
Abstract
Parent–child sexual communication has been associated with reducing adolescent sexual risk behaviors. Limited research on parent–child sexual communication has been conducted on African American (AA) adolescent males who are at increased risk of sexually transmitted infections (STIs) including HIV/AIDS. The purpose of this research was to examine AA father–son sexual communication and the effect of contextual factors on the sexual risk behaviors. The final sample consisted of 96 AA adolescent males, ages 16–21 years. Structural equation modeling was used to examine the variables of interest (neighborhood characteristics, father–son closeness and connectedness, father–son communication, sexual permissiveness, condom attitudes, sexual risk behaviors). A path model was developed and tested. Results demonstrated that AA father–son closeness and connectedness were related to father–son communication. AA father–son communication was negatively related to sons’ permissiveness and positively related to condom attitudes. Sons’ permissiveness positively predicted their sexual risk behaviors. AA sons’ condom attitudes did not negatively or positively predict their sexual risk behaviors. The findings from this study demonstrate that AA father–son communication is an important factor in decreasing AA adolescent males’ sexual risk behaviors and HIV risk.
AAs represent only 12% of the U.S. population; however, they account for 44% of new HIV infections and 40% of people living with HIV/AIDS (Centers for Disease Control and Prevention [CDC], 2018a; Kaiser Family Foundation, 2017). The rate of new HIV infections per 100,000 AAs is eight times that of Caucasians and twice that of Hispanics (The Kaiser Family Foundation, 2018). In 2015, AAs accounted for 45% of all newly diagnosed infections and 40% of individuals living with HIV (CDC, 2017a). In 2016, approximately 14% of new HIV diagnoses were among heterosexual men, and AA males represented 63% of these men (CDC, 2017b; Middleton & Francis, 2018). Even more significant is that among youth 13–24 years old, AA adolescent males account for 47.3% (4,002 cases) of the 8,451 new HIV infections cases, while their female counterparts account for only 7.4% (626 cases; CDC, 2018b). Recent estimates suggest that 1 in 20 heterosexual AA men and 1 in 2 AA men who have sex with men (MSM) are likely to be infected with HIV at some point during their lifetime (CDC, 2017a). Although researchers suggest that HIV diagnoses have fallen 8% from 2011 to 2015 among AAs, this racial group remains disproportionately affected (CDC, 2018a). Because of this disparity, the National HIV/AIDS Strategy for the United States continues to prioritize the AA population for increased education, prevention, and treatment interventions (The White House, 2015; U.S. Department of Health & Human Services, 2017).
Background
Sexual Risk
Multiple factors place AA males at significant risk for acquiring HIV/AIDS (CDC, 2017a). AA adolescent males are more likely to be sexually active (vaginal, oral, or anal sex) than their peers of other races. Fifty-nine percent of AA male adolescents between the ages of 14 and 18 years have engaged in sexual activity compared to 45% of Hispanic and 40% of Caucasian adolescent males (Kann, McManus, & Harris, 2016). AA adolescent males are also more likely to initiate sex prior to 13 years of age (CDC, 2014; Kann et al., 2016), have multiple sexual partners (Weekes, Haas, & Gosselin, 2014), acquire STIs (Lenoir, Adler, Borzekowski, Tschann, & Ellen, 2006), and are more likely to father a child than other racial groups (Scott, 2012). In addition, multiple factors place AA males at greater risk of acquiring HIV with each act of unprotected intercourse. These include a high prevalence of HIV in the AA community, increased rates of STIs, and AA dating practices of seeking sexual partners within the same racial/ethnic group (CDC, 2017a; Robinson, Swaruup, & Moodie-Mills, 2012).
Contextual Factors and Sexual Risk
Contextual factors, specifically neighborhood contextual factors such as urban setting, high crime rate, and poverty have been linked to sexual risk behavior among AA adolescents (Jones, Salazar, & Crosby, 2017). Neighborhood contextual factors have also been associated with lower health status, including HIV infection (Bowleg & Raj, 2012), and poorer health behaviors and management of HIV infection (Shacham, Lian, Önen, Donovan, & Overton, 2013). Researchers have also reported an association between neighborhood context and sexual risk behavior among urban heterosexual AA men (Bowleg et al., 2014). Less is known about the effect of parental communication as a protective factor. While parental monitoring (being aware of where adolescents are and who they are with) may mitigate some adolescent risk behavior (Jones et al., 2017), monitoring is not equivalent to communication. Research that directly explores parent–adolescent communication and contextual sexual risk is limited (Wilson & Donenberg, 2004).
Additionally, social and structural risk factors, such as incarceration and low educational attainment, may affect AA males’ sexual risk factors. Among AA men born after 2001, one in three is likely to be incarcerated during their lifetime and most men in prison are fathers (The Sentencing Project, 2013). AA children are 7.5 times more likely to have a parent in prison compared to Caucasian children (The Sentencing Project, 2013). When AA fathers are separated from their children due to incarceration, there are reduced and disrupted chances for positive role modeling and mentoring.
Significant disparities in educational attainment continue to persist today. Approximately 18% of AA males have less than a high school diploma and 35% have only obtained a diploma or GED when compared to their Caucasian counterparts (Musu-Gillette et al., 2017). Lower educational attainment is associated with lower employment and income levels (Kena et al., 2015). AA male incarceration rates combined with low educational attainment may play a significant role in AA male parenting abilities and subsequent sexual communication with their sons.
Parenting and Sexual Risk
Researchers have demonstrated that family structure, cohesion, parental monitoring and engagement, as well as parent–child connectedness positively affect adolescent sexual health (Markham et al., 2003, 2010). Miller and colleagues conducted a study to examine whether family process variables (maternal monitoring, communication, sexual communication, and maternal attitudes toward sex) and family structure variables (education, income, and maternal marital status) would predict adolescent sexual activity and sexual risk behaviors among AA adolescents (Miller, Forehand, & Kotchick, 1999). Results indicated that family processes were associated with a reduction in adolescent sexual activity and sexual risk behaviors. Likewise, Huebner and Howell (2003) reported similar results regarding the importance of parental process in reducing adolescent sexual behaviors. Furthermore, a 2016 study of family process among 5,600 AA youth found that AA youth who reported a father figure were less likely to report sexual debut (Langley, 2016). AA youth with a father figure reported greater family rules, maternal warmth, and ability to communicate about sex (Langley, 2016).
Researchers conducted a meta-analysis of 24 studies that spanned 30 years (1984–2014) to examine the effect of parental monitoring on adolescent sexual behaviors. These behaviors included intercourse, condom use, and contraceptive use (Dittus et al., 2015). Higher parental monitoring was associated with delayed vaginal intercourse, decreased vaginal intercourse, and increased contraceptive and condom use. In this study, parental knowledge about adolescent sexual activity (vaginal intercourse) and specific sexual behaviors was associated with a reduction in sex risk behaviors (Dittus et al., 2015). In addition to investigating the connection between parental monitoring and adolescent sexual behavior, researchers have also examined the concepts of connectedness and caring. Adolescents who reported a greater level of connectedness with their parents and reported feeling cared for were more likely to report higher self-esteem and more positive health behaviors, including a reduction in sexual risk behaviors (Ackard, Neumark-Sztainer, Story, & Perry, 2006; Kerpelman, McElwain, Pittman, & Adler-Baeder, 2013).
Parenting process also includes the modeling of values and behaviors, which in turn may shape adolescent norms such as approval of sexual behavior (Donenberg, Wilson, Emerson, & Bryant, 2002; Langley, 2016). Past research had demonstrated that parental permissiveness has been associated with sex risk behaviors in adolescents (Donenberg et al., 2002; Wilson, Weber-Shifrin, & Donenberg, 2000). In a qualitative study of fathers, participants were more likely to report expressing more permissive ideas about sexual activity with sons and were less likely to encourage delaying sex than with daughters (Wilson, Dalberth, & Koo, 2010). In more recent research, sexually permissive attitudes have been associated with greater acceptance of extramarital sexual activity and a greater number of sexual partners, especially among millennials compared with older generations (Twenge, Sherman, & Wells, 2015). These researchers have suggested that attitudes have changed for young adults and may be influencing the attitudes and beliefs of parents who communicate these messages to their children.
Parent–Child Sexual Communication
Parental–child communication is of particular importance during adolescence. Communication provides a vehicle by which parents communicate their attitudes, values, and beliefs about a variety of topics including sex and sexuality to their children (Albert, 2009; Grossman, Jenkins, & Richer, 2018; Ikramullah, Manlove, & Cui, 2009; Ritchwood et al., 2018). Researchers who conducted a recent meta-analysis of 52 studies reported a significant positive association between parent–child sexual communication and adolescent safe sex behavior. These results were found across cross-sectional and longitudinal studies as well as among younger and older adolescents (Widman, Choukas-Bradley, Noar, Nesi, & Garrett, 2016). Conversations that include content about delaying sexual activity, learning to say no to sex, setting rules, and the importance of using contraception have demonstrated a reduction in the initiation of vaginal intercourse among adolescents (Hyde et al., 2013). Among sexually active adolescents, parent–child sexual communication has been shown to increase condom use and reduce sexual risk behaviors (Hutchinson & Montgomery, 2007). In a recent systematic review of parent–adolescent sexual communication, the researcher documented that communication between parents and adolescents about sexual topics and behaviors resulted in greater awareness of the consequences of having sex, greater safe sex efficacy/intentions, and more positive attitudes toward using condoms (Rogers, 2016).
Mother–Daughter Sexual Communication
Much of the parent–child communication literature to date has focused on mother–daughter sexual communication. Explorations of parent–child communication have identified that mothers are more likely to talk to their daughters about sex and fathers more likely to talk with sons (DiIorio, Kelley, Hockenberry-Eaton, 1999; Wilson & Koo, 2010). Overall, mothers are more likely to engage in sexual communication with their children than fathers are (Wyckoff et al., 2007). The content and context of the conversations also differs by race and gender. AA parents are more likely to believe that sexual conversations are the responsibility of mothers and therefore are more likely to have mothers conduct adolescent sex conversations (Kapungu et al., 2010). AA mothers have more numerous conversations about sex with their daughters, and these conversations frequently are focused on pregnancy prevention and abstinence until marriage. This is in contrast to fathers’ conversations with their sons, which center around condom use (Sneed, Somoza, Jones, & Alfaro, 2013). Researchers who conducted a recent meta-analysis of parent–adolescent sexual communication also found differences between mothers and fathers. Although parent–adolescent sexual communication was linked to overall safer sexual behaviors, the effects of the communication were larger when discussions occurred between mothers and adolescents, especially between mothers and daughters (Widman et al., 2016).
Father–Son Sexual Communication
The literature on father–son sexual communication is much more limited. In surveys of adolescents, researchers demonstrated that father–son conversations about sex ranged from reports of never/rarely to occasionally (Raffaelli, Bogenschneider, & Flood, 1998; Sprecher, Harris, & Meyers, 2008). In a 2010 study of parent–child sexual communication among 162 AA male and female adolescents, AA males reported more conversations with their mothers; however, conversations with their fathers were more likely to include discussions about condom use and include paternal attitudes toward adolescent sexual activity (Kapungu et al., 2010). This finding that supports most fathers’ conversations with their sons center around condom use has also been reported by additional researchers (Bleakley, Khurana, Hennessy, & Ellithorpe, 2018; Wilson et al., 2010).
More recently, researchers reported that fathers and sons still differed on how much communication is needed about sexual health behaviors, but that father–son dyads held positive beliefs about attending a sexual risk reduction program (Baker et al., 2018). Certain associated factors have been identified that affect sexual communication. Fathers are more likely to engage in father–son sexual communication if their own fathers had talked to them about sex, if they feel comfortable having a sexual conversation with their sons, if they believe their sons would benefit from the conversation, and if they have more tolerant attitudes toward adolescent sexual activity (Lehr, Demi, DiIorio, & Facteau, 2005). A recent qualitative study of AA fathers’ perspectives on father–son sexual communication supported these findings. Participant fathers were more likely to engage in father–son sexual communication if they were accepting of their roles and responsibilities of fatherhood. Additional factors that were associated with fathers engaging in sexual communication included feeling responsible for sexual education and health, having a positive relationship with their sons, and the perception that they were able to speak openly and honestly with their sons about sex (Randolph, Coakley, Shears, & Thorpe, 2017).
Although the research is limited, parent–child sexual communication and father–son sexual communication may be an important factor in reducing sexual risk among AA adolescent males. The influence of AA father–son sexual communication in sexual risk reduction represents a significant gap within the literature. Therefore, the purpose of this study was to examine the role of AA father–son sexual communication and contextual factors (neighborhood) on the sexual risk behaviors among a sample of AA adolescent males. Specifically, it was hypothesized that AA adolescent males’ background, neighborhood characteristics, father–son closeness and connectedness, father–son sexual communication, sexual permissiveness, condom attitudes, and sexual risk behaviors were related in the following ways: (a) The degree of AA father–son closeness and connectedness will be related to family and neighborhood characteristics; (b) AA father–son closeness and connectedness will predict the amount of father–son sexual communication; (c) AA father–son communication will impact AA sons’ attitudes toward sex and condom use: and (d) AA sons’ sexual and condom attitudes will influence their likelihood of engaging in risky sexual behaviors.
Methods
Procedures
After receiving institutional review board (IRB) approval from Boston College and Yale University, participants were recruited from a large Northeastern city in the United States. Recruitment occurred over 5 months, from April 2015 to August 2015. AA adolescent males between the ages of 16 and 21 years were approached by a community recruiter who explained the purpose of the study to participants. Participants were recruited from neighborhood sports venues, community centers, and through key informants who included AA residents. These key informants were long-time community leaders who worked with AA youth and included church youth ministers, community activists, and outreach workers. Specific inclusion criteria were (a) identified as AA, (b) male, (c) between 16 and 21 years of age, (d) had contact with biological father at least monthly, (e) able to read and speak English, and (f) lived in the specific neighborhoods of recruitment. Parental consent and participant assent were obtained for participants under 18 years old. Parental consent was obtained by the principal investigator (PI) during an in-person meeting with the recruited participant’s parent. Consent was completed in a private area where the survey was being administered. After receiving an explanation of the study purpose and obtaining consent, the participants completed an anonymous Web-based survey via tablet computer. Surveys were completed at neighborhood venues such as libraries, restaurants, parks, and community centers. At each location, privacy was ensured. The survey had 174 questions and took approximately 90 minutes to complete. A total of 100 adolescent AA males completed study measures. As remuneration for their time, all participants who completed the survey measures received a $25 Target® gift certificate.
Measures and Instruments
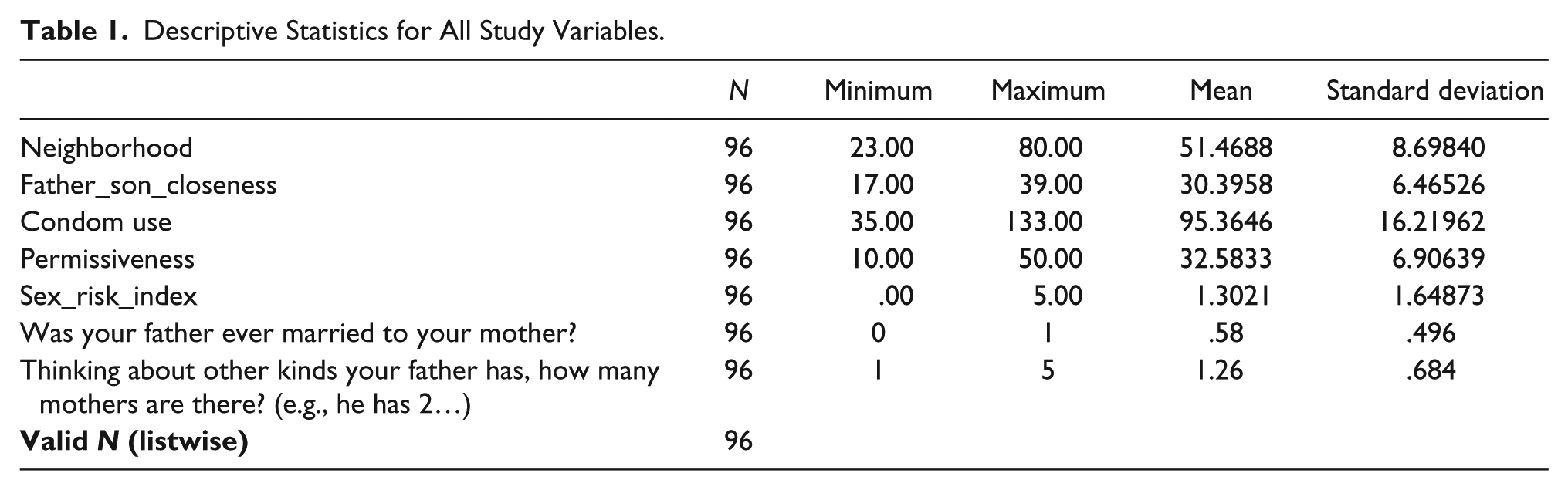
Demographic characteristics included age, education level, employment, income, and relationship status. Remaining survey questions focused on family status, neighborhood characteristics, father–son closeness, father–son communication, sexual risk, and attitudes toward sex and condoms. Descriptive statistics for study variables are located in Table 1.
Descriptive Statistics for All Study Variables.
Family
The relationship between the participants’ mother and father is a factor that may affect the relationship between fathers and sons. This variable was measured by a dichotomous survey question: “Was your father ever married to your mother?” Another variable that may potentially influence the father–son relationship is the number of women that the father has children with, as this indicates among how many different “family units” the father has to distribute his attention. Therefore, another variable indicating the number of women that a participant’s father had children with, including the participant’s mother, was included in the analysis.
Neighborhood
Neighborhood characteristics were measured by 15 items adapted from the Perceived Neighborhood Problems scale and the Perception of Neighborhood Cohesion subscale (Buckner, 1988; Ellaway, Macintyre, & Kearns, 2001). These items asked the participant to describe the extent to which certain issues (e.g., drugs, vandalism) were a problem in their neighborhood, and responses were recorded on a 3-point Likert scale, with 1 representing not a problem in the respondent’s neighborhood to a 3 representing a serious problem. An exploratory factor analysis revealed that all 15 items had at least a moderate (>0.4) loading onto the same factor, so all items were retained. Scale reliability was measured by Cronbach’s α and was sufficiently high (α = 0.889). Participants’ responses to all scale items were summed to produce an overall Neighborhood score, which was used in the remainder of the analysis.
Father–son closeness
Father–son closeness and connectedness was measured using a 13-item scale from Fuligni and Eccles (1993). These items asked the participants to describe how much they enjoyed spending time with their father, how highly they thought of their father, and how much they were praised by their father. Responses were noted on a 3-point Likert scale, with a response of 1 indicating not at all to 3 indicating a lot (Fuligni & Eccles, 1993). An exploratory factor analysis revealed a two-factor solution in which nine items loaded highly onto the first factor (factor loadings > 0.7) and the remaining four items loaded onto a second factor. These four items were all reverse worded. Since the separation of reverse-worded items in factor analysis is a commonly observed phenomenon on otherwise unidimensional scales (Bagozzi, 1993; Bagozzi & Heatherton, 1994; Baumgartner & Steenkamp, 2001; Brown, 2003; Carmines & Zeller, 1979; Marsh, 1992, 1996; Spector, Van Katwyk, Brannick, & Chen, 1997), all items were retained. Scale reliability was measured by Cronbach’s α and was sufficiently high (α = 0.908). Participants’ responses to all scale items were summed to produce an overall Father-Son Closeness and Connectedness score, which was used in the remainder of the analysis.
Father–son sexual communication
Father–son sexual risk communication was measured by eight items from the Parent-Teen Sexual Risk Communication (PTSRC-III) scale (Hutchinson, 2007). Items on the PTSRC-III assessed how much information adolescents received from their father about sexual topics such as contraception, STIs, and waiting to have sex. The PTSRC-III is a 5-point Likert scale, with a response of 1 indicating none and 5 indicating everything. An exploratory factor analysis indicated that all items loaded highly (factor loadings > 0.65) onto the same factor. Scale reliability was measured by Cronbach’s α and was sufficiently high (α = 0.942). Participants’ responses to all scale items were summed to produce an overall Father-Son Sexual Communication score, which was used in the remainder of the analysis.
Sex attitudes
Participants’ attitudes toward sex were measured via the 10-item Sexual Permissiveness subscale taken from the Brief Sexual Attitudes Scale (Hendrick, Hendrick, & Reich, 2006). Participants responded to these items, indicating their attitude toward casual sex, using a 5-point Likert scale from 1 strongly disagree to 5 strongly agree. An exploratory factor analysis revealed that nine items loaded highly onto a single factor (factor loadings > 0.7). The remaining item “I do not have to be committed to a person to have sex with him/her” had a much lower factor loading (0.437). A factor loading of this value is not considered significant for a sample of this size (Hair, Black, Babin, & Anderson, 2010). However, all 10 scale items were ultimately retained in order to maintain the theoretical constructs of the original scale. Scale reliability was measured by Cronbach’s α and was sufficiently high (α = 0.941). Participants’ responses to all scale items were summed to produce an overall Sexual Permissiveness score, which was used in the remainder of the analysis.
Condom attitudes
Participants’ attitude toward condom use was measured by 28 items with five Likert-type response categories ranging from 1 strongly disagree to 5 strongly agree (Brafford & Beck, 1991). An exploratory factor analysis revealed that 21 of the 28 items loaded onto the first factor, while the remaining 7 reverse-worded items loaded onto a second factor. Since this is a fairly common phenomenon among psychological questionnaire items, all 28 items were retained for the subsequent analysis. Scale reliability was measured by Cronbach’s α and was sufficiently high (α = 0.958). Participants’ responses to all scale items were summed to produce an overall Condom Attitudes score, which was used in the remainder of the analysis.
Sexual risk
An index measuring participants’ sexual risk was created by combining information from five survey questions indicating the participants’ overall number of sexual partners in their lifetime, number of sexual partners in the past 30 days, number of sexual encounters in the past 30 days, the percentage of sexual encounters that included a condom in the past 30 days, and the number of women the participant has gotten pregnant. Participants were not assessed for condom use with main or secondary sex partners. All participants were classified as risky (1) or not risky (0) on each of these variables according to the following criteria: number of lifetime sexual partners > 4 (this cutoff was based on the sample mean of 4.63 lifetime sexual partners); number of sexual partners in the past 30 days > 1; number of sexual encounters in the past 30 days > 4; percentage of sexual encounters that included a condom in the past 30 days < 100%; and number of women impregnated > 0. Classifications for all five risk factors were summed to create an index, with total scores ranging from 0 to 5. A score of 0 indicated very low sexual risk and a score of 5 indicated very high sexual risk. All questions were weighted equally. Thirty-eight participants reported that they were not sexually active. These participants were retained in the sample and assigned a value of 0 (very low risk) on the sexual risk index.
Analysis
Four of the participants had missing data on at least one of the variables of interest; therefore, only the remaining 96 participants were included in the dataset for analysis. A sample size of at least 100 is generally recommended for structural equation modeling, with larger samples considered ideal. However, there is no straightforward consensus on minimum sample size for adequate power in structural equation models. Some researchers have reported that path models with single indicators have adequate power with as few as 70 observations, as long as the underlying variables are measured reliably (Wolf, Harrington, Clark, & Miller, 2013). All measures demonstrated high reliability (Cronbach’s α greater than 0.88 in all cases) and acceptable factor loading. The final model was an excellent fit with all indicators included. A sample size of 96 participants with only 4% missing data was determined to be sufficient for analysis using structural equation modeling.
Structural Equation Model
Based on the four research hypotheses, a structural equation model was proposed to capture the relationship between all variables of interest. Structural equation modeling is a useful tool for this analysis because it allows for examination of the direct and indirect relationships among a large set of variables with complex hypothesized relationships. All models were analyzed using LISREL® version 8.8 (Joreskog & Sorbom, 1996).
The initial path model that was developed described the hypothesized relationships between variables, and this model was the starting point for analysis. These relationships were tested by examining the fit of the model to the data. The χ2 statistic was evaluated as an indicator of model fit as it is likely to indicate a good fit when sample size is smaller (Bentler & Bonett, 1980). Several additional indices of model fit were examined. The comparative fit index (CFI) ranges from 0 to 1, where values closer to 1 indicate greater improvement compared to a hypothetical baseline model. The root mean square error of approximation (RMSEA) and standardized root mean residual (SRMR) were also examined. These statistics are based on the residuals and provide an overall indicator of the error present in the hypothesized model. Very small values indicate good model fit. Together, these four indicators provided information about how well the hypothesized model fit the data.
When model fit based on these four indicators was less than ideal, modification indices were examined. Modification indices are provided by LISREL and indicate the change in model fit that would result if the model were changed to include additional explanatory pathways between previously unconnected variables (Joreskog & Sorbom, 1996). Based on modification indices, underlying theory, and evaluation of improvement in model fit based on difference in the χ2 statistics of nested models, additional paths were added to the model where appropriate until the model fit was adequate.
After an iterative process of structural equation modeling, examination of modification indices, and revision of model pathways, a final model was reached. The final model retained all of the original hypothesized structures but added additional direct pathways between father–son closeness and connectedness, sexual risk behaviors, and condom attitudes, and between father–son sexual risk communication and sexual risk behaviors (Figure 1). With 16 degrees of freedom, the model χ2 statistic was nonsignificant (χ2 = 15.261, p = .506), indicating that model fit was not significantly different from perfect fit. The RMSEA (0.0) and SRMR (0.0545) fall below their respective thresholds for good model fit. Finally, the CFI is 1.00, which indicates the model fit is excellent.

Final hypothesized AA father–son sexual communication model with coefficients.
Results
Demographic Characteristics
The final sample included 96 AA males with ages ranging from 16 to 21 years (mean age = 17.95). Almost half of the participants were still attending high school (45%), many others were high school graduates (43%), and a minority had completed some college (12%). The vast majority of the sample (95%) reported that they were unmarried, and 30% reported that they were in a committed relationship. Sixty-two percent of respondents reported that they were sexually active (i.e., engaged in vaginal, oral, and/or anal intercourse), and the mean age at first sexual encounter was 15.74 years (with a range from 12 to 18). The number of lifetime partners ranged from 0 to 75, with an average of 4.63 life partners. Participants most commonly reported one or fewer sexual partners in the past 30 days (83%). Additional demographic information is located in Tables 2 and 3.
Demographics.

Demographics—Sexual Behaviors.

In addition to overall model fit previously described, the size and significance of the model pathways provide information about the relationships between variables. This allowed the hypotheses to be addressed.
Post Hoc Analysis
During analysis, the direct pathway between father–son sexual communication and sexual risk behaviors was also found to be significant and positive (B = 0.074, p < .01). This finding was in direct contrast to the theoretical basis, which is that increased communication between fathers and sons about sexual issues will lead to a decrease in sons’ sexual risk behaviors. After accounting for the indirect impact of sexual communication on sons’ sexual risk behaviors through the negative impact of communication on sexual permissiveness, communication about sex was also positively related to sexual risk behaviors. Because this finding was surprising, a post hoc analysis was done to examine whether different types of father–son sex communication have an impact on sons’ tendency to engage in sexual risk behaviors. Specifically, we sought to explore whether father–son conversations about (a) contraception/protection from STIs and (b) the importance of self-control about sexual matters differed in the strength and/or direction in relationship to sons’ sexual risk behaviors.
To perform the post hoc analysis, father–son sexual risk communication was split into two variables. The first variable (SRC_1) comprised the first five questions of the sex risk communication scale, all of which asked about contraception/prevention of STIs: (a) How much information did he [your father] give you about contraception/preventing pregnancy? (b) How much information did he [your father] give you about STIs? (c) How much information did he [your father] tell you about HIV/AIDS? (d) How much information did he [your father] give you about ways to protect yourself from getting STIs or AIDS? (e) How much did your father tell you about condoms specifically?
The second variable (SRC_2) comprised the last three questions of the sex risk communication scale, all of which asked about waiting and resisting pressure to have sex: (a) How often did he [your father] talk with you about waiting until you were older or not having sex? (b) How much did he [your father] tell you about peer pressure and sexual pressure from dating partners? (c) How much did he [your father] tell you about how to resist pressure from peers and dating partners?
Responses for each set of questions were summed to produce total scores for each scale. Reliability was sufficiently high for each scale individually (α = 0.934 and α = 0.783, respectively). With 19 degrees of freedom, the model χ2 statistic was significant (χ2 = 36.812, p < .01), indicating that model fit was significantly different from perfect fit. The RMSEA was 0.088 and the SRMR was 0.054. These values are slightly larger than ideal but are borderline acceptable. Finally, the CFI was 0.956, which indicates acceptable fit.
Model coefficients can be found alongside their respective paths in Figure 1. Interestingly, neither communication variable predicted either condom attitudes or sex risk behaviors, and only father–son communication about sexual self-control predicted sexual permissiveness (B = −1.509, p < .01). Father–son communication about contraception and STI prevention did not significantly predict sons’ condom attitudes, defying expectation. And neither communication variable had a direct effect on sexual risk behaviors.
Discussion
The purpose of this research was to explore the role of AA father–son sexual communication and contextual factors on the sexual risk behaviors on a sample of AA adolescent males. The current research demonstrated that AA father–son closeness and connectedness was related to AA father–son sexual communication, and this in turn was negatively related to sexual permissiveness and positively related to condom attitudes. Sexual permissiveness of AA adolescent sons was associated with increased sexual risk behaviors. However, AA sons’ condom attitudes were not associated with a decrease in sexual risk behaviors of AA sons. Further exploration of the relationship between AA father–son sexual communication and AA adolescent sons’ sexual risk behaviors identified that AA father–son communication about sexual self-control (i.e., delaying sexual debut, peer and sexual pressure, and resisting sexual pressure) was related to decreasing sexual permissiveness. Additionally, contextual factors of neighborhood organization and parental marital relationship had an impact on sexual communication through father–son closeness between AA fathers and their adolescent sons, and this in turn impacted sons’ sexual risk behaviors.
Consistent with findings from other researchers, the results of this study revealed that AA father–son closeness and connectedness was related to AA father–son sexual communication. Researchers have documented that parents, who as reported by their adolescent children, displayed caring and warmth, were knowledgeable about sexual topics, comfortable with sexual conversations, and communicated their expectations clearly were more likely to have an impact on the sexual decision making of their children (Bleakley et al., 2018; DiIorio, Kelley, & Hockenberry-Eaton, 1999; DiIorio, Pluhar, & Belcher, 2003; Wang et al., 2013). Additionally, parents who demonstrated warmth, love, concern, and caring were more likely to have adolescents who practiced abstinence or reduced the number of sexual partners (Aspy et al., 2007). Furthermore, AA fathers believe that it is their responsibility to communicate with their sons (Randolph et al., 2017; Wilson et al., 2010) and that the quality of the father–son relationship could impact parent–son sexual communication. However, despite the relationship quality, AA fathers understood the importance of educating their sons about sex even if the relationship was strained or inconsistent (Baker et al., 2018).
With regard to the impact of AA father–son sexual communication, it was expected that this communication would have a positive effect on sons’ sexual risk behavior; that AA father–son sexual communication would reduce the sexual risk behaviors of AA adolescent males. Instead, this prediction did not hold true. Results revealed that AA father–son sexual communication impacted AA sons’ sexual risk behaviors through discussions about self-control and may have increased sons’ sexual permissiveness. These results are contrary to those reported by previous researches who reported that parent–child sexual communication was associated with a decrease in sexual activity and sex risk behaviors (DiIorio et al., 1999; Glenn, Demi, & Kimble, 2008; Hutchinson & Montgomery, 2007; Lehr et al., 2005). The reasons for the conflicting results are unclear. The specific details of the conversations between fathers and sons were not explored and therefore no conclusions can be drawn beyond what was measured in this study. Future research that focuses on the content and quality of sexual information relayed from fathers to sons is necessary for more definitive conclusions.
The results from research on the effectiveness of parent–child sexual communication on adolescent sexual risk behaviors are mixed and have evolved over the past four decades. Researchers have reported a range of results, from parent–child sexual communication being more likely to reduce sexual activity among adolescent females, but not among adolescent males (Moore, Peterson, & Furstenberg, 1986), to parent–child sexual communication being associated with increased likelihood for sexual activity among some adolescents (Jaccard, Dittus, & Gordon, 1996; Somers & Paulson, 2000). More recently, a meta-analysis of 52 studies of parent–child sexual communication and adolescent sexual risk behavior found an association between parent–child sexual communication and condom use among adolescent females and a reduction in risk behaviors among both genders overall (Widman et al., 2016).
Parent–child sexual communication has also been linked to specific behaviors. Previously, researchers have documented that among AA participants, parents were less likely to discuss abstinence with adolescent males than with adolescent females (DiIorio et al., 1999). Other researchers discovered that among older adolescents (college students), open and honest sexual communication was associated with delayed sexual debut and increased condom use (Lehr, DiIorio, Dudley, & Lipana, 2000). More recently, parent–child sexual communication among mother–adolescent dyads was associated with a decrease in HIV risk behaviors in the past 90 days and an increase in HIV protective behaviors among the adolescents (Kapungu et al., 2010). Furthermore, in a study of 134 young adult AA adolescent males, researchers found that parent–child closeness and sexual communication was associated with condom use self-efficacy, more consistent condom use, and a decrease in sex risk behaviors (Harris, Sutherland, & Hutchinson, 2013). In contrast, in this study, father–son communication about contraception and STI prevention did not have a significant effect on sons’ condom attitudes.
Results of this study suggested that problematic neighborhood factors had a negative effect on the relationship between AA fathers and sons. Prior studies identified that neighborhood disorganization and disadvantage could have a negative effect on adolescent development (Browning, Soller, & Jackson, 2015; Clarke et al., 2013; Elliott et al., 1996; Wodtke, 2013). Additional researchers reported that adolescents from disadvantaged neighborhoods were more likely to experience caregiver hostility. This association predicted negative sexual outcomes, including early sexual debut and multiple sexual partners in the adolescent (Gardner, Martin, & Brooks-Gunn, 2012). Neighborhoods without disorganization were more likely to support the parent–child relationship and parent–child closeness and communication. Neighborhood connectedness has been identified as an important factor in reducing adolescent initiation of sexual intercourse, reducing pregnancy, and improving contraception use (Oman et al., 2013).
The results of this study indicated that a relationship existed between parental marital dynamic, whether parents were currently or ever married, and AA father–son closeness. Researchers have previously suggested that adolescents whose parents are currently married or were previously married enjoy more warmth, connectedness, and closeness than adolescents whose parents were never married (Brown, 2004; Carlson, 2006; Hofferth & Anderson, 2003). Perhaps the significance of marriage is that fathers who resided with their children can develop a closer, more lasting relationship with their child. This proximity and closeness may translate into improved parent–child communication including conversations about sex and sexuality. More recently, researchers documented that parental marriage had a positive impact on AA adolescent son’s condom use and number of sexual partners (Harris et al., 2013). In this study, participants were not required to live with their father, but they did need to have contact at least monthly. Even with nondaily contact, this relationship had an impact on father–son closeness, which has implications for promoting father–son communication.
The findings of this study suggest that further research is needed in AA father–son sexual communication. Many researchers have documented that AA mothers are the primary communicators of sexual information to their children (Harris, 2016; Hutchinson & Montgomery, 2007; Kapungu et al., 2010). However, AA fathers play an important role in the sexual socialization of their sons. Researchers have demonstrated that fathers are more likely to engage in sexual communication with their sons than with their daughters. This is due to the belief that women are the primary sexual educators of daughters (Coakley et al., 2017; DiIorio et al., 1999; Hutchinson, Jemmott III, Jemmott, Braverman, & Fong, 2003; Hutchinson & Montgomery, 2007; Rogers, 2016). It has been suggested that fathers may be more likely to embrace the role of sexual educator with sons because of their increased comfort with sons as compared to daughters (Wyckoff et al., 2007).
The results of this study have implications for the development of intervention programs and policies that target AA males. Researchers have called for a reframing of the AA fatherhood experience from the negative exposure of absenteeism to positive experiences of relationship building and engagement. This focus on the positive aspects of interactions between fathers and sons can strengthen the father–son relationship (Cooper, 2015). The inclusion of AA fatherhood role models has been an effective strategy for supporting positive parenting practices (Julion, Breitenstein, & Waddell, 2012). Future interventions should include aspects that acknowledge the importance of fatherhood, provide education for both adolescents and fathers, and incorporate effective parenting strategies for AA fathers at all stages of adolescence.
Today, many public policies that relate to father–child relationships are concerned with child support enforcement. Although financial support of children is imperative, fathers’ relationships with their children include more than just monetary support. Public policies must address strategies that support fatherhood engagement, which is associated with improved childhood development and health outcomes (Harris & Metler, 2014). In addition, policies should support fatherhood programs that encourage engagement for both residential and nonresidential fathers as well as programs that offer education, financial assistance, and partner relationship support. Programs with these features have been found to be effective in supporting father–child engagement (Caldwell, Rafferty, Reischl, De Loney, & Brooks, 2010; Cowan, Cowan, Kline Pruett, & Pruett, 2007; Knox, Cowan, Pape Cowan, & Bildner, 2011).
Limitations
There are several limitations to this study, which decrease generalizability. First, this was a study of AA adolescent males who have a relationship and/or contact with their father. The results do not represent adolescents who lack paternal involvement. Recruitment efforts for this population were challenging. Many AA adolescent males who were offered participation reported very limited or no involvement with their fathers. This is consistent with national data that indicates approximately 58% of AA children do not live with their fathers (Vespa, Lewis, & Kreider, 2013) and may have limited or no contact with them. Second, no data were collected from the fathers and the results represent the perspectives of AA adolescent sons only. AA fathers’ perspectives may yield different results. Third, key informants from the community were utilized to recruit participants. Although they had access to community members, the information provided by key informants might be biased or might not fully represent the community at large (McKenna & Main, 2013). Additionally, participants were recruited from inner city neighborhoods in one geographical area in the Northeastern United States. AA males from suburban and rural neighborhoods were not recruited, which further limits the study’s generalizability. Finally, the sample size was relatively small but adequate for structural equation model construction. Due to limited variability in the data, socioeconomic status, age, and education were not controlled for during data analysis.
Despite these limitations, the study had notable strengths. It specifically focused on sexual communication between AA male adolescents and their fathers. This perspective is underrepresented in published literature. This research addressed a significant gap in the evidence on father–son communication about sexual risk behaviors. The results of this study have the potential to provide foundational knowledge in the development of interventions to prevention HIV and STI risk behavior among AA adolescent males.
Conclusion
AA adolescent males face significant sexual health disparities. Although there has been a significant body of research on AA parent–child sexual communication, most of the research has been among samples of AA mothers and daughters. Significantly fewer studies of AA father–son sexual communication have been undertaken. Adolescents report that parents have significant influence on their decision making regarding sexual behaviors (Aspy et al., 2007; Rosengard et al., 2012). Given this knowledge, it is important to continue to support the parent–child relationship and foster sexual communication among AA fathers and their sons.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by a small grant to Dr. A. Harris from the National Institutes of Mental Health and Yale University (1R25MH87217; T. Kershaw, PI), Research Education Institute for Diverse Scholars (REIDS) at the Center for Interdisciplinary Research on AIDS, Yale University.