
Abstract
The possible effects of sildenafil citrate administration at therapeutic dosage on visual acuity, color vision, intraocular pressure, macular thickness, macular volume, and central serous chorioretinopathy in patients with erectile dysfunction were evaluated. The study consisted of 43 male patients diagnosed as having erectile dysfunction according to the first five question version of International Index of Erectile Function (IIEF-5). All patients were given sildenafil citrate 50 mg po 2 to 3 times/week for a month. The patients were evaluated at the first week and at the end of the treatment. The macular thickness and volume assessments with optic coherence tomography did not differ significantly in foveal, parafoveal areas, parafoveal superior hemisphere, parafoveal inferior hemisphere, parafoveal temporal, superior, nasal, and inferior quadrants. Central serous chorioretinopathy was not found in any of the patients.
Introduction
Erectile dysfunction (ED) is defined as the persistent inability to achieve and/or maintain a sufficient erection for satisfactory sexual performance (NIH Consensus Conference, 1993). Worldwide, approximately 152 million men have ED, including about 31 million Europeans (Aytac, McKinlay, & Krane, 1999). With the advent of effective oral therapy, a number of patients with ED expect their sexual activity to be normal. The advent of phosphodiesterase type 5 (PDE5) enzyme inhibition oral therapy for ED introduced a new area in the clinical management of ED. The first PDE5 enzyme inhibitor, sildenafil citrate, has been widely prescribed for ED since 1998. The drug was effective and well tolerated in clinical studies (Morales, Gingell, Collins, Wicker, & Osterloh, 1998; Padma-Nathan, Steers, & Wicker, 1998).
The phosphodiesterases degrade cyclic nucleotides, including cyclic adenosine monophosphate and cyclic guanosine monophosphate (cGMP). Sildenafil citrate relaxes corpus cavernosum by inhibiting PDE5, an important enzyme in signal processing (Dunn, 1998). Inhibition of this enzyme leads to an increase in cGMP, which activates several other molecules causing a decrement in intracellular calcium levels and finally relaxation of the smooth muscle cells (Stief, Uckert, Becker, Truss, & Jonas, 1998). Several studies reported that other vascular structures of organs that contain PDE5 such as lungs, brain, heart, and liver were also affected by sildenafil citrate (Gillies, Roblin, & Jackson, 2002; Michelakis et al., 2003; Rosengarten et al., 2006).
Ocular effects of sildenafil citrate are still being investigated due to some adverse effects such as bluish vision and altered perception of brightness. These effects were attributed to its partial inhibitory effect on phosphodiesterase type 6 (PDE6) enzyme, which regulates the phototransduction cascade. Because PDE5 enzyme is the predominant type of phosphodiesterase in the penis, it is the target of selective PDE5 enzyme inhibitors in the treatment of ED. Inhibitors of PDE5 enzyme cross the blood–retina barrier and can inhibit the retina-specific PDE6 enzyme, which is similar to the PDE5 enzyme and is involved in regulating the phototransduction cascade (Cote, 2006; Laties & Sharlip, 2006). In the international literature on PDE5 enzyme inhibitors, there are some recent articles that describe treatment-related ocular adverse events with sildenafil citrate, such as optic neuropathy, blush vision, subretinal hemorrhage, increased intraocular pressure, and altered perception on brightness (Cunningham & Smith, 2001; Laties & Sharlip, 2006; Morales et al., 1998; Pomeranz, Smith, Hart, & Egan, 2002). Moreover, some case reports describe the central serous chorioretinopathy (CSC) as associated with therapeutic doses of sildenafil citrate (Allibhai, Gale, & Sheidow, 2004; Murata, Ideta, & Kawasaki, 2000; Quiram, Dumars, Parwar, & Sarraf, 2005). CSC is characterized by the focal accumulation of fluid under the neurosensory retina due to the dysfunction of the retinal pigment epithelium. Furthermore, an increase in macular thickness and macular volume has also been shown (macular detachment). Patients typically present with unilateral distortion or loss of central vision, decreased color perception, and relative scotoma. The exact incidence of CSC attributed to sildenafil is not known (Tittl et al., 1999). Also, the mechanism of possible relation between CSC and sildenafil is not clearly shown but mostly speculated. To our knowledge, there has been no published prospective study to date investigating the association between the sildenafil citrate treatment and CSC development.
The aim of the current study was to assess the short-term effects of sildenafil citrate treatment at a therapeutic dose on visual acuity, color vision, intraocular pressure, macular thickness, macular volume, and CSC development in patients with ED.
Method
The study was approved by the local ethical committee, and informed consent was obtained from all subjects before enrollment procedures. A total of 43 patients with a mean age of 49.1 (range = 28-67) years who were admitted to our outpatient clinic for ED were included in the current study. ED was diagnosed on the basis of the first five question version of the International Index of Erectile Function (IIEF-5; score ≤21 = ED). According to physical examination findings, no patient had genitourinary tract abnormality. The European Association of Urology Guideline on Male Sexual Dysfunction recommends that sildenafil citrate could be administered in 25, 50, and 100 mg doses. The recommended starting dose is 50 mg and should be adapted according to the patient’s response and side-effects (Wespes et al., 2012). In light of the guideline, our patients were asked to take 50 mg sildenafil citrate (Viagra®, Pfizer Inc., New York, NY) p.o. two to three times per week. The duration of the treatment was 1 month. Before and after the treatment, the patients were asked to fill the IIEF-5. The patients underwent a detailed ophthalmological examination, which consisted of visual acuity, color vision, intraocular pressure measurements with macular thickness, and volume assessments before and after sildenafil citrate treatment. The ocular examination was performed before, at the first week, and 4 weeks after the treatment. Snellen acuity chart was used for visual acuity assessments. A Goldmann applanation tonometer was used for intraocular pressure measurements. Color vision deficiency was tested with the Ishihara test (38 plate full edition printed in 1990, Kanehara and Co., Tokyo, Japan). Macular thickness and volumes of the patients were measured with RTVue-100 Fourier Domain Optical Coherence Tomography (Optovue Corporation, Freemont, CA). Enhanced macular map five- and three-dimension protocols were used to obtain measurements. Scans with the accurate fixation and ideal signal strength index were selected. Topographic maps contained foveal region of 1 mm diameter, parafoveal region of 3 mm diameter, and perifoveal region of 5 mm diameter.
Patients with previous PDE5 enzyme inhibitor treatment history, corticosteroid use, nitrate usage, hypertension, abnormal liver function tests, alcoholism and/or drug abuse, history of glaucoma, uveitis, past intraocular surgical procedure, diabetic retinopathy in preproliferative stage, and macular pathology history were excluded from the study. Before the treatment, type 2 diabetes mellitus was detected in 7 of the 43 patients (16.2%). These patients did not have proliferative diabetic retinopathy findings in ocular examination. No patient had hypertension history. The most common retinal findings in hypertensive retinopathy include focal or generalized constriction of retinal arterioles. Fluorescein angiography shows focal arteriolar hypoperfusion in early phases and multiple subretinal areas of leakage in late phases (Klein, Klein, Moss, & Wan, 1993). In proliferative diabetic retinopathy, the new vessels increase in size and extent, with an increased fibrous component. Moreover, the new vessels regress, leaving residual fibrovascular proliferation along the posterior hyaloid (American Academy of Ophthalmology, 2006). Since the above-mentioned findings of the retinopathy could be mixed with the findings of the CSC, patients having hypertension and/or proliferative diabetes mellitus were excluded from the study.
The patients were reexamined 1 week and 1 month later, with the same procedure described above. To eliminate statistical bias and to make a standardized allocation, only measurements taken from the right eyes were analyzed.
Statistical Analysis
Statistical analyses were performed with Statistical Package for Social Sciences for Windows Version 17.0 (SPSS, Chicago, IL). All variables were tested by Kolmogorov–Smirnov test for normality. This test reported that all variables had a normal distribution. Repeated-measures analysis of variance (ANOVA) test was used to compare measurements taken at the start and measurements taken at the end of the first week and at the end of the first month. All data are represented as mean ± standard deviation. The corresponding 95% confidence intervals (CIs) were estimated using repeated-measures ANOVA test, including macular thickness and macular volume parameters. A p value less than .05 was considered significant.
Results
According to IIEF-5 scores, the patients’ erectile function significantly improved after the treatment (pretreatment IIEF-5 score: 11.2 ± 3.8, posttreatment IIEF-5 score: 17.3 ± 4.9, p < .001).
None of the patients had abnormal visual acuity, color vision, and increased intraocular pressure after the treatment. Visual acuity measurements were the same in all patients before and after the treatment. There was no alteration in visual acuities. There was no disturbance in color vision assessments, performed at the same time as visual acuities. The mean intraocular pressure measurements were also similar, and they did not show any significant variation among measurements performed before, at the first week, and after 4 weeks of the treatment. The mean intraocular pressure was 14.56 ± 3.21 mmHg before the treatment, 14.2 ± 3.01 mmHg at the end of first week, and 14.32 ± 3.03 mmHg at the end of 4 weeks (p = .814).
Macular thickness measurements did not identify any significant change among three measurement times, in all thickness assessment areas in foveal, parafoveal, and perifoveal regions (Table 1). Also, macular volume measurements did not show statistically significant differences in relation to the time among cases (Table 2).
Macular Thickness Measurements of the Patients.

Note. CI = confidence interval.
Macular Volume Measurements of the Patients.
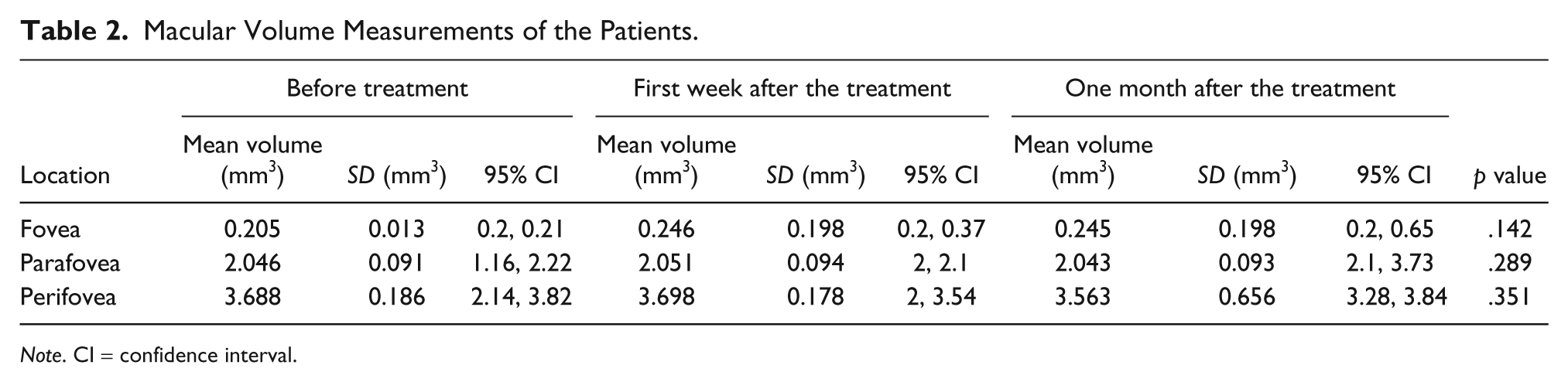
Note. CI = confidence interval.
Discussion
PDE5 enzyme inhibitor oral therapy has radically changed the clinical management of ED. Since becoming available in 1998, the PDE5 enzyme inhibitor sildenafil citrate has become the most widely prescribed drug for ED. Sildenafil citrate is responsible for degradation of cGMP in the corpus cavernosum of the penis, promoting smooth muscle relaxation and increasing the inflow of blood into the corpus cavernosum (Dunn, 1998; Gillies et al., 2002; Michelakis et al., 2003; Rosengarten et al., 2006). Sildenafil citrate has possible effects on ocular circulation. After administration of sildenafil citrate, Sponsel and associates reported a significant increase in pulsatile ocular blood flow (Sponsel et al., 2000). A significant increase in ophthalmic artery flow velocity was also reported by Dundar, Dundar, Kocak, Dayanir, and Ozkan (2001), thought to be secondary to vasodilatation effect. However, a study reported no significant changes in optic nerve rim or foveolar choroidal blood flow (Grunwald, Siu, Jacob, & Dupont, 2001). Another adverse ocular effect possibly associated with PDE5 enzyme inhibitors has been recently published, describing optic neuropathy leading to loss of vision (Cunningham & Smith, 2001; Laties & Sharlip, 2006; Morales et al., 1998; Pomeranz et al., 2002).
CSC typically affects both men and women between 30 and 60 years of age. There is typically no pain and no history of trauma. Diagnosis is clinical and confirmed by fluorescein angiography. An array of risk factors, including refractive state, systemic high blood pressure, male gender, age, ethnic background, and corticosteroid usage, have been identified. Spontaneous visual recovery occurs in approximately 85% of patients with CSC within 1 to 6 months (Tittl et al., 1999).
In 2000, Murata and associates published the first case report: a unilateral case of CSC in a 33-year-old man taking sildenafil citrate (Murata et al., 2000). The condition spontaneously resolved within days when sildenafil citrate treatment was stopped (positive dechallenge) and recurred (positive rechallenge) when he took the same agent again, 1 year later. In 2004, Allibhai and coworkers described a unilateral case of CSC in a 37-year-old man taking sildenafil citrate with positive dechallenge within 3 weeks of discontinuing sildenafil citrate(Allibhai et al., 2004). In 2005, Quiram and colleagues reported two cases of CSC after stopping sildenafil citrate treatment who had positive dechallenge (Quiram et al., 2005). One patient in this report, who was followed for a total of 16 months, had no recurrence of CSC after stopping sildenafil citrate treatment. The other case was a 70-year-old man with bilateral CSC in whom a positive rechallenge occurred with sildenafil citrate. In 2008, Fraunfelder and Fraunfelder reported 11 men with CSC who had taken sildenafil citrate (Fraunfelder & Fraunfelder, 2008). Of the 8 men who stopped sildenafil citrate after the onset of CSC, 6 had improved vision and 2 continued to manifest CSC. It is unclear from these case reports whether sildenafil citrate causes CSC, because the majority of patients with the disorder are expected to improve spontaneously. In 2010, French and colleagues reported a case–control postmarketing surveillance study (French & Margo, 2010). According to the study, the likelihood of past exposure to PDE5 enzyme inhibitors among newly diagnosed patients with CSC was compared with two age-matched control groups after excluding subjects with risk factors for CSC. In this study, among 577 men, aged 59 years and younger with newly diagnosed CSC during the study year, 19.2% (n = 111) were prescribed a PDE5 enzyme inhibitor (sildenafil citrate 100 mg). The proportions of age-matched controls prescribed a PDE5 enzyme inhibitor in the two groups were 18.5% and 21.5%. The authors concluded that patients with CSC had no increase in prescription exposure to PDE5 enzyme inhibitors than did age-matched control subjects. Also, they stated that their results do not support an association between CSC and PDE5 enzyme inhibitors, and postmarketing surveillance methods for drug-related side effects have acknowledged limitations.
The mechanism by which sildenafil citrate could cause CSC and macular detachment is up for debate. It is possible that sildenafil citrate has an effect of choroidal vasculature. Prunte and Flammer (1996) claimed that CSC occurs secondary to abnormalities in choroidal perfusion. Localized vascular congestion and impairment of circulation results in ischemia, allowing choroidal exudation through a focally hyperpermeable choroid. McCulley, Luu, Marmor, and Feuer (2002) reported a 33% increase in choroidal thickness; however, this did not correlate with loss of vision. Quiram et al. (2005) proposed that engorgement of the choroid in select patients could lead to leakage across the retinal pigment epithelium and accumulation of subretinal fluid. Metelitsina, Grunwald, DuPont, and Ying (2005), however, did not find that sildenafil caused a statistically significant change in the foveolar choroidal circulation in a subset of macular degeneration patients. CSC usually resolves rapidly after discontinuation of sildenafil citrate treatment (Allibhai et al., 2004; Quiram et al., 2005; Sponsel et al., 2000).
In the present study, our patients’ macular thickness and macular volume did not significantly change after a 1-month treatment with a therapeutic dose of sildenafil citrate. Also, CSC did not develop in any of our patients. Moreover, visual acuities and intraocular pressures did not change, and no color vision abnormalities were detected.
Finally, our short-term prospective study showed that sildenafil citrate treatment at a therapeutic dose did not lead to CSC and visual abnormality in our patients. In light of literature, a causal relationship has not yet been established between sildenafil citrate treatment and CSC development. To our knowledge, there has been no published prospective study to date investigating the association between sildenafil citrate treatment and CSC development. In the literature, CSC facts emerged during the use of sildenafil citrate in various time scales (1 day to 2 years). That is why it is not possible to be certain about which dose of sildenafil citrate has caused CSC in which time scale. The main weakness of this study could be short-term follow-up of patients and use of a lower dose (instead of 100 mg, 50 mg was used). These results should be verified by further studies with long-term follow-up of patients and the use of a higher dose.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.