
Abstract
This panel study explored the effects of male, female, mixed, or idiopathic factor of infertility on the fertility quality of life (FertiQoL) in involuntarily childless males undergoing fertility workup for the first time. A convenience sample of 255 married males (age range = 22–51 years, mean = 30.24 years), 254 (99.6%) of whom suffered from primary infertility were assessed (1) at the baseline, before their initial fertility evaluation (T1); (2) before their second andrological appointment, 2–3 months after diagnostic disclosure (T2); and (3) before subsequent treatment-related/ follow-up appointments (T3, T4). The timing of psychological assessment was strictly related to andrological appointments and routine medical procedures. Respondents completed Emotional, Mind–Body, Relational, and Social subscales of the Polish version of FertiQoL and a baseline demographic survey. The research demonstrated that the FertiQoL scores across the Emotional, Mind–Body, and Relational subscales markedly decreased after the diagnostic disclosure, particularly in the subgroups with male and concurrent male and female factor. Social subscale scores in all subgroups remained stable after the diagnostic disclosure (at T2) but significantly decreased in the follow-up (at T3 and T4). Significant differences in FertiQoL scores associated with respondents’ infertility factor could be demonstrated at each time point. The study identifies the FertiQoL in unintentionally childless males is significantly affected by their factor of infertility and evolves across the pathway of treatment-related/follow-up appointments.
Keywords
Unintended childlessness, which is described by a failure to attain pregnancy following 12 months of regular intercourse without birth control, remains a common public health concern. It affects up to 10%–15% of the population, a large proportion of whom is seeking medical help for the problem (Boivin et al., 2007; Datta et al., 2016). An extensive body of research demonstrated males from couples with an unfulfilled child wish manifest signs of distress due to low self-esteem, frustration, guilty feelings, or complicated grief. Infertility-related distress could be aggravated by a social pressure to become a biological parent. In most cultures biological fatherhood is not only an important social value but also a hallmark of good health status and masculinity (Fisher & Hammarberg, 2012). The failure to achieve societal norms of masculine procreation may stereotypically be viewed as a sign of loss of masculinity. Moreover, the stigma of infertility may lead to social isolation. Additionally, infertility checkup and treatment (e.g., collecting a semen sample for examination, timing of sexual intercourse in relation to ovulation) may negatively affect various aspects of male sexuality. Publications demonstrate unintentionally childless males are likely to experience significant anxiety, mood disturbances, or depression with some studies indicating depression in infertile males is as common as in infertile females (Drosdzol & Skrzypulec, 2009). The risk of depression can be determined by the male’s age, income, cause of infertility, prognosis, duration of infertility, availability of affordable treatments, and perceived social support. The physical and psychological burdens of obtaining the diagnosis and the treatment of unintended childlessness may affect the quality of life of males from couples with an unfulfilled child wish (Bechoua et al., 2016; Gameiro et al., 2012; Hanna & Gough, 2015; Holter et al., 2007; Kumbak et al., 2010; Martins et al., 2016; Pook & Krause, 2005; Schmidt et al., 2012; Warchol-Biedermann, 2019; Wischmann et al., 2009; Wischmann & Thorn, 2013). The term quality of life, defined as one’s perception of their position in life in the context of the culture and value systems in which they live and in relation to their goals, expectations, standards, and concerns, remains an important issue in reproductive medicine and has often been used in the analyses of psychological outcomes of unwanted childlessness (The WHOQOL Group, 1998). In this context, Boivin et al. (2011) argued that the effect of unfulfilled child wish and treatment of unintended childlessness on personal, interpersonal, and social aspects of quality of life was unique. Consequently, Boivin’s team developed the concept of fertility quality of life (FertiQoL) to delineate the specific impact of infertility difficulties on individuals’ overall physical health, emotions, marital relationships/partnership, and family and social interactions. Boivin and co-workers also constructed and validated the FertiQoL questionnaire (www.fertiqol.org) that could be administered to individuals with unintended childlessness regardless of their gender, the etiology of unintended childlessness, or cultural setting (Sexty et al., 2016). The FertiQoL showed good overall psychometric characteristics with various clinical populations (e.g., Aarts et al., 2011; Boivin et al., 2011; Donarelli et al., 2016; Hsu et al., 2013; Melo et al., 2012; Maroufizadeh et al., 2017; Sexty et al., 2018; Volpini et al., 2019). The FertiQoL questionnaire has now been considered a gold standard for measuring outcomes of psychological well-being in individuals and couples with unintended childlessness. Reports using this measure have provided significant contributions to the literature on unwanted childlessness and shed light on predictors of FertiQoL at various stages of infertility diagnostics or treatment. Huppelschoten et al. (2013) analyzed couples undergoing infertility treatment (in vitro fertilization procedure) and demonstrated females had significantly lower scores on FertiQoL total scale and the Emotional, Mind–Body, and Social subscales of QoL than their partners. Zeren et al. (2019) pointed out FertiQoL was associated with the couple’s dyadic adjustment. Madero et al. (2017) and Sexty et al. (2016), in turn, demonstrated that FertiQoL could be determined by gender, ethnicity, or cultural background. Additionally, Namavar Jahromi et al. (2018) examined infertile couples in the course of common fertility treatments and reported that the FertiQoL was associated with respondents’ educational status, duration of infertility, and type of treatment. The author’s preliminary report demonstrated that the disclosure of impaired semen quality does affect male FertiQoL, whereas the degree of semen quality impairment does not (Warchol-Biedermann, in preparation). These investigations added to our knowledge on FertiQoL but most of them used the cross-sectional design and were focused on understanding of respondents’ experiences at a specific time point across the treatment pathway (at the beginning of treatment, when medical procedures were underway or after the cessation of treatment).
There is a dearth of studies that give consideration to the fact that the experience of infertility consists of subsequent stages while infertility events take place on the pathway of diagnosis and treatment-related or follow-up appointments. A couple who intend to have a biological child and have not achieved pregnancy within 1 year of trying usually become suspicious about their inability to conceive and decide to undergo diagnostic assessment. Difficulties conceiving may also be accompanied by sexual dysfunction that puts an additional strain on a couple’s relationship (Lotti & Maggi, 2018; Peterson et al., 2012; Smith et al., 2009; Wincze, 2015). Then after they had undergone the diagnostic testing, they learn the cause of their fertility problems at the reproductive specialist’s office. The couple’s unwanted childlessness can be traced to the male partner (male factor), to the female partner (female factor), to both partners (mixed factor), or the cause of unwanted childlessness cannot be determined (idiopathic/unexplained infertility factor [UFI]). After the workup, partners in a couple pursue the necessary treatment or follow-up visits. Finally, if the standard treatment is unsuccessful, the couple may decide to initiate treatment with the use of assisted reproductive technologies (ART treatment) or pursue other paths to parenthood such as initiating adoption procedures (Fisher & Hammarberg, 2012). The effect of each of these fertility events throughout the treatment trajectory on individual’s FertiQoL has not been clarified yet (Cusatis et al., 2019; Zurlo et al., 2018).
It is important to explain the role of the so-called male (MFI), female (FFI), mixed (Mixed FI), or UFI, which are associated with significant infertility-related distress (Fisher & Hammarberg, 2012; Warchol-Biedermann, 2019; Wischmann & Thorn, 2013). In light of these considerations, the goal of the study was to assess the FertiQoL of males with unwanted childlessness while (1) seeking their initial infertility testing; (2) learning of their role in previous reproductive failure; and (3) during subsequent treatment-related or follow-up testing appointments. In the current study it was hypothesized that the FertiQoL was affected by MFI, FFI, Mixed FI, UFI factors of infertility and would fluctuate across the treatment trajectory.
Materials and Methods
Participants
Two hundred and fifty-five males who sought fertility evaluation for the first time were recruited from a convenience sample of males who decided to be examined at an andrological outpatient clinic in Poznan, Poland.
Recruitment Procedure
Subjects were reached through infertility staff at the reception desk or in the waiting room of the clinic and were asked for participation in the study. Of the 255 baseline respondents, 253 respondents completed the testing twice, 215 respondents completed the testing 3 times, while 185 respondents completed the testing 4 times. One respondent returned an unfinished questionnaire, 4 respondents withdrew from the study, while 65 of them discontinued treatment. Respondents discontinued treatment or participation in the study due to the following reasons: (1) the couple conceived a pregnancy; (2) the couple opted for ART procedure; or (3) poor perceived chance of successful fertility treatment. No statistical differences associated with respondents’ etiology of infertility (male, female, mixed, or unexplained) and subsequent dropout could be observed (p value = .23). Two subjects who initially enrolled were excluded from the sample due to a prior diagnosis of azoospermia. Respondents attended the andrological visit along with their spouses. Two hundred and forty-eight (97.2%) spouses had already undergone fertility examination and knew their fertility status at the baseline. The remaining seven spouses were routinely asked to undergo their evaluation and provide the results of their fertility examination for diagnostic reasons. The data were collected in a way that guaranteed respondent’s anonymity.
Design of the Study
This panel study included the baseline evaluation (T1) and the three subsequent psychological evaluations (T2, T3, T4), which were 2–3 months apart. Respondents were administered the testing when they provided a semen sample for fertility evaluation, on the day before their andrological appointment. The timing of psychological testing was strictly related to andrological visits and to medical procedures, that is, respondents completed the tests (1) before their first fertility testing (T1) at the baseline, before a diagnostic disclosure; (2) before the second andrological visit, 2–3 months after the diagnostic disclosure when their emotional response to the diagnosis stabilized (T2); and (3) before the third and the fourth treatment-related or checkup testing appointments (T3, T4). This strategy was used in order to maintain research participation and to investigate the effect of the course of events related to the diagnostic disclosure and treatment-related/follow-up andrological appointments on FertiQoL of males with unintended childlessness. The respondents did not know their fertility status at the baseline because they obtained the results of their initial fertility evaluation during the first doctor’s visit on the next day. The semen quality analysis was performed using computer-assisted sperm analysis in full accordance with World Health Organization norms and recommendations (Cooper et al., 2010; Talarczyk-Desole et al., 2017).
Measures
Respondents’ FertiQoL was assessed through the Polish version of the Core module of the FertiQoL questionnaire (retrieved from http://sites.cardiff.ac.uk/fertiqol/download/) (Boivin, 2011). The authors of the paper were given a full permission to use the questionnaire in this research study.
The FertiQoL is a fertility-specific questionnaire commonly used to measure psychological function of individuals with fertility issues. The questionnaire focuses on the impact of fertility condition on their emotional status, psychophysical health and well-being, marital relationship/partnership, social relationships and interactions, work life, and plans for the future. The Core module of FertiQoL (FertiQoL_COR) consists of 24 items that are related to 4 domains of FertiQoL (each domain is addressed by 6 items). The emotional domain (the Emotional subscale; FertiQoL_EMO) focuses on emotions due to an unfulfilled wish for a child, and the Mind–Body domain (the Mind–Body subscale; FertiQoL_MB) examines the effect of unwanted childlessness on general and cognitive health. The relational domain (the Relational subscale; FertiQoL_REL), in turn, assesses the effect of infertility on sexual and marital relationship/partnership while the social domain (the Social subscale; FertiQoL_SOC) concentrates on the effect of infertility on social interactions, for example, perceived social support, and inclusion/isolation due to infertility. Respondents answer each item using a five-point Likert scale with higher scores on the FertiQoL scale or any subscale indicating better QoL (Boivin et al., 2011). The demographic information was collected as part of the baseline assessment of study participants, whereas their medical and psychiatric history with the information on their female partner’s reproductive health status was taken during the first andrological visit and updated in the follow-up.
Ethical Approval
Each subject was informed about the purpose and importance of the study, assured of their anonymity and confidentiality and voluntarily gave their verbal consent to participate. Subject’s informed consent was obtained but not recorded to maintain their anonymity. Subjects did not receive any compensation for participation in the study. The investigator also made sure subjects knew they could leave the study at anytime without giving reasons. The ethics approval has been obtained from our university’s Bioethical Committee (Approval No: 920/14).
Statistical Analysis
Respondents’ data were collected using Excel spreadsheets. In order to assess the effect of respondent’s infertility factor and FertiQoL outcomes, respondents were divided into four defined subgroups: respondents with the MFI; respondents with the FFI; respondents with the Mixed FI; and respondents with UFI. Their scores in the Emotional, Mind–Body, Relational, Social, and Core domains of FertiQoL at subsequent stages of the procedure (T1, T2, T3, and T4) were calculated using the Researchers Excel scoring FertiQol online system (http://sites.cardiff.ac.uk/fertiqol/scoring/). The statistical analysis was performed using the appropriate nonparametric Mann–Whitney’s U test. Post hoc power of the test ranged from 68% to 98% depending on the size of the group. Statistical analyses were performed using Statistica 13.1 statistical software package (StatSoft, 2013) and open source G Power software (https://www.psychologie.hhu.de/arbeitsgruppen/allgemeine-psychologie-und-arbeitspsychologie/gpower.html). The results were analyzed with significance level set at <.05.
Results
The Polish version of FertiQoL was pilot tested on 10 healthy native speakers of Polish with background in psychology who were fluent in English. They were asked to provide critical feedback on vocabulary used and clarity of test items to ensure questionnaire’s cross-cultural validity. All participants completed the questionnaire within –5–10 min and reported that all items were easy to understand and adequate in addressing infertility issues. The reliability of the Polish version of FertiQoL was determined using Cronbach’s α. The values of Cronbach’s α are presented in Table 1. Overall, all the FertiQoL scales have good internal consistency with Cronbach’s α values ranging from .83 to .89 (see Table 1 for details).
Reliability Measures for the Four Scales of the Core FertiQoL at Subsequent Assessments (T1, T2, T3, T4).

Note. FertiQoL = fertility quality of life.
Characteristics of the Sample
The baseline sample consisted of 255 married males, who were 22–51 years old with a mean age of 30.24 ± 4.29 years. The subjects had a marriage length of between 1 and 11 years (M = 2.16 ± 1.02) and, with the exception of one subject with a child from a previous relationship, were coping with primary infertility (i.e., 99.6% of them had no previous children). The subjects’ spouses were 21-42 years old with a mean age of 28.42 ± 3.7 years. Respondents reported having been trying to conceive for 8–24 months (M = 14.53 ± 3.17; Me = 14). Detailed sociodemographics are presented in Table 2.
Baseline Demographic Characteristics of Males Participating in the Study.

Note. n = the number of respondents within a given category.
The Analysis of the FertiQoL Outcomes of Males in the Course of Unintended Childless at the Baseline, After the Diagnostic Disclosure, and in the Follow-up (at T1, T2, T3, and T4)
The respondents’ FertiQoL outcomes in Core, Emotional, Mind–Body, Relational, Social, and domains of FertiQoL at subsequent stages of the procedure (M; Me; SD) are presented in Table 3, and in Figures 1a–e.
Respondents’ FertiQoL Outcomes at Subsequent Stages of the Procedure (M, Me, SD).
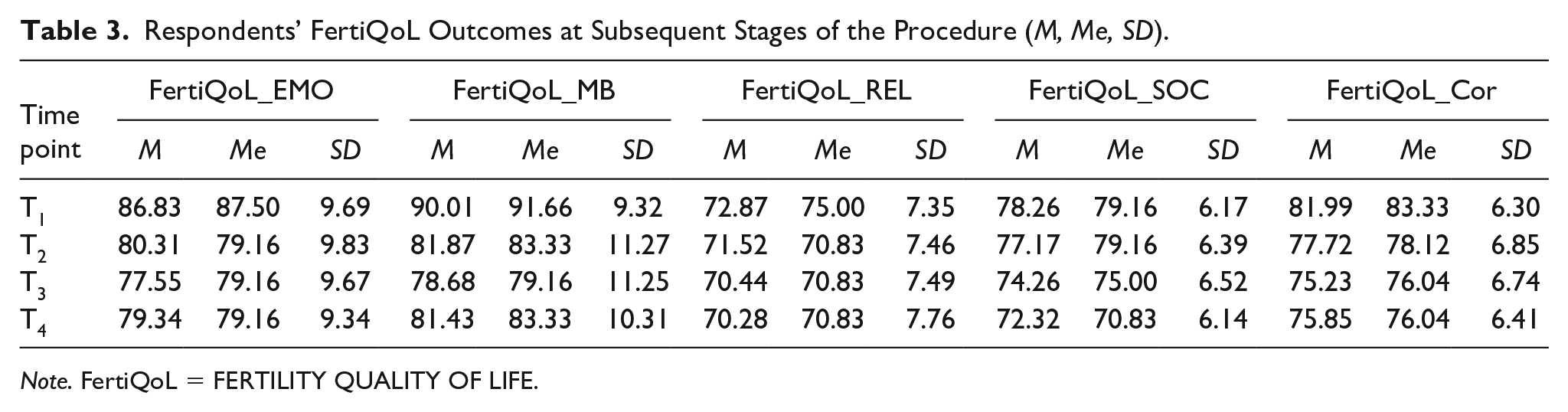
Note. FertiQoL = FERTILITY QUALITY OF LIFE.

(a) Average FertiQoL_Cor scores in the sample at subsequent stages of the procedure. (b) Average FertiQoL_EMO scores in the sample at subsequent stages of the procedure. (c) Average FertiQoL_MB scores in the sample at subsequent stages of the procedure. (d) Average FertiQoL_REL scores in the sample at subsequent stages of the procedure. (e) Average FertiQoL_SOC scores in the sample at subsequent stages of the procedure.
The Core FertiQoL
The Core FertiQoL score in the sample, which averaged at 81.99 ± 6.30 at the baseline (T1), significantly decreased at T2 and at T3 (p values =.000 and =.000, respectively) and then remained stable at T4 (p value =.35) (see Figure 1a for details).
The Emotional Subscale of FertiQoL
The analysis indicated that the average score in the Emotional subscale in the sample, which amounted to 86.83 ± 9.69 at T1, significantly decreased after the diagnostic disclosure (at T2) (p value = .000). The scores significantly decreased again at T3 (p value = .004). Then, no significant changes in the respondents’ scores could be found at T4 (p value = .08) (see Figure 1b for details).
The Mind–Body Subscale of FertiQoL
The mean score in the Mind–Body subscale in the sample, which reached 90.01 ± 9.32 at T1, significantly decreased after the diagnostic disclosure (at T2) (p value = .000) and then decreased again at T3 (p value = .002). Subsequently, a significant increase in the respondents’ scores was observed at T4 (p value = .016) (see Figure 1c for details).
The Relational Subscale of FertiQoL
The mean score in the Relational subscale in the sample, which amounted to 72.87 ± 7.35, at T1, significantly decreased after the diagnostic disclosure, at T2 (p value = .024). Significant changes in respondents’ scores could not be demonstrated at T3 and at T4 (p values = .12 and = .83, respectively) (see Figure 1d for details).
The Social Subscale of FertiQoL
The average score in the Social subscale of FertiQoL in the sample, which amounted to 78.26 ± 6.17 at the baseline, remained stable after the diagnostic disclosure (p value = .08) and significantly decreased at T3 (p value = .000). Subsequently, a marked decrease in respondents’ scores could be observed again at T4 (p value = .004) (see Figure 1e for details).
FertiQoL in Respondent Subgroups Across the Timeline of Treatment-related/Follow-up Andrological Appointments
Table 4 presents FertiQoL outcomes (M; Me; SD) in respondents with MFI, FFI, Mixed FI, and UFI at subsequent stages of the procedure (T1, T2, T3, and T4). The effects of infertility factor on FertiQoL outcomes at subsequent stages of the procedure are demonstrated in Table 5.
FertiQoL Outcomes in Respondent Subgroups (M, Me, SD) at Subsequent Stages of the Procedure (T1, T2, T3, and T4).

Note. FertiQoL = fertility quality of life; FFI = female infertility factor; MFI = male infertility factor; Mixed FI = mixed infertility factor; UFI = unexplained infertility factor.
Changes in FertiQoL Domains in Respondent Subgroups with MFI, FFI, Mixed FI, and UFI at Subsequent Stages of the Procedure.
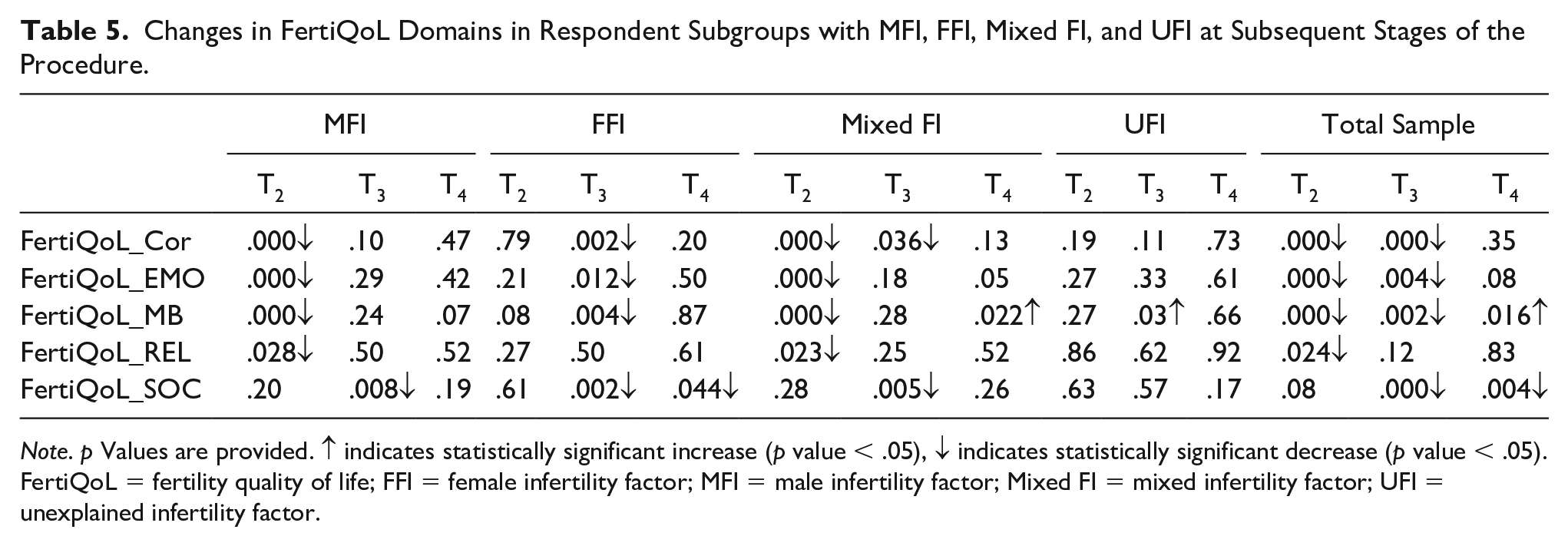
Note. p Values are provided. ↑ indicates statistically significant increase (p value < .05), ↓ indicates statistically significant decrease (p value < .05).
FertiQoL = fertility quality of life; FFI = female infertility factor; MFI = male infertility factor; Mixed FI = mixed infertility factor; UFI = unexplained infertility factor.
The Core FertiQoL Score
The statistical analysis indicated that the average FertiQoL core score in the MFI subgroup, which reached 83.70 ± 6.53 at the baseline, significantly decreased after the diagnostic disclosure (at T2) (p value = .000). The scores in this subgroup remained stable in the follow-up (at T3 and T4) (p values = .10 and = .47, respectively).
The average score in the FFI subgroup amounted to 79.81 ± 6.35, at T1. The score remained stable after the diagnostic disclosure (at T2) (p value = .79), then significantly decreased at T3 (p value = .002) and plateaued at T4 (p value = .20).
The analysis indicated that the average core score in the Mixed FI subgroup, which reached 82.04 ± 5.71 at the baseline (T1), significantly decreased after the diagnostic disclosure (at T2) and at T3 (p values = .000 and = .036, respectively). The scores remained stable at T4 (p value = .13).
The mean score in the UFI subgroup, which amounted to 83.97 ± 4.95, at T1 has not significantly changed after the diagnostic disclosure and in the follow-up (at T3 and T4) (p values = .19, = .11, and = .73, respectively) (see Figure 2a for details).

(a) The association between respondents’ infertility factor and Core FertiQoL scores at subsequent stages of the procedure. (b) The association between respondents’ infertility factor and Emotional FertiQoL scores at subsequent stages of the procedure. (c) The association between respondents’ infertility factor and Mind–Body FertiQoL scores at subsequent stages of the procedure. (d) The association between respondents’ infertility factor and Relational FertiQoL scores at subsequent stages of the procedure. (f) The association between respondents’ infertility factor and Social FertiQoL scores at subsequent stages of the procedure.
The Emotional Subscale of FertiQoL
The analysis of the results of the subgroup with the MFI indicated that their average score in the Emotional subscale of FertiQoL, which reached 88.98 ± 9.82 at the baseline (T1), significantly decreased after the diagnostic disclosure (at T2) (p value = .000). The analysis could not determine any significant statistical changes in respondents’ scores at T3 and at T4 (p values = .29 and = .42, respectively).
The average baseline score in the subgroup with the FFI reached 84.16 ± 10.27. No significant changes in the scores could be observed at the second assessment (at T2) (p value = .21). The scores significantly decreased at T3 (p value = .012) and remained stable at T4 (p value = .50).
The baseline score in the subgroup with the Mixed FI, which averaged at 86.64 ± 8.60, significantly decreased after the diagnostic disclosure (at T2) (p value = .000) but remained stable at T3 and at T4 (p values = .18 and = .05, respectively). The average score in the subgroup with the UFI reached 89.88 ± 8.49 at T1. The analysis could not indicate any significant changes in respondents’ scores at T2, T3, and T4 (p values = .27, = .33 and = .61, respectively) (see Figure 2b for details).
The Mind–Body Subscale of FertiQoL
The analysis of the results in the MFI subgroup indicated that the average score in the Mind–Body subscale in this subgroup, which amounted to 92.59 ± 9.29 at T1, significantly decreased at T2 (p value = .000). No significant changes in respondents’ average scores could be observed at T3 and at T4 (p values = .24 and = .07, respectively).
The mean baseline score in the FFI subgroup, which amounted to 87.07 ± 9.14, remained stable after the diagnostic disclosure (at T2) (p value = .08). The score significantly decreased at T3 (p value = .004) and reached stability at T4 (p value = .87).
The average score in the subgroup with the MFI, which amounted to 89.52 ± 9.00 at the baseline, significantly decreased after the diagnostic disclosure (at T2) (p value = .000). The score remained stable at T3 (p value = .28) and then significantly increased at T4 (p value = .022).
The baseline score in the UFI subgroup, which averaged at 93.65 ± 7.97, remained stable after the diagnostic disclosure (T2) (p value = .27). The score significantly increased at T3 (p value = .03) and then plateaued at T4 (p value = .66) (see Figure 2c for details).
The Relational Subscale of FertiQoL
The analysis demonstrated that the average score in the Relational subscale in MFI respondents, which amounted to 74.01 ± 7.48 at T1, significantly decreased at T2 (p value = .028). No significant changes in the scores could be demonstrated at T3 and at T4 (p values = .50 and = .52, respectively).
The mean score in FFI respondents amounted to 70.20 ± 7.98, at T1. The analysis could not demonstrate any significant changes in the scores at T2, T3, and T4 (p values = .27, = .50, and = .61, respectively).
The average score in Mixed FI respondents, which amounted to 73.98 ± 6.01 at the baseline, significantly decreased after the diagnostic disclosure (at T2) (p value = .023). The scores remained stable at T3 and at T4 (p values = .25 and = .52, respectively).
The average score in the UFI respondents, which reached 74.80 ± 6.65 at T1, remained stable after the diagnostic disclosure (T2) (p value = .86). Subsequently, no significant changes could be found at T3 and T4 (p values = .62 and = .92, respectively) (see Figure 2d for details).
Social Subscale of FertiQoL
The analysis of the results indicated that the average score in the Social subscale of FertiQoL in the MFI subgroup, which amounted to 79.16 ± 6.47 at T1, remained stable after the diagnostic disclosure (at T2) (p value = .20). The scores significantly decreased at T3 (p value = .008) but the analysis could not determine any significant changes in the scores at T4 (p value = .19).
The mean score in the FFI subgroup, which amounted to 77.81 ± 6.14, at T1 has not significantly changed after the diagnostic disclosure (p value = .61). The scores significantly decreased at T3 (p value = .002) and then decreased again at T4 (p value = .044).
The average score in the subgroup with the MFI, which amounted to 77.99 ± 6.03 at the baseline, remained stable after the diagnostic disclosure (p value = .28) and then significantly decreased at T3 (p value = .005). The score remained stable at T4 (p value = .26).
The average Social subscale score in the UFI subgroup reached 77.57 ± 5.66 at the baseline (T1). The score remained stable after the diagnostic disclosure (T2) (p value = .63) and in the follow-up (at T3 and T4) (p values = .57 and = .17, respectively) (see Figure 2e for details).
The Association Between Respondents’ Factor of Unwanted Childlessness and Their FertiQoL Across the Timeline of Treatment-related/Follow-up Andrological Appointments.
Differences in FertiQoL outcomes between respondent subgroups with MFI, FFI, Mixed FI, and UFI in the course of unintended childlessness (at T1, T2, T3, and T4) are presented in Table 6.
The Association Between Infertility Factor and FertiQoL Outcomes in Males in the Course of Unintended Childlessness at the Baseline, Following Diagnostic Disclosure and in the Follow-up (T1, T2, T3, T4).

Note. FertiQoL = fertility quality of life; FFI = female infertility factor; MFI = male infertility factor; Mixed FI = mixed infertility factor; UFI = unexplained infertility factor.
Core FertiQoL
The analysis of respondents’ average scores at the baseline indicated statistically significant differences between the following subgroups: MFI and FFI respondents (p value = .000); MFI and Mixed FI respondents (p value = .033); FFI and Mixed FI respondents (p value = .030); and between respondents with FFI and UFI (p value = .005). Then, at T2, significant differences were found between the following subgroups: MFI and UFI respondents (p value = .002); FFI and Mixed FI respondents (p value = .029); FFI and UFI respondents (p value = .016); and between respondents with the mixed and with the UFI (p value = .000). The analysis of the results at T3 demonstrated that respondents with the male, the female, and the mixed factors significantly differed in the core FertiQoL from subjects with the unexplained factor of infertility (p values = .008, = .000, and = .000, respectively). Then at T4 significant differences were found between FFI and UFI respondents (p value = .004) and between Mixed FI and UFI respondents (p value = .003).
Emotional Domain
The statistical analysis of respondents’ baseline results in the Emotional subscale demonstrated significant differences between MFI and FFI respondents (p value = .002) and between FFI and UFI subjects (p value = .022). However, at the second assessment (T2), when respondents already knew their diagnosis, statistical differences in the average scores could be found between the following subgroups: MFI and FFI respondents (p value = .044); MFI and UFI subjects (p value = .000); FFI respondents and subjects with Mixed FI (p value = .012); and subjects with the mixed factor and UFI respondents (p value = .000). Then, at the third assessment (T3), statistically significant differences were found between the following subgroups: MFI and UFI respondents (p value = .004); FFI and UFI respondents (p value = .006); and between subjects with the mixed FI and UFI respondents (p value = .000) (Mann–Whitney test, the results are significant at p < .05).
Mind–Body Domain
The analysis of respondents’ results in the Mind–Body scale of the FertiQoL at T1 demonstrated statistically significant differences between the following subgroups: MFI and FFI respondents (p value = .000); MFI and Mixed FI respondents (p value = .006); FFI and UFI respondents (p value = .001); and between Mixed FI and UFI respondents (p value = .033).
Then, at the second assessment (T2), statistical differences could be found between the following subgroups: MFI and FFI respondents (p value = .036); MFI and UFI subjects (p value = .000); FFI respondents and subjects with the Mixed FI (p value = .001); FFI subjects and UFI respondents (p value = .000); and between Mixed FI and UFI subjects (p value = .000). The analysis of the scores at T3 indicated statistically significant differences between the following subgroups: MFI and UFI respondents (p value = .001); FFI and UFI respondents (p value = .001); and between Mixed FI and UFI respondents (p value = .000).
Then, at T4, statistical differences could be found between the following subgroups: MFI and UFI respondents (p value = .026); FFI and UFI subjects (p value = .000); and between Mixed FI respondents and subjects with the unexplained factor (p value = .001).
Relational Domain
The analysis of respondents’ T1 results in the Relational subscale of the FertiQoL demonstrated statistically significant differences between the following subgroups: MFI and FFI respondents (p value = .001); FFI and Mixed FI respondents (p value = .003); and FFI and UFI respondents (p value = .017) (Mann–Whitney test, the results are significant at p value <.05). Then, at the fourth assessment (T4), statistical differences could be found between FFI respondents and respondents with the unexplained factor (p value = .035).
Social Domain
No significant differences could be observed at any time point (p values ≥ 0.05) (Mann–Whitney test, the results are significant at p value <.05).
Discussion
There are several reports documenting that the experience of the diagnostic process and medical treatment for infertility may affect emotional status, psychosomatic well-being, quality of marital relationship/partnership, and social relations of individuals with an unfulfilled wish for a child. At present, most studies on the impact of fertility workup and treatment on individuals’ quality of life rely on cross-sectional data collected at a single time point across the course of infertility (e.g., Chachamovich et al., 2010; Keramat et al., 2014; Li et al., 2019; Sexty et al, 2018; Zurlo et al, 2019). These studies improve our understanding of psychosocial effects of unintended childlessness but their nature only allows for insight into a single psychological assessment (Greil, 1997; Henning et al., 2002). With an accumulating body of evidence, there has been increased attention to the variability in FertiQoL over the course of unintended childlessness (e.g., Agostini et al., 2017; Neumann et al., 2018; Wu et al., 2020). In the current investigation a panel study design was used to examine variations in FertiQoL in males with unwanted childlessness who were followed from the baseline (before their first round of testing and the diagnostic disclosure; T1) across the timeline of infertility-related events (diagnostic disclosure and treatment-related/follow-up visits; T2, T3, T4). The study also analyzed whether FertiQoL in the sample differed by infertility diagnosis (identification of MFI, FFI, Mixed FI, or UFI). The sample of respondents underwent psychological testing at four time points (T1, T2, T3, and T4) on the day before their andrological appointment so psychological testing was strictly timed with their andrological visits. Due to the time gap between andrological appointment and the subsequent testing, the confounding effect of a momentary condition could be reduced.
The analysis demonstrated that respondents’ mean FertiQoL scores in Emotional, Mind–Body, and Relational domains reached maximum values at the baseline before the fertility workup and then dropped after the diagnostic disclosure (at T2). In this respect, the decrease was statistically significant in individuals with MFI and combined MFI and FFI. These outcomes demonstrate that the impact of diagnostic disclosure on respondents’ emotional status, psychophysical well-being, and marital relationship was particularly significant if the reproductive failure was caused by isolated male or combined male and female etiology adversely affected. A negative impact of MFI could be seen in several studies. For instance, Smith’s team (2009) observed an increased negative sexual and personal impact associated with isolated MFI while Asazawa et al. (2019) demonstrated that the diagnosis of male factor etiology predicted lower FertiQoL in unintentionally childless males. Similarly, the Osadchiy, Mills and Eleswarapu’s (2020) qualitative study of online forums for males with an unfulfilled wish for a child suggested that male factor of unintended childlessness can affect a man’s sense of masculinity and self-worth. The author of the current paper observed that the association between semen quality and various domains of FertiQoL was often statistically insignificant suggesting that the disclosure of MFI may be more important than learning about one’s poor semen quality (Warchol-Biedermann, in preparation).
In contrast, the analysis of results in the social domain of FertiQoL demonstrated that respondents’ scores, which also peaked at T1, remained stable after the diagnostic disclosure and then significantly dropped in the follow-up (at T3). These data suggest that continuous infertility treatment could be associated with a marked decrease in patients’ social functioning (lowered perceived social support, increasing feelings of social isolation and/or inability to meet social expectations related to conceiving a child). These outcomes corroborate previous findings on gender differences in the experience of infertility-related support. Studies carried out in various cultural or ethnic settings demonstrate that males may find it difficult to disclose the diagnosis (e.g., negative outcomes of infertility testing or unsuccessful treatments) and display their emotions (e.g., shame, guilty feelings) to their partners or wives. They are also reluctant to share their feelings or concerns with the natural support networks in the family or at work (e.g., parents or -in laws, co-workers). Moreover, males from couples with unintended infertility are even unwilling to openly discuss their health status or infertility issues with their fertility doctor or other medical staff. Papers suggest these obstacles to good communication exchange may stem from stereotypical vision of masculinity, perceived societal attitudes, the perceived stigma of male infertility (e.g., the traditional link between masculinity and the ability to conceive), and the adherence to masculine restrictive emotionality norms (e.g., the value of suppressing one’s emotions and supporting others instead of being supported). Some publications report males differ from females in their coping style preferences (males seek instrumental support while females are more likely to ask for emotional support). Males may find it easier to connect with their peers using social media support networks or online discussion boards. Consequently, they are more likely to benefit from online social support networks (Arya & Dibb, 2016; McCray et al., 2020; Miner et al., 2019; Nagórska et al., 2019; Richard et al., 2017). Nagórska and the team reported that males from infertile couples who participated in their study were reluctant to openly discuss their infertility problems with friends, colleagues, or even medical staff and thus were less likely to benefit from social support networks than their female partners. In this context, it is also worth mentioning that the analyzed sample of respondents was simultaneously screened for clinically significant distress (at T1, T2, T3, and T4). As could be observed, the risk of clinically significant distress in the sample markedly increased after the diagnostic disclosure (at T2) and dropped in the follow-up (at T3). The risk of clinically significant distress in the sample was inversely associated with the mean scores in the social subscale of FertiQoL (the results were published in Warchol-Biedermann, 2019). These findings suggest that continued infertility treatment could be associated with lowered perceived social support but with less distress. Similar findings were reported by Casu’s team (2019) who investigated couples starting their first ART cycle. Casu’s team demonstrated that greater levels of support from social network were directly associated with higher individual stress in male participants of their study. The investigation of the results at the baseline and in the follow-up also demonstrated respondents with UFI were characterized by significantly higher scores in the Emotional, Mind–Body, and Relational domains than those with other diagnoses. These results may suggest that respondents with UFI remain optimistic about their prospects of pregnancy because the cause for their unintentional childlessness is not obvious. Our outcomes are partially discordant with the results of the study by Santoro et al. (2016). Santoro and co-workers indicated differences in FertiQoL associated with the perceived diagnosis but male UFI participants of Santoro’s study were characterized by lower FertiQoL scores compared with FFI respondents whose partners had polycystic ovary syndrome.
The outcomes of the present study clearly demonstrate infertility factor may determine FertiQol of males with unintended childlessness. One may also note the varied effect of infertility factor on Emotional, Mind–Body, Relational, and Social domains of FertiQoL. This observation indicates that support programs for males with an unfulfilled wish for a child should be individualized and tailored to the support needs of individuals with various infertility factors. These support programs should also adequately consider the fact that patients’ needs for support fluctuate across the timeline of treatment-related/follow-up andrological appointments.
The findings of this study have to be seen in light of some limitations. First, the sample respondents were treated at a single medical setting and covered the costs of andrological procedures at the clinic themselves. Secondly, the investigation analyzed the role of the etiology of infertility on FertiQoL. In fact, respondents’ FertiQoL outcomes could have been determined by other variables that have not been considered in the study such as respondents’ cultural setting or religious background. However, the longitudinal design of the study adds to our knowledge on variability in FertiQoL over the course of unintended childlessness and could be used by physicians, nurses, midwives, and other professionals working with males with unintended childlessness.
Footnotes
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.