
Abstract
The study introduces a path model that links between paternal feelings and child’s anxiety symptoms, aiming to test the mediational role of father–child insecure attachment and the child’s difficulties in emotional regulation in the occurrence of anxiety disorders among a sample of 148 fathers and their children (65 boys and 83 girls aged 8–18) attending the child psychiatric center of a public hospital. Participants completed a battery of diagnostical and research questionnaires, including the Parental Feelings Inventory (PFI), the Difficulties in Emotion Regulation Scale (DERS), the Screen for Child Anxiety–Related Emotional Disorders (SCARED), and the Experiences in Close Relationships Scale–Revised Child version (ECR-RC). Using structural equation modeling, we found father’s anger to be associated with father–child anxiety attachment, while the latter simultaneously mediated the link to the child’s anxiety both directly and indirectly (through emotion regulation [ER]). Consistent with previous evidence, we found insecure attachment and emotional regulation to be uniquely associated with the child’s anxiety. The current findings are among the first to demonstrate the interrelations between these variables in the context of father–child relations, suggesting that the child’s exposure to paternal anger might contribute to developing difficulties in ER and elevated anxiety due to a father–child insecure-anxious attachment relationship. The theoretical and practical implications of the findings are discussed in light of parental gender.
Introduction
Anxiety disorders (ADs) are one of the most prevalent childhood and adolescent mental disorders (Kessler & Wang, 2008; Polanczyk et al., 2015). Approximately 10% of all children meet the diagnostic criteria for an AD during childhood (Copeland et al., 2014; C. E. Kerns et al., 2017). Anxious children and adolescents characteristically present exaggerated levels of fear, worry, physical complaints, and avoidant behaviors (Beesdo et al., 2009) and these symptoms do not tend to remit unless treated (Connolly & Bernstein, 2007; Essau et al., 2014; Swan & Kendall, 2016). In addition to creating internal distress, ADs are associated with impairment in psychosocial functioning and academic performance (Mychailyszyn et al., 2010; Sahithya & Raman, 2021) as well as increased risk for later types of psychopathology, particularly clinical depression (Bittner et al., 2007; Rapee et al., 2009).
The etiology of ADs is assumed to be partly genetic and partly due to environmental influences (Narmandakh et al., 2021; Rapee, 2012; Suveg et al., 2010). Specifically, temperamental factors (e.g., behavioral inhibition) and environmental variables (e.g., family emotional environment) have been strongly related to ADs (Rapee, 2012). Scholars suggest that compared with genetic factors that account for a small percentage of variance in ADs, environmental factors play a critical role (Suveg et al., 2010). Most research on family emotional environment variables in the context of child anxiety refers to parents’ behaviors, such as parental overprotection and low encouragement of autonomy (Cooper-Vince et al., 2014; Hudson et al., 2009; McLeod et al., 2011), criticism, and lack of warmth (Hudson et al., 2008). Other aspects of a child’s environment that have also been examined are the role of stressful life events, sibling and peer relationships, social media, and school environment (Creswell et al., 2020; Lawrence et al., 2019). Relatively less work has been conducted on other aspects of parent–child interactions, such as parental feelings and ER, for their role in explaining the association between parent and child anxiety, but findings are beginning to emerge (e.g., Borelli et al., 2015; Breinholst et al., 2019). Specific family emotional environment components that have been examined in the context of children with ADs refer to parental cognitive biases toward threat and threatening interpretations, which were found to be associated with the child’s over-interpreting threat with consequent and exaggerated levels of fear (e.g., Lester et al., 2010; citation removed for anonymity), encouraging the suppression of the child’s emotional expression, both directly by little discussion regarding emotions and indirectly by the existence of a negative emotional atmosphere in the home, teaching the child that emotional interaction is unpleasant (Suveg et al., 2010). Given that parents present a variety of environmental emotional stimuli, understanding the way these emotional experiences, those related to parental roles, affect children is an important area of inquiry. Most of the existing studies do not explicitly examine negative parental feelings and their effects on the child’s healthy development or maladjustment but rather focus on the parents’ experiences of emotion in real-time, with a particular focus on the intensity of the emotion (e.g., Nelson et al., 2013; Nelson-Coffey et al., 2019; Taquet et al., 2016). Another limitation of the existing research is the relative neglect of the paternal role (e.g., Bariola et al., 2012). Those limited studies that have examined the paternal role separately from the maternal role have reported that fathers have a unique contribution to child attachment and emotional development (e.g., Cassano et al., 2007). Children with ADs tend to have difficulty in expressing and managing anger and sadness and perceive themselves as less able to successfully manage emotionally provocative situations (e.g., Suveg & Zeman, 2004). Furthermore, parents of children with ADs tend to encourage the suppression of emotional expression and express less positive and more negative emotions themselves (Hudson et al., 2008; Suveg et al., 2008). Previous studies emphasized the specific nature of the feelings experienced by parents related to their role (e.g., Bradley et al., 2013), suggesting that parental feelings may play a key role in parent–child interaction and child development (Fijałkowska & Bielawska-Batorowicz, 2021).
Attachment Theory: Theoretical Links with Anxiety
Attachment theory provides one of the most comprehensive frameworks for understanding the development of anxiety (Bowlby, 1969, 1973). Bowlby (1973) underlined that children’s concerns about attachment figures’ availability and accessibility constitute the basis of anxiety and postulated a link between attachment insecurity and child anxiety. Based on their experiential history with caregivers, children learn to predict the attachment figures’ availability. If the children’s attempts to predict the caregivers’ availability fail, they respond with fear and anxiety (Brumariu & Kerns, 2008). The empirical evidence for the theoretical link between insecure attachment and anxiety has been reflected in several recent review works (e.g., Brumariu & Kerns, 2010; Colonnesi et al., 2011; Groh et al., 2012; Madigan et al., 2013), all of them pointing to the association between insecure attachment and higher anxiety levels in children and adolescents. The attempt to trace which specific form of insecure attachment places children at greater risk for experiencing anxiety problems yielded mixed findings, with some studies suggesting that ambivalently attached children may be more vulnerable to developing ADs (e.g., Brumariu & Kerns, 2008; Colonnesi et al., 2011; Dallaire & Weinraub, 2005), while other studies did not predict this (Bar-Haim et al., 2007; Marsh et al., 2003). Avoidant attachment has not shown a consistent relation with anxiety (Brumariu & Kerns, 2008).
These works show that inconsistencies across studies in the form of insecure attachment that is principally related to AD may be due to the use of different methodologies, different references to the nature of AD (whether anxiety symptoms, ADs, or internalizing disorders), and different age groups.
However, other scholars have proposed that specific forms of insecure attachment, especially the ambivalent form, may be linked to anxiety. For example, Carlson and Sroufe (1995) suggested that while both avoidantly and ambivalently attached children may be vulnerable to developing depression, only the latter are at greater risk of anxiety due to consistent concerns about the availability of attachment figures. Furthermore, theoretically, insecure-ambivalent children are hypothesized to develop anxiety due to the chronic worry about the availability of the caregiver (Carlson & Sroufe, 1995). More recently, Colonnesi et al. (2011) examined the role of ambivalent attachment and concluded that this pattern was associated with anxiety symptoms. Another limitation in the literature concerns the minority of studies that focused on clinical populations. Given the need to broaden the understanding regarding the etiology of the ADs among children and adolescents, additional empirical studies that will focus specifically on clinical populations are required (Breinholst et al., 2019). More gap in the existing research literature concerns the relative neglect of the paternal role as attachment figures, as most studies focused on attachment to mothers only (Groh et al., 2012; Madigan et al., 2013), while limited number of empirical studies included fathers (Breinholst et al., 2019). Specifically, the limited number of studies on father–child attachment, and their potential associated problems in children ADs, has resulted in these studies being excluded from two out of four reviews on the topic (Groh et al., 2012; Madigan et al., 2013). Further proof of the importance of research among fathers emerges from a study by Breinholst and colleagues (2019) among a clinically anxious sample. Their study investigated the direct and indirect relationship between parent–child attachment and negative parental behaviors separately for mothers and fathers, indicating that insecure attachment to the father accounted for a significant proportion of variance in anxiety. This study aims to ameliorate these limitations by focusing on two populations that have received little attention in the literature: fathers as attachment figures and children and adolescents among the clinical population.
Theoretical Links Between ER, Parent–Child Attachment, and Child’s Anxiety
Another construct that has received increasing attention in the context of parent–child attachment and ADs is ER. ER is defined by Gross (1998), as “processes by which individuals influence which emotions they have, when they have them, and how they experience and express these emotions” (p. 275). ER functions to decrease (downregulate) or increase (upregulate) facets of emotional responding, such as the intensity, duration, and frequency of a given emotion (Sheppes et al., 2015). ER processes are initially developed in the family context (Eisenberg et al., 1998; Gottman et al., 1996; Morris et al., 2007), shaped in the parent–child attachment relationship, as children use the attachment figures as a resource to regulate their own emotions (e.g., K. A. Kerns & Brumariu, 2014) and are also associated with ADs (e.g., Thompson, 2001).
Parent–child interactions provide the context in which children learn about emotions and ER features through observing, learning, and modeling (Morris et al., 2007), by observing their attachment figures’ expression of their own emotions and regulation abilities (Denham et al., 2010) and by communicating about their own emotions and ways they are helped to regulate their emotional responses (Brumariu, 2015). Insecurely attached children, compared to securely attached children and adolescents, are less flexible in regulating their negative emotions, as they have reduced opportunities to learn appropriate ER abilities in their relationships with their attachment figures (Esbjørn et al., 2012; Thompson & Meyer, 2007). For example, ambivalently attached children exaggerate their display of negative emotions in an attempt to gain the attention of their inconsistently available attachment figure (Cassidy & Berlin, 1994), whereas children with an anxious attachment style develop a sense of vulnerability and doubts about their ability to handle distress without the help of their attachment figures (Mikulincer et al., 2003).
ER processes are also related to anxiety, as anxiety, by definition, reflects difficulties in managing emotional arousal and the intense experience of negative emotions (Thompson, 2001). Scholars have demonstrated that aspects of dysfunctional patterns of ER play an important role in clinical conditions, such as ADs (e.g., Brumariu et al., 2012; Gross, 2013; Hofmann et al., 2012). For example, the study of Brumariu et al. (2012), which examined whether the relation of mother–child attachment with anxiety symptoms is mediated by ER processes, in 10- to 12-year-olds, reported that children with high levels of anxiety had difficulty in managing their emotions and the relations of insecure attachment with anxiety symptoms were partially mediated by emotional awareness. Other studies indicated that ADs in children and adolescents are associated with a lack of emotional clarity, limited access to effective ER strategies, as well as nonacceptance of negative emotional responses (Bender et al., 2012; Neumann et al., 2010). Bender and colleagues (2015) addressed the interrelations among attachment security, emotion dysregulation, and anxiety on a sample of 673 children and adolescents (ages 9–16), showing a direct negative association between attachment security and anxiety. However, when emotion dysregulation was introduced as a mediating factor, this direct association was replaced by an indirect association (between attachment security and anxiety). The results indicate that more securely attached children and adolescents reported less emotion dysregulation and that children and adolescents who had fewer ER difficulties experienced less anxiety. The model was confirmed by the authors for both children and adolescents.
Similarly, Masten and Cicchetti (2010) suggested that insecure attachment may lead to ADs in part because insecurely attached children have difficulties in regulating emotions, and this, in turn, further increases children’s risk of developing ADs. Insecure attachment may be associated with ADs, in part, because insecurely attached children are less likely to develop competent ER abilities, which, in turn, places them at risk of experiences that contribute to the development of ADs.
This study aims to explore the relations between paternal feelings, parent–child attachment, ER, and anxiety symptoms among children and adolescents, while focusing on fathers as attachment figures and on their parental feelings through father–child dyadic analysis. The study introduces a path model that links between paternal feelings and child ADs through insecure attachment and ER, aiming to test the mediational role of insecure attachment with the father and emotion dysregulation in the occurrence of ADs among a sample of referral children and adolescents. The model is based on the understanding that both insecure attachment and ER are associated with ADs, while insecurely attached children are also more likely to have difficulties in regulating emotions, which may further contribute to anxiety. The study aims to inspect the contribution of parental feelings in these variables’ context, as we theorized that paternal feelings may be associated with father–child attachment style, which, in turn, may associate with child’s ADs both directly and via ER.
In line with the literature reviewed above, we hypothesized that insecure father–child attachment would be related to both emotion dysregulation and anxiety. We further hypothesized that part of the association between insecure attachment and anxiety would be mediated by the child’s difficulties in emotion dysregulation. We expected that insecure attachment would be associated with anxiety both directly and indirectly (i.e., via emotion dysregulation), and that paternal feelings (i.e., happy, anger, and anxious/sad) would be associated with father–child insecure attachment. Consequently, it is hypothesized that paternal feelings will be associated with the child’s anxiety and ER via insecure attachment as a mediator.
Method
Participants and Procedure
The sample included 148 fathers and their children attending the child and adolescent psychiatric center of a public hospital that serves a multiethnic population in its region. The center provides assessment and treatment in individual outpatient clinics for a variety of mental health problems. Families attending the psychiatric center are briefly assessed by a clinician and referred to a specific clinic according to the assessment for a deeper assessment and treatment plan. The families (about 80% Israeli-Jewish and the rest Israeli-Arab; these groups do not differ in the study variables and hence are treated as a whole as part of the study’s statistical analyses) who participated in this study had been referred to the psychiatric center for the following clinical conditions: anxiety and post-trauma, attention deficit hyperactivity disorder (ADHD), eating disorders, depression, and sexual abuse. The children’s and adolescents’ (65 boys and 83 girls) age ranged from 8 to 18 (M = 13.93, SD = 2.76), and the father’s age ranged 33 to 68, (M = 47.80, SD = 6.39). Fathers and their children completed the study questionnaires before their first evaluation meeting (intake). The questionnaires are part of a broader set of questionnaires that parents and children attending the center complete and are used by the center’s professionals in the evaluation process and were not given only for research purposes. Participants gave their informed consent to take part in the study by signing an informed consent form. The Helsinki Committee of Ziv Medical Center, Tzfat, Israel approved the study (approval number: 0083-19-Ziv).
Measures
The study uses separate informants to assess the father’s and the child’s variables: father’s reports were used to assess paternal feelings, while children’s and adolescents’ reports were used to assess the child’s emotional difficulties (i.e., attachment insecure pattern, emotion dysregulation, and anxiety). The specific instruments used in the study are as follows:
Parental Feelings Inventory (PFI; Bradley et al., 2013)
This 26-item questionnaire is designed for assessing parental emotions within the parenting role through parent’s self-report. The PFI presents emotion adjectives to which the parents are asked to indicate the degree they experience that emotion in their role as parents (i.e., “during the last month did you feel the following in your role as a parent/guardian?”). The questionnaire was tested among parents of 3-year-old children with behavior problems, originally yielding three scales of parental emotion: Angry (e.g., Annoyed), Happy (e.g., Cheerful), and Anxious/Sad (e.g., Afraid). The developers reported a good internal consistency reliability for each of the PFI scales with reference to both maternal and paternal measurement (with all Cronbach’s Alpha indices exceeding the .90 point) and demonstrated evidence for the scales’ predictive and concurrent validity. The PFI’s validity and reliability were tested with parents of adolescents by Yaffe and colleagues (in press), after translating the scales’ items from the English PFI into Hebrew using three steps of back-forward translation procedure. In this study, we recorded a good internal consistency reliability for all three PFI scales, with their Alpha coefficients ranging from .80 to .90.
The Difficulties in ER Scale (DERS; Gratz & Roemer, 2004)
The DERS consists of 36 items that load onto six subscales (nonacceptance, goals, impulsivity, awareness, strategies, and clarity). The instrument has been widely used in diverse populations for different research purposes (e.g., Kaufman et al., 2016; Neumann et al., 2010). Respondents (child’s self-report) are asked to indicate how often the items apply to themselves, with the response scale to an item ranging from 1 to 5, where 1 = almost never, 2 = sometimes, 3 = about half the time, 4 = most of the time, and 5 = almost always. The DERS has high internal consistency (α = .93), good test–retest reliability (r = .88, p < .01), and adequate construct and predictive validity (Gratz & Roemer, 2004). The instrument’s validity was tested with adolescents aged 11 to 17, revealing a similar factorial structure to the one originally found with adults (Neumann et al., 2010). The Hebrew form administered in this study has been successfully and widely used in previous studies in Israel (e.g., Azoulay et al., 2020). Consistent with previous studies’ data using the Hebrew translated scale, in this study, we also recorded an indication of a good internal consistency reliability for the total ER scale (α = .82).
The Screen for Child Anxiety–Related Emotional Disorders (SCARED; Birmaher et al., 1999) is designed to identify primary ADs in children and adolescents 8 years old and older via the child’s self-report. The questionnaire contains 41 items divided into five scales corresponding to the Diagnostic and Statistical Manual of Mental Disorders (4th ed.; DSM-IV; American Psychiatric Association, 1994)’s classification of children’s ADs: Panic–Somatic (13 items, e.g., “When I am afraid, I feel like I’m going to pass out”); Generalized AD (9 items, e.g., “I worry that things do not work out for me as I want”); Separation Anxiety (8 items, e.g., “I have bad dreams that something bad happens to my parents”); Social Anxiety (7 items, e.g., “I feel nervous when I’m with people I do not know well”); and School Anxiety (4 items, e.g., “I am worried or afraid when I have to go to school”). The response scale for an item ranges from 0 (not true) to 2 (very true) and the total score for each anxiety type is calculated by adding up the responses for all the scale’s items. The questionnaire is valid for screening anxiety and to pre-identify types of specific ADs for research purposes in children and adolescents, with its versions widely used in Israel and around the globe (e.g., Bar-Haim et al., 2007; Muris et al., 1999). In this study, we obtained an indication for an adequate internal consistency reliability for the questionnaire’s overall scale (α = .75).
The Experiences in Close Relationships Scale–Revised Child Version (ECR-RC; Brenning et al., 2014)
The short-form of the questionnaire is adapted for children and adolescents self-reporting and includes 12 items. Its statements are ranked on a 7-points scale, with 1 representing “strongly disagree” and 7 representing “strongly agree.” Of the instrument’s items, six measure anxious (or ambivalent) attachment and six measure avoidance attachment, yielding two separate scores for the respondent’s insecure attachment level. A higher score indicates a higher insecure attachment pattern of this type, while a lower score represents a more secure attachment pattern. For the study’s purposes, we used only the version that refers to the child’s attachment to the father. The questionnaire has previously exhibited good indexes of reliability and validity measures in several works (e.g., Brenning et al., 2014), which are consistent with the excellent reliability indices obtained in this study for the two insecure attachment scales in the Hebrew version (.86–.93).
Results
The chapter opens by presenting descriptive statistics of the study’s scales by the child’s sex (Table 1), followed by a statistical indication of sex differences for each variable. We display the zero-order correlations and the descriptive statistics for the study’s general scales and the participants’ age for the whole sample (Table 2), which initially and partially confirms our hypothesis regarding the associations between paternal feelings and the child’s emotional variables. Finally, as part of testing our research hypothesis, we introduce a path analysis model linking between paternal feelings and child’s anxiety, through insecure attachment and difficulties in emotional regulations as mediators.
Sex Differences in the Research Variables.

Note. PFI = Parental Feelings Inventory (Bradley et al., 2013); SCARED = Screen for Child Anxiety–Related Emotional Disorders (Birmaher et al., 1999); ECR-RC = Experiences in Close Relationships Scale-Revised Child version (Brenning et al., 2014); DERS = Difficulties in Emotion Regulation Scale (Gratz & Roemer, 2004); ER = emotion regulation.
p ≤ .05.** p ≤ .005.
Means, Standard Deviations, and Zero-Order Correlations Between Study Variables.
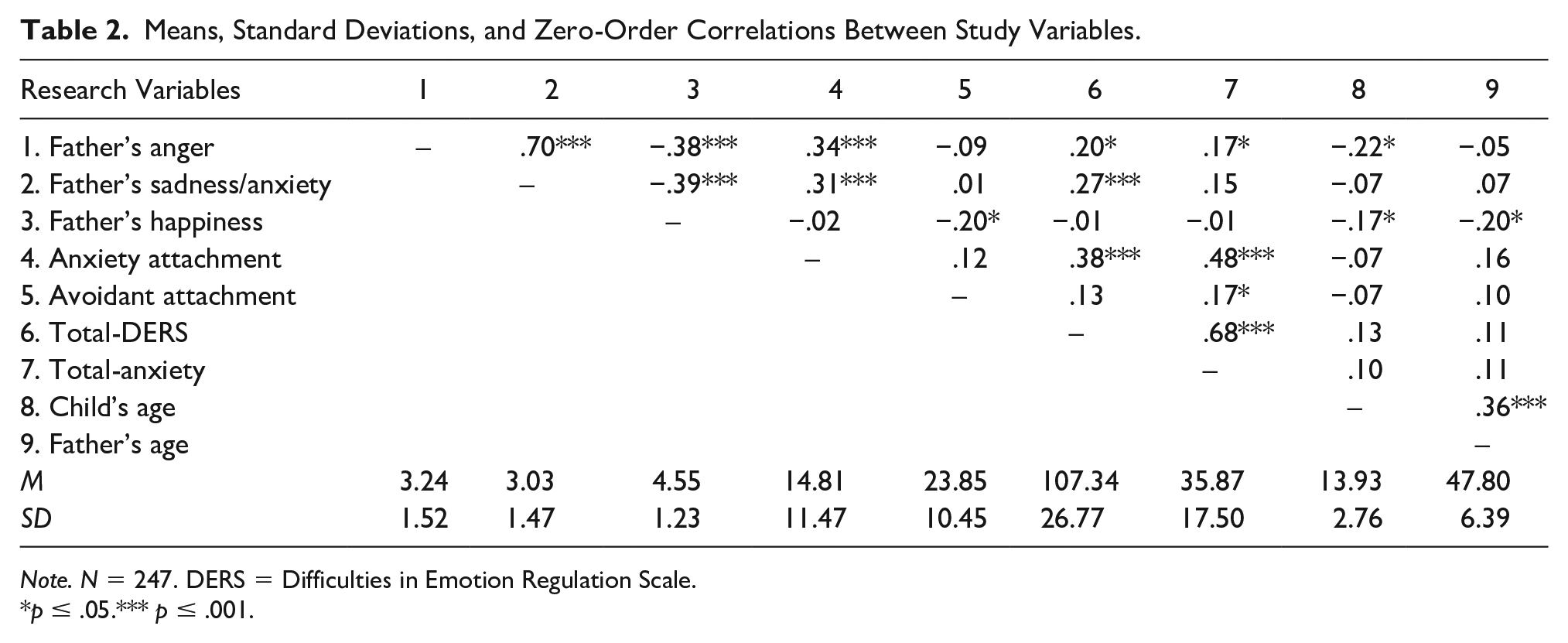
Note. N = 247. DERS = Difficulties in Emotion Regulation Scale.
p ≤ .05.*** p ≤ .001.
Preliminary Analyses
In general, girls scored significantly higher than boys in the total anxiety level and partially in insecure attachment (i.e., boys and girls differed only on avoidant attachment scale). Sex differences with respect to the DERS total score (i.e., difficulties in ER) are insignificant (p = .06(, meaning that girls’ and boys’ scores on this scale are comparable.
The correlations that initially support our hypotheses are between father’s anger and child’s anxiety attachment (r = .34, p < .001), father’s sadness/anxiety and child’s anxiety attachment (r = .31, p < .001), and between the latter variable and the anxiety total score (r = .48, p < .001) and the DERS total score (r = .38, p < .001). The child’s anxiety is strongly associated with DERS (r = .68, p < .001), which, taken together with the other results, initially establishes the mediation model between paternal feelings and child’s anxiety with attachment and DERS as mediators. As expected, avoidant attachment is insignificantly related to both anxiety and DERS in the current sample. Finally, both the father’s and the child’s age were not correlated with most of the study variables, especially with the endogenous ones (i.e., mediating or dependent variables in the model, such as DERS, anxiety, and anxiety attachment). These patterns apply similarly for boys and girls, and therefore the participants’ age was not taken into account in the following mediational model, testing the research hypothesis.
Path-Analysis—The Associations Between Paternal Feelings and the Child’s Emotional Variables
The regression model predicting the child’s anxiety from the paternal feelings with attachment to father and difficulties in DERS as mediators is embodied in the path analysis in Figure 1. As indicated in the Method section, separate reports were used for parent and child variables, with each informant self-reporting his own emotions (see Table 1). The model explains about 53% of the participants’ anxiety variance, with their attachment to father and DERS significantly and directly affecting the former variable. Attachment is also indirectly associated with the child’s anxiety via DERS, with the latter significantly mediating that link (as indicated by the lower CI bootstrap value, which is exceeding zero in Table 3). Since only the father’s anger reached significance as part of the correlations between paternal feelings and attachment with father (i.e., the first mediator), the data of the indirect links from the father’s happiness and sadness/anxiety were excluded from the table. Next, we calculated the indirect effects of the father’s anger on the child’s DERS and the father’s anger on the child’s anxiety (i.e., via attachment), and both of their CI positive ranges indicate a significant indirect path. That is to say that children and adolescents with angrier fathers are more anxious and have more difficulties in ER due to their insecure-anxious attachment with their fathers.

Path Analysis Describing the Direct and Indirect Links Between Paternal Feelings and Child’s Emotional Variables (Indices Represent Standardized Estimates).
Path Estimates, SEs, and Bootstrapped 95% CIs for the Regression Model Predicting the Child’s Anxiety From Paternal Feelings With Anxiety Attachment to Father and Difficulties in Emotion Regulation as a Mediators.

Note. CI = confidence interval; DERS = difficulties in emotion regulation.
Based on the hypothesized model presented in Fig. 1, we examined the overall model fit, revealing a good fit of the model to data (χ2 = .575, p > .05, χ2/df = .100; normed fit index [NFI] = .998; comparative fit index [CFI] = 1.000, root mean square of error approximation [RMSEA] = .000). The model does not account for the child’s age, as its correlations with the model’s variables were negligible (see Table 2). The model was tested for sex moderation, to find out whether it differs for boys and girls (i.e., whether the current pattern of associations between the variables would be influenced by child’s sex). We tested for significance differences in model fit between the unconstrained model and the fully constrained model, given that insignificant difference in the chi-square value between the two models across groups rules out sex moderation (Dabholkar & Bagozzi, 2002). Using Chin’s (2000) formula for chi-square difference test (also see: Lowry & Gaskin, 2014), we found no significant change in chi-square values between the models, indicating the general model’s equality across sexes. Each individual path was constrained in a sequence to trace possible sex differences in the model’s path between boys and girls. This resulted in a single sex difference in the path leading from DERS to anxiety (see Figure 1), where the correlation between the variables is significantly stronger for boys, despite its positive direction and significance in both sex groups.
Discussion
The study introduces a mediational path model that predicts ADs in children and adolescents from paternal feelings, insecure attachment to the father, and emotion dysregulation. While previous research has abundantly studied the association between child/adolescent insecure attachment and elevated anxiety for mother–child relations (e.g., Breinholst et al., 2019; Groh et al., 2012; Madigan et al., 2013), the current investigation of this issue focuses on father–child relations in an adolescent clinical sample. The study utilizes separate sources of information to assess the father’s and child’s variables, in an attempt to minimize inflated correlation potentially caused by single informant reports (Campbell & Fiske, 1959). Consistent with our main hypothesis, we found that anxious/ambivalent father–child attachment is associated with children’s and adolescents’ anxiety both directly and indirectly through emotion dysregulation. First, this finding generally corroborates the core premise that insecurely attached children and adolescents are more likely to have anxiety problems, which was demonstrated in a long list of studies (e.g., Brumariu & Kerns, 2010; Colonnesi et al., 2011; Groh et al., 2012; Madigan et al., 2013). Second, in line with previous work mainly conducted with nonclinical populations (Bender et al., 2015; Brumariu et al., 2012), these findings suggest that children and adolescents with insecure attachment to their parents tend to be more anxious, partially due to their impaired ER abilities. Altogether, the results presented here as the findings of Brumariu and colleagues (2012) and Bender and colleagues (2015) provide empirical evidence for the theoretical view that the quality of attachment in children may be related to child and adolescent anxiety because of the effect attachment has on children’s developing ability to regulate their emotions (Esbjørn et al., 2012). That is to say, ER processes are one mechanism that may explain why insecure attachment is related to ADs. This corresponds with the notion presented by Thompson and Meyer (2007), that insecurely attached children might be less flexible in regulating their negative emotions, as they have reduced opportunities to learn appropriate ER abilities in their relationships with their attachment figures (Esbjørn et al., 2012; Thompson & Meyer, 2007). Insecurely attached children are thus less likely to develop competent ER abilities, which puts them at greater risk of experiences that contribute to the development of anxiety (Masten & Cicchetti, 2010). This assumption is supported by the results presented by Bosquet and Egeland (2006), who assessed attachment pattern at an earlier time point than ER abilities, indicating that insecure attachment precedes ER difficulties in later life. In line with the notion that childhood anxiety may be best conceptualized as being primarily a dysregulation of negative emotional responses (Weems, 2008), the results demonstrate that children and adolescents who scored high on ER difficulties also indicated higher levels of anxiety. These findings lend support to the notion that emotion dysregulation is a key factor to consider in treatment and research of anxiety in children and adolescents.
The current findings underpin the importance of the father’s potential role in the etiology of descendants’ ADs (i.e., children, adolescents, and emerging adults), which was reported in some previous studies to differ from the mother’s etiologic role in several aspects of parent–child relations (e.g., Breinholst et al., 2019; Mattanah, 2001; Yaffe, 2018, 2020). Specifically with respect to the relationship between children’s and adolescents’ attachment style and anxiety, the current findings are consistent with those presented by Breinholst and colleagues (2019), suggesting that father–child insecure attachment may play an important, unique role in the occurrence of childhood anxiety. The model introduced in this study focused on the anxious (or ambivalent) attachment style to predict the participants’ anxiety, following previous research evidence indicating that the ambivalent/anxious attachment style holds the strongest association with ADs (Colonnesi et al., 2011). The current data, showing moderate unique-direct and indirect links between anxious attachment and increased anxiety, are consistent with this evidence, generally confirming our hypothesis regarding the relationships between the child’s insecure attachment with the father and anxiety symptoms in children and adolescents.
One of the study’s main goals was to investigate the role of paternal feelings in the context of child’s internalizing variables, as relatively less empirical attention has been devoted to the importance of such parenting aspects other than parenting rearing practices and styles. Parental emotional experiences within the parenting role are likely to be important for children (Bradley et al., 2013), while negative parental feelings in particular might adversely affect the parent–child connection and impair the child’s emotional well-being. The study’s findings partially supported this thesis embodied in our hypothesis, showing a significant unique association for paternal anger and father–child insecure attachment, which, in turn, mediated the association between paternal anger and both the child’s emotional dysregulation and his or her anxiety. In other words, paternal feelings were related to the adolescent’s emotional variables in the current sample only through insecure attachment. While the exposure of a child to parental anger might contribute to developing an angry response pattern to outside stimuli and to fostering difficulties in ER (Plickert & Pals, 2020), our findings suggest that this process mainly occurs in the context of an insecure-anxious parent–child attachment relationship. This is consistent with the notion that ER is initially developed in the family context and is shaped by the parent–child attachment relationship (Eisenberg et al., 1998; K. A. Kerns & Brumariu, 2014; Morris et al., 2007). Furthermore, children and adolescents exposed to persistent parental anger (albeit not necessarily aggression per se) are more likely to experience an increased negative expression from the parent, low parental emotional responsiveness, and parental rejection, which might adversely impact the evolving attachment quality with their parent (Muris et al., 2004). In addition, previous studies suggest that negative emotions cause more arousal and may be more challenging to regulate than positive emotions (e.g., Cacioppo et al., 2000). As a result of this higher level of emotional arousal, a preponderance of negative emotion is likely to make regulation more difficult (Suveg et al., 2010). Thus, the findings of the study highlight the importance of negative paternal feelings in the context of clinical populations and their contribution to the acquisition of nonadaptive regulation patterns, while emphasizing the importance of building intervention programs designed to help parents of children and adolescents with ADs acquire adaptive tools for dealing with negative emotions. Studies in the field of parent–child relations primarily focus on parental practices and behaviors, with only a few dealing with the role of parental feelings in the context of the child’s emotional difficulties, and even fewer considering father–child attachment at all. This study is among the first to offer specific empirical support for that theoretical view, by demonstrating a unique association between paternal anger and the anxious father–child attachment style.
Our model seemed to apply similarly for boys and girls, yet in the current sample, the latter exhibited significantly more anxiety symptoms than the former. These gender differences in anxiety level are consistent with the premise that ADs are more common in girls than in boys, confirming gender as a risk factor for these disorders. Gender is sometimes considered the strongest predictor of anxiety (Narmandakh et al., 2021). Some argue that gender differences in the prevalence of anxiety among girls compared to boys have a biological basis related to differential sex hormone effects, which start earlier in girls and involve significantly higher levels compared to boys (e.g., Peper & Dahl, 2013). Another explanation may stem from socio-cultural reasons associated with differences in gender role expectations regarding the expression of feelings. That is, social norms that see women as more vulnerable and sensitive allow girls to express more feelings of stress, share them with others, and ask for help (Rickwood et al., 2007; Van Droogenbroeck et al., 2018).
Ultimately, few works have studied the relationship between parental anger pe se (as mentioned, this is not identical to aggressive or hostile parenting) and children’s and adolescents’ emotional well-being (see Plickert & Pals, 2020), non-of-them specifically tested children’s and adolescents’ anxiety as an outcome variable. Apart from the fact that our findings provide the first evidence to suggest that parental anger could play a familial role in relation to the child’s anxiety, the current findings are distinct in two ways. First and foremost, here we referred to anger as a parental emotion within the parental context (Bradley et al., 2013), which does not correspond to the generic construct used by Plickert and Pals (2020) in defining parental anger. Since the operational framework used here to define paternal feelings is relatively new, more empirical development and clarification about the scale’s construct is needed to understand its convergence with and divergence from other relative constructs. In addition, we found that this parental emotion is associated with children’s and adolescents’ anxiety only through insecure attachment, meaning that the sample’s children and adolescents who were exposed to paternal anger were more anxious because they had an insecure-anxious attachment with their fathers. In this regard, more empirical interrogation is required to deepen our understanding regarding the role-played by these parental emotions, and anger in particular, in the context of the child’s anxiety. Given that paternal anger was related to both child’s outcome variables tested here (i.e., ER and anxiety) only via a mediator, this implies that paternal feelings are primarily related to paternal behavior and practice patterns rather than directly to the child’s outcomes. This conclusion should be further validated against several other parent’s and child’s variables. Based on the current findings, it is difficult to determine the directionality of the association between paternal feelings and the child’s anxiety. It is also possible that there is a transactional relationship in which both paternal feelings and the child’s anxiety impact one another over time. Longitudinal studies are necessary to broaden the understanding of the relationships between them and to track the trajectory of these factors over time.
Study Limitations, Implications, and Directions for Future Research
There is a need for research investigating whether ER processes are differentially related to other specific insecure attachment patterns, such as disorganized attachment. Considering the importance of the family context to processes of developing emotional abilities, future studies may consider examining other family factors, such as the parents’ marital status and socioeconomic indicators, when studying the associations of attachment and parent’s feeling. In this cross-sectional study design, we assessed the study variables (i.e., parental feeling, attachment, ER difficulties, and anxiety) at a single time point. It is, however, conceivable that an attachment pattern develops prior to the onset of anxious symptomatology, and that difficulties in ER precede the development of anxiety.
Another limitation relates to the fact that the data are based on self-report measures and are subject to both response bias and common method bias. In future studies, a mixed methodology, including measures from different sources (e.g., clinician assessment) and qualitative investigation (e.g., open-ended questions), may help to reduce the potential for such bias (Podsakoff et al., 2003).
Studies involving fathers do not distinguish between children with clinical anxiety, children with anxiety symptoms, and children displaying internalizing disorders (Bögels & Phares, 2008; Van der Bruggen et al., 2008). Future studies may compare the unique roles of attachment to mothers and fathers in relation to different levels of children’s anxiety. Our results have implications for treatment processes targeted to anxious children and adolescents, as they support the importance of working with fathers on their feelings in the parental role, providing their children a model of adaptive ER abilities that can lead to secure attachment relationship between the father and the child. The implications for doing this are that fathers might play different roles regarding children’s and adolescents’ anxiety, and based on this knowledge, paternal variables might need to be included in the assessment of childhood anxiety and case formulation, and fathers might also need to be included in the treatment of anxiety.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.