents a condition distinct from NAFLD.
The age distribution of lean NAFLD patients has been reported to differ between men and women, with men patients being younger (Tobari et al., 2019; Younes et al., 2021) because the secretion of estrogen before menopause can decrease the risk of NAFLD (Tobari et al., 2019). Equol, a metabolite of soy isoflavone daidzein produced by the gut microbiota, shows estrogenic activity. The ability to produce equol varies among individuals; thus, equol producers only constitute 20% to 30% of the populations in Western countries (Atkinson et al., 2005; Rowland et al., 2000), and 40% to 60% of those in Asian countries (Akaza et al., 2004; Ko et al., 2010). To our knowledge, no previous study has evaluated the association between NAFLD onset and the ability to produce equol.
Thus, the aim of this study was to evaluate the equol production ability in patients with lean NAFLD and to clarify the characteristics of the gut microbiota in relation to lean NAFLD and equol production.
Materials and Method
Study Participants
The Iwaki Health Promotion Project is an ongoing community-based health promotion study of Japanese people (range, 20–88 years) designed to prevent lifestyle-related diseases and prolong the lifespan of this population. This program has been conducted annually since 2005, with more than 1,000 participants in the Iwaki region of Hirosaki City, Aomori Prefecture, located in north Japan (Iino, Endo, et al., 2019; Iino et al., 2018; Iino, Shimoyama, et al., 2019). Study participation was voluntary and occurred in response to public announcements. Approximately 800 data points were collected from each participant, including demographic characteristics, medical history, lifestyle data, NAFLD state, equol production ability, gut microbiota, food consumption pattern, and blood chemical analysis data. The present study on the association between NAFLD and equol production ability is a part of this project. In 2018, a total of 1,056 individuals participated in the project (Figure 1). Of these, we excluded 33 participants with positive results on hepatitis B surface antigen or anti-hepatitis C virus tests, 217 participants with excessive alcohol intake (men, >30 g/day; women, >20 g/day), 9 participants administered agents associated with steatosis, such as amiodarone, methotrexate, prednisolone, and tamoxifen, 27 participants whose stool samples were not collected, 20 participants whose urine was undetectable, and 66 participants whose transient elastography examinations failed or yielded unreliable data. The remaining 684 participants were included in the analysis. A lean state was defined by body mass index (BMI) ≤22 kg/m2.

The Study Flowchart.
Clinical Parameters
The following clinical parameters were recorded: sex, age, height, body weight, BMI (calculated by dividing the weight in kilograms by the squared height in meters), results for hepatitis B surface antigen or anti-hepatitis C virus tests, and the levels of aspartate aminotransferase, alanine aminotransferase, gamma-glutamyl transpeptidase, albumin, total bilirubin, glucose, insulin, hemoglobin A1c, total cholesterol, high-density lipoprotein cholesterol, low-density lipoprotein cholesterol, triglycerides, and platelets.
Diagnosis of NAFLD and NASH
Transient elastography with measurement of the liver stiffness (LS) and the controlled attenuation parameter (CAP), which quantifies hepatic fat, was performed using FibroScan (Echosens, Paris, France). Five well-trained hepatology specialists performed the examinations. In cases where LS or CAP values could not be obtained after at least 10 attempts, the examinations were considered to have failed. LS measurement was considered unreliable if the ratio of its interquartile range with the median LS value was >0.30, with the median LS value set at 7.1 kPa, according to previously established criteria (Boursier et al., 2013). NAFLD was diagnosed when the CAP was ≥237.8 dB (Sasso et al., 2010). NASH (non-alcoholic steatohepatitis) was diagnosed when the LS is ≥7 kPa in NAFLD (Imajo et al., 2016).
Definition of Equol Production Status
The concentrations of equol and daidzein in urine were measured by using a modified high-performance liquid chromatography method (Lundh et al., 1988). Urine samples were deconjugated by incubating with β-glucuronidase/sulfatase (G0876, Sigma), extracted twice with ethyl acetate, and evaporated. Equol production status was defined by a urinary log10-transformed equol/daidzein ratio of −1.75 as described previously (Setchell & Cole, 2006).
Intake of Daidzein
Daidzein intake was calculated based on the results of a brief self-administered diet history questionnaire (BDHQ), a convenient diet assessment questionnaire developed in Japan (Kobayashi et al., 2012). The BDHQ included questions concerning the intake frequency of 58 food and beverage items commonly consumed in Japan. These foods included three traditional Japanese soybean products: natto, tofu, and fried tofu.
Analysis of Gut Microbiota
After overnight fasting, fecal samples from each participant were collected into commercial containers (TechnoSuruga Laboratory Co., Ltd., Shizuoka, Japan) on the morning of the survey (TechnoSuruga Laboratory Co., Ltd., Shizuoka, Japan) and suspended in guanidine thiocyanate solution (100 mM Tris–HCl [pH 9.0], 40 mM Tris–EDTA [pH 8.0], 4 M guanidine thiocyanate). These samples were stored at −80°C until DNA extraction. Frozen fecal solids were beaten with zirconia beads at 5 m/s for 2 min by using a FastPrep 24 Instrument (MP Biomedicals, Santa Ana, CA). DNA was extracted from 200 µL of the suspension by using a Magtration System 12 GC (Precision System Science, Japan), with MagdDEA DNA 200 (Precision System Science, Japan) as the reagent for automatic nucleic acid extraction. Consistent with previous studies, samples were analyzed for a series of typical bacteria in the human gut microbiota by using primers for the V3 to V4 region of the 16S rDNA of prokaryotes (Hisada et al., 2015; Takahashi et al., 2014). Sequencing was conducted using an Illumina MiSeq system (Illumina, San Diego, CA). Quality filtering was performed as follows: Only reads with quality value scores ≥20 for more than 99% of the sequence were extracted for the analysis. Detection and identification of bacteria from the sequences were then performed using Metagenome@KIN software (World Fusion Co., Tokyo, Japan) and the TechnoSuruga Lab Microbial Identification database DB-BA 10.0 (TechnoSuruga Laboratory) at 97% sequence similarity. We calculated the relative abundance of the gut microbiota and the percentage composition of the reads of a bacterium to the total reads of the gut microbiome. A linear discriminant effect size (LEfSe) analysis (https://huttenhower.sph.harvard.edu/lefse/) was performed to identify the members of the microbial community that were present at different levels in comparisons between two groups. We compared the gut microbiota between NAFLD patients and normal individuals, equol producers and non-producers, normal lean men and men with lean NAFLD, and men and women with lean NAFLD.
Statistical Analysis
Statistical analyses of the clinical data were performed using JMP ver. 12.1 (SAS Institute, Cary, NC). Categorical variables are shown as frequencies and percentages, and continuous variables are shown as means with standard deviations. Categorical variables were compared using the chi-square test, and continuous variables were compared using Student’s t test. Groups divided by NAFLD status and lean status were assessed using one-way analysis of variance and Dunnett’s test for post hoc comparisons. Statistical significance was set at p < .05. LEfSe combines the Kruskal–Wallis test or pairwise Wilcoxon rank-sum test with linear discriminant analysis (LDA). LEfSe also ranks features by effect size, providing features that explain most of the biological difference at the top. The LEfSe analysis was performed under the following conditions: α value for the statistical test was 0.01, and the threshold of the logarithmic LDA score for discriminative features was 2.0 (Segata et al., 2011)
Study Approval
This study was performed in accordance with the ethical standards of the Declaration of Helsinki and was approved by the ethics committee (Authorization number: 2018-062). All participants who underwent health examinations as part of the project received an explanation of the details of the examination and principal aims of the study, and written informed consent was obtained prior to study commencement.
Results
Characteristics of NAFLD, NASH, and Equol Producer
Among the 684 participants, 276 (40%) were diagnosed with NAFLD and 293 (43%) were identified as equol producers (Table 1). The rates of equol production in the normal and NAFLD groups were almost the same. Among the patients with NAFLD, 55 (20%) had lean NAFLD (Table 2), of which 18 (33%) were identified as equol producers. There were no significant differences in the rates of equol producers and daidzein intake.
The Rates of NAFLD and Equol Producer in All Subjects.

Note. NAFLD = nonalcoholic fatty liver disease.
Characteristics in All Subjects.

Note. NAFLD = nonalcoholic fatty liver disease; BMI = body mass index; WC = waist circumference; AST = aspartate aminotransferase; ALT = alanine aminotransferase; GGT = gamma-glutamyl transpeptidase; HOMA-IR = homeostasis model assessment of insulin resistance; HbA1c = hemoglobin A1c; HDL = high-density lipoprotein; LDL = low-density lipoprotein; CAP = controlled attenuation parameter; LS = liver stiffness; NASH = non-alcoholic steatohepatitis.
p < 0.05 (compared to the normal lean group), one-way ANOVA and Dunnett’s test for post hoc comparisons.
Reduced Equol Production in Men With Lean NAFLD
When the participants were divided into eight groups based on gender, lean status, and NAFLD status, the rate of equol producers in men with lean NAFLD was 8%, which was the lowest (Table 3). The corresponding rate in the other participants was approximately 40%.
Evaluation of Subjects Divided Into Eight Groups Based on Gender, the Status of Lean, and the Status of NAFLD.

Note. NAFLD = nonalcoholic fatty liver disease; NASH = non-alcoholic steatohepatitis.
Characteristics of Gut Microbiota in Patients With NAFLD and Equol Producer
The gut microbiota of patients with NAFLD and normal participants also showed some differences, including increased abundances of Lactobacillus and Roseburia and reduced abundances of Turicibacter and Eggerthella at the genus level in patients with NAFLD (Figure 2). The gut microbiota of equol producers and nonproducers also showed many differences (Figure 3).
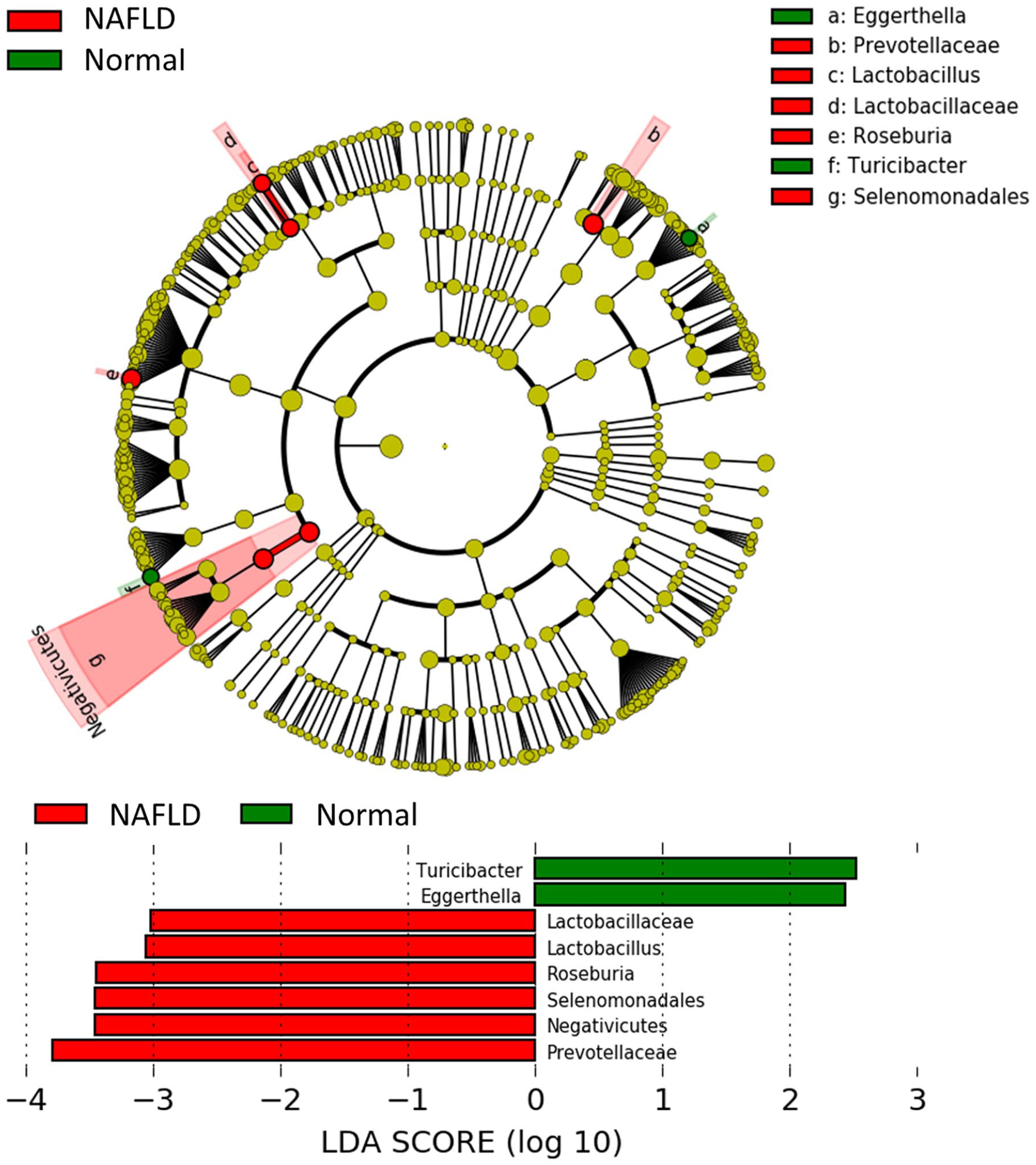
Characteristics of the Gut Microbiota of Patients With NAFLD and Normal Participants. The Relative Abundance of Lactobacillaceae, Lactobacillus, Roseburia, Selenomonadales, Negativicutes, and Prevotellaceae in NAFLD Were Statistically Higher Than Those in Normal Participants. The Relative Abundance of Turicibacter and Eggerthella in NAFLD Were Statistically Lower Than Those in Normal Participants.

Characteristics of the Gut Microbiota of Equol Producers and Nonproducers. The Relative Abundance of 73 Species in NAFLD Was Statistically Higher Than Those in Normal Participants. The Relative Abundance of 38 Species in NAFLD Was Statistically Lower Than Those in Normal Participants.
Comparison Between Men With Lean NAFLD and Normal Lean Men
The comparison between men with lean NAFLD and normal lean men showed significant differences in the rates of equol producers and CAP (Table 4). The gut microbiota of lean men with NAFLD showed lower abundances of equol producers. The LEfSe analysis revealed increased abundances of Caulobacter and Bosea and reduced abundances of Slackia, Terrisporobacter, and Lachnospiraceae at the genus level in men with lean NAFLD (Figure 4). There was no significant difference in the diversity of the gut microbiota between men with lean NAFLD and normal lean men (Shannon index: Median 2.580 vs. 2.617, p = .203; Simpson index: Median 0.880 vs. 0.883, p=.468).
Characteristics of Lean NAFLD and Lean Normal in Men.

Note. NAFLD = nonalcoholic fatty liver disease; BMI = body mass index; WC = waist circumference; AST = aspartate aminotransferase; ALT = alanine aminotransferase; GGT = gamma-glutamyl transpeptidase; HOMA-IR = homeostasis model assessment of insulin resistance; HbA1c = hemoglobin A1c; HDL = high-density lipoprotein; LDL = low-density lipoprotein; CAP = controlled attenuation parameter; LS = liver stiffness; NASH = non-alcoholic steatohepatitis.
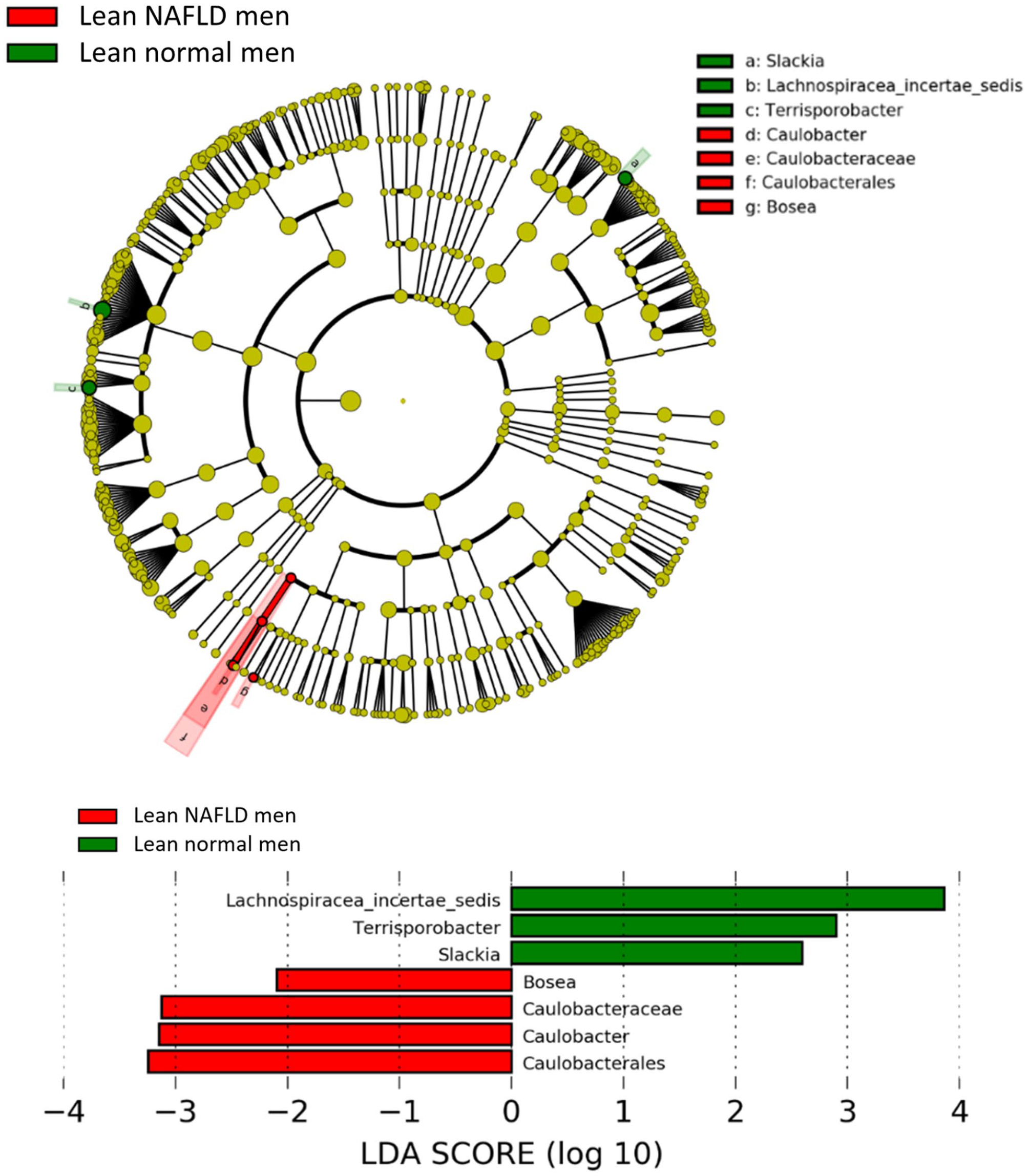
The Comparison of the Gut Microbiota Between Men With Lean NAFLD and Normal Lean Men. The Relative Abundance of Bosea, Caulobacteraceae, Caulobacter, and Caulobacterales in Lean NAFLD Men Were Statistically Higher Than Those in Lean Normal Man. The Relative Abundance of Lachnospiracea Incertae Sedis, Terrisporobacter, and Slackia in Lean NAFLD Men Were Statistically Lower Than Those in Lean Normal Man.
Comparison Between Men and Women With Lean NAFLD
The comparison between men and women with lean NAFLD showed significant differences in the rates of equol producers, alanine transaminase, and high-density lipoprotein (Table 5). LEfSe analysis of the gut microbiota showed increased levels of Caulobacter and Ruminococcus2 at the genus level and reduced levels of Slackia, Terrisporobacter, and Anaerotruncus levels in lean NAFLD patients (Figure 5).
Characteristics of Men and Women in Lean NAFLD.

Note. NAFLD = nonalcoholic fatty liver disease; BMI = body mass index; WC = waist circumference; AST = aspartate aminotransferase; ALT = alanine aminotransferase; GGT = gamma-glutamyl transpeptidase; HOMA-IR = homeostasis model assessment of insulin resistance; HbA1c = hemoglobin A1c; HDL = high-density lipoprotein; LDL = low-density lipoprotein; CAP = controlled attenuation parameter; LS = liver stiffness; NASH = non-alcoholic steatohepatitis.

The Comparison of the Gut Microbiota Between Men and Women With Lean NAFLD. The Relative Abundance of Alphaproteobacter, Caulobacter, and Ruminococcus in Lean NAFLD Men Was Statistically Higher Than Those in Lean NAFLD Woman. The Relative Abundance of Anaerotruncus, Terrisporobacter, and Slackia in Lean NAFLD Men Was Statistically Lower Than Those in Lean NAFLD Woman.
Discussion
The current study demonstrated that almost all men with lean NAFLD lacked the ability to produce equol; their gut microbiota showed unique characteristics with reduced abundance of Slackia at the genus level. To our knowledge, this is the first study to examine the association between NAFLD and equol-production ability and determine the association of the findings with the gut microbiota.
Patients with NAFLD and normal participants showed almost no differences in the rates of equol production. However, only one man with lean NAFLD showed equol-producing ability, whereas, in the remaining 7 groups divided by gender, NAFLD status, and lean status, almost 40% of participants showed equol-producing ability. These findings suggest that the presence of lean NAFLD in men is strongly associated with equol-producing ability. Intestinal bacteria metabolize isoflavone daidzein to O-desmethylangolensin and equol (Rafii, 2015). Bacteria in both ileum and colon are involved in the first metabolism of natural isoflavones. The bacteria converting primary metabolites to secondary are mainly found in the colon. Equol has a high affinity for estrogen receptors. The lack of equol-producing ability would have a lower influence on women because of their high levels of endogenous estrogen. Estrogen is known to protect the liver from NAFLD development. Indeed, the prevalence of NAFLD is lower in premenopausal women who produce endogenous estrogen, than in men, while it is higher in women after menopause than in men (Hamaguchi et al., 2005; Kojima et al., 2003; Yang et al., 2014). The mechanism by which estrogen protects against NAFLD has not been fully elucidated. However, several experimental studies have suggested that estrogens drive fat accumulation in the gluteofemoral subcutaneous adipose tissue and promote free fatty acid β-oxidation in the liver and directly suppress triglyceride synthesis in addition to regulating energy homeostasis, whole-body glucose metabolism, and insulin sensitivity (Ballestri et al., 2017; Varlamov et al., 2014). The antisteatotic and antioxidant roles of estrogen protect against the development of NAFLD (Ballestri et al., 2017; Besse-Patin et al., 2017). In this study analysis of women older than 50 years, the rates of equol production were lowest in lean NAFLD. However, half of the participants in non-lean NAFLD and normal lean had the ability to produce equol. Therefore, in postmenopausal women, equol cannot be a primary factor in the pathogenesis of NAFLD except in that of lean NAFLD.
The gut microbiota of lean NAFLD patients showed unique characteristics. In comparisons between men and women with lean NAFLD, and between normal lean men and men with lean NAFLD, men with lean NAFLD showed a reduced abundance of Slackia at the genus level. The comparisons between equol producers and nonproducers also showed many differences in gut microbiota, including a reduced abundance of Slackia. Slackia includes Slackia isoflavoniconvertens, which converts daidzein to equol. In our previous study, Slackia isoflavoniconvertens was most frequently responsible for equol production in the gut microbiota, which is associated with equol production (Iino, Shimoyama, et al., 2019). Considering the commonly observed decrease in Slackia in the two comparisons, reduced abundance of Slackia appears to be a characteristic of equol nonproducing men with lean NAFLD. These characteristics suggest that lean NAFLD may be strongly associated with equol-producing ability.
Obese men with NAFLD showed the same rates of equol-producing ability as the other participants. Although the underlying mechanisms have not been clarified fully, studies on patients with lean and obese NAFLD have revealed that lean NAFLD shows a distinct metabolic profile and different pathological mechanisms, with adiponectin concentrations, amino acids, bile acids, and gut microbiota being different from those in obese NAFLD (Chen et al., 2020; Feldman et al., 2017). The ability to produce equol, which has strong estrogen action, seems to be an important factor associated with the pathogenesis of lean NAFLD, especially in men.
There were no participants with NASH in men with lean NAFLD, and participants in nonlean NAFLD account for the majority of those with NASH. Similar to this result, a recent study reported that lean NAFLD had a less severe histological disease course compared with non-lean NAFLD (Younes et al., 2021). Half of the participants with NASH were equol producers. Therefore, equol cannot protect sufficiently against the development of liver fibrosis in non-lean NAFLD.
This study had several limitations. First, there was no standard definition for lean NAFLD. The BMI cutoff points for lean NAFLD are not uniform worldwide. The most frequently used definition is NAFLD with a BMI <25 kg/m2 in the Western population and <23 kg/m2 in the Asian population. However, one review for lean NAFLD instead used the definition for the term “lean” in Asia (BMI < 22 kg/m2; Albhaisi et al., 2019). In the current study, the cutoff point for lean NAFLD was defined as 22 kg/m2 because the average BMI of the participants was <23 kg/m2, which is lower than that in a previous study (Eguchi et al., 2012). Second, we did not evaluate the gut microbiota directly between equol producers and nonproducers in men with lean NAFLD, as only one man with lean NAFLD was an equol producer. Therefore, to clarify the characteristics of the gut microbiota in men with lean NAFLD, we compared the gut microbiota between men with lean NAFLD and normal lean men, and between men and women with lean NAFLD. Third, although liver biopsy is required for the diagnosis of NASH, it is an invasive procedure. Performing liver biopsy in this study based on a mass survey would have been unethical. Therefore, NASH was diagnosed when NAFLD participants had liver fibrosis on evaluation by transient elastography.
Conclusion
Almost all men with lean NAFLD lacked the ability to produce equol, and their gut microbiota uniquely showed a reduced abundance of Slackia at the genus level. The pathology of lean NAFLD in men may be strongly associated with their equol-producing ability and specific characteristics of their gut microbiota.
Footnotes
Acknowledgements
This study was based on the Iwaki Health Promotion Project as a project by Hirosaki University Graduate School of Medicine, in collaboration with the Aomori Heath Evaluation and Promotion Center and the Hirosaki City Office. The study was funded by Japan Science and Technology Agency Center of Innovation (grant number JPMJCE1302).
Author Contributions
Conceptualization, C.I.; methodology, C.I.; software, C.I.; validation, C.I.; formal analysis, C.I.; investigation, C.I., K.I., T.E., T.T., S.S., G.I., H.S.; resources, K.I., H.S.; data curation, C.I.; writing-original draft preparation, C.I.; writing-review and editing, C.I.; visualization, C.I.; supervision, K.M., Y.Y., S.N., S.F.; project administration, T.E., S.N. All authors have read and agreed to the published version of the manuscript
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.