
Abstract
Former research has identified stigmatizing attitudes toward cancer patients in the general population. Little is known about (implicit) attitudes of physicians toward cancer patients. By using the prototype approach, the study investigated German physicians’ prototypical perceptions of cancer patients. Five hundred nineteen physicians (mean age: 46 years, 47% female) who regularly treat cancer patients participated in the questionnaire study. Participants were asked to state three prototype attributes that describe the “typical cancer patient.” Open format answers were coded on the dimensions favorability (coded with unfavorable, favorable, or neutral) and gender-stereotypicality (coded with masculine stereotypical, feminine stereotypical, or gender-neutral). Of all prototype attributes (N = 1,589), 69.9% were coded as unfavorable and 14.3% as favorable, the remaining attributes were neutral (15.9%). Analysis of gender-stereotypicality revealed that nearly half of the attributes (49.5%) were compatible with the feminine, whereas only 6.5% were compatible with the masculine stereotype. The remaining attributes (44.0%) were gender-neutral. There were no significant associations between prototype favorability or gender-stereotypicality and demographic/professional characteristics of physicians. The prototype approach was successful to identify (implicit) attitudes toward cancer patients and might be more sensitive than social distance scales when investigating stigmatizing attitudes. Physicians described the “typical cancer patient” with predominantly unfavorable and feminine attributes, while favorable attributes were underrepresented and positive masculine attributes were barely mentioned. The finding that the “typical cancer patient” lacks (positive) masculine attributes should be followed up in further research.
Introduction
Prevalence and Consequences of Cancer Patient Stereotypes
What is the image of the typical cancer patient? Nearly 50 years ago, Tringo (1970) examined the social distance of U.S. students and rehabilitation workers toward individuals with different disabilities, such as alcoholism, blindness, diabetes, mental illness, and cancer. The author let the participants rate the degree of closeness they would allow persons with several disabilities. He reported the social distance to people with cancer to be higher than, for example, to people with heart disease, blindness, or to amputees. Katz et al. (1987) conducted a study among U.S. lay people and healthcare personnel with a focus on their perceptions of cancer, AIDS, cardiac, and diabetic patients, using semantic differential items. Cancer patients were perceived as less competent, more depressed, more dependent, and sicker compared to patients with diabetes, heart diseases and the comparison group “most people.” Cho, Smith, et al. (2013) investigated public attitudes toward cancer patients in a large population of people with no history of cancer in South Korea. The authors reported that 23–48% of participants agreed or strongly agreed to discriminating statements (e.g., „I feel uncomfortable when I am with cancer patients”). The public image of cancer and the related stigma as perceived by Health Care Professionals (HCP) was the focus of a qualitative study conducted by Simon et al. (2011) in the UK. Twenty-one HCP were asked how they perceive the prevailing stereotype of, and the public attitudes related to cancer in the general population. According to the participating HCP, the public attitude of cancer is dominated by negative and pessimistic beliefs (e.g., cancer as a “death sentence”), while positive views, for example, successes in cancer treatment, are underrepresented (Simon et al., 2011).
Marlow and Wardle (2014) focused on public cancer stigma and developed the Cancer Stigma Scale (CASS), a questionnaire that aims to assess cancer stigma in non-patient populations. In 2015, a study using the CASS in large UK sample revealed that lung cancer attracts the highest stigma compared to breast, cervical, colorectal and skin cancer (Marlow et al., 2015). A large study conducted with a German representative population (N = 2,420) assessed stigmatizing attitudes toward cancer patients using a 9-item social distance scale (Ernst et al., 2016). The survey reported some indication for stigmatization, that is, 19% of the respondents said that they would not use the same dishes as cancer patients and 15% said they would have problems to have a person with cancer as a daughter/son in law. But altogether the prevalence of stigmatizing attitudes was rather low. The authors point to some serious methodological limitations of the used scale and acknowledge the possibility that answers might have been biased by social desirability tendencies.
Consequences of stereotyping or stigmatization on cancer patients’ psychological well-being have been investigated in several studies. Results indicate that perceived stigma among cancer patients can be associated with negative emotional states like anxiety (Cataldo & Brodsky, 2013), depression (Cataldo & Brodsky, 2013; Cho, Choi, et al., 2013; Phelan et al., 2013) and self-blame (Else-Quest et al., 2009). A review on cancer stigma and resulting health consequences pointed out that the fear of being stigmatized might influence preventive and illness behavior, that is, lead to under-utilization of healthcare services and low adherence to physicians’ recommendations (Fujisawa & Hagiwara, 2015).
Cancer Patient Stereotypes in Healthcare
What do physicians have in mind when they think of the typical cancer patient? To our knowledge there is no study that explicitly asked physicians how they perceive the typical cancer patient. Research has revealed that physicians are not free from (stereotypical) assumptions and implicit biases in their patient-physician interaction (Chapman et al., 2013; FitzGerald & Hurst, 2017; Liang et al., 2019; Sriram et al., 2015; van Ryn & Burke, 2000). Stereotypical beliefs and assumptions can be related to demographic, social or behavioral characteristics of patients, for example, age, socioeconomic status, education, perceived likeability and competence, or type of disease (Gerbert, 1984; Kearney et al., 2000; Liang et al., 2019; van Ryn & Burke, 2000). A recent systematic review by FitzGerald and Hurst (2017) concluded that healthcare professionals exhibit the same levels of implicit bias related to various patient characteristics (e.g., age, gender, race or patients’ social circumstances) as the wider population. A large study including N = 1,778 U.S. participants investigated implicit and explicit attitudes regarding lung versus breast cancer among cancer patients, caregivers, healthcare providers and members of the otherwise general public (Sriram et al., 2015). The study revealed that all four groups had comparable levels of negative implicit bias toward lung cancer.
Examining cancer stereotypes and attitudes held by physicians is considered crucial for finding out how physicians potentially reinforce stereotypes in their physician-patient interaction (Harwood & Sparks, 2003). For example, physicians’ perceptions might impact self-stereotyping of cancer patients. The stereotype embodiment theory by Levy (2009) postulates how stereotypes are embodied and how they influence functioning and health. The theory was proposed as a psychosocial approach to aging and the consequences of negative aging stereotypes. Levy states that internalized stereotypes gain salience and become incorporated over time. As a result, stereotypes influence individuals on multiple pathways and become relevant on a psychological, behavioral and physiological level (Levy, 2009).
The current study focuses on physicians’ perceptions of cancer patients using the prototype approach. Assessing prototypes allows investigating attitudes toward groups of people in an indirect way and might therefore be better suited to identify negative attitudes than direct measures as used in the recent German survey of Ernst et al. (2016).
Prototype Approach: Favorability, Similarity, and Gender-Stereotypicality
Prototype matching theory introduced by Niedenthal et al. (1985). postulates that social decisions (e.g., favoring a situation or a behavior) are more likely if the prototype of the typical representative (of this situation or this behavior) is perceived as (rather) favorable and similar to one’s own self-concept (Niedenthal et al., 1985). This approach has since been applied in health psychology to predict health risk behavior of adolescents through gathering (implicit) attitudes about different groups of persons, for example, about the “typical smoker” (Gibbons & Eggleston, 1996), the “typical (un-) healthy eater” (Gerrits et al., 2009) or the “typical drinker” (van Lettow et al., 2013). In prototype research, prototype favorability and prototype similarity are two central determinants used to explain the influence of prototype perceptions on behavior (Gibbons et al., 1995). In the current study which aimed to assess the contents of the typical cancer patient prototype, the perception of prototype favorability of a typical cancer patient represents a central dimension. The perception of similarity of self-concept to prototype is not considered in this study, as study participants were physicians (and not cancer patients).
Instead of examining similarity to protoype, a second, self-constructed dimension was used in this study, which is assumed to be relevant in assessing prototype perceptions. Previous prototype research has not yet considered the extent to which prototypes are described with typically masculine or feminine characteristics. Accordingly, in addition to the evaluation of prototype favorability, in this study gender-stereotypicality is considered as a second dimension. The dimension gender-stereotypicality is used to examine to what extent the “typical cancer patient” complies with traditionally masculine and feminine gender stereotypes.
Traditional Masculinity and Chronical Illness
Being a cancer patient is often associated with negative affect like anxiety, fear, depression (Anderson et al., 2008) and the feeling of loss of control (McWilliam et al., 2000). These characteristics contradict attributes that are traditionally considered to be masculine strengths, such as being strong, dominant, robust and independent (Bem, 1974; Williams et al., 1999) and they also contradict masculine norms like winning, pursuit of status, emotional control, risk-taking or self-reliance (Levant et al., 2020; Mahalik et al., 2003). In his influential theory of gender and health, Courtenay cited Kaufman (1994) and described that “Men’s acquisition of power requires, for example, that men suppress their needs and refuse to admit to or acknowledge their pain” (Courtenay, 2000, p. 1389).
Research with cancer patients indicates that getting cancer can be regarded as a particular challenge for men especially when they endorse a traditional conception of masculinity. A large longitudinal study among 8,054 U.S. cancer patients reported that cancer led to more negative psychological impacts in men than in women. The study revealed that cancer patients of both sexes who had a strong adherence to traditional masculine ideals (e.g., being confident and taking control) had more depressive symptoms, compared to patients with less adherence to dominant masculinity beliefs (Pudrovska, 2010). To investigate the specific challenges of cancer in terms of masculinity, Hoyt et al. (2013) have developed a questionnaire that measures cancer-related masculine threat (CMT). A longitudinal study including 66 prostate cancer patients revealed that CMT predicted decreases in prostate-cancer related functioning (i.e., urinary, bowel, sexual), as well as decreased emotional processing. The authors conclude that the belief that having cancer is inconsistent with their masculinity makes male cancer patients vulnerable for declines in prostate-related functioning and for negative effects on emotional coping (Hoyt et al., 2013). A qualitative study among male German bowel cancer patients provided insights in how patients experience body and identity crisis and (self) stigmatization (Reuter & Reuter, 2018). Repeated statements of participants on the association of health and physical fitness with masculinity led the authors to conclude that symptoms like weakness, loss of vitality and physical fitness were not only regarded as signs of illness, but also as unmanly and as a threat to patients’ “identity as a man.”
Aim of the Study
The aim of this study was to examine the perception of the “typical cancer patient” by physicians. The focus was on physicians treating patients with breast, prostate or colorectal cancer, as these cancer types are among the most common. In order to interpret characteristics describing the “typical cancer patient,” special focus was on two dimensions: (1) The (un-) favorability hypothesis: the “typical cancer patient” is described by more unfavorable than favorable attributes, and (2) the gender-stereotypicality hypothesis: the “typical cancer patient” is described by more attributes that are compatible with the feminine than with the masculine stereotype. We explored if physician’s demographic and professional variables are associated with their tendency to state more unfavorable and/or more feminine attributes among physicians. The study by Ernst et al. (2016) reported that stigmatizing attitudes were more common in people who had little contact with cancer patients. We were interested in the question whether medical experience (in years) or the number of cancer patients treated would influence the prototype perception.
Methods
Participants and Procedure
The study is part of the Momentum Project Heidelberg on HCP’s attitudes regarding supportive strategies during cancer treatment (registration number NCT02678832). Ethical approval was obtained from the Ethics Commission of the Faculty of Behavioral and Cultural Studies of the University of Heidelberg [AZ Siev 2015/1-1, AZ Siev 2016/1-2].
Eligible participants consisted of general practitioners, urologists, gynecologists, gastroenterologists, surgeons, medical oncologists and radiation oncologists who had regular contact to patients with breast, prostate or colorectal cancer. We focused on attitudes of physicians who are in regular contact to patients with breast, prostate and colorectal cancer, as these cancer types rate among the most prevailing cancer types.
Paper-pencil questionnaires were either sent to physicians’ practices and hospitals that were randomly drawn on basis of compulsory listings or handed out on national medical congresses. The number of contacted practices and hospitals in each federal state of Germany was selected proportionately to its number of inhabitants. In addition, the link to an online version of the questionnaire was distributed via online and print media and newsletters for physicians. Written informed consent was obtained from all participants. Each participant received 25€ as incentive. For more details about the study see (Tsiouris et al., 2018).
Of the 1,865 distributed paper-pencil questionnaires, 8 were returned as undeliverable, resulting in a total of 1,857 distributed questionnaires. The response rate was 19% (358/1,857). With 194 online-participants, a total of N = 552 physicians completed the questionnaire. 33 participants were excluded from further analyses, either because they stated that there are no typical prototype attributes to cancer patients (N = 12), or because of missing values (N = 21), resulting in a total of 519 physicians, who reported at least one prototype attribute.
Measures
Demographic Information
Demographic information in-cluded age, sex, medical specialization and number of years in practice. Professional information included number of treated cancer patients per month, primarily treated tumor types, primarily administered cancer treatment types (e.g., chemotherapy, radiation therapy) and percentage of treated cancer patients being under curative treatment.
Prototype Attributes
Participants were asked to state prototypical attributes regarding the “typical cancer patient” in open text fields. Prior research (e.g., Zimmermann & Sieverding, 2010) has suggested that the prototype approach using open format increases the probability of detecting stereotypes and reduces answers biased by central tendency errors and social desirability.
Participants were presented a modified definition of a prototype taken from Gibbons et al. (1995): ‘The following question concerns your images of people. For example, we all have ideas about what typical movie stars are like or what the typical grandmother is like. We might think of the typical movie star as being pretty or rich and the typical grandmother as sweet and frail. We are not saying that all movie stars or all grandmothers are exactly alike, but rather that many of them share certain characteristics. Then, participants were asked to “Think about the typical person with cancer. Please note 3 typical characteristics that come to your mind’.
Coding Procedure
Based on thematic analysis (Braun & Clarke, 2006), prototype attributes were coded on two dimensions: favorability and gender-stereotypicality. Codings of favorability and gender-stereotypicality were conducted by three independent raters (AT for favorability, AH and research assistant KSC for gender-stereotypicality). Before raters conducted the coding, they received a standardized coding instruction. The coding instruction emphasized the importance to conduct the coding from a general perspective (How favorable/unfavorable/neutral respectively feminine/masculine/gender-neutral is this characteristic perceived in general?). For this purpose, raters were additionally provided a coding system that served as the basis for a consistent coding process (see coding guidelines for favorability and gender-stereotypicality). Fifty percent of all characteristics were coded by two independent raters (research assistants). Interrater agreement was very good with κ = .90 for favorability and κ = .87 for gender-stereotypicality.
Prototype favorability has been proven to be a central component in prototype perception (Gibbons et al., 1995), while gender-stereotypicality has to our knowledge so far not yet been used to characterize prototypical attributes. Both dimensions have been operationalized in coding guidelines. The coding guidelines for both dimensions are based on prior research but were further developed during the coding process. The coding process thus followed a deductive-inductive approach (Kuckartz, 2016). At first, the deductive coding guideline was applied to the data. Prototype attributes that could not be assigned in the first step were used to refine the coding guideline, which represents an inductive procedure.
Coding Guidelines for Favorability and Gender-Stereotypicality
The coding guideline for favorability was based on a compilation of adjective listings taken from the Multiple Affect Adjective Check List (Gotlib & Meyer, 1986) and the General Dimensions Scales for negative and positive affects taken from the PANAS-X (Watson & Clark, 1999). Characteristics were assigned to one of three categories: favorable attributes (equivalent to positive adjectives; e.g., kind), unfavorable attributes (equivalent to negative adjectives; e.g., sad) and attributes that were not clearly assignable as unfavorable or favorable (e.g., thoughtful).
Gender-stereotypicality coding was conducted following the Pancultural Gender Stereotype List (PGSL) by Williams et al. (1999). The list was supplemented by further characteristics of the Bem Sex Role Inventory (Bem, 1974). Prototype attributes were assigned to one of three categories: feminine stereotype (e.g., anxious), masculine stereotype (e.g., aggressive) and gender-neutral attributes that were not clearly assignable to a masculine or feminine stereotype (e.g., higher age).
In order to gain a greater understanding of the gender-related stereotypes relevant for Hypothesis 2, we additionally conducted a comparison of gender-related prototypes mentioned in the present study with gender stereotypes, defined in the PGSL by Williams et al. (1999). For that purpose, we sought out all attributes of the current study that matched the exact wording or meaning of adjectives given in the PGSL. This procedure provided the absolute frequency of characteristics that were congruent to adjectives in the PGSL.
General Favorability and General Gender-Stereotypicality
Two variables were created to quantify physicians’ perceptions regarding a) how many unfavorable attributes and b) how many feminine stereotypes they stated. Thereby, for each participant, the unfavorability-score represents the number of unfavorable prototype attributes divided by number of valid prototype attributes given by the participant. Analogically, the femininity-score was calculated.
Statistical Analysis
Analyses were conducted using IBM SPSS statistics Version 25. Professional and demographic information was analyzed using descriptive statistics. For testing hypothesis 1 and 2, frequencies of favorability and gender-stereotypicality were compared with one-dimensional χ²-analyses; a significant p-value was set at .05.
The unfavorability- and the femininity-scores were used to analyze whether attitudes toward cancer patients were associated with physicians’ experience or sociodemographic characteristics. These scores were correlated with continuous demographic and professional variables of physicians (Spearman’s rank correlation) and group differences (t-tests and analysis of variances, ANOVA) were used to compare categorial variables.
Results
Characteristics of the study participants are presented in Table 1. In brief, the relation between male and female participants was almost balanced with 47.5% female respondents (Table 1), mean age was 45.7 years (± 11.4) and the mean number of years in practice was 17.2 years (± 11.1).
Descriptive Statistics of Physicians’ Demographic and Professional Information (N = 519, if not otherwise stated).

Note. aItem: “Which cancer diseases do you primarily deal with?” Multiple responses possible.
Item: “Which cancer therapies do you primarily deal with?” Multiple responses possible.
Of the 519 participants, 82.3% mentioned three prototype attributes (as asked in the questionnaire); 7.7% mentioned four attributes and the remaining 10% percent mentioned either 1–2 or 5–6 attributes, resulting in a mean of 3.1 prototype attributes per participant. In sum, 1,589 prototype attributes were coded. Figure 1 displays the results of the coding procedure on the dimensions favorability and gender-stereotypicality.
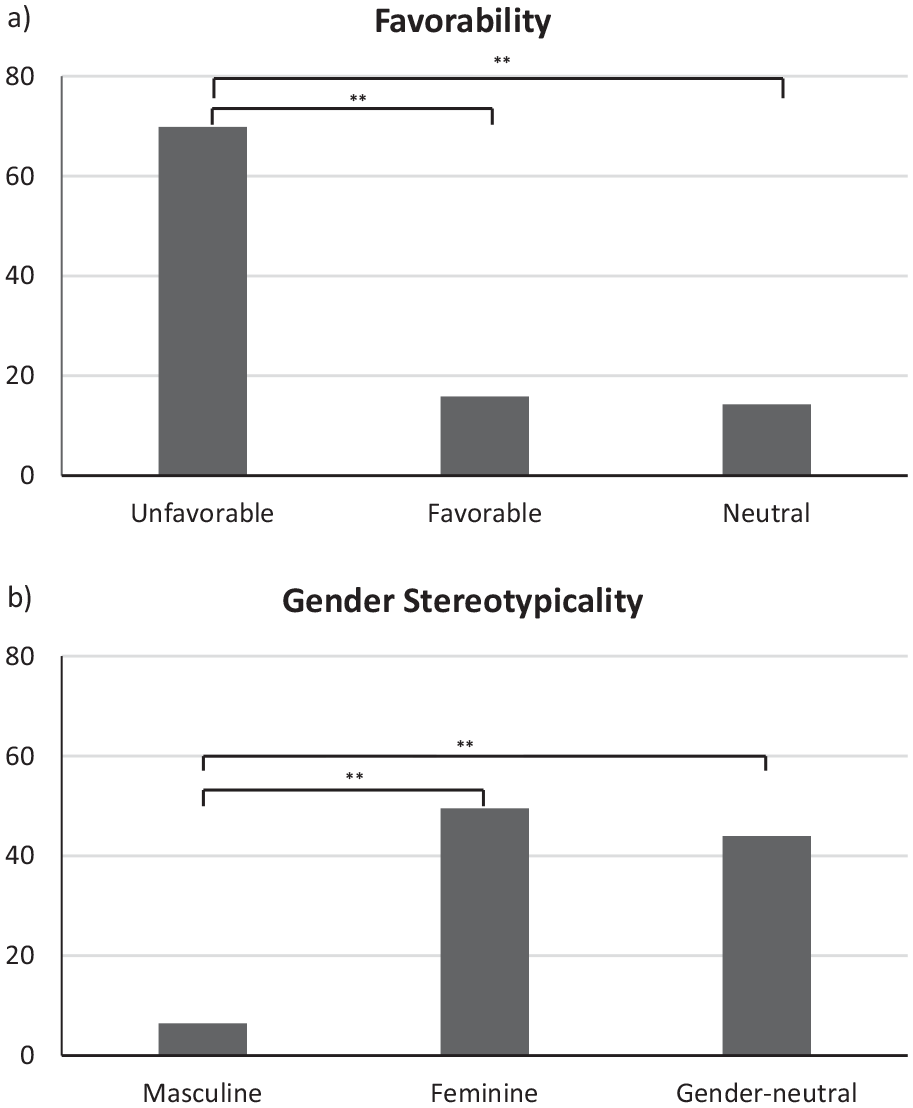
Percentage of attributes (N = 1,589) that were categorized (a) as unfavorable, favorable, or neutral, and (b) as a masculine stereotype, a feminine stereotype, or as gender-neutral.
Most attributes (N = 1,110, 69.9%) were coded as unfavorable. The number of unfavorable, favorable (N = 252, 15.9%), and not assignable (N = 227, 14.3%) prototype attributes differed significantly (χ²(2) = 954.36, p < .001) (Figure 1). Feminine stereotyped attributes made up nearly half of the named attributes (N = 787, 49.5%), and there was a significant difference (χ²(2) = 522.864, p < .001) in the number of masculine (N = 103, 6.5%), feminine and gender-neutral (N = 699, 44.0%) prototype attributes (see Figure 1).
Prototype attributes that were repeatedly stated by physicians include insecure (N = 98), depressed (N = 75), worried (N = 27), sad (N = 22), hopeful (N = 33), grateful (N = 18), battling/fighting (N = 17), and age-related characteristics, for example, higher age, elder (N = 30).
In the next step, the results demonstrated on the dimension gender-stereotypicality in Figure 1 were complemented by further analyses. Table 2 presents a complementing in-depth analysis of gender-stereotypical attributes that match with the gender stereotypes as identified in the PGSL (Williams et al., 1999). Of the 1,589 stated prototype attributes, 342 attributes (21.5%) were identified to match with adjectives of the PGSL. Of those, 324 are feminine gender stereotypes (20.4% of total number of attributes), while the percentage of masculine stereotypes is marginal (1.1% of the total number of attributes). Even though this complementing analysis includes only a fifth of all prototype attributes, the results presented in Table 2 demonstrate that attributes constituting the masculine stereotype are clearly underrepresented in the perception of the typical cancer patient (e.g., strong, self-confident) or even not represented at all (e.g., independent, courageous).
Comparison of Named Attributes with Masculine and Feminine Stereotypes Taken from the Pancultural Gender Stereotypes List (PSGL) by Williams et al. [30] with the Frequency within the Prototype Answers Given by Physicians in the Current Study.

Note. aAnxious and fearful were combined in this table, since both adjectives can be translated with the word ängstlich into the German language.
PGSL = Pancultural Gender Stereotypes List.
Spearman’s rank correlation analyses with metric variables (age, number of years in practice, number of patients treated per month, and percentage of treated cancer patients being under curative treatment) revealed no significant associations with the unfavorability- and the femininity-score. t-tests and ANOVA with categorial variables (sex and medical specialization) revealed no statistically significant differences in the group means. This finding suggests that prototype perception regarding favorability and gender-stereotypicality is not associated with demographic and professional characteristics of physicians.
Discussion
The aim of the study was to explore how physicians perceive the “typical cancer patient,” with a focus on favorability and gender-stereotypicality. The results of this study corroborate the hypotheses that physicians describe the “typical cancer patient” with predominantly unfavorable and feminine attributes, while favorable and masculine attributes remain the exception. The comparison with the PGSL (Williams et al., 1999) highlighted that especially the feminine stereotypes fearful/anxious and weak were frequently mentioned and accounted for the high number of feminine attributes. The tendencies to state unfavorable or feminine attributes were not associated with demographic or professional characteristics of the physicians.
Research on physicians’ perceptions and implicit bias related to cancer patients is scarce (Liang et al., 2019; Sriram et al., 2015). Our results suggest that attributes describing the “typical cancer patient” have primarily unfavorable connotations. The study by Simon et al. (2011) which reported HCP’s perceptions of the prevailing stereotype toward cancer in the public revealed that the general perception of cancer is characterized by negative attitudes. The current study demonstrates that physicians tend to state rather unfavorable characteristics when being asked to describe the “typical cancer patient.”
For several reasons, this perception is plausible, as physicians witness the negative consequences of cancer and cancer treatment on patients’ physical functioning and psychological well-being in their daily work-routine. Prominent attributes mentioned in this study (e.g., anxious and depressed) are in line with emotions expressed by cancer patients, which mainly include anxiety, fear, depression, and anger (Anderson et al., 2008). The results of the current study emphasize that physicians’ perceptions of the “typical cancer patient” correspond to the view which has been identified in studies investigating public attitudes, and feelings often reported by cancer patients themselves.
Regarding gender-stereotypicality of the prototype associations, about half of the attributes associated with the typical cancer patient where gender-neutral, the other half could be assigned to gender stereotypes, but of these, only very few gender-stereotyped attributes were assignable to the masculine stereotype. We identified a much stronger tendency to describe the prototype with feminine (than masculine) stereotyped attributes. As this is the first study investigating the cancer prototype as perceived by physicians with a focus on gender-stereotypical content, the results demonstrate that traditional masculine attributes are significantly underrepresented.
One reason for the dominance of rather feminine attributes could be due to differences in the expression of emotions among men and women when dealing with a serious illness like cancer. For example, it is possible that female cancer patients express more fear and anxiety to their physicians than men do, not because they are more fearful and anxious, but because male patients are less comfortable expressing these emotions in front of the physician 1 . There is some empirical evidence which supports this assumption: In a study of Linden et al. (2012), women with cancer showed higher rates in anxiety and depression than men with cancer. In another study of Seale et al. (2006), female cancer patients were reported as more likely to seek for emotional and social support, whereas male cancer patients were more likely to seek for information. Future research should investigate this interesting hypothesis.
Conceptualizations of Masculinity
The absence of traditional masculine stereotypes in the cancer patient prototype corroborates the assumption that being a cancer patient threatens and might be incompatible with a traditional masculine ideal that is characterized by attributes such as being strong and independent (Bem, 1974; Courtenay, 2000; Williams et al., 1999) and masculine norms of winning, risk-taking and emotional control (Levant et al., 2020). Cancer patients with high adherence to traditional masculine ideals were reported to have higher levels of depression, compared to cancer patients with low adherence (Pudrovska, 2010). For these patients, the image of a “weak and unmanly” cancer patient prototype may represent an additional burden in the adjustment to and acceptance of the disease.
When referring to socially constructed conceptions of masculinity or femininity, it is important to keep in mind that social constructs may be subject to social change (Connell & Messerschmidt, 2005). The definitions of traditional masculinity used here were reported about 20 years ago (Courtenay, 2000; Williams et al., 1999). During this time, the social roles of men and women have changed, which requires potential changes in stereotypes and norms to be taken into account. However, a recent meta-analysis published in April 2020 which analyzed the contents of gender stereotypes from 1946 to 2018 (Eagly et al., 2020) revealed that the stereotype of men being more agentic (e.g., being ambitious, competitive) than women did not change.
The highly cited and often used “Conformity to Masculinity Norms Scale” (Mahalik et al., 2003) was recently refined and shortened using a large heterogenous community sample. The masculine norms remained the same: Winning, Risk-taking, Emotional Control, Self-Reliance, Playboy, Violence, Heterosexual Self-Presentation, Pursuit of Status, Primacy of Work, Power over women, and the study assessed measurement invariance across a broad spectrum of ethnic identities. Approval ratings were highest for the emotional-control norm among white men and men of color followed by pursuit of status norm (Levant et al., 2020).
Limitations and Strengths
There are several limitations to the study that need to be considered. One limiting factor is that the cross-sectional character of the study does not allow drawing conclusions on potential consequences that result from the unfavorable and rather feminine prototype. A subsequent step could be to investigate whether the physicians’ views affect cancer patients’ self-images, according to Levy’s stereotype embodiment theory (Levy, 2009). A further limitation is that this study investigated the prototypical cancer patient as described by physicians in Germany. Attitudes toward cancer and cancer patients may be diverse across cultures and thus it is likely that perceptions of the prototypical cancer patient may vary depending on the cultural context. A cross-cultural examination of the “typical cancer patient” could reveal similarities and differences in the prototype perception compared to German physicians. Finally, the low response rate of 19% is a limitation that restricts the generalizability of the results. The questionnaire, in which the prototype attributes were collected, focused on supportive strategies (like physical activity) as self-management strategies for people with cancer. It can be assumed that mainly physicians who are open-minded toward self-management strategies for cancer patients participated. Reasons for non-participation could not be recorded but could be due to lack of time among physicians and the incentive of 25€ being too low. This assumption is supported by a German study that investigated the reasons for non-participation in empirical studies among general physicians. Besides a generally negative attitude toward participation in studies, lack of time, too much effort and too little compensation were identified as main barriers (Bartsch et al., 2015). The low response rate reported in the current study corresponds to response rates in similar studies with physicians and healthcare providers (Hardcastle et al., 2018; Park et al., 2015).
The study is characterized by several strengths. The large and professionally divers sample enabled to control different demographic and professional factors. The applied prototype approach can be considered a strength. The use of explicit scales, as that is, applied by Ernst et al. (2016), has methodological limitations, as the socially desired answer is often very clearly recognizable. It is not surprising that agreement to stigmatizing attitudes was rather low (Ernst et al., 2016). The strength of the prototype approach, especially the open format approach, is that it can better identify implicit negative attitudes toward certain groups of people compared to social distance scales.
Further research is needed that investigates associations between physicians’ cancer stereotypes and implications for patient-physician interaction and whether prototypical associations might influence cancer patient’s self-concept. In this context, it would be interesting to investigate whether favorable and resource-oriented prototype perceptions held by physicians can have a supportive effect on cancer patients’ mental adjustment to the disease. Moreover, assessing the perception of the prototypical cancer patient from the perspective of cancer patients themselves might be a valuable contribution to the current study. Finally, future research investigating cancer prototype perception in the general population might help explain cancer prevention and screening behavior, since there is first evidence that higher cancer stigma is associated with irregular or non-participation (Vrinten et al., 2019).
Conclusion
In conclusion, this study applying the prototype approach gives insights in how physicians perceive the prototypical cancer patient. Prototype attributes were revealed as predominantly unfavorable. Regarding gender-stereotypicality, more prototype attributes corresponded to feminine than to masculine stereotypes. These results encourage further studies to examine potential consequences of prevailing cancer prototypes on physician-patient interaction, patients’ self-stereotyping and health-seeking behavior, and finally on participation in cancer screenings among healthy adults.
Footnotes
Acknowledgements
We thank Sophie Madlinger, Kim Schouten, and Jasmin Stein for their help in the recruitment and coding procedure.
Authors’ Note
Angeliki Tsiouris has moved to a new institution since completing the research. New affiliation: Department of Psychosomatic Medicine and Psychotherapy, University Medical Center Mainz, Johannes Gutenberg University Mainz, Untere Zahlbacher Straße 8, 55131 Mainz, Germany
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was part of the Momentum Project Heidelberg and was supported by a grant from the German Cancer Aid (Grant No. 110512, 110551 and 111223).