
Abstract
The existing literature identifies parent communication as a protective mechanism in the reduction of sexual risk behaviors among youth; however, not much is known about father–child communication and bonding and its association with HIV testing. Therefore, this study examines the link between the relationship, bonding, and communication shared by African American (AA) fathers and their children and HIV testing over time. This secondary data analysis included data from Waves 1 and 3 of the National Longitudinal Study of Adolescent to Adult Health on the health of adolescents to adults in a sample of AA males and females (N = 509), with a mean age of 16 years. The independent variables included fathers’ communication, bonding, and relationships, and the dependent variables included HIV testing. A multinomial analysis assessed the factors that contributed to or prevented HIV testing. It was found that the overall model was statistically significant; F(24, 55) = 8.95; p < .001. The results suggest that father–adolescent communication was statistically significant and positively associated with HIV testing (B = 23.88; p < .05). AA adolescents who reported going to the doctor or making a nursing visit were more likely to get tested multiple times (B = 13.91; p < .001). Our findings indicate that father–child relationships are essential to adolescent sexual development and serve as a protective factor against threats to sexual health. Future studies should be designed to investigate the cognitive mechanisms through which the father–child bonding and communication may impact HIV testing.
Parent–child sexual communication among youth has been associated with decreased sexual risk behaviors, increased adoption of sexual protective behaviors—including condom use and a reduction in the initiation of sexual intercourse—and decreased risk of HIV and other sexually transmitted infections (Hadley et al., 2009; Harris et al., 2019; Kapungu et al., 2010; Lehr et al., 2005; Nelson, Thach, et al., 2015; Nelson, Wilton, et al., 2015). Most of the studies on parent–child sexual communication conducted among African American (AA) youth has focused on mother–daughter and mother–son sexual communication (Kapungu et al., 2010; Widman et al., 2016), which typically focuses on pregnancy prevention. However, there is a dearth of research examining father–child sexual communication among AA youth (Harris et al., 2019; Randolph et al., 2017), and even less exploring the association between this communication and HIV testing (Boyd et al., 2020).
Given the fact that father–child communication among AA youth has been positively associated with HIV protective behaviors (e.g., condom use), there is a necessity to explore its potential efficacy for HIV prevention among AA youth. In a study on parent–child sexual communication among 162 AA females and male adolescents, the adolescents reported having more conversations with their mothers; however, conversations with their fathers centered sexual topics such as condom use and paternal attitudes toward sex (Kapungu et al., 2010). In a more recent study (2018) of AA father–son sexual communication (N = 96) for ages 16–21 years when it comes to sexual behaviors, father–son communication was negatively related to sons’ permissiveness and positively associated with attitudes toward condoms. In addition, AA sons’ permissiveness positively predicted their sexual behaviors. This is important, despite the limited research, as father–child sexual communication and other relational factors may be important in helping increase the HIV testing uptake of AA adolescents (Harris et al., 2019). The influence of AA father–adolescent sexual communication on HIV prevention uptake constitutes a significant gap in the literature.
We examined the relationship between father–child communication, bonding, and relationships, condom self-efficacy, and other factors among AA adolescents and HIV testing longitudinally. Our study extends the current literature by investigating AA father–adolescent communication and other relational factors as well as the way these factors contribute to HIV prevention uptake (e.g., HIV testing) among a national sample of AA youth over a period time.
Methods
The data for this study were derived from the National Longitudinal Study of Adolescent to Adult Health (Add Health), a nationally representative cohort study based in the United States (Harris et al., 2009). The Add Health data were obtained from a study conducted from 1994–1995 to 2008 in order to survey adolescents and their parents over time with the aid of complex survey weights and clustering. The respondents were recruited during the 1994–1995 school year (Wave 1) when they were in grades 7–12 and were last surveyed in 2016–2018 (Wave 5). A wide range of information was collected from respondents across the four waves to examine the social, emotional, physical, and health aspects. The details of the sample design have been described elsewhere (Harris et al., 2009). The sample was taken from a stratified probability sample of 134 schools in the United States (79% of those sampled). An in-school survey was completed by 90,118 students, and 20,745 students participated in an additional detailed at-home interview (75.6% and 79.5% of eligible students, respectively). During the at-home interview, 85% of the students’ parents were also interviewed (N = 17,760; Harris et al., 2009). Three subsequent follow-up interviews were conducted, including a Wave 4 at-home interview in 2008–2009. For this study, we used data from the home interviews conducted during Waves 1 and 3, comprised of 2344 AA youth (female = 1195; male = 1148) and in the final analytical sample (N = 553); the average age was 16 years for both males and females.
Measures
HIV testing, the dependent variable in this study, was determined based on the participants’ response (Waves 1 and 3). The four-level polytomous response-dependent variable is a measure of HIV testing from two waves of data, where four possible responses were made available to the respondents (1 = Not tested for HIV; 2 = Yes, tested in Wave 1; 3 = Yes, tested in Wave 3; and 4 = Tested in both waves), where they were asked “Have you been tested for HIV/AIDS in the past 12 months?” The following variables—the independent ones—include variables pertaining to AA father–child communication, relationship, and support.
Father–Child Bonding (Wave 1): This two-item scale (1 = Strongly disagree to 5 = Strongly agree) asked the respondents to score the following statements: (1) “Most of the time, your father is warm and loving towards you” and (2) “Overall, you are satisfied with your relationship with your father.” These items were reverse-scored as necessary such that a higher score indicated more of the attributes named in the label. The Cronbach’s α for this scale was .85.
Father–Child Communication (Wave 1): This single-item scale (1 = Strongly disagree to 5 = Strongly agree) asked the respondents to score the statement “You are satisfied with the way your father and you communicate with each other.”
Father–Child Relationships (Wave 1): This single-item scale (1 = Strongly disagree to 5 = Strongly agree) asked the respondents to score the statement “Overall, you are satisfied with your relationship with your mother/father.”
Other independent variables included were:
Condom-Self-Efficacy (Wave 1): This three-item scale (1 = Very unsure to 5 = Very sure) asked the respondents the following: (1) “How sure are you that you could plan ahead to have some form of birth control available?” (2) “If you wanted to use birth control, how sure are you that you could stop yourself and use birth control once you were highly aroused or turned on?” (3) “How sure are you that you could resist sexual intercourse if your partner did not want to use some form of birth control?” These items were reverse-scored as necessary so that a higher score indicated more of the attributes named in the label. The Cronbach’s α for this scale was .72.
Chances of Contracting HIV (Wave 1): This item (1 = Almost no chance to 5 = Almost certain) asked the respondents “Suppose that sometime soon you had sexual intercourse for a whole month, as often as you wanted to, without using any protection. What is the chance that you would get the AIDS virus?”
Health-Care Provider (Wave 3): This item (0 = No and 1 = Yes) asked the respondents “Have you ever gone to see a doctor or nurse because you thought you might have a sexually transmitted disease or HIV?”
Covariates
The following covariates were included: parent education, gender, and age. Parent education and age were included as covariates. Parents indicated their level of education (Wave 1) on a two-item scale (1 = no high school, 2 = high school diploma or GED, 3 = some college or trade, 4 = college degree, 5 = graduate school) when they were asked “How far in school did he/she go?” Age was reported as a continuous variable. Gender was coded as 0 = male, and 1 = female.
Data Analysis
The study consisted of AA males and females (N = 2,344), and the average age was 16 years. First, a descriptive analysis (Table 1) was conducted to separately explore each variable in the dataset. Second, a bivariate regression analysis (Table 2) was performed with the independent variables (father–child bonding, father–child communication, father–child relationship, condom self-efficacy, health-care provider) and control variables (chances of contracting HIV, parent’s education and age) and the dependent variable (HIV testing). Finally, a multinomial logistic regression (Table 3) analysis was used to analyze the independent and control variables and a four-level polytomous response to HIV testing (N = 553). For the multinomial logistic regression analysis, relative risk ratios (RRRs) and 95% confidence intervals (CIs) are presented. All analysis was conducted using STATA 15.
Descriptive Statistics (N = 2,344).

The mean of age and parent education is reported along with SE. SE = standard error.
Bivariate Analysis on HIV Testing (N = 2,344).

Note. *p < .05, **p < .01, ***p < .001. RRR = relative risk ratio; SE = standard error.
Multinomial Analysis on HIV Testing (N = 553).
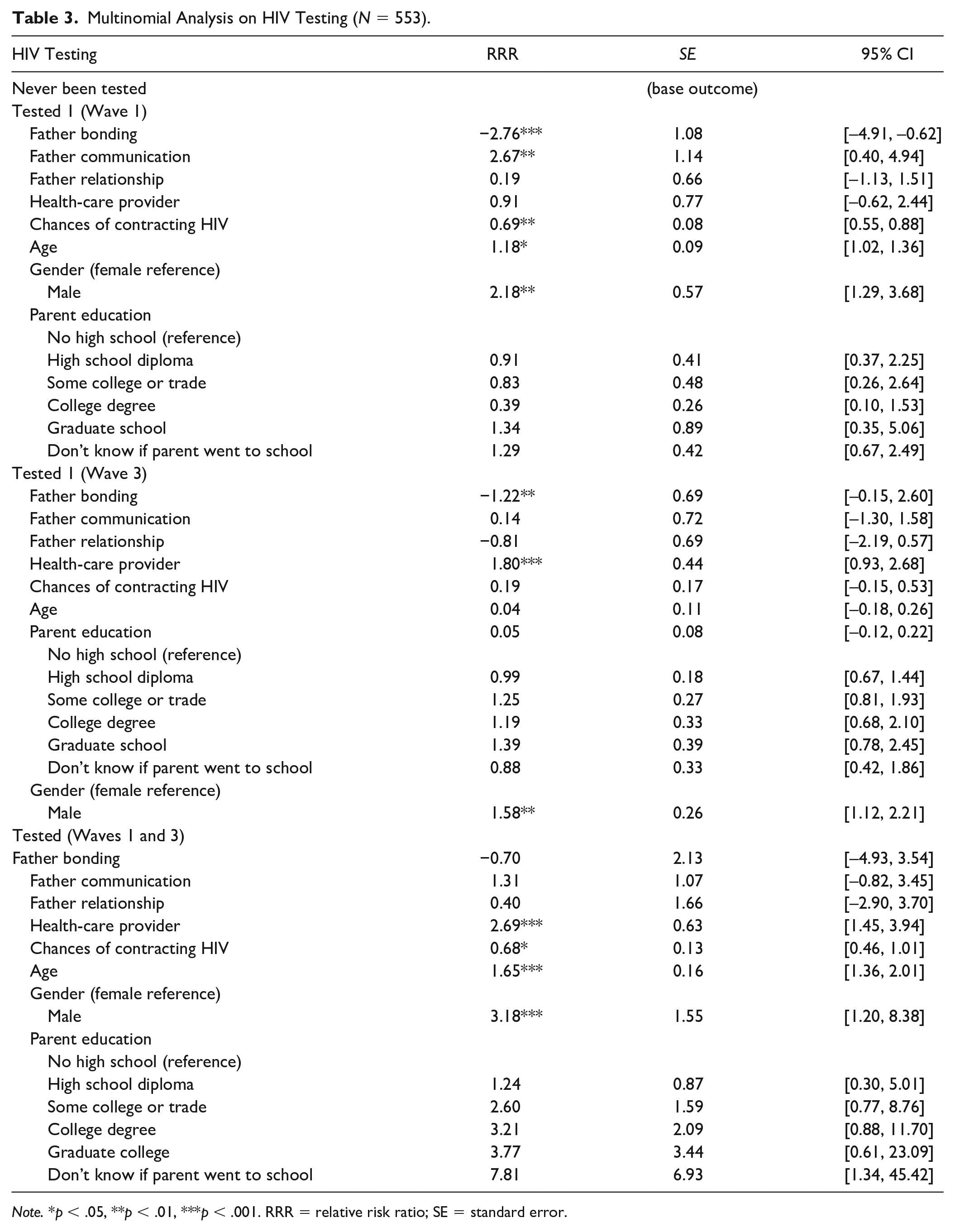
Note. *p < .05, **p < .01, ***p < .001. RRR = relative risk ratio; SE = standard error.
Results
Descriptive Statistics
Table 1 summarizes the descriptive statistics, which includes proportions, means (M), and standard errors (SE). The average age of the individuals in the sample of Wave 1 was 16.18 (SE = 0.19), and the average age of sexual debut was 14.71 (SE = 1.72). Females (N = 1195) comprised 51% and males (N = 1148) 49% of the sample (N = 2344), and most parents had a high school diploma (M = 5.54; SE = 0.15). Seventy-three percent of individuals indicated that they had never been tested for HIV/AIDs, and 2% of individuals indicated that they had been tested multiple times.
Bivariate Regression
Table 2 presents the bivariate regression analysis on HIV testing. AA youth who visited a health-care provider were 2.3 times more likely to get tested multiple times than youth who were never tested for HIV. AA females were two times more likely to get tested for HIV than males at Wave 1 and 1.5 times more likely at Wave 3. Older youth were 1.6 times more likely to get tested for HIV multiple times than younger youth who were never tested for HIV. AA males and females who believed that they had an increased chance of contracting HIV were 1.46 times more likely to get tested for HIV multiple times than those who were never tested for HIV. AA youth having parents with a high a school diploma were 1.34 times more likely to get tested for HIV multiple times than youth who parents did not have a high school diploma.
Multinomial Analysis
Table 3 presents a multinomial logistic regression, and the overall model was statistically significant, F(24, 55) = 8.95; N = 509; p < .001. The results revealed, surprisingly, that father–adolescent bonding was statistically significant and was actually negatively associated with HIV testing (RRR: –2.67; 95% CI [–4.91, –0.62]), indicating that AA adolescents with a decrease in father–child bonding were less likely to be tested for HIV than those who have never been tested. For everyone, as the unit of father–adolescent bonding increased as they got older (18–26), they were 1.22 times less likely to get tested for HIV. AA youth who reported positive father–child communication were 2.67 times more likely to get tested than males who had never been tested for HIV during Wave 1. Individuals who visited a health-care provider because they thought they had a sexually transmitted disease or HIV were almost 1.80 times more likely to get tested at least once than individuals who were never tested for HIV (Wave 1). Older AA youth (18–26) who visited a health-care provider for similar reasons were also 2.69 times more likely to be tested for HIV multiple times (Waves 1 and 3) than those who have never been tested for HIV. Older AA (18–26) youth were 1.18 times more likely to be tested for HIV at Wave 1 and 1.65 times more likely to be tested for HIV in both Waves 1 and 3 than younger youth. Girls were 2.18 times more likely to be tested for HIV than boys at Wave 1, 1.58 times more likely at Wave 3, and 3.18 times more likely to be tested multiple times at Waves 1 and 3. AA males and females who believed they had a decreased chance of contracting HIV were 31% less likely to get tested for HIV at Wave 1 and 32% less likely at Wave 3.
Discussion
This study contributes to and extends the existing literature on parent–adolescent communication and bonding and HIV prevention. The findings of our study support the assertion that the influence of fathers is prominent in modifying HIV-related sexual risk behaviors in AA adolescents. We noted significant associations among fathers, health-care providers, and AA adolescents’ HIV testing behaviors, which was noteworthy since 74% of the sample reported to have never been tested for an HIV infection. AA adolescents who communicated with their fathers reported to being tested for HIV once compared to those who had never been tested. Our results also highlight the importance of early exposure to health care, as AA adolescents in our national sample who visited the doctor were more likely to be tested for HIV multiple times compared to those who had never been tested. In this context, the microsystem (fathers) and macrosystem (health-care provider visits) favorably influence the HIV prevention uptake of AA adolescents.
Our findings also suggest that father–child communication positively predicts HIV testing among AA adolescents during Wave 1. This finding is consistent with prior literature on the importance of parent–adolescent communication that serves as a protective mechanism against sexual risk behaviors and influences HIV uptake (Boyd et al., 2020; Boyd, Quinn, & Waller, 2020; Harris et al., 2018). This is significant due to the fact that it indicates the importance of AA fathers not only in their child’s psychological development but also in their child’s sexual development. Existing literature has also indicated that father–adolescent conversations are more likely to be around condom use and their attitude toward their children’s sexual activity (Bleakley et al., 2018; Harris et al., 2018). Thus, clinicians may want to find ways to develop interventions for fathers in sexual health and HIV prevention uptake in order to ensure the healthy development of their child.
Surprisingly, we identified that AA father-child bonding was negatively associated with HIV testing in Waves 1 and 3. These findings are not consistent with the literature that has documented how adolescents with parents who displayed warmth and caring are less likely to engage in sexual activity that would put them at risk for HIV and other sexually transmitted diseases (STDs) (Coakley et al., 2017; Pengpid, & Peltzer, 2018; Rogers, 2017). This finding might suggest that adolescents have different bonding experiences with their fathers than their mothers. However, this is an opportunity where fathers can learn to become more involved with their children’s sexual health development by attending health-care visits. This is also an opportunity for health-care providers to provide fathers with an education on their child’s sexual health development and the importance of participating in their health care. Finally, researchers and providers can strategically find ways to engage fathers and their children in interventions and prevention programs around sex, sexuality, and HIV, which may lead to fathers being more comfortable in discussing these topics with their children as well as finding new bonding opportunities.
Given that AA adolescents are disproportionately affected by HIV, and as evidenced by our study findings, a great number of them did not undergo testing. Hence, we noted that AA adolescents who visited a health-care provider’s office were nearly 1.80 times more likely to get tested at least once than those who had never been tested. Moreover, AA adolescents were almost three times more likely to be tested more than once if they visited a health-care provider’s office. These findings suggest that early exposure to health care is critical for HIV prevention uptake for AA adolescents into young adulthood and highlight the importance of physicians and the role they play in a routine care. This also sheds light on other structural factors that could influence AA adolescents’ participation in the improvements of their health and well-being. Although AA adolescents experience a higher rate of HIV infection, this is not equally distributed across the population.
Age was statistically and significantly associated with HIV testing, which is consistent with the existing literature. Older AA adolescents were more likely to get tested for HIV than younger youth. This may be due to the fact that older youth are more sexually experienced and have potentially engaged in HIV prevention efforts previously. However, it is important for all sexually active youth, older that 13 of course, to get tested for HIV. Younger youth may be benefit from an HIV education in schools and schools, which can reinforce the importance of sexual health and testing before they start engaging in sexual behaviors.
Our results indicate that females are more likely to get tested for HIV than males in Waves 1 and 3 as well as more likely to get tested for HIV multiple times. This is consistent with current literature that says that females are more likely to get tested than males (Boyd et al., 2018; MacQueen et al., 2015; Moore & Belgrave, 2019). Females may be presented with more opportunities to get tested for HIV over time due to gynecological visits, where HIV testing is done. It is possible that Black males are less likely to get to tested for HIV than females due to the fact that they have negative attitudes toward HIV because of the stigma around the disease. Reducing negative attitudes should be considered a part of HIV prevention and intervention programing, which, in turn, may increase testing among males.
Limitations
The results of our study should be interpreted in consideration of several limitations. First, father–child communication was defined broadly. Questions around communication did not center just sex but were general. Therefore, we do not know if sexual health communication was taking place between fathers and their children. Second, we do not know if the people engaged were biological fathers or a father figure of AA youth in this study. Another limitation is that we are not aware of whether the doctors’ visits were happening in a clinic, provider office, or AIDS serving organization, which may impact whether or not adolescents consistently visited them. Additionally, Add Health data were first collected in 1994–1995, with the most recent data being collected in 2018 (Wave 5) as the adolescents became adults. However, the data are still widely used and relevant till today. Lastly, another limitation is the use of self-reported measures in our study, which may have led to social desirability and recall biases, with potential resultant effects on our estimates. Nonetheless, utilizing the sample weights in the analysis may have contributed to reducing selection bias and variance.
Conclusion and Future Direction
Our current study uniquely focuses on father–child bonding and sexual communication, which is a relatively unexplored area of parent–child relationships, and its role in HIV testing. The finding that AA adolescents with increased father bonding and positive father communication were more likely to test for HIV infection could significantly impact future research efforts. Subsequent studies are required to further explore what constitutes father–child relationships among AA adolescents and identify specific contexts through which these relationships confer a protective advantage and influence the initiation or adoption of sexual health-protective behaviors such as HIV testing. Previous studies have also drawn attention to the need for family-centered care and its role in improving health outcomes. Thus, findings from this study, indicating that AA adolescents’ exposure to health care, in addition to father–child relationships, influences HIV testing, presents an apt intersection point that will benefit from further research on ways father–child relationships drive family-centered care within and beyond clinical settings. With the significant impact of HIV infection on the health and lives of AA adolescents, the results from our current study contribute toward addressing a much-needed knowledge gap in the ways to improve HIV testing and care (Boyd, Lea, & Quinn, 2020; Nelson, Thach, et al. 2015; Nelson, Wilton, et al. 2015; Ogunbajo et al., 2020) and present father–child relationships as a promising area for future targeted interventions (Coakley et al., 2017)
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.