
Abstract
Context:
Several studies reported the application of androgen deprivation therapy and radiotherapy in patients with biochemical recurrence after prostate cancer operation.
Objective:
To perform a systematic review and meta-analysis evaluating of endocrine therapy and radiotherapy in patients with biochemical recurrence after prostate cancer surgery. The primary end point was biochemical progression-free survival (bPFS). Secondary end point was overall survival (OS).
Methods:
A systematic review of PubMed/Medline, Embase, and Cochrane databases to identify relevant studies published in English up to March 2020. Twelve studies were selected for inclusion.
Results:
There were 11 studies included in the present study. Including two randomized controlled trials and nine cohort studies. The meta-analysis shows a significant bPFS benefit from androgen deprivation therapy and radiotherapy in patients with biochemical recurrence after prostate cancer operation. (hazard ratio [HR]: 0.57; 95% confidence interval CI, 0.52–0.63; p < .001). For patients with GS < 7 and low-risk patients, combined treatment can have a benefit for BPFs (HR: 0.53; 95% CI, 0.37–0.76; HR: 0.58; 95% CI, 0.36–0.93). Androgen deprivation therapy and radiotherapy in patients with biochemical recurrence was associated with a slightly OS improvement (HR: 0.73; 95% CI, 0.57–0.93; p = 0.01).
Conclusions:
Compared with salvage radiotherapy alone, This meta-analysis shows a significant bPFS benefit from endocrine therapy combined with salvage radiotherapy in patients with biochemical recurrence after prostate cancer operation. And benefit more for high-risk groups. However, there was no significant benefit in group GS ≥ 8. It shows a slightly OS benefit from endocrine therapy combined with salvage radiotherapy in patients with biochemical recurrence.
Introduction
Prostate cancer has become the second most common male cancer in the United States, and its incidence rate is on the rise (Siegel et al., 2018). Approximately 15 to 30% of prostate cancer patients after primary local therapy are at risk of PSA recurrence (Charles et al., 1999; Ward et al., 2003). Patients with elevated PSA level after prostate cancer surgery face greater risk of metastasis (Moul et al., 2004). For the patients with biochemical recurrence, it is quite difficult to distinguish between local prostate cancer bed recurrence and distant metastasis recurrence by image data, especially for the early stage of biochemical recurrence. In previous studies, androgen deprivation therapy (ADT) by medical or surgical castration is a treatment for biochemical recurrence after prostate cancer operation, because the androgen receptors play an important role in the development of prostate cancer (Charles Huggins & Clarence, 1941). Endocrine therapy can improve the endpoint of high-risk prostate cancer, but chemoradiotherapy appears to improve the risk/benefit ratio even further (Dirk et al., 2016).
Several recent clinical studies have shown that salvage radiotherapy can improve the overall survival of patients with biochemical recurrence after prostate cancer surgery (Picchio et al., 2003; Scattoni et al., 2003). Nevertheless, it is contradictory whether salvage radiotherapy combined with endocrinotherapy can improve the clinical efficacy. (King et al., 2004; Soto et al., 2012). We hope to find out whether androgen deprivation combined with salvage radiotherapy is beneficial to patients’ disease progression through this meta-analysis.
Methods
Literature Search and Study Selection
The identification and selection of the studies were conducted according to the Preferred Reporting Items for Systematic Reviews and Meta-analysis (PRISMA) criteria and the Population, Intervention, Comparator, Outcomes (PICO) methodology. PICO was defined as follows: Patients with biochemical recurrence after radical prostatectomy (P) Salvage radiotherapy combined with endocrine therapy (I) Salvage radiotherapy (C) overall survival, biochemical progression-free survival (O) (Shamseer et al., 2015). This meta-analysis database mainly consists of PubMed, Embase and Cochrane Library. Search the database until March 01, 2020. The retrieval strategy is free word and subject word method. The specific search terms are “radiotherapy,” “salvage radiotherapy,” “androgen deprivation therapy,” “endocrine therapy,” “radical prostatectomy.” The supplementary literature mainly comes from the references after the literature. The original text cannot be retrieved from the database. Contact the author by e-mail to obtain the data. The meta-analysis is based on the analysis and evaluation of previous published articles, so it does not involve medical ethics.
Data Extraction and Study Quality
This Meta-analysis has the following criteria: (1) The risk point estimate was reported as an HR with the 95% CI, Or the survival curve and related data can be used to calculate HR indirectly. (2) Types of study: randomized controlled trials or cohort study. (3) Patients reach the biochemical recurrence standard after radical prostatectomy. (4) The initial treatment of prostate cancer is radical rostatectomy. (5) The experimental group was endocrine therapy combined with salvage radiotherapy, while the control group was only salvage radiotherapy. Patients were excluded if they had undergone previous androgen deprivation therapy or pelvic radiotherapy, if the initial status at the time of surgery was pN1, if histology findings showed cancer other than adenocarcinoma. The diagnosis standard of biochemical recurrence of prostate cancer was PSA ≥ 0.2 ng/mL twice in a row after radical prostatectomy (Carter et al., 2013). BPFS was defined as serum PSA rising above the posttreatment nadir to a level of 0.2 ng/mL or more with a confirmatory value or by the initiation of salvage ADT after completion of SRT (Stephenson et al., 2007). All patients received three-dimensional (3D) conformal radiotherapy or intensity modulated radiotherapy, based on dosimetric CT scans. The planned target volume included the prostate operative bed. The dose given to the prostate bed was 66 Gy in 33 fractions, 5 days a week for 7 weeks. For each selected study, the following items were recorded in an Excel: Primary Endpoints, Secondary Endpoints, Treatment, Subgroup Source, Follow-up time, Average age. The cohort study used Newcastle-Ottawa Scale (NOS) scoring criteria. Randomized controlled study mainly used Cochrane Collaborative Network bias risk assessment criteria.
Statistical Analysis
The meta-analysis method mainly relies on Review 5.3 software systems. Meta-analyses were performed for primary and secondary outcome parameters: overall survival, Biochemical progression free survival. Heterogeneity was assessed using Cochran Q statistic and quantified using the I2 statistic. The heterogeneity was classified as low (I2 ≤ 50%) and high (I2 > 50%). If the heterogeneity is high, a random effect model is used. If the heterogeneity is low, a fixed effect model is used (Stephenson et al., 2007). If the heterogeneity is high, subgroup analysis and sensitivity analysis are used to find the reason of high heterogeneity.
Result
Characteristics of Studies
A total of 6795 documents were included in the selection. After gradual screening, 11 documents were finally included in this meta-analysis. The process of literature search and screening are detailed in Figure 1. Basic information of finally documents included in Table 1. The risk of bias is detailed in Figure 6.

Preferred reporting items for systematic reviews and meta-analyses flow chart for study selection. RCT = randomized controlled trial.
Basic Information Included in the Literature.

Note. *BF = biochemical failure; BPFS = Biochemical progression free survival; OS = overall survival; RCT = randomized controlled trial.
bPFS
The meta-analysis shows a significant bPFS benefit from androgen deprivation therapy and radiotherapy in patients with biochemical recurrence after prostate cancer operation (hazard ratio [HR]: 0.57; 95% confidence interval CI, 0.52–0.63; p < .001) (Figure 2). There was no significant heterogeneity between studies (I2 = 23%). For patients with GS < 7 points, combined treatment can have a benefit for bPFF (HR: 0.53; 95% CI, 0.37–0.76; p < .001). But there was no significant benefit in patients with GS ≥ 8 points (HR: 0.79; 95% CI, 0.54–1.14; P = .21) (Figure 3).

Forest plots of the effect of endocrine therapy and radiotherapy in patients with biochemical progression-free survival after prostate cancer surgery.

Forest plots of the effect of endocrine therapy and radiotherapy in patients with biochemical progression-free survival after prostate cancer surgery. Subgroup analysis: (1.2.1) GS ≤ 7 points; (1.2.2) GS ≥7 points; (1.2.3) low/intermediate risk patients; (1.2.4) High risk patients.
Overall Survival
Only two retrospective studies reported the effect of combination therapy on OS. Androgen deprivation therapy and radiotherapy in patients with biochemical recurrence was associated with a slightly OS improvement (HR: 0.73; 95% CI, 0.57–0.93; p = .01) (Figure 4).

Forest plots of the effect of endocrine therapy and radiotherapy in patients with OS after prostate cancer surgery.
Publication Bias
In the literature analysis of different outcome indicators, we found no significant publication bias. Because funnel plots show that the literature is in a relatively symmetrical position, we believe that there is less possibility of publication bias (Figure 5). At the same time, Egger’s test results showed that t = 0.46, p = .673. indicating that the possibility of publication bias is low.
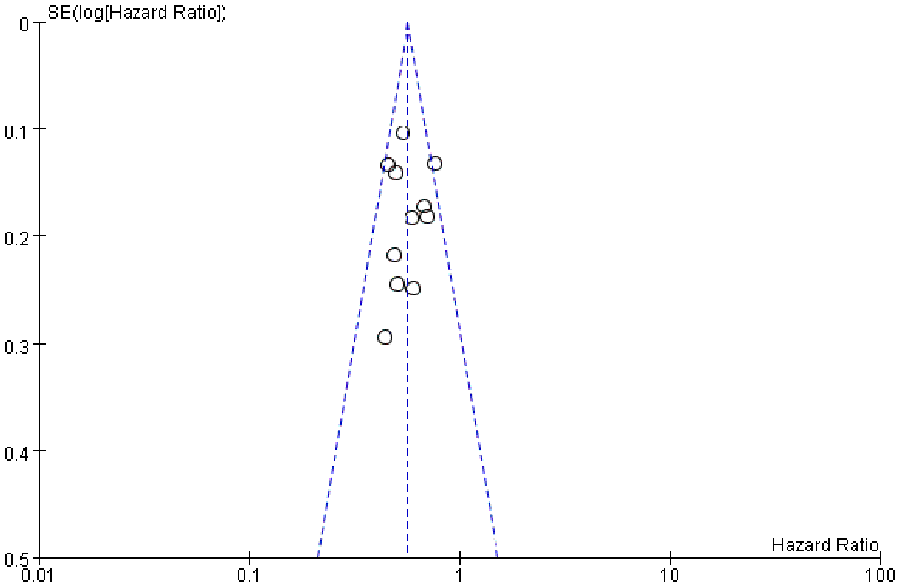
Funnel chart of publication bias.

Cochrane Collaborative Network Bias Risk Assessment Criteria for RCT.
Discuss
This meta-analysis is the first comprehensive report on the influence of salvage radiotherapy combined with ADT on the biochemical recurrence of prostate cancer after operation. It is also the most detailed meta- analysis with 6,795 participants. Among men with biochemical recurrence after prostate cancer surgery, we found a significant bPFS benefit. Compared with the low-risk group, the benefit was more significant for patients with high-risk prostate cancer. But there was no significant benefit in different GS subgroups. It may be related to the small number of included samples. Only two retrospective studies conducted statistical analysis in detail with different GS scores. Patients with biochemical relapses had a slight improvement in OS after androgen deprivation therapy and radiation therapy. Twelve articles were included, of which 10 cohort studies had NOS scores above 6, of which 2 RCT had a low risk of bias according to Cochrane Collaborative Network bias risk assessment criteria.
About one-third of prostate cancer patients had biochemical relapse of PSA, and there was no evidence of clinical and imaging recurrence (Charles et al., 1999). Antonarakis et al. found that among biochemical recurrence patients without salvage radiotherapy, 5-year and 10-year metastasis-free survival rates were 67% and 48%, respectively (Antonarakis et al., 2011). In a study of 2657 subjects, Boorjian et al. found that salvage radiotherapy reduced the risk of distant metastasis by 75% (Boorjian et al., 2009). Shipley et al found in an RCT that bicalutamide combined with radiotherapy can improve the 2-year overall survival rate of patients, and benefit more for the population with PSA greater than 1.5 µg/mL (Shipley et al., 2011). This is consistent with our meta-analysis results, but in our meta-analysis, the original study has a longer follow-up period and the results are more meaningful.
The first randomized controlled trial of salvage radiotherapy combined with endocrine therapy was started in 1998, involving 760 patients. The endocrine therapy program was bicalutamide treatment for 24 consecutive months. The results showed that the combination of drugs can slightly improve survival time (HR: 0.76; 95% CI, 0.59–0.99; p = .04) (Struss & Black, 2017). Another follow-up randomized controlled trial also showed a significant benefit to bPFS (HR: 0.50; 95% CI, 0.38–0.66; p < .01) (Christian & Ali, 2016). Compared with the conclusion of meta-analysis, the improvement of bPFS is more obvious in this randomized controlled experiment. It is not difficult to find that this RCT androgen deprivation therapy is only injection of goserellin. Further studies are needed to confirm whether monotherapy can improve the prognosis. Similar results were also found in previous retrospective cohort studies. The high risk factors of tumor recurrence include lymph node metastasis, positive margin, tumor size and tumor pathological score. In the two cohort studies (Jang et al., 2012; King et al., 2004), it was found that for the group with GS score <7, the combination of drugs could significantly benefit BPFs, but for the group with GS score >7, there were conflicting results, only one study showed slight benefit. In the retrospective study, only one report reported the effect of BPFs on patients with positive margin after prostate cancer operation. We can find a significantly benefited in patients with positive margin, but not in patients with negative margin (Parekh et al., 2015). Due to the limitations of the original literature, no subgroup analysis was conducted on the margin and GS scores during the meta-analysis.
Radiotherapy develops from traditional two-dimensional radiation to precise radiation, it can greatly increase the dose of tumor irradiation and reduce the dose of normal tissue. The curative effect of radiotherapy for localized prostate cancer is equivalent to that of radical operation. According to the literature, compared with the traditional radiotherapy technology, 3 dimensional conformal radiation therapy and intensity modulated radiation therapy have a lower rate of adverse reactions, and higher BRFS rate and local control rate (Ost et al., 2009). The disease-free survival rate of patients with prostate capsule invasion and positive margin is only 37%~70%. Postoperative adjuvant radiotherapy can further improve local control rate and disease-free survival rate of prostate cancer patients at risk of recurrence (Ehmann and Wenz, 2013). According to this meta-analysis, salvage radiotherapy combined with endocrine therapy after prostatectomy can significantly improve the clinical effect. The comprehensive application of radiotherapy in different treatment periods of prostate cancer will bring new choices for clinical treatment.
There are still many limitations in this meta-analysis. First, this literature search is limited to articles published in English, so there may be publication bias. Secondly, the number of literatures included in this meta-analysis is small, and the total number of samples included is only 6795, which affects the promotion of the results. Third, the vast majority of the included literature are retrospective studies, only 2 randomized controlled trials, need more high-quality, large sample randomized controlled trials to further improve.
Conclusion
This meta-analysis shows a significant bPFS benefit from endocrine therapy combined with salvage radiotherapy in patients with biochemical recurrence after prostate cancer operation. And benefit more for high-risk groups. However, there was no significant benefit in group GS ≥ 8. It shows a slightly OS benefit from endocrine therapy combined with salvage radiotherapy in patients with biochemical recurrence. Due to the limitation of original literature, the results of meta-analysis in this paper need to be further verified and improved by large sample and high-quality randomized controlled trials.
Supplemental Material
sj-docx-1-jmh-10.1177_15579883211024881 – Supplemental material for Effect of Salvage Radiotherapy and Endocrine Therapy on Patients with Biochemical Recurrence After Prostate Cancer Operation— a Meta‑Analysis
Supplemental material, sj-docx-1-jmh-10.1177_15579883211024881 for Effect of Salvage Radiotherapy and Endocrine Therapy on Patients with Biochemical Recurrence After Prostate Cancer Operation— a Meta‑Analysis by Yong Yuan, Qiang Zhang, Chaofan Xie and Tao Wu in American Journal of Men's Health
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the City of Nanchong Strategic Cooperation with Local Universities Foundation of technology (19SXHZ0332).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.