
Abstract
Although there has been no direct empirical evidence linking sexual dysfunction (SD) with gun ownership, speculation has been widespread and persistent for decades. In this paper, we formally examine the association between SD and gun ownership. Our primary hypothesis, derived from the psychosexual theory of gun ownership, asserts that men experiencing SD are more likely to personally own guns than other men. To test this hypothesis, we used recently collected data from the 2021 Crime, Health, and Politics Survey (CHAPS), a national probability sample of 780 men, and binary logistic regression to model gun ownership as a function of SD. Our key finding is that men experiencing SD are no more likely to own guns than men without SD. This interpretation was supported across several indicators of SD (performance anxiety, erection trouble, and ED medication) and gun ownership (personal gun ownership, purchasing a gun during the pandemic, and keeping a gun in one’s bedroom). To our knowledge, we are the first to have directly tested the association between SD and gun ownership in America. Our findings are important because they contribute to our understanding of factors associated with gun ownership by challenging the belief that phallic symbolism and masculinity somehow drive men with SD to purchase guns. Our results also remind us of the perils of gun culture rhetoric, which, in this case, function to discredit gun owners and to further stigmatize men with ED. We conclude by calling for more evidence-based discussions of SD and guns in society.
Are men who experience sexual dysfunction (SD) more likely to own guns than other men? Although there is no direct empirical evidence linking SD with gun ownership, speculation has been widespread and persistent for decades. In 1968, Arthur Schlesinger, Jr. (1968:46), the noted historian who served under the Kennedy administration, claimed that “the hysteria expressed by some at the thought that guns should be licensed, like automobiles, dogs and marriages, only strengthens the psychiatric suspicion that men doubtful of their own virility cling to the gun (like Clyde in Bonnie and Clyde) as a symbolic phallus and unconsciously fear gun control as the equivalent of castration.” In 1999, Camille Paglia, a prominent feminist scholar, told us that “American society’s problem isn’t firearms – it’s the sexually dysfunctional men and women who abuse them” (Paglia, 1999). In 2010, the headline of a satirical science report read: “New Study Links Guns, Sexual Dysfunction” (Frazier, 2010). In 2013, a professor of humanities blogged about the “connection between American men’s experience of their own diminished virility and the proliferation of firearms in American society” and the “Freudian lens” that best “captures the dual phenomenon of sexual impotence and the quest for potency through more, and more powerful, guns” (Settles, 2013). In 2016, an editorial in HuffPost argued that “the compulsion to own firearms stems from an unconscious need to compensate for a deep-seated psychological sense of insecurity and inadequacy in terms of power: in males, specifically for having a small or smaller-than-desired penis” (Blumenfeld, 2016). In 2020, John Cleese, a famous comedian, quipped on Twitter that “the British are proud that they DON’T [emphasis in original] need a gun to make themselves feel manly” and that Americans need “assault weapons” to “keep ED [erectile dysfunction] away” (Smith, 2020). In this paper, we formally test, for the first time, whether men experiencing SD are in fact more likely to personally own guns.
The psychosexual theory of gun ownership has three primary propositions. The first proposition is that guns are phallic symbols. In his Introductory Lectures on Psycho-Analysis, Freud (1922, pp. 179–180) argued that “the penis is symbolized primarily by objects which resemble it in form, being long and upstanding, such as sticks, umbrellas, poles, trees, and the like; also by objects which, like the thing symbolized, have the property of penetrating, and consequently of injuring, the body,—that is to say, pointed weapons of all sorts: knives, daggers, lances, sabres; fire-arms are similarly used: guns, pistols and revolvers, these last being a very appropriate symbol on account of their shape.” The noted symbolic link between guns and male genitalia has persisted for nearly a century in psychology, psychiatry, sociology, gender studies, feminist studies, communication studies, and media studies (Blum, 2019; Cooke & Puddifoot, 2000; Diener & Kerber, 1979; Hall, 1953; Hill, Dowd-Arrow, Davis, et al., 2020; Kelley, 1995; Moffic, 2013; Nathenson, 2020; Neville-Shepard & Kelly, 2020; Potts, 2000; Sasson-Levy, 2003).
The second proposition is that guns are symbols of masculinity. In U.S. culture, guns are associated with masculinity because they are primarily used by men (Azrael et al., 2017; Dowd-Arrow et al., 2019; Goss, 2017; Hepburn et al., 2007; Parker et al., 2017; Smith & Smith, 1995; Smith et al., 2019) and because they can be used to project power, strength, and a capacity to engage in violent and lethal forms of aggression (Cassino & Besen-Cassino, 2020; Cukier & Sheptycki, 2012; Cukier & Eagen, 2018; Diener & Kerber, 1979; Kahan & Braman, 2003; Nathenson, 2020; Neville-Shepard & Kelly, 2020; Pfaffendorf et al., 2021; Potts, 2000; Stroud, 2012; Tonso, 1982). Stroud (2012, p.221) explains that “because guns are so lethal, they imbue their users with traits associated with masculinity—control and power.”
The final proposition is that some men acquire guns as a means of compensation when they perceive losses in virility and masculinity. SD (e.g., the inability to achieve or maintain an erection during sexual activity) can be emotionally distressing because it is emasculating or in direct contradiction with popular conceptions of masculinity (Brubaker & Johnson, 2008; Burnett et al., 2020; Burns & Mahalik, 2007; Chambers et al., 2017; Nicolini et al., 2019; Occhipinti et al., 2019; Potts, 2000; Wentzell et al., 2017). According to Potts (2000, p.90), “the absence of—or difficulty in ‘achieving’ and ‘maintaining’— a robust ‘hard on’ in appropriate circumstances presents as a disastrous affliction in the male—an abnormality, a failure to stand up and be counted as a ‘real’ man.” In this context, many men experiencing erectile dysfunction (ED) never seek treatment for their condition, and those men who do often wait until their symptoms become too severe to ignore (Burns & Mahalik, 2007; Sand et al., 2008e). When men are willing to seek help, they are sufficiently motivated by their distress to entertain a wide range of potential treatments, including changes in diet and exercise, smoking cessation, cutting alcohol and drug use, periodontal treatment, herbs (e.g., red ginseng), acupuncture, natural hormones (e.g., DHEA) and amino acids (e.g., L-arginine), psychological counseling, prescription medications (e.g., Viagra), urethral suppositories, topical creams, testosterone replacement therapy, vacuum pumps, penile injection therapy, external penile prostheses, penile implants, vascular reconstructive surgery, stem cell therapy, platelet-rich plasma therapy, penile shockwave therapy, and penile transplants (Brubaker & Johnson, 2008; Burnett et al., 2020; Dong et al., 2019; Efesoy et al., 2018; Farook et al., 2021; Gurtner et al., 2017; Hatzimouratidis, 2007; Irfan et al., 2020; Ismail et al., 2019; Lau et al., 2008; Li et al., 2017, 2019; Mulhall et al., 2011; Punjani et al., 2018; Raina et al., 2007; Tsai et al., 2017; Ulloa et al., 2008; Walther et al., 2017; Wentzell et al., 2017).
The psychosexual theory of gun ownership suggests that men with SD may also obtain guns in the pursuit of lost virility and masculinity. The idea is that men with SD are initially attracted to guns because they have been socialized to see guns as symbols of male genitalia and masculinity. With this ingrained cultural knowledge, men may seek guns through processes that are either unconscious (because the loss of virility is too painful) or conscious (to communicate manliness to themselves and to others) to overcome their impotence, to somehow make themselves “hard” again (Blum, 2019; Cassino & Besen-Cassino, 2020; Cooke & Puddifoot 2000; Hall, 1953; Nathenson, 2020; Pfaffendorf et al., 2021; Potts, 2000; Stroud, 2012). By allowing men “who have felt disempowered to engage with an archetypal symbol of power” (Nathenson, 2020, p.210), guns may provide some men with the “virility” that their “aging body has surrendered” (Stroud, 2012, pp. 227–228).
In the pages that follow, we use recently collected national survey data to directly examine the association between SD and personal gun ownership. Our primary hypothesis, derived from the psychosexual theory of gun ownership, is that men experiencing SD will be more likely to personally own guns than other men. To formally test this hypothesis, we examine several indicators of SD (performance anxiety, erection trouble, and ED medication) and gun ownership (personal gun ownership, purchasing a gun during the pandemic, and keeping a gun in one’s bedroom).
Data
For this investigation, we use data from the 2021 Crime, Health, and Politics Survey (CHAPS). CHAPS is based on a national probability sample of 1,771 community-dwelling adults aged 18 and over living in the United States. Respondents were sampled from the National Opinion Research Center’s (NORC) AmeriSpeak© panel, which is representative of households from all 50 states and the District of Columbia (https://amerispeak.norc.org/Documents/Research/AmeriSpeak%20Technical%20Overview%202019%2002%2018.pdf). Sampled respondents were invited to complete the online survey in English between May 10, 2021 and June 1, 2021. The data collection process yielded a survey completion rate of 30.7% and a weighted cumulative response rate of 4.4%. The multistage probability sample resulted in a margin of error of ±3.23% and an average design effect of 1.92. The median self-administered web-based survey lasted approximately 25 minutes. All respondents were offered the cash equivalent of $8.00 for completing the survey. The primary purpose of CHAPS is to document the social causes and social consequences of various indicators of health and well-being in the United States during the coronavirus (COVID-19) pandemic. The omnibus survey includes measures of psychosocial characteristics, religious beliefs and experiences, political views and behaviors, neighborhood conditions, experiences with crime and police, stressful life events, health behavior and health lifestyles, mental health, physical health, sexual and reproductive health, and sociodemographic characteristics.
Measures
Gun Ownership
Gun ownership is measured with three items: (a) whether a respondent personally owns “at least one gun or firearm” (1 = yes; 0 = no), (b) whether a personal gun owner purchased “a gun or firearm during the coronavirus (COVID-19) pandemic” (1 = yes; 0 = no), and (c) whether a personal gun owner “keeps any guns or firearms in the bedroom where they sleep” (1 = yes; 0 = no).
Sexual Dysfunction
Sexual dysfunction is also measured with three items: (a) whether a respondent felt “anxious about their ability to perform sexually” in the past year (1 = never to 5 = always), (b) whether a respondent had “trouble achieving or maintaining an erection during sexual activity” in the past year (1 = never to 5 = always), and (c) whether a doctor or health professional had ever prescribed a respondent “any medication for erectile dysfunction or ED (e.g., Viagra, Levitra, or Cialis)” (1 = yes; 0 = no). The first two items were drawn from the work of Laumann and colleagues (1992). The medication question was developed from information provided by a publicly available erectile dysfunction questionnaire.
Background Variables
Analyses include several potential background correlates of gun ownership and SD, including age (continuous years), race/ethnicity (1 = non-Hispanic white; 0 = otherwise); rural residence (1 = rural; 0 = otherwise); southern residence (1 = South; 0 = otherwise), college degree (1 = 4-year college degree or higher; 0 = otherwise), employment (1 = employed; 0 = otherwise), and annual household income (1 = < $10,000 to 9 = ≥ $150,000). Finally, financial strain is measured as the mean response to three items (α = 0.89). Respondents were asked to indicate the extent to which a respondent’s household had trouble paying for (a) for needed health care, (b) monthly bills, and (c) food (1 = never to 5 = all the time).
Analysis
Given our focus on erectile dysfunction, our analytic sample is limited to a national probability sample of 844 men (total possible sample size). Due to listwise deletion of missing data on erection trouble (n = 64), performance anxiety (n = 61), ED medication (n = 59), gun ownership (n = 14), financial strain (n = 11), and rural residence (n = 11), our analytic sample ranges from 780 to 790 respondents or between 92% and 94% of the total sample of men.
Post-stratification weights were used in subsequent analyses to reduce sampling error and non-response bias. NORC developed post-stratification weights for CHAPS via iterative proportional fitting or raking to general population parameters derived from the Current Population Survey (https://www.census.gov/programs-surveys/cps/data.html). These parameters included age, sex, race/ethnicity, education, and several interactions (age*sex, age*race, and sex*race).
Our analyses begin with weighted descriptive statistics for all study variables, including variable ranges, sample means, and standard deviations (Table 1). We then use binary logistic regression to model our dichotomous gun ownership outcomes as a function of SD measures (Tables 2–4). We present six regression models with odds ratios, 95% confidence intervals, and two-tailed statistical tests. Models 1–3 regress personal gun ownership on each measure of SD (separately). Model 4 regresses personal gun ownership on all three measures of SD (together). Model 5 adds age, race, rural residence, and southern residence. Finally, Model 6 introduces college degree, employment, household income, and financial strain to represent our full model. Output and supplemental analyses are available upon request from the lead author.
Weighted Descriptive Statistics (CHAPS 2021).

Note. n = 780.
Weighted Logistic Regression of Personal Gun Ownership (CHAPS 2021).
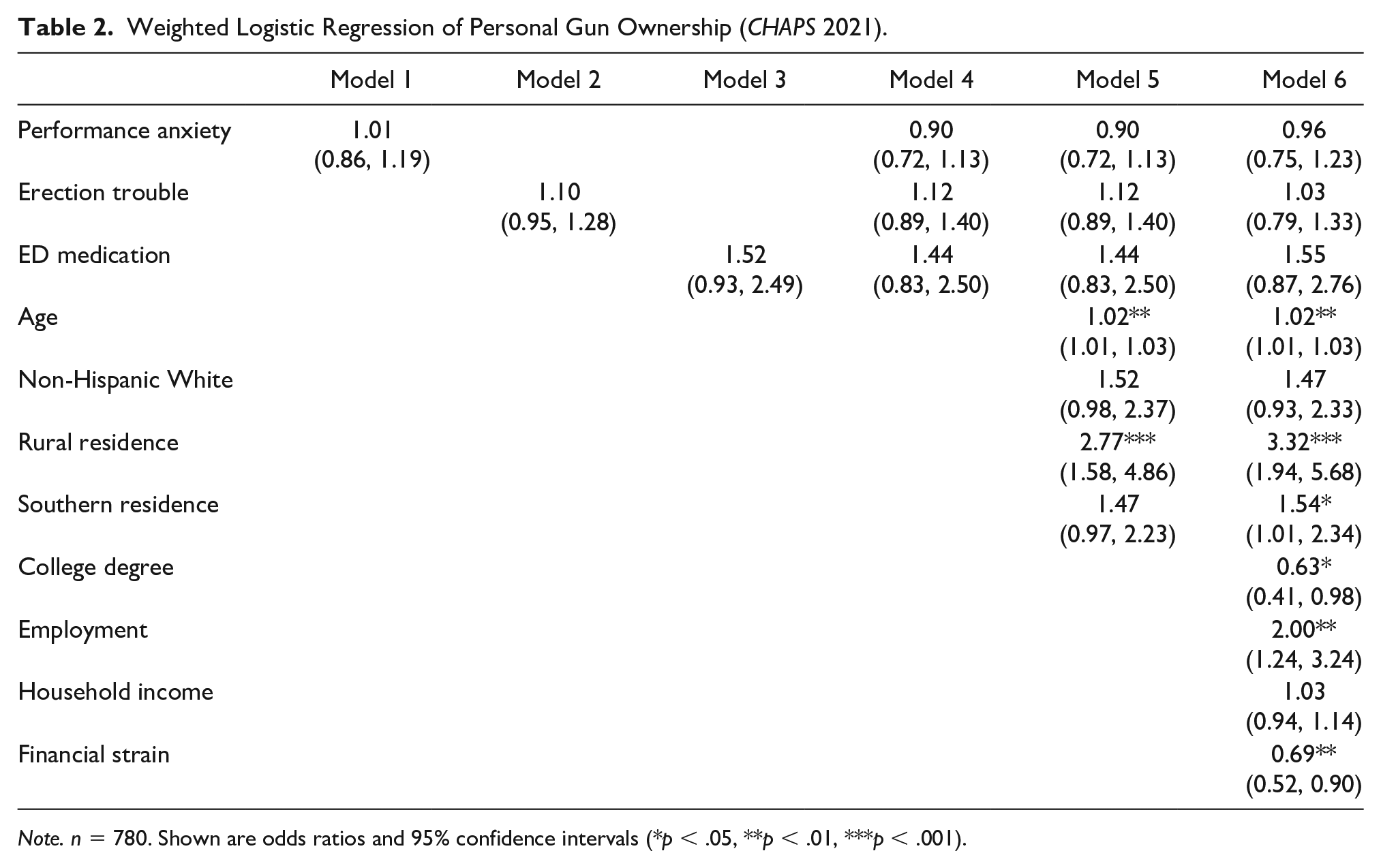
Note. n = 780. Shown are odds ratios and 95% confidence intervals (*p < .05, **p < .01, ***p < .001).
Weighted Logistic Regression of Pandemic Gun Purchase (CHAPS 2021).

Note. n = 790. Shown are odds ratios and 95% confidence intervals (*p < .05, **p < .01, ***p < .001).
Weighted Logistic Regression of Having a Bedroom Gun (CHAPS 2021).

Note. n = 789. Shown are odds ratios and 95% confidence intervals (*p < .05, **p < .01, ***p < .001).
Results
Descriptive Analyses
Table 1 shows that 37% (n = 289) of men reported personal ownership of a gun, 8% (n = 62) reported purchasing a gun during the pandemic, and 27% (n = 211) reported keeping a gun in the bedroom where they sleep. In terms of SD, the average respondent “rarely” felt anxious about their ability to perform sexually or like they had any trouble achieving or maintaining an erection during sexual activity in the past 12 months. Approximately 19% (n = 148) of men reported having ever been prescribed medication for erectile dysfunction or ED. The average age of the sample was nearly 48 years. The median age of the sample was 46 years. The sample included non-Hispanic whites (63%, n = 491), non-Hispanic blacks (9%, n = 70), Latinos (16%, n = 125), and respondents of other races and ethnicities (12%, n = 94). While few men reported living in a rural area (15%, n = 117), over one-third of men reported living in the South (38%, n = 296). Over one-third of men reported having a 4-year college degree or higher (38%, n = 296), and nearly two-thirds reported being employed full- or part-time. The average respondent also reported an annual household income between $50,000 and $74,999 and “rarely” having any difficulty paying for health care, food, or other bills.
Regression Analyses
Table 2 features the regression models for personal gun ownership. The odds ratios (ORs) reported in this table can be manipulated ([OR - 1] × 100) to describe the percentage difference in the odds of personally owning a gun for each one-unit change in the independent variable of interest. These models are easily interpreted. Across all models, with and without adjustments for background variables, we failed to observe any associations between SD and the odds of personally owning a gun. There was no evidence to suggest that men who felt anxious about their ability to perform sexually, had trouble achieving or maintaining an erection during sexual activity, or were ever prescribed medication for erectile dysfunction were more or less likely to personally own a gun than men who did not report these issues. In Model 6, the full model, we observed that the odds of personally owning a gun were 2% higher for each additional year of age ([1.02 - 1] × 100), 255% higher for residents of rural areas, 54% higher for residents of southern states, 37% lower for men with college degrees, 100% higher for employed men, and 31% lower for each unit increase in financial strain.
Table 3 presents the regression models for pandemic gun purchases. In Models 1–3, we failed to observe any associations between SD and the odds of personal gun owners having purchased a gun during the pandemic. In Model 4, we see some inconsistent associations. While each unit increase in sexual performance anxiety increased the odds of a pandemic gun purchase by 44%, each unit increase in erection trouble reduced the odds of a pandemic gun purchase by 36%. In Model 5, these associations were attenuated to insignificance with adjustments for age, rural residence, and southern residence. The associations observed in Model 4 were largely explained by the fact that older men and southern residents reported higher levels of performance anxiety and erection trouble and were more likely to have purchased a gun during the pandemic. Across models, we failed to observe any associations between having ever been prescribed medication for ED and the odds of pandemic gun purchases. In the end, there was no consistent evidence to suggest that men who felt anxious about their ability to perform sexually, had trouble achieving or maintaining an erection during sexual activity, or were ever prescribed medication for ED were more or less likely to have purchased a gun during the pandemic than men who did not report these issues. In Model 6, we observed that the odds of a pandemic gun purchase were 174% higher for rural residents and 135% higher for southern residents.
Table 4 displays the regression models for keeping a gun in one’s bedroom. Once again, across models, with and without adjustments for background variables, we failed to observe any associations between SD measures and the odds of keeping a gun in one’s bedroom. There were, however, several statistically significant background variables in Model 6. In this full model, the odds of keeping a gun in one’s bedroom were 2% higher for each additional year of age, 126% higher for residents of rural areas, 112% higher for residents of southern states, 107% higher for employed men, and 31% lower for each unit increase in financial strain.
In supplemental analyses (not shown), we replicated our focal findings for SD in unweighted regression models. We created a mean SD index using sexual performance anxiety and erection trouble. In fully adjusted weighted regression models (Model 6 specification), the SD index was unrelated to personal gun ownership (OR = 0.98; p > 0.10; 95% C.I. = 0.78, 1.22), pandemic gun purchases (OR = 0.98; p > 0.10; 95% C.I. = 0.73, 1.32), and keeping a gun in one’s bedroom (OR = 0.96; p > 0.10; 95% C.I. = 0.77, 1.20). We considered alternative categorical specifications for sexual performance anxiety and erection trouble. These results were also null. We considered several additional background variables, including marital status, the presence of children under the age of 18, political orientation, religiosity, masculinity, and psychological distress (symptoms of depression and anxiety). None of these variables had any substantive impact on our focal analyses. Finally, we tested interactions between our SD measures and several background variables, including age, race, southern residence, rural residence, and education. We tested 60 total interactions across our gun ownership outcomes. The effects of SD did not vary by age, race, rural residence, or education. However, we were able to detect three statistically significant interactions with southern residence. In the prediction of personal gun ownership, the effects of the SD index (OR = 0.68; p < .05; 0.47, 0.99) and erection trouble (OR = 0.63; p < .05; 0.45, 0.89) were less pronounced for southern residents. In the prediction of keeping a bedroom gun, the effect of erection trouble (OR = 0.63; p < .05; 0.45, 0.89) was also less pronounced for southern residents (OR = 0.68; p < .05; 0.48, 0.97). Although the magnitude of the effects of personal gun ownership and the SD index varied in magnitude by southern residence, their main effects remained null in subsample analyses.
Discussion
Although the association between SD and gun ownership has been popular in social commentary and scholarly work, it has escaped any direct empirical analysis. In this paper, we formally tested whether men experiencing SD are in fact more likely to personally own guns in a national sample of men. Our primary hypothesis, derived from the psychosexual theory of gun ownership, stated that men experiencing SD would be more likely to personally own guns than other men. Our key finding is that the likelihood of gun ownership is comparable for men with and without SD. This conclusion was supported across several indicators of SD (performance anxiety, erection trouble, and ED medication) and gun ownership (personal gun ownership, purchasing a gun during the pandemic, and keeping a gun in one’s bedroom). To our knowledge, we are the first to have formally tested the association between SD and gun ownership in America.
Our analyses are notable because they call into question nearly a century of provocative theorizing, but we are not the first to have cast doubt on the validity of these claims. Nearly five decades ago, Barry Bruce-Briggs (1976), a policy analyst and historian, noted the paucity of scientific support for what he described as the “phallic-narcissist theory.” He revealed that when Arthur Schlesinger, Jr. was asked about the source of his famous statement vis-à-vis men with low virility clinging to their guns, “he responded that he thought it was a ‘cliché.’” (Bruce-Briggs, 1976, p.59). Bruce-Briggs (1976, p.59) went on to explain: “Such statements never cite sources because there are no sources. Every mention of the phallic-narcissist theory assumes it is well known, but there is no study or even credible psychoanalytical theory making the point.”
Guns are clearly phallic symbols (the first proposition). Guns are clearly associated with masculinity (the second proposition). However, the psychosexual theory of gun ownership seems to fail in its assertion that men experiencing SD acquire guns as a means of compensation for lost virility and masculinity. The idea that SD “strikes at the very core of men’s masculine self-concept” is not universally accepted (Sand et al., 2008, p.591). And we have noted that our focal associations were unchanged when we adjusted for masculinity in supplemental analyses. Thus, while some arguments for “compensatory masculinity” are quite credible (e.g., violence as a means of asserting masculinized power in a virulent and criminal fashion), our study cautions against universalizing this theoretical construct to include all behaviors that some may find objectionable (Courtenay, 2000).
If men do not own guns to cope with the lived experience of SD, why do men own guns? It turns out that men primarily own guns for protection (65%) (Parker et al., 2017). In supplemental analyses, we also found that men with SD primarily own guns for protection. This includes men who have been prescribed medication for ED (62%, n = 49), men who reported having trouble achieving or maintaining an erection during sexual activity (68%, n = 144), and men who reported feeling anxious about their ability to perform sexually (67%, n = 145). Men who own guns, with and without SD, mostly own guns to protect themselves and their families, not to project virility and masculinity upon the world. If we accept these self-reports from various sources, most men who own guns are not trying to dominate others. Instead, they are consciously acting to prevent others from dominating them (Stroud, 2012).
We acknowledge that our analyses are limited in several respects. Because our analyses are based on a cross-sectional design, no causal or temporal inferences can be made. Although we suggest that SD might predict gun ownership, this model will require longitudinal data to assess changes in SD and changes in gun ownership. One reason for this is that handling guns has been reported to increase testosterone levels in experimental settings (Klinesmith et al., 2006). Given that androgen deficiency contributes to ED (Yassin & Saad, 2008), gun ownership may be a cause and a consequence of ED. These simultaneous processes could conceivably explain our null findings. While ED could lead to gun ownership, having a gun could in turn protect against ED by increasing testosterone. With this consideration in mind, we are confident that more rigorous longitudinal designs are unlikely to reveal any statistically significant associations between SD and gun ownership. Because our measures of SD and gun ownership are limited to only a few items, the veracity of our analyses is contingent upon replication with more detailed assessments (e.g., the Sexual Health Inventory for Men, SHIM). Finally, there is also the possibility of social desirability bias in self-reports of sexual behavior (Krumpal, 2013). To minimize the potential for bias in reporting (e.g., the experience of shame from reporting ED to another person), CHAPS employed self-administered surveys.
Conclusion
In this study, we showed that men experiencing SD are no more likely to own guns than men without SD. Our findings are important because they contribute to our understanding of factors associated with gun ownership by challenging the belief that phallic symbolism and masculinity somehow drive men experiencing SD to purchase guns. Our findings also remind us of the perils of gun culture rhetoric, which is often characterized by misinformation and political propaganda. Gun owners make a lot of claims about guns. Many will tell you that guns improve their lives, make them happy, and help them to sleep better at night, but none of these claims have been established empirically (Hill, Dowd-Arrow, Davis, et al., 2020; Hill, Dowd-Arrow, Burdette, Hale, et al., 2020; Hill, Dowd-Arrow, Burdette, Warner, et al. 2020). People who do not own guns will tell you that gun owners are motivated by impotence and fear, but these ideas are also unfounded (DeFronzo, 1979; Dowd-Arrow et al., 2019; Hauser & Kleck, 2013; Kleck, 1997). In these instances, gun culture rhetoric functions to justify guns (guns are helpful to me personally), discredit gun owners (gun owners are compensators), and further stigmatize men with SD as “dysfunctional nonpenetrative males” who need guns to cope with their broken bodies (Potts, 2000). Ultimately, these kinds of discussions are counterproductive for society because they distract us from the observable realities of guns and SD. We know that guns threaten public health in the United States (Fleegler et al., 2013; Fowler et al., 2015; Gani et al., 2017; Gramlich, 2019; Miller et al., 2002, 2007; Spitzer et al., 2017; Van Kesteren, 2014). We also know that SD can undermine the well-being of men (Brubaker & Johnson, 2008; Burnett et al., 2020; Burns & Mahalik, 2007; Chambers et al., 2017; Nicolini et al., 2019; Occhipinti et al., 2019; Potts, 2000; Wentzell et al., 2017). These issues will persist until we commit ourselves to more evidence-based discussions of SD and guns in society.
Footnotes
Acknowledgements
The authors thank Cindy Jacobs for valuable comments on previous drafts.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The authors thank the Claude Pepper Center at Florida State University for providing financial support to publish this article in an open access format.
Ethics Approval
The survey was reviewed and approved by the institutional review boards at NORC (21-05-279) and the University of Texas at San Antonio (FY20-21-29). Written informed consent was obtained from all participants.