
Abstract
Little attention has been given to esophageal disorders in diabetes mellitus. Pathophysiology of esophageal motility disorders (EMD) in patients with diabetes mellitus is multifactorial. The aims of the present study were: (a) to evaluate the prevalence of EMD in patients with Type 2 diabetes mellitus and (b) to determine the relationship between EMD and autonomic neuropathy as assessed by heart rate variability (HRV). All the patients completed a questionnaire about diabetes characteristics and gastrointestinal symptoms. Conventional esophageal manometry was performed in all patients. HRV was measured in three different situations (Lying Position 1, standing position, and Lying Position 2). The temporal and frequency domain parameters were considered for analysis. The prevalence of EMD in our patients was 60.5% (n = 23). Low score physical activity was significantly more frequent in patients with EMD (p = .03). There was an increase in sympathetic activity represented by the low frequency (LF) parameter (p = .027) in the presence of EMD. Whereas parasympathetic modulation of heart rate represented by the high frequency (HF) parameter (p = .027) was declined in patients with EMD compared to those without. The LF/HF ratio was significantly higher (p = .002) in patients with EMD. EMD were prevalent in diabetes mellitus and were associated to autonomic nervous system dysfunction predominantly at the parasympathetic component.
Introduction
Diabetes mellitus (DM) affects different systems of which the gastrointestinal (GI) tract. Fifty to 76% (Annese et al., 1999; Krishnan et al., 2013) of diabetic patients report GI symptoms including esophageal symptoms.
Although little attention has been given to esophageal disorders in DM, the prevalence of esophageal symptoms, such as heartburn and dysphagia, is estimated to be between 25% and 87% (Annese et al., 1999; Gustafsson et al., 2011; Natalini et al., 2015; Wang et al., 2008). Esophageal manometry (EM) is considered to be the gold standard for diagnosing esophageal motility disorders (EMD; Spechler & Castell, 2001). EM assesses esophageal motility patterns by measuring pressure in the esophagus. There are two main types of manometric recording systems: the conventional EM and the high-resolution EM. According to this last technology, there is a new classification scheme of EMD known as the Chicago Classification (Yadlapati et al., 2021). Based on the diagnosis, treatment options can be proposed. In diabetic patients, EM revealed frequencies up to 65% of EMD (Annese et al., 1999; Boronikolos et al., 2015; Gustafsson et al., 2011; Roman et al., 2014). Major patterns of EM abnormalities are incomplete lower esophageal sphincter (LES) relaxation or inadequate basal LES, delayed peristalsis progressing, abnormal amplitude in distal peristaltic waves, or high incidence of simultaneous contractions (>10%).
Pathophysiology of EMD in patients with DM seems to be multifactorial and still unclear (Monreal-Robles & Remes-Troche, 2017). Main mechanisms described include hyperglycemia as well as autonomic neuropathy (AN). In fact, several studies have reported that poor glycemic control is associated with a higher frequency of EMD (Boer et al., 1992; Boronikolos et al., 2015). Esophageal dysfunctions occur frequently in patients with diabetic autonomic neuropathy (DAN; Ascaso et al., 2006; Channer et al., 1985). The prevalence of EMD in diabetic patients with AN varies widely according to studies ranging from 13% to 70% (Annese et al., 1999; Jermendy et al., 1991; Kinekawa et al., 2001; Ohlsson et al., 2006). The aims of the present study were: (a) to evaluate the prevalence of EMD in patients with DM (T2DM), and (b) to determine the relationship between EMD and AN as assessed by heart rate variability (HRV).
Patients and Methods
This study was approved by the Ethics Committee of Farhat HACHED Hospital, Sousse, Tunisia; approval number: 291012). Patients were recruited from primary health care centers of the governorate of Sousse (Tunisia) given that the data to be collected were the same for all the diabetics followed within the framework of a public health strategy. This choice allowed more homogeneity in the information obtained on the population under study. The selection of patients was made taking into account the inclusion criteria. All patients gave written, informed consent before participating in the study.
Study Design
This cross-sectional study was conducted at the Department of Functional Explorations of Nervous System Exploration (Sahloul Hospital, Sousse, Tunisia). Patients with one or more of the following criteria were not included in the study: Type 1 diabetes, gestational diabetes, severe renal failure demanding dialysis, severe cardiac disease, a recent cerebrovascular accident, history of esophageal tumor or surgery, AN secondary to another associated pathology (scleroderma, Parkinson disease. . .), intake of heart rate (HR) affecting drugs’ (beta-blockers, beta-agonists, tricyclic antidepressants. . .), dementia, psychosis.
At the time of inclusion, the patients completed a questionnaire concerning socio-demographic data. Physical activity was evaluated by the Voorrips physical-activity questionnaire to calculate a total score which classifies the patients as high, moderate, or low in daily physical activity (Voorrips et al., 1991).
Duration of diabetes, drug treatments, the last glycosylated hemoglobin (HbA1c), and fasting glucose levels were recorded from the medical reports of primary health care center. Diabetic complications were also noted: retinopathy (based on fundus photography), microalbuminuria, peripheral neuropathy (PN) based on Neuropathy Total Symptom Score (NTSS; Bastyr et al., 2005). AN was described according to established clinical criteria: orthostatic hypotension, resting tachycardia, impaired hypoglycemia awareness, sexual and vesico-sphincteric dysfunction, profound sweating, and abnormal pupillary responses (Vinik et al., 2003).
The following symptoms related to complications of the GI tract were also included in the questionnaire, namely, dysphagia, heartburn, regurgitation, eructation, meal-related cough, chest pain, abdominal fullness, early satiety, epigastralgia, nausea, vomiting, bloating, diarrhea, constipation, dyschesia, incontinence, weight loss, loss of appetite and symptomatic postprandial hypoglycemia (Vinik et al., 2003). Physical examination was carried out to measure body mass index (BMI), capillary blood glucose, and orthostatic blood pressure. Patients were asked to fast overnight and the study of EM and HRV were realized at the same time of day (8h00–10h00) in the morning to avoid the influence of diurnal variation.
Esophageal Manometry
Conventional EM was performed by a water perfusion catheter (MMS probe E4-5-5-5) connected to external transducers perfusion pump. The LES resting pressure was measured during a slow pull-through at the end of expiratory phase. Esophageal body motility function analysis was performed using a series of 10 wet swallows with 5 mL water each separated by 30 s.
The EMD was diagnosed if patients fulfilled one or more of the following five criteria (Spechler & Castell, 2001):
resting pressure in LES <10 or >45 mmHg,
relaxation pressure in LES >8 mmHg,
speed of the peristaltic wave <2 or >8 cm/s in the distal esophagus,
mean peristaltic contraction amplitude <30 or >180 mmHg in the esophagus,
Percentage of simultaneous, nonpropulsive peristaltic waves in the esophagus > 10%.
HRV Study
Patients were instructed to abstain from intense effort at least 2 hr before the start of the test and during the duration of the recording of the HR (Voss et al., 2015). The patient was installed in a quiet room, relieved (empty bladder and rectum), without too bright light. All tests were preceded by a resting period of at least 15 min in supine position. HRV was recorded for 7 min in three successive positions (supine, standing, and supine) using Polar S810i watch (Polar Electro Oy, Finland, 1,000 Hz). HRV data analysis was carried out using the Kubios HRV software (University of Eastern Finland, Kuopio, Finland).
From time domain, the following standard HRV indices were calculated according to the Task Force of the European Society of Cardiology (Voss et al., 2015): (a) sdNN (ms): standard deviation of NN interval time series, (b) pNN50 (%): percentage derived by dividing the number of interval differences of successive NN intervals >50 ms by the total number of NN intervals, and (c) rMSSD (ms): square root of the mean squared differences of successive NN intervals.
From power spectra (Fast Fourier transformation), the following frequency domain standard HRV indices were determined: (a) low frequency (LF; ms²): power in the “low” frequency band 0.04 to 0.15 Hz and LF (n.u): normalized LF power = LF / (LF + HF); (b) high frequency (HF; ms²): power in the “high” frequency band 0.15 to 0.4 Hz and HF (n.u): normalized HF power = HF / (LF + HF); and (c) LF / HF: ratio between LF and HF.
The Poincaré plot analysis, which is a geometrical and nonlinear quantitative method for the evaluation of the HRV dynamics (Voss et al., 2015), was also analyzed by calculating three indices: (a) SD1 (ms): standard deviation of the short-term NN interval variability, (b) SD2 (ms): standard deviation of the long-term NN interval variability, and (c) SD1/SD2: ratio between SD1 and SD2.
Statistical Analysis
All statistical analyses were carried out by Statistica version 6.0. All variables were analyzed for normal distribution by Kolmogorov–Smirnov test. Qualitative variables were expressed as absolute numbers and percentages while quantitative variables as median mean ± SD.
The two-way analysis of variance (ANOVA) was performed to study the parameters of HRV in patients with or without EMD in the three recording positions. A p value of .05 was accepted as significance level.
Results
Prevalence of Esophageal Motility Disorder
EM was done in 38 male patients suffering from T2DM. EMD were identified in the majority of patients, with a prevalence of 60.5% (n = 23). The most frequent EMD in our study were abnormalities of the LES pressures (Table 1). Half (n = 19) of the patients had a low resting pressure of the LES and 39.5% (n = 15) presented a defect of relaxation of LES.
Esophageal Manometric Abnormalities in Patients.
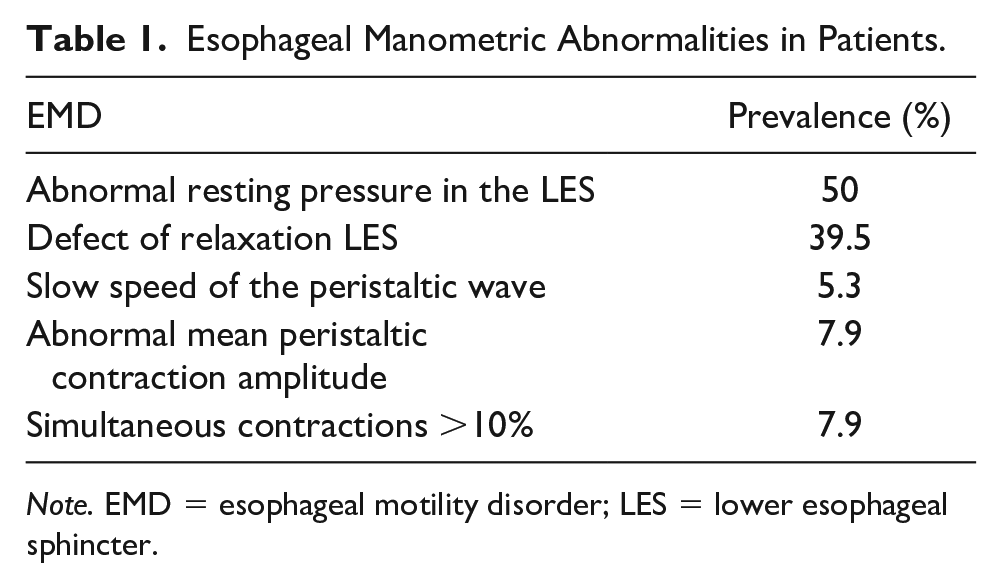
Note. EMD = esophageal motility disorder; LES = lower esophageal sphincter.
The main characteristics of our patients were detailed in Table 2. Low score physical activity was significantly more frequent in patients with EMD (p = .03).
Characteristics of Patients With Normal and Abnormal Esophageal Motility.

Note. BMI = body mass index.
Heartburn affected almost a third of our study population (n = 13; 34.2%) and was also the most prevalent symptom seen in patients with EMD (n = 10; 43.5%; Table 3). However, there was no correlation between EMD and GI symptoms.
Prevalence of Gastrointestinal Symptoms in Patients With Normal and Abnormal Esophageal Motility.

The clinical signs of autonomic nervous system (ANS) dysfunction, namely exercise intolerance and resting tachycardia, were the most frequent (n = 9; 39.1%) within diabetes presenting EMD (Table 4). However, there was no significant difference in the presence or absence of EMD for all signs of diabetic dysautonomia.
Prevalence of Clinical Signs of Autonomic Nervous System Dysfunction in Patients With Normal and Abnormal Esophageal Motility.

Heart Rate Variability and Esophageal Motility Disorders
HRV was evaluated through its temporal and frequency domain parameters measured in three different situations (Lying Position 1, standing position, and Lying Position 2) for both patients with and without EMD (Table 5).
Heart Rate Variability Parameters in Patients During the Three Positions.

Note. P < .05 was considered statistically significant. rMSSD = square root of mean squared differences of successive RR intervals; pNN50 = percentage of RR intervals with more than 50 ms variation; SDNN = standard deviation of RR intervals; LF = low frequency; HF = high frequency; LF/HF = low frequency/high frequency ratio; SD1 (ms) = standard deviation of the short-term normal-to-normal interval variability; SD2 (ms) = standard deviation of the long-term normal-to-normal interval variability; SD1/SD2 = ratio between SD1 and SD2.
The levels of temporal domain indices (rMSSD, pNN50, and SDNN) were comparable between the two groups of patients with and without EMD during the three positions.
Considering frequency domain, all indices (LF, HF, and LF/HF) differed significantly between the two groups in standing position. Indeed, there was an increase in sympathetic activity represented by the LF parameter in the presence of EMD. Whereas parasympathetic modulation of HR represented by the HF parameter was declined in patients with EMD compared to those without. Thus, the LF/HF ratio was significantly higher in patients with EMD.
The nonlinear HRV indices (SD1, SD2, and SD1/SD2) were no different between the two groups in the three positions.
Discussion
The aims of our study were to evaluate the prevalence of EMD in patients with T2DM and to determine the relationship between EMD and AN as assessed by the HRV. Thus, our major findings were a relatively high prevalence of EMD in population of T2DM and the presence of AN in patients with EMD.
The prevalence of EMD in our study population was comparable to other studies whether they used the conventional EM (Annese et al., 1999; Gustafsson et al., 2011; Ohlsson et al., 2006) or esophageal high-resolution manometry (Boronikolos et al., 2015; Roman et al., 2014).
The most frequent EMD identified in our study were abnormalities of the LES pressure mainly a low resting pressure or a defect of relaxation. Nevertheless, the data in the literature remain controversial. In agreement with our research, several studies have reported a low resting pressure of the LES (Annese et al., 1999; Hüppe et al., 1992) while others have rather observed an elevated pressure (Ascaso et al., 2006; Hollis et al., 1977). In addition, few studies reported a defect of relaxation of the LES exclusively in patients compared to the control group (Thayer et al., 2012).
Progression of the peristaltic waves of esophageal body (velocity) was slow in 5.3 % of our patients. Most of the literature data confirm the presence of velocity deceleration in DM (Hollis et al., 1977; Jorge et al., 2012; Roman et al., 2014; Thayer et al., 2012).
The amplitude of the esophageal body peristalsis was normal in almost all of the patients (92%) as reported in other studies (Annese et al., 1999; Ascaso et al., 2006; Jorge et al., 2012). Some studies have instead reported a decrease in the mean amplitude of contractions in patients (Hüppe et al., 1992; Thayer et al., 2012).
In our study, control of diabetes was evaluated using fasting glucose and serum HbA1c levels. The majority of patients with EMD had a poor glycemic control, without reaching the level of significance (Table 2). Previous studies have reported that poor glycemic control was associated with a higher frequency EMD (Boronikolos et al., 2015; De Boer et al., 1992). It should be emphasized that the pathophysiology of esophageal alterations in diabetes is complex and multifactorial. Chronic hyperglycemia induces esophageal remodeling and therefore an alteration of its biomechanical properties (Zhao & Gregersen, 2016). Thus, glycemic imbalance could be the cause behind EMD but also a consequence of slowing transit by decreased esophageal motility (Holloway et al., 1999) which increases the occurrence of postprandial hypoglycemia (Ohlsson et al., 2006).
In this study, we noted that low physical activity score was significantly associated with EMD. This result could be due to the role of physical activity in improving glycemic control, which is known to decrease the occurrence of GI complications of diabetes including EMD (Colberg et al., 2016; Healy et al., 2007; Hu et al., 1999). Indeed, transient relaxations of the lower esophageal and deceleration of peristalsis are more frequent in the presence of hyperglycemia (Boer et al., 1992).
The majority of our patients suffered from GI symptoms with heartburn and dysphagia being the most common. However, none of these symptoms was associated with objectively measured esophageal dysmotility. This result is in agreement with most of the studies (Annese et al., 1999; Clouse, 2002; Gustafsson et al., 2011; Ohlsson et al., 2006; Roman et al., 2014). Indeed, EMD were present in up to 60% of asymptomatic diabetics according to Clouse et al (Clouse, 2002). The absence of clinical manifestation in diabetics with EMD may be explained by the esophageal sensory alterations due to neuropathy of long progression in DM, namely, hyposensitivity and reduced sensations (Frøkjær et al., 2007).
ANS dysfunction was assessed in the present study by looking for clinical signs, orthostatic hypotension and by measurement HRV. Resting tachycardia and exercise intolerance were the most frequent signs of AN in our patients with and without EMD but the difference was not significant as reported elsewhere (Rothstein, 1990). Orthostatic hypotension was not significantly correlated with the presence of EMD, as it has been notified by other studies (Annese et al., 1999; Roman et al., 2014).
The measurement of HRV is considered as noninvasive and reliable way to assess ANS (Kamath & Fallen, 1993). The assessment of the HRV is valid as the Ewing test (Sucharita et al., 2011) and this for the recordings of both long (24 hr) and short duration (Chen et al., 2015). We measured HRV in three different positions in order the study the sympathovagal balance (Perini & Veicsteinas, 2003). Indeed, in healthy subjects, sympathetic nervous function preponderates in vertical position, while vagal function predominates in supine position. From the supine to the standing position, we noted in patients with EMD, a significant increase in sympathetic activity as represented by the LF parameter and a decline in parasympathetic modulation of HR as represented by the HF parameter. Thus, the LF/HF ratio or the sympathovagal balance was significantly higher in patients with EMD.
Consequently, through these results, we demonstrated that patients with EMD had an ANS dysfunction, predominantly on the parasympathetic component. In fact, AN in DM affects both the sympathetic and parasympathetic components of the ANS (Pop-Busui, 2010; Takase et al., 2002). It has been proven that parasympathetic nervous system dysfunction precedes that of sympathetic one as suggested by our study. We conclude through these results that there is an association between EMD in DM and AN.
The pathogenesis of EMD in diabetes has long been debated but no consensus has yet been well established given the controversial results of the different studies. The lack of homogenization of the results was mainly caused by methodological differences. Consistent with our results, two studies using Ewing’s testing (Vannini et al., 1989) concluded that the ANS was affected in patients with EMD. Other studies (Jermendy et al., 1991; Kinekawa et al., 2001; Ohlsson et al., 2006) have not reported a correlation between EMD and AN. Although Kinekawa et al. (2001) used HRV but it is important to emphasize that their analysis was based only on time domain parameter, whereas in the present study, a complete analysis in both time and frequency domains was carried out.
Our study has several limitations. Our sample size was relatively small. This was due to the highly restrictive required inclusion and exclusion criteria established in order to minimize the influence that diseases or conditions could have on the evaluation of the AN system. We aimed to include a control group of healthy subjects but they were reluctant to do EM (mistakenly perceived as painful).
We did not use the high-resolution manometry which is actually the best technique to analyze esophagogastric junction compared to the conventional technique (Roman et al., 2016). Indeed high-resolution technique remains more expensive than the conventional one.
In summary, EMD were prevalent in DM and were associated to ANS dysfunction predominantly at the parasympathetic component.
Footnotes
Acknowledgements
The authors would like to express their sincere gratitude to the patients who contributed to this study.
Author contributions
G.S. contributed to conception and design of the work. G.S., K.M., and L.I. contributed to data collection. G.S., K.M., K.H., and L.I. contributed to data analysis and interpretation. G.S., K.M., and L.I. contributed to drafting the article. G.S. and L.I. critically revised the article. G.S., K.M., K.H., and L.I. approved the final version to be published. All authors read and approved the final manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.