
Abstract
This research aims to describe and compare the effects of partial-body cryotherapy (PBC) and cold-water immersion (CWI) on the physiological responses of soccer players after cycling in a hot and humid environment. Sixteen elite soccer players participated in three experiments, and received CWI (13°C for 15 min), PBC (110°C−140°C for 3 min), and CON (room temperature: 21°C ± 2°C), respectively, after aerobic and anaerobic cycling in a hot and humid environment (temperature: 35°C–38°C; humidity: 60%–70%). Heart rate (HR), blood lactate (BLa-), perfusion index (PI), oxygen saturation (SaO2), core temperature (Tc), skin temperature (Ts), and rating of perceived exertion (RPE) were assessed at baseline and through 20 min (5-min intervals). HR was lower in CWI than CON after 20 min (p < .05). SaO2 was higher in CWI than PBC and CON between 10 and 20 min (p < .05). Tc was lower from CWI and PBC than CON between 10 and 20 min (p < .05). Ts was lower in PBC than CWI between 15 and 20 min (p < .05). RPE was lower in PBC than CON 20 min after the exercise (p < .05). No main group differences for BLa- and PI were observed. The physiological effects of PBC are generally similar to CWI. Compared with CON, both CWI and PBC could promote the recovery of physiological indexes within 20 min of exercise in a hot and humid environment. However, PBC can lead to a decrease in SaO2 due to excessive nitrogen inhalation.
Keywords
Introduction
The adverse effects of a hot and humid environment on football are a growing concern worldwide (Nassis et al., 2015). For example, Qatar, which will host the 2022 World Cup, is a country with high temperatures, and FIFA has had to move the tournament from summer to winter to ensure safety and high quality (Sofotasiou et al., 2015). When athletes compete in hot and humid environments, their ability to dissipate heat will be limited, leading to a decrease in sports performance (Stachenfeld, 2014). It can also lead to dehydration and shock, life-threatening in severe cases (Laitano et al., 2020), so it is essential to lower body temperature and recover quickly.
Cold therapy has been widely proven as a quick and effective measure to lower body temperature and has been introduced into sports science (Costello et al., 2012; Kwiecien et al., 2019; Lombardi et al., 2017). Studies suggest that the mechanism by which cold exposure promotes recovery is due to its vasoconstrictive effect and subsequent reduction in inflammation and metabolism (Hohenauer et al., 2020). Furthermore, as an effective recovery measure, cold therapy has been increasingly used in high-level football teams in recent years (Elias et al., 2013; Russell et al., 2017). In sports science, cold-water immersion (CWI) and partial-body cryotherapy (PBC) are two commonly used forms of cold therapy.
CWI is a traditional treatment method that has been extensively studied for its effectiveness in promoting post-exercise recovery in early published studies (J. Leeder et al., 2012; J. D. C. Leeder et al., 2019). One study reported that CWI significantly reduced rectal temperature in cyclists and maintained endurance during subsequent high-intensity exercise (Peiffer et al., 2010). Another study identified that following intermittent-sprint exercise in the heat, CWI accelerated the thermal and cardiovascular load reduction immediately and 2 hr post-recovery (Pointon et al., 2012). Besides, a previous study has reported that CWI immediately after a one-off soccer match reduces muscle damage and discomfort, possibly contributing to a faster recovery of neuromuscular function (Ascensao et al., 2011). The efficiency of CWI to achieve these effects under strict laboratory conditions has not been well studied.
PBC is an emerging cold treatment that has received much attention recently. During this treatment, participants stand upright in a head-free cabin, and cold air is produced through the vaporization of liquid nitrogen. The treatment temperature of the vaporized air can reach up to −195°C with exposure times of up to 3 min (Bouzigon et al., 2016). The study has shown that PBC (−180°C, 3 min) can significantly lower skin temperature (Ts) and core temperature (Tc; Hoshikawa et al., 2019). Another study reported that PBC could lower heart rate and boost post-training recovery (Piras et al., 2019). However, the physiological profile of PBC intervention after high-intensity intervals training in hot and humid environments has not been well studied.
Although no single marker can be taken as an indicator for acute recovery, the regular monitoring of a combination of factors is proposed to be the best strategy (Meeusen et al., 2013). Well-known indicators describing the acute recovery of the cardiovascular and subjective recovery are heart rate (HR), blood lactate (BLa-), perfusion index (PI), oxygen saturation (SaO2), Tc, Ts, and rating of perceived exertion (RPE; McCarthy et al., 2016; Vaile et al., 2011). Heart rate is a vital monitoring indicator used by all scientific teams in football (Akenhead & Nassis, 2016). HR, BLa-, PI, and SaO2 can all assess the state of the circulatory system. It has been widely proven that cold treatment reduces body temperature (Costello et al., 2012). More about those indicators after CWI or PBC have consistently been reported (Hohenauer et al., 2019; Vaile et al., 2011).
To sum up the above, it is essential to explore the physiological responses of PBC and CWI on football players after high-intensity intervals in hot and humid environments. Furthermore, although CWI and PBC are popular and competing strategies for post-exercise recovery, to our knowledge, no direct comparison of changes in physiological function between CWI and PBC following exercise in a humid heat environment has been published. Therefore, this study aimed to describe and compare the effects of CWI and PBC on the circulatory system, body temperature, and RPE within 20 min of exercise in a humid heat environment. It also provides help for applying these two cold interventions in practice.
Materials and Method
Participants
Sixteen elite male soccer players (mean ± SD; age = 22.0 ±1.9 years; height = 179.1 ± 7.8 cm; weight = 71.2 ±8.7 kg; body mass index [BMI] = 22.2 ± 1.7 kg/m2) from football academy in
Experimental Design
The study was a randomized effect study with repeated measures. Participants visited the Exercise and Environment Laboratory of
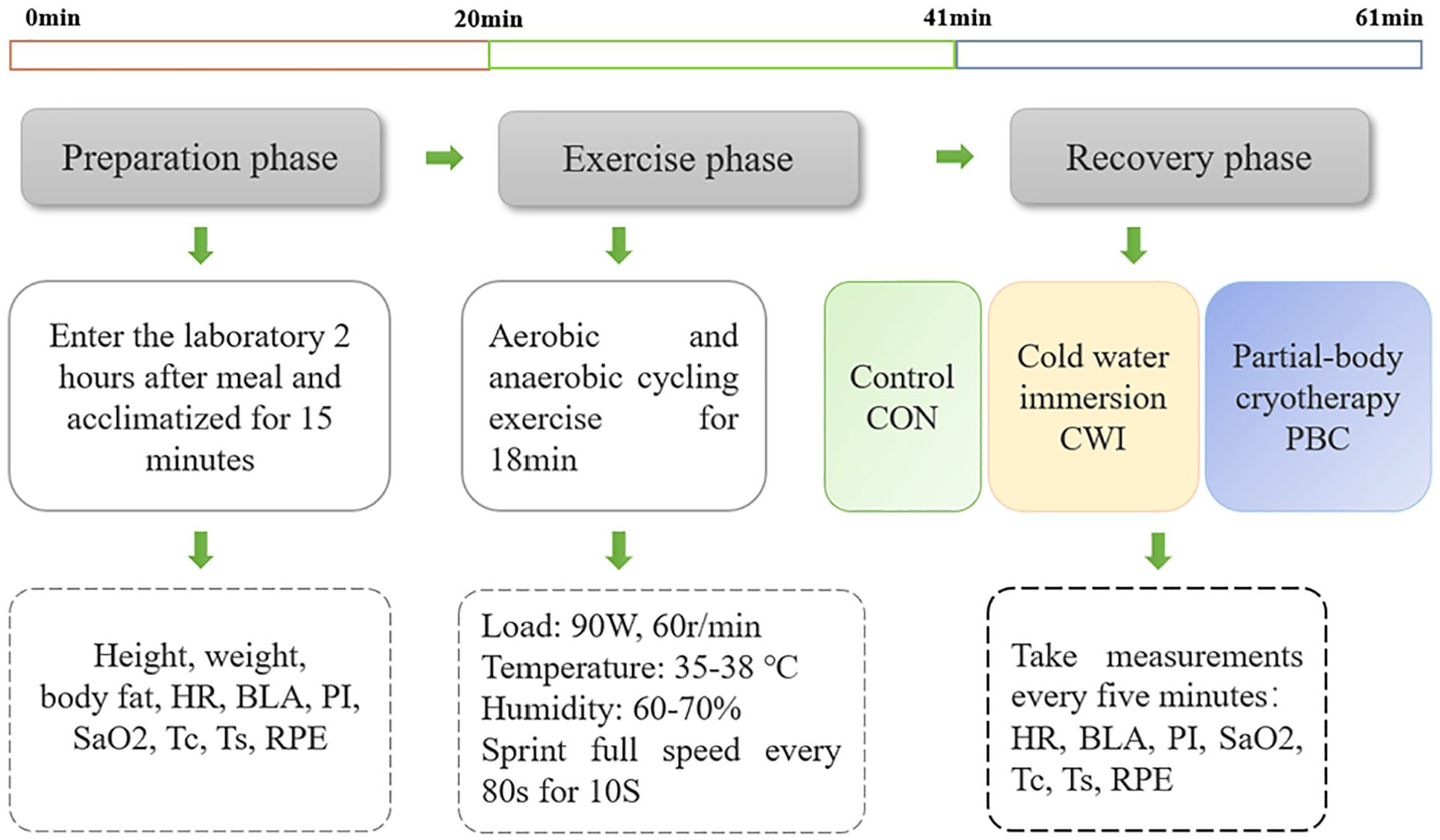
Schematic of the Experimental Protocol
Experimental Environment Control
Two conditions can be called hot environments: living environments above 35°C and working environments above 32°C (Rupp et al., 2015). According to the relationship between ambient temperature and human thermal balance, an environment with relative humidity above 60% is usually called high humidity (Fang et al., 2019).
In this research, the experiment was conducted in the environmental simulation laboratory of
Exercise Scheme
The exercise scheme is designed to combine aerobic and anaerobic exercise to make it more in line with the football game (refer to the
Cold Treatments
After an exercise in a hot and humid environment, the participants received one of the two cold treatments (either CWI or PBC) or the control (CON) condition in a randomized order.
The CWI was performed with cold treatment equipment manufactured by iCoolSport of Australia. The water in the cold treatment pool can be reduced and kept constant within the set temperature range by water cycle refrigeration. The temperature of cold water immersion was set at 13°C, the duration was 15 min (Machado et al., 2016), and intervention started from the fifth minute after exercise. The subject was wearing swimming trunks and immersed in water below the navel.
During PBC, participants entered a mobile cryocabin (Krion KAET-01, Russia) and were exposed to vaporized liquid nitrogen for a total duration of 3 min. The temperature range of PBC is from −110°C to −140°C, and intervention starts from the fifth minute after exercise. This experimental setup was already used in the previously published studies (Costello et al., 2012; Polidori et al., 2018b). During this treatment, participants wore woolen boots as recommended by the manufacturer. Participants were instructed to place their hands at the edge of the cabin. After the 3 min lasting treatment, participants laid down supine for the follow-up measurements.
During CON, participants received no treatment and rested in bikinis in a supine position for 20 min (room temperature: 21°C ± 2°C, relative room humidity: 45% ± 5%).
Physiological Measurements
Blood Circulation System
Indicators related to the blood circulation system include HR, BLa-, PI, and SaO2. The HR was continuously monitored by Polar RS800CX BIKE. After entering the laboratory, subjects wore Polar RS800CX BIKE, and the HR was recorded at the required time. Lactate Plus™ BLa- analyzer, Nova Biomedical, USA, was used for BLa- testing. A calibration test is performed before the test, BLa- is tested at the required time points, and the results are recorded. PI and SaO2 were monitored continuously using Masimo Radical-7. The tester was clamped on the nondominant ring finger of the subject, and the PI and SaO2 were recorded at the required time point.
Body Temperature
In the present study, body temperature includes measuring Tc and forehead Ts. Tc is replaced by ear temperature, the most popular noninvasive measuring Tc. Ear temperature was measured using Terumo (model EM* 30CPL) electronic thermometer and tested by the same tester.
The commonly used multipoint comprehensive calculation of skin temperature did not apply to this experiment, as subjects were immersed in water below their navel during the cold-water immersion. In the present study, the TIR 1 infrared thermography instrument produced by Fluke company was used to measure the skin temperature, replaced by the facial forehead temperature. The test position was kept consistent during each measurement to ensure the accuracy of the data.
Rating of Perceived Exertion
RPE is one of the most widely used subjective perception scales, a significant correlation between RPE and psychological and physiological indexes in sports. The present study measured the subjective feeling of exercise-induced fatigue by the exercise self-perception 6 to 20 scale.
Data Analysis
Descriptive results are reported as means ± standard deviations (SD). The assumption of normality was verified using the Shapiro–Wilk test. The physiological and recovery variables were analyzed using repeated-measures analyses of variance (ANOVAs) mixed design with treatment (CWI, PBC, and CON) as between factor, and time (baseline, 0, 5, 10, 15, and 20 min) as within factor (see Figure 1). Post hoc analyses using Bonferroni correction were performed where appropriate. One-way ANOVAs with Tukey corrected post hoc analyses were used to evaluate the differences between CWI, PBC, and CON per time point (baseline, 0, 5, 10, 15, 20 min). The effect size was expressed as partial eta squared (η2partial) values, with 0.01, 0.06, and 0.14 considered small, medium, and large, respectively. All statistical analyses were performed using the Statistical Package for the Social Sciences (SPSS Inc.), Version 25.0, with the level of significance set at p < .05.
Results
Blood Circulation System
HR
No significant treatment effect (F2, 45 = 0.046, p = .955, η2partial = 0.002) was observed for HR. However, a significant time effect (F5, 41 = 991.426, p < .001, η2partial = 0.991) and Treatment × Time interaction (F10, 84 = 3.924, p < .001, η2partial = 0.318) were evident. In all three groups, HR decreased after the exercise. HR was significantly lower in the CWI group compared with the CON group after 20 min (CWI 20 min: 78.94 ± 11.16 bpm vs. CON 20 min: 88.81 ± 13.06 bpm, p = .016). No differences were detected between PBC and CON for HR (Figure 2).

Dynamic Changes of HR in Each Group
Blood Lactate
A significant time effect (F5, 41 = 80.003, p < .001, η2partial = 0.907) and Treatment × Time interaction (F10, 84 = 0.825, p < .001, η2partial = 0.089), but no significant treatment effect (F2, 45 = 0.198, p = .821, η2partial = 0.009) were observed in BLa-. BLa- decreased in all three groups throughout the 20-min follow-up period (Figure 3).

Dynamic Changes of BLa- in Each Group
Perfusion Index
For PI, despite no significant treatment effect (F2, 45 = 1.524, p = .229, η2partial = 0.063) or Treatment × Time interaction (F10, 84 = 1.832, p = .067, η2partial = 0.063), a significant time effect (F5, 41=4.803, p = .002, η2partial = 0.369) was observed (Figure 4).

Dynamic Changes of PI in Each Group
Oxygen Saturation
For SaO2, a significant treatment effect (F2, 45 = 9.529, p<.001, η2partial = 0.298), time effect (F5, 41=16.846, p<.001, η2partial= 0.673), and Treatment × Time interaction (F10, 84 = 3.009, p = .003, η2partial = 0.264) were observed. In the CON and PBC group, SaO2 decreased over time, whereas it increased in the CWI group. No differences were observed between PBC and CON at any time point. SaO2 values were significantly higher in the CWI versus the CON group after 10 min (CWI 10 min: 97.94% ± 0.93% vs. CON 10 min: 96.69% ± 0.79%, p =.002), 15 min (CWI 15 min: 97.75% ± 1.34% vs. CON 15 min: 96.50% ± 0.73%, p =.01), and 20 min (CWI 20 min: 98.38% ± 0.96% vs. CON 20 min: 96.81% ± 0.83%, p < .001). SaO2 was also higher in the CWI compared with the PBC group after 10 min (CWI 10 min: 97.94% ± 0.93% vs. PBC 10 min: 96.06% ± 1.34%, p < .001), 15 min (CWI 15 min: 97.75% ± 1.34% vs. PBC 15 min: 96.31% ± 1.08%, p = .007), and 20 min (CWI 20 min: 98.38% ± 0.96% vs. PBC 20 min: 96.38% ± 1.41%, p < .001) (Figure 5).
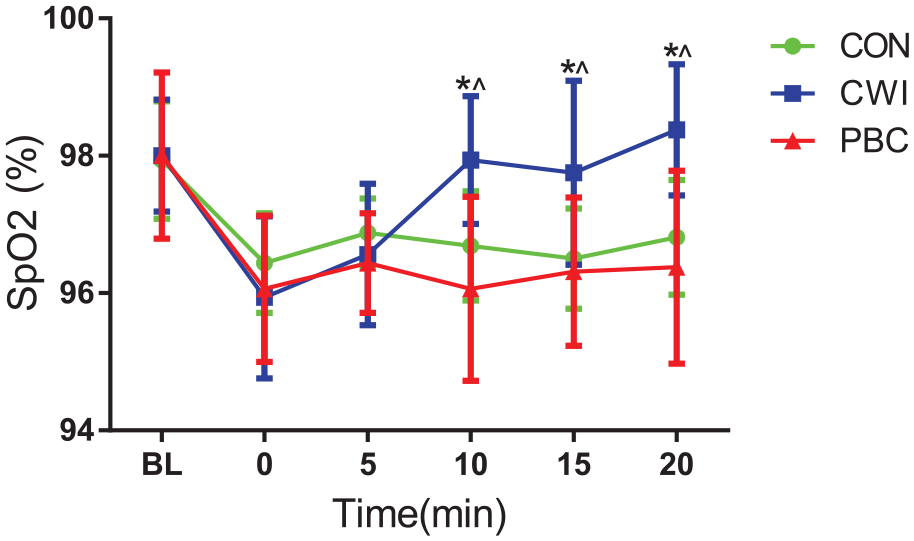
Dynamic Changes of SpO2 in Each Group
Body Temperature
Core Temperature
For Tc, a significant treatment effect (F2, 45= 3.854, p = .029, η2partial= 0.146), time effect (F5, 41= 265.583, p < .001, η2partial= 0.970), and Treatment × Time interaction (F10, 84=9.241, p < .001, η2partial = 0.524) were observed. In all three groups, Tc decreased after the exercise. Tc values were significantly lower in the CWI versus the CON group after 10 min (CWI 10 min: 36.48 ± 0.35°C vs. CON 10 min: 36.88 ± 0.33°C, p =.005), 15 min (CWI 15 min: 36.01°C ± 0.43°C vs. CON 15 min: 36.58°C ± 0.41°C, p <.001), and 20 min (CWI 20 min: 35.78°C ± 0.41°C vs. CON 20 min: 36.21°C ± 0.38°C, p < .001). Tc was also lower in the PBC compared with the CON group after 10 min (PBC 10 min: 35.99°C ± 0.45°C vs. CON 10 min: 36.88°C ± 0.33°C, p < .001), 15 min (PBC 15 min: 35.78°C ± 0.40°C vs. CON 15 min: 36.58°C ± 0.41°C, p < .001), and 20 min (PBC 20 min: 35.84°C ± 0.40°C vs. CON 20 min: 36.21°C ± 0.38°C, p = .011). Furthermore, Tc was higher in the CWI compared with the PBC group after 10 min (CWI 10 min: 36.48°C ± 0.35°C vs. PBC 10 min: 35.99°C ± 0.45°C, p = .001) (Figure 6).
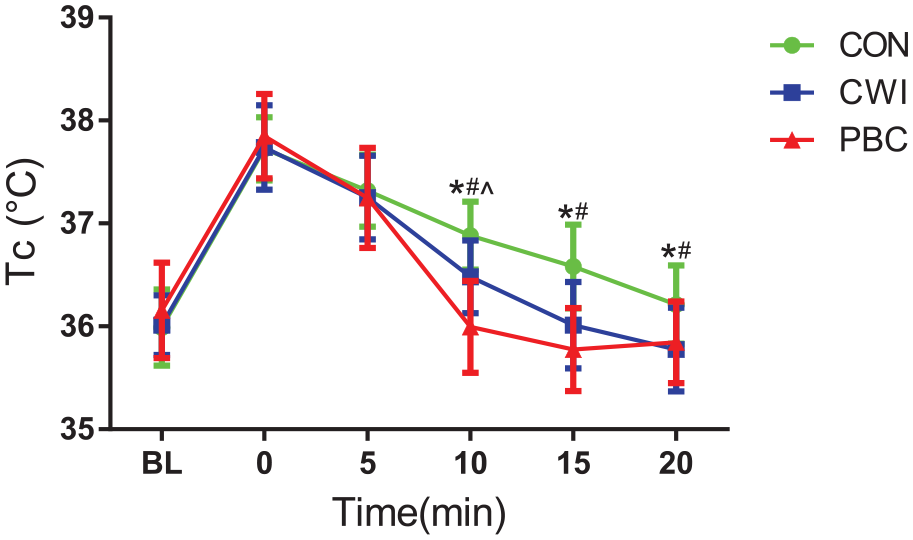
Dynamic Changes of Tc in Each Group
Forehead Skin Temperature
A significant time effect (F5, 41= 39.032, p < .001, η2partial= 0.826), but no treatment effect (F2, 45=1.102, p = .341, η2partial= 0.047), or Time × Treatment interaction (F10, 84= 0.605, p = .805, η2partial = 0.067) was observed in forehead skin temperature. In all three groups, forehead skin temperature showed decreasing first and then rising. Forehead skin temperature was significantly higher in the CWI compared with the PBC group between 15 min (CWI 15 min: 35.41°C ± 0.64°C vs. PBC 15 min: 34.80°C ± 0.80°C, p = .030) and 20 min (CWI 20 min: 35.31°C ± 0.84°C vs. PBC 20 min: 34.66°C ± 0.67°C, p = .025) (Figure 7).

Dynamic Changes of Ts in Each Group
Rating of Perceived Exertion
No significant treatment effect (F2, 45= 0.897, p = .415, η2partial= 0.038) or Treatment × Time interaction (F10, 84= 0.623, p = .790, η2partial = 0.069), but a significant time effect (F5, 41=53.160, p < .001, η2partial = 0.866) were observed for RPE. RPE decreased in all three groups throughout the 20-min follow-up period. RPE was significantly lower in the PBC group compared with the CON group 20 min after the exercise (PBC 20 min: 7.69 ± 1.54 vs. CON 20 min: 9.19 ± 1.97, p = .035). No differences were detected between CWI and CON for RPE (Figure 8).

Dynamic Changes of RPE in Each Group
Discussion
The basis for setting the ratio of aerobic and anaerobic exercises was determined by referring to literature and the data measured with the Chinese U23 National Olympic Football Team for scientific research. A total of 34 players participated in the last two games of the Chinese Olympic Team before the Asian Games in Jakarta were selected, the 2-1 victory over Malaysia in Changzhou, Jiangsu province, on August 5, 2018, and the 3-2 victory over Iran in Suzhou, Jiangsu Province, on August 9, 2018. On August 5, the weather in Changzhou was 27°C to 36°C, and the humidity was 67%. On August 9, the weather in Suzhou was 27°C to 35°C, and the humidity was 63%. The weather of the two matches was a hot and humid environment. According to the data calculation, players in a high-level football game sprint every minute and a half. In addition, the study of B. Evangelos et al. also identified that athletes sprint every 90 s on average during the game (Bekris et al., 2016). Therefore, the exercise program used in this study is well-founded and relevant.
This study compared the recovery characteristics of football players during PBC (−110°C ~−140°C for 3 min), CWI (13°C for 15 min), and a passive control treatment after exercise in a hot and humid environment. The main findings of this study are as follows: (a) the physiological effects of PBC are generally similar to CWI; (b) compared with CON, Tc decreased quicker during both CWI and PBC, whereas minor differences in BLa- and PI were observed between the three treatments; and (c) HR in CWI and RPE in PBC decreased quicker than CON group.
HR is widely used as a vital monitoring index in football teams (Akenhead & Nassis, 2016). We observed a significant decrease in HR during cold-water immersion as reported in other studies (Yeung et al., 2016) but no significant decrease in the PBC group. A possible explanation might be that the cold stimulation produced by cold treatment will result in a shorter excitation time of the parasympathetic nerve than that of the sympathetic nerve so that the vagus nerve will be rapidly reactivated, and the activated vagus nerve can quickly regulate HR variability so that the recovery speed of heart rate was accelerated. However, due to the shorter cold treatment time, the HR recovery in the PBC group was not as apparent as that in the CWI group.
Although no significant difference in BLa- and PI was observed, it was noted that the PI rebounded at 15 min after exercise in the PBC group. In contrast to the previous findings (Hohenauer et al., 2019; Vaile et al., 2011), Vaile tested HR, rectal temperature, blood lactate, resting limb blood flow, and re-exercise ability. Furthermore, the arm blood flow was significantly lower than the active recovery after CWI, whereas the leg blood flow was not different (Vaile et al., 2011). Ihsan et al. concluded that post-exercise cooling decreased microvascular perfusion and muscle metabolic activity. These findings are consistent with the suggested mechanisms by which CWI is hypothesized to improve local muscle recovery (Ihsan et al., 2013). We observed an increase in PI after PBC in the present study as reported in other studies (Hohenauer et al., 2019). It has been suggested that cold treatment leads to cutaneous vasoconstriction, decreasing peripheral blood flow. Nevertheless, after the PBC, body temperature rises causing cutaneous vasodilation. Large amounts of blood are pumped out of the heart and into the skeletal muscles and extremities, causing increased blood perfusion.
Numerous studies have reported that oxygen saturation decreases after exercise (Englund et al., 2018; Scott et al., 2017). As expected, a significant increase in SaO2 was observed in the CWI group compared with PBC and CON group. However, we did not observe a significant increase in SaO2 during PBC compared with CON. The reason may be that the breathing deepens and accelerates after the body was stimulated by cold treatment, and even hyperventilation occurred. Therefore, more oxygen is ingested into the blood during breathing, increasing oxygen saturation. However, the PBC group had little change in oxygen saturation due to excessive nitrogen inhalation during cryotherapy.
Tc is replaced by ear temperature, the most popular noninvasive measuring Tc. With this method, which uses infrared waves, it is possible to measure body temperature quickly and noninvasively by placing the probe inside the ear canal. This method is more convenient than other methods and is less influenced by thermal and environmental artifacts (Moran & Mendal, 2002). There are two prominent locations for measuring temperature in the ear: the tympanic membrane and the ear canal. The tympanic membrane gets its blood supply from a section of the aorta that supplies blood to the thermoregulatory center in the brain. It is an important site for measuring body Tc. In addition, access to the ear canal is very convenient (Moran & Mendal, 2002). Exercise in a hot and humid environment increases core and skin temperature, accelerating sports fatigue (Tyler et al., 2016). Cold treatment as an effective method of reducing the core and skin temperatures has been widely proved (Hoshikawa et al., 2019; Lindsay et al., 2017; Polidori et al., 2018a). In agreement with the existing literature, Tc in CWI and PBC were significantly reduced compared with CON. Because PBC can lower the Tc faster, it is more effective and more suitable for competitions and training, but the disadvantage is that it is more expensive (Bouzigon et al., 2016). We did not observe significant reductions in forehead skin temperature in CWI and PBC compared with CON. In contrast with the previous findings (Vaile et al., 2011), the forehead skin temperature of the subjects reached the peak immediately after exercise, reached the lowest at 5 min after exercise, and then began to rise. The difference may be that the body part of the skin temperature measured was the forehead, whereas the body part of the cold treatment in this study does not include the head. Therefore, when the body is stimulated by cold treatment, it will lead to vasoconstriction, and peripheral blood will concentrate to the head, resulting in different test results (Polidori et al., 2018b).
Rating of Perceived Exertion is an important index to evaluate fatigue, created by Swiss psychologist Borg Gunner (Foster et al., 2001). This index is widely used in football training monitoring (Impellizzeri et al., 2004). RPE was significantly lower in the PBC group than in the CON group 20 min after the exercise in this research. RPE will affect the athletes’ psychology, thus affecting the athletes’ competitive ability. Cold treatment can accelerate blood circulation and promote recovery and promote the psychological effect of athletes and then promote the subjective initiative of athletes. Compared with CWI, PBC had a better psychological promotion effect due to lower temperature and more muscular stimulation. Therefore, PBC has a more positive and significant effect on the recovery of RPE.
Although this study reveals essential discoveries, there are also limitations. To ensure the safety of the cold treatment process, we did not use the most accurate measurement method of skin temperature and Tc. Although the exact method has been used to prove that measuring the tympanic membrane is convenient and accurate, there are still some deviations in this method (Cuttell et al., 2017; Moran & Mendal, 2002).
Conclusion
CWI and PBC significantly improved the circulatory system and body temperature recovery within 20 min of exercise in a hot and humid environment, whereas HR in CWI and RPE in PBC elicited a generally more significant decrease than CON. However, PBC may reduce SaO2 due to excessive nitrogen inhalation, which deserves our application.
Supplemental Material
sj-docx-1-jmh-10.1177_15579883221079150 – Supplemental material for The Physiological Profile Following Two Popular Cold Interventions After Activity in Hot and Humid Environment
Supplemental material, sj-docx-1-jmh-10.1177_15579883221079150 for The Physiological Profile Following Two Popular Cold Interventions After Activity in Hot and Humid Environment by Zewen Wang, Yongzhao Fan, Xiaoyang Kong, Patrick Viroux, Ivo J. H. Tiemessen and Hao Wu in American Journal of Men’s Health
Supplemental Material
sj-pdf-1-jmh-10.1177_15579883221079150 – Supplemental material for The Physiological Profile Following Two Popular Cold Interventions After Activity in Hot and Humid Environment
Supplemental material, sj-pdf-1-jmh-10.1177_15579883221079150 for The Physiological Profile Following Two Popular Cold Interventions After Activity in Hot and Humid Environment by Zewen Wang, Yongzhao Fan, Xiaoyang Kong, Patrick Viroux, Ivo J. H. Tiemessen and Hao Wu in American Journal of Men’s Health
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.