
Abstract
This panel study aimed to explore the effects of male, female, mixed or idiopathic factor of infertility on the course of clinical distress and possible psychiatric morbidity in involuntarily childless males undergoing fertility evaluation for the first time. A sample of 255 males completed the General Health Questionnaire-28 (GHQ-28) (a) at the baseline, before their initial fertility evaluation (T1); (b) before their second andrological appointment 2–3 months after diagnostic disclosure (T2); and (c) before subsequent treatment-related/follow-up appointments (T3, T4) to be screened for clinically significant distress and risk for psychiatric morbidity. Then they were dichotomized as non-cases and cases. The timing of psychological testing was strictly related to andrological appointments and medical procedures. The research demonstrated that the baseline prevalence of clinical distress and psychiatric morbidity in all the subgroups was similar to reference values, but then significantly surged after the diagnostic disclosure, particularly in male and mixed factor respondents. However, the percentage of clinically distressed mixed or idiopathic factor of infertility respondents remained stable after diagnostic disclosure and during the entire follow-up. The prevalence of clinically significant distress and risk for psychiatric morbidity in the male factor of infertility, female factor of infertility, and mixed factor subgroups decreased during the follow-up but remained higher than at the baseline. The study identifies that the course of distress and risk of psychiatric morbidity of males is significantly affected by their factor of infertility and changes across the pathway of treatment-related/follow-up appointments.
It is estimated that 10%–20% of all couples experience difficulties conceiving (Agarwal, Mulgund, Hamada, & Chyatte, 2015; Boivin, Bunting, Collins, & Nygren, 2007). Studies have reported that unwanted childlessness affects psychological status and well-being of couples who are unable to achieve pregnancy. Investigations also indicated that males and females experiencing unintended childlessness differ in their attitudes or psychological reactions to their fertility problems (Cui, 2010; Culley, Hudson, & Lohan, 2013; Dooley, Dineen, Sarma, & Nolan, 2014; Dooley, Norman, & Sarma, 2011; National Institute for Health and Clinical Excellence, 2013; Schaller, Griesinger, & Banz-Jansen, 2016; Schick, Rösner, Toth, Strowitzki, & Wischmann, 2016; Wischmann & Thorn, 2013). The research on the influence of involuntary childlessness or infertility treatment on men’s psychological health is limited, but studies indicate infertile males may manifest symptoms of elevated distress, anxiety, and depression (Fisher & Hammarberg, 2012; Holley et al., 2015; Yang et al., 2017).
The studies so far have not sufficiently considered the fact that patients’ experiences take place on a timeline of events, when patients face life circumstances, which may notably affect their psychological distress or their risk of developing symptoms of depression. In this context, it is noteworthy that a couple is usually referred for infertility evaluation after they have unsuccessfully tried to conceive for a year (National Institute for Health and Clinical Excellence, 2013). As time goes by, both partners grow increasingly concerned about their inability to conceive, so they come to a decision to undergo fertility testing. The results of the testing usually identify the partner who is responsible for the reproductive failure so far, that is, the couple’s inability to achieve pregnancy can be attributed to the male partner (male factor), to the female partner (female factor), or to both partners (mixed factor), or the causes of unwanted childlessness remain unexplained (idiopathic/unexplained infertility factor). Studies indicate the diagnosis of infertility can affect the couple’s relationship. Both partners may experience decreased sexual satisfaction, lower self-esteem, and increased anxiety (Peterson et al., 2012). However, the outcomes of the fertility workup may be particularly burdensome to the partner with poor results of testing (Fisher & Hammarberg, 2012; Wischmann & Thorn, 2013). Diagnostic testing is followed by necessary treatment for individuals who need it or follow-up visits for the healthy ones. The final stage is often marked by the couple’s decision to start adoption procedures or to undergo assisted reproductive technology (ART) treatment (Fisher & Hammarberg, 2012). Considering the sequence of events related to the diagnosis and treatment, one may suppose that the research on the influence of unwanted childlessness on distress and mental health status of males (a) while seeking initial infertility testing; (b) while learning of their role in previous reproductive failure; and (c) during subsequent treatment-related or checkup testing appointments may expand the knowledge on the impact of unintended childlessness on male psychological distress and risk of psychiatric morbidity. In this respect, it would be valuable to investigate the role of the so-called male, female, mixed, or idiopathic infertility factors, which not only cause failure to conceive but may also stigmatize the spouses (Fisher & Hammarberg, 2012; Wischmann & Thorn, 2013).
The impact of the sequence of events related to infertility testing, obtaining the diagnosis, and necessary treatment on distress reactions and prevalence of mental health symptoms such as depression in males from infertile couples remains an underresearched area, which should be clarified for several reasons. Male factor of unwanted childlessness is involved in up to half of all infertility cases, so males are often treated for infertility (Brugh & Lipshultz, 2004). Psychological distress may indirectly influence the results of infertility therapy by exerting negative effects on semen quality via action on the neuroendocrine system (Hanna & Gough, 2015; Nordkap et al., 2016). Increased psychological strain and compromised well-being may affect patient adherence to medical regimes and may cause discontinuation of infertility treatment despite a favorable prognosis and ability to cover the costs of treatment (Gameiro, Boivin, Peronace, & Verhaak, 2012). Infertility specialists and other health-care providers involved in diagnostic procedures or treatment of unwanted childlessness should understand how an unfulfilled wish for a child affects male mental health status to prevent or counteract its negative effects. Assessment of male psychological reaction to infertility diagnosis and treatment and its determinants is essential for preparation of accurate prevention and support programs (Frederiksen, et al., 2015; Schmidt, Sobotka, Bentzen, Nyboe Andersen, & ESHRE Reproduction and Society Task Force, 2012; Wischmann, Scherg, Strowitzki, & Verres, 2009).
The goal of this study was to assess the level of distress and the risk of stress-related psychiatric disorders such as depression in males with unwanted childlessness who sought the help of a fertility doctor for the first time. In the current study it was hypothesized that the distress and risk of common mental health disorders would increase after the diagnostic disclosure and then decrease during the follow-up.
Male distress and risk of psychiatric morbidity were suspected to be affected by male, female, mixed, or idiopathic factors of infertility.
Materials and Methods
Participants
Two hundred and fifty-five males without a history of previous or present physical (cardiac or other) disease and psychiatric treatment who sought fertility evaluation for the first time were recruited from a convenience sample of males who decided to be examined at an andrological outpatient clinic in Poznan, Poland.
Participant Recruitment
Subjects were approached by infertility staff at the reception desk or in the waiting room of the clinic. Of the 255 respondents who initially enrolled, some individuals were lost during follow-up, that is, they completed the questionnaires less than four times. One respondent returned an incomplete questionnaire, four respondents withdrew from the study, and 65 of them withdrew from treatment. Respondents withdrew from treatment and from the study because (a) respondent’s spouse became pregnant; (b) the couple decided to start ART procedure; or (c) they believed their chance of successful fertility treatment success was poor. The statistical analysis could not determine any significant association between (male, female, mixed, or unexplained) factor of infertility and respondent dropout. Two hundred and fifty-three respondents completed the testing twice, 215 respondents completed the testing three times, and 185 of them completed the testing four times. Two subjects who initially enrolled were excluded from the sample because they had previously been diagnosed with azoospermia. Respondents’ medical history including the information on their female partner’s health status and psychiatric history was gathered during the first andrological visit and then updated at the follow-up appointments. Respondents attended the andrological visit along with their spouses. Two hundred and forty-eight out of 255 (97.2%) respondents’ partners had already undergone fertility examination and knew their fertility status at the baseline. The spouses who failed to provide the results of their fertility examination at the first andrological appointment were routinely asked to undergo their evaluation and provide the results of their fertility examination for diagnostic reasons. The data were collected in a way that guaranteed respondents’ anonymity.
Design of the Study
This panel study included the baseline evaluation (T1) and the three subsequent psychological evaluations (T2, T3, T4), which were 2–3 months apart. The assessments were carried out on the day when respondents provided a semen sample for fertility evaluation, 1 day before their andrological appointment. The timing of psychological testing was strictly related to andrological visits and to medical procedures, that is, respondents completed the tests (a) before their initial fertility testing (T1); (b) before the second andrological visit, 2–3 months after they had learned of their role in previous reproductive failure when their emotional response to the diagnosis stabilized (T2); and (c) before the third and the fourth treatment-related or checkup testing appointments (T3, T4). This strategy not only maximized follow-up response rate but also made it possible to observe the effect of the sequence of events related to the effect of diagnostic disclosure and treatment-related/follow-up andrological appointments on the course of distress and the risk of psychiatric morbidity of unintentionally childless males. As the baseline assessment took place 1 day before the first andrological appointment, the respondents were not informed of their fertility status and they obtained information about the results of their initial fertility evaluation during the first doctor’s visit on the next day.
Measures
Along with a sociodemographic questionnaire to be completed only once at the baseline, all participants individually filled up the Polish version of the General Health Questionnaire-28 (GHQ-28). The GHQ-28 is a self-administered screening tool commonly used in medical settings to detect individuals who manifest symptoms of elevated emotional distress and are likely to have or be at risk of developing mood disorders such as depression, which frequently leads to social and occupational disability or suicide (Overholser, Braden, & Dieter, 2012; Seo et al., 2017; Yang et al., 2015). Respondents used a 4-point Likert scale to describe changes in their mood/behavior over the past 4 weeks. The traditional (binary) method of calculating the GHQ score was employed, where answers Not at all and No more than usual scored 0, while the answers Rather more than usual and Much more than usual scored 1. In the present study the GHQ was evaluated with the use of a commonly accepted cutoff point indicating elevated levels of psychological distress and an increased risk of stress-related mood disorders such as depression. Additionally, individuals with scores below or above the cutoff point were dichotomized as non-cases and cases (individuals characterized by clinically significant distress levels who are at risk of psychiatric morbidity), respectively. Since GHQ-28 is used to assess self-reported alterations in a subject’s mental status and not lifelong personal characteristics, it was considered to be particularly well suited for the purpose of the current study, which focuses on the impact of obtaining one’s infertility diagnosis and treatment over time. GHQ-28 is characterized by high test–retest reliability (.78–.9), high internal consistency, and excellent intrarater/interrater reliability (Cronbach’s α .9–.95) and correlates well with the Hospital Depression and Anxiety Scale (HADS). Similarly, the Cronbach’s α of the Polish version of the questionnaire reached the value of .934 (Goldberg & Blackwell, 1970; Goldberg & Williams, 1988; Makowska, Merecz, 2001; Merecz-Kot & Andysz, 2014; Richard, Lussier, Gagnon, & Lamarche, 2004).
Then in order to explore how diagnostic disclosure and treatment-related or follow-up andrological appointments affected respondents’ risk of psychiatric morbidity, respondents were divided into defined respondent subgroups based on their specific subtype of infertility.
Respondents with male factor of infertility, respondents with female factor of infertility, respondents with mixed factor of infertility, and respondents with unexplained (idiopathic) factor of infertility were compared using appropriate non-parametric statistical tests (χ2 test, χ2 test with Yates’s correction for continuity, Fisher’s exact test) with significance level set at <.05. The results of each subgroup were also referred to the outcomes of a separate GHQ-28 testing in a nationwide randomly selected sample of individuals. The sample included individuals 19–65 years old who had no history of previous or present chronic disease or psychiatric treatment (Merecz-Kot & Andysz, 2014). The statistical analysis was performed with the use of Statistica 13.1 (Statsoft, 2013).
Ethical Approval
All subjects were informed about the purpose and importance of the study and assured of their anonymity and confidentiality, and they voluntarily gave their verbal consent to participate. Subjects’ consent was not recorded to maintain their anonymity. The investigator also made sure subjects knew they could stop the testing at any moment. The study proposal was approved by the bioethical committee of our university (Approval No: 920/14), which ensures ethical procedures in data collection and analysis.
Results
Characteristics of the sample
The investigation included 255 male participants, who were 22–51 years old with a mean age of 30.24 ± 4.29. They were married and, except for one respondent who had a child from a previous relationship, childless. Their spouses were 21–42 years old with a mean age of 28.42 ± 3.7. Their waiting time to conception (length of time the couple have been trying to conceive) ranged from 8 to 24 months (M = 14.53 ± 3.17; median value (Me) = 14), while the duration of their current marriage ranged from 1 to 11 months (M = 2.16 ± 1.02). Detailed sociodemographics are presented in Table 1.
Detailed Baseline Sociodemographic Characteristics of Study Participants.

Note. n = the number of respondents within a given category.
The prevalence of clinically significant distress and psychiatric morbidity across the timeline of treatment-related/follow-up andrological appointments
Statistical analysis indicated that the estimated prevalence of clinically significant distress and psychiatric morbidity in the sample amounted to 10.9% at the baseline (baseline assessment; T1). Next, after diagnostic disclosure (second assessment; T2), the percentage of significantly distressed individuals in the sample significantly increased and reached 45.8% (Fisher’s exact test, p value < .00). There were no significant changes at the third assessment (44.6% at T3), but then at the fourth assessment, a significant decrease in the analyzed percentage was observed (25.9% at T4; Fisher’s exact test, p value = .00). The comparison demonstrated that the observed baseline proportion of significantly distressed individuals (10.9%) was lower than the reference value of 12% (the corresponding proportion of significantly distressed individuals in a nationally representative sample of occupationally active individuals aged 19–65 years; Merecz-Kot & Andysz, 2014), but the difference did not reach statistical significance. However, after diagnostic disclosure (at T2), the proportion of significantly distressed individuals in the sample significantly exceeded reference value (χ2, p = .00). These differences remained significant at the third and at the fourth assessment (T3 and T4; χ2, p values = .00 and= .00, respectively).
The impact of diagnostic disclosure on respondents’ distress and mental health status
Of the 255 respondents who enrolled, there were 76 respondents with the male factor of infertility and 80 with the female factor of infertility; 78 respondents came from couples with mixed infertility factor, while 21 were diagnosed with idiopathic (unexplained) infertility factor.
The investigation of the association between respondents’ infertility factor and their distress and risk of psychiatric morbidity has shown that the prevalence of clinically significant distress in the subgroup of respondents with the male factor of unwanted childlessness, which reached 9.2% at the baseline (T1) significantly increased after diagnostic disclosure and reached 59.2% at T2 (p value = .00). At the third and at the fourth assessment (49.2% at T3 and 34.6% at T4), statistically significant changes in the percentage of significantly distressed male factor of infertility respondents could not be determined. The analysis has also shown that the baseline proportion of male factor of infertility respondents was lower than the corresponding reference value of 12% (Merecz-Kot & Andysz, 2014), but statistical differences could not be determined. After diagnostic disclosure (T2), the proportion of significantly distressed individuals with the male factor significantly exceeded the reference value (χ2, p value = .00). These differences persisted at T3 and T4, (χ2, p values = .00 and = .00, respectively).
Next, the analysis indicated that the percentage of significantly distressed respondents with female infertility factor amounted to 13.7% at the baseline and increased to 21.5% at T2. Although significant changes in the prevalence of clinically significant distress in this subgroup could not be indicated after diagnostic disclosure, a significant increase in the percentage of significantly distressed female factor of infertility individuals was observed at the third assessment (42.6% at T3; p value = .04). Finally, at the fourth assessment before the fourth andrological appointment, significant changes in the percentage of clinically distressed female factor of infertility respondents could not be observed (34.4% at T4). The analysis has also shown that the baseline proportion of abnormally distressed female factor of infertility respondents at risk for psychiatric morbidity (13.7%) was greater than the reference value, but the statistical differences were insignificant (Merecz-Kot & Andysz, 2014). At the second assessment (T2), the percentage of significantly distressed female factor of infertility respondents was significantly greater than the reference value (χ2, p value = .04). These statistically significant differences continued at T3 and T4 (χ2, p values < .00 and <.00, respectively).
The assessment of the subgroup with the mixed infertility factor showed the percentage of respondents with clinically significant distress and elevated risk for psychiatric morbidity in this subgroup amounted to 11.5% at baseline (T1) but significantly increased at the second visit, after diagnostic disclosure (67.5% at T2; Fisher’s exact test, p value = .04). At the third assessment before the third andrological visit, the percentage of distressed individuals with mixed infertility factor has not significantly changed (50.7% at T3). At the final assessment before the fourth andrological appointment, the analyzed percentage significantly dropped (16.3% at T4; p value = .00). The analysis has also demonstrated that the baseline (T1) prevalence of clinically significant distress in the subgroup of respondents with mixed factor of involuntary childlessness (11.5%) was lower than the reference value (12%), but the statistical differences were insignificant (Merecz-Kot & Andysz, 2014). At the second assessment (T2), after diagnostic disclosure, the percentage of distressed individuals with the mixed factor was significantly greater than the reference value (χ2, p value = .00). These statistically significant differences persisted at the third visit (T3;, χ2, p value = .00). At the fourth visit (T4), the proportion of significantly distressed individuals with the mixed factor (16.7% and 12%, respectively) still exceeded the reference value, but the differences were statistically insignificant (p value > .05).
The evaluation of the course of distress in the subgroup with idiopathic (unexplained or unknown) infertility factor revealed that the percentage of significantly distressed respondents in this subgroup amounted to 4.7% at the baseline. That proportion has not significantly changed throughout the entire follow-up observation (9.5% at T2, 15.7% at T3, and 0% at T4; see Figure1 for details).
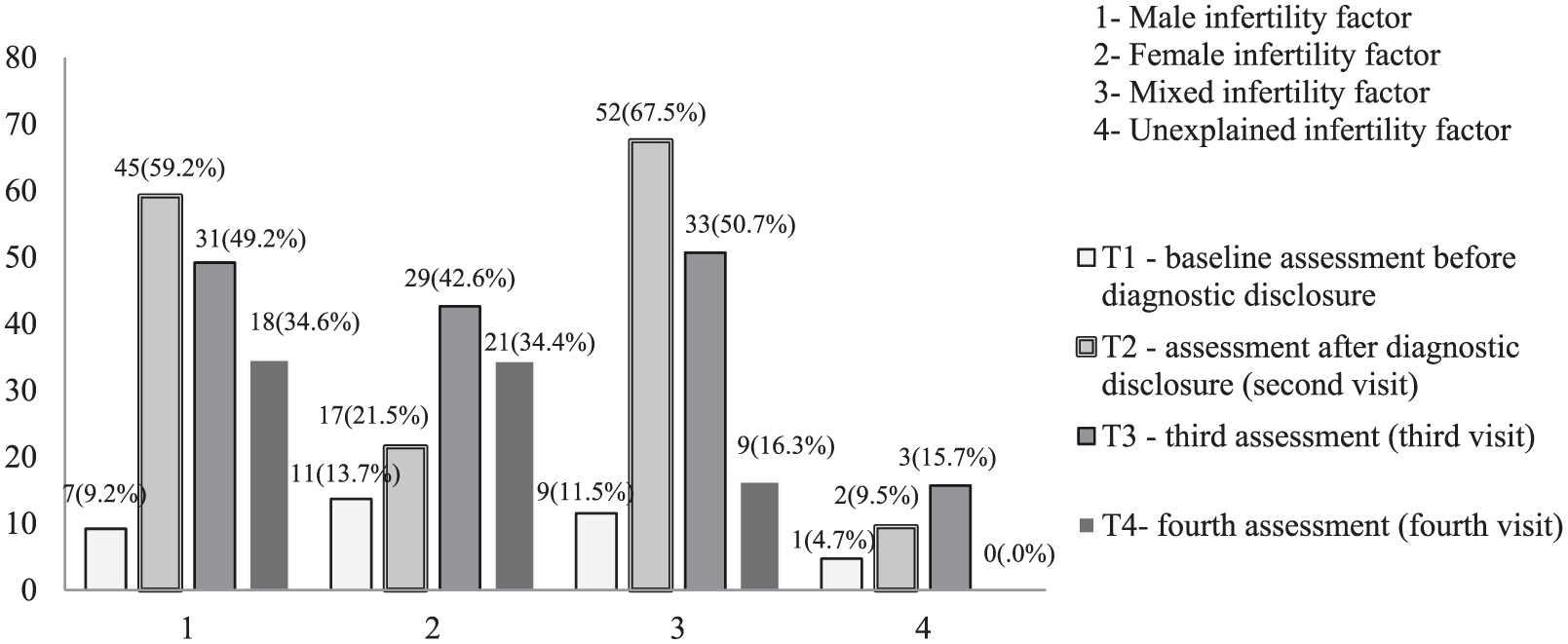
The numbers and percentages of respondents at risk for psychiatric morbidity at various stages of the procedure.
To add, statistical analysis was performed to explore statistical differences in the prevalence of clinically significant distress and risk of psychiatric morbidity between subgroups with male, female, mixed, or idiopathic infertility factor at the baseline and at subsequent psychological assessment before andrological appointments. Here, statistically significant differences could not be determined at the baseline assessment (T1), before the diagnostic disclosure. However, at the second assessment (T2) the prevalence of clinically significant distress was significantly higher in the male factor of infertility respondents than in female factor of infertility respondents (p value = .00) or the mixed or idiopathic factor of infertility subgroup (p value = .01). Distress was also markedly more prevalent in the subgroup with the mixed factor than in the female factor of infertility respondents (p value = .00) or subjects with mixed or idiopathic factor of infertility (p value = .00). Then, these differences persisted at the third and the fourth assessment (T3 and T4), as the analysis has not determined any significant statistical differences associated with respondent’s factor of infertility (χ2, the results are significant at p < .05).
Discussion
Unwanted childlessness may have adverse consequences for male psychological status and well-being. An unfulfilled child wish has been associated with elevated anxiety, low self-esteem, mood disturbances, or depression in males (Fisher & Hammarberg, 2012; Holley et al., 2015; Schick et al., 2016; Wischmann & Thorn, 2013; Yang et al., 2017). The outcomes of the studies were largely determined by the time of the diagnosis, duration of infertility, the length of time the couple had been pursuing medical therapy, or the type of treatment (e.g., respondents were examined prior to making a decision to undergo or while undergoing ART treatment).
This investigation focused on the course of male distress at different stages of fertility experience including fertility workup, diagnostic disclosure, treatment process, and repeated treatment-related or follow-up visits. The timing of psychological testing was strictly related to andrological visits, that is, respondents completed the tests (a) before their initial fertility testing; (b) before the second visit, 2–3 months after they had learned of their role in previous reproductive failure when their emotional response to the diagnosis stabilized; and (c) before the third and the fourth treatment-related or checkup testing appointments. This research design eliminated the effect of a direct emotional response to the diagnostic disclosure and information about the patient’s health status because the respondent’s emotional reaction could stabilize during the time interval between andrological appointments.
The analysis demonstrated that 10.9% respondents had high levels of distress and were at risk for psychiatric morbidity at baseline, before they learned of their andrological diagnosis. These results are similar to the corresponding proportion of significantly distressed individuals in a nationally representative sample of occupationally active individuals aged 19–65 years, which was used as a reference value in the study (Merecz-Kot & Andysz, 2014). In contrast, the analysis has shown that after diagnostic disclosure, the percentage of respondents who were significantly distressed and at risk for psychiatric morbidity markedly exceeded the corresponding baseline percentage or reference values. Learning of the diagnosis led to a marked surge, which was followed by a drop in the percentage of significantly distressed individuals. However, the proportion of significantly distressed individuals at follow-up was significantly greater than the baseline percentage.
The study also aimed to analyze whether the occurrence of clinically significant distress was associated with the learning of one’s biological role in reproductive failure. Respondents were divided into four defined subgroups: respondents with the male factor of infertility, respondents with the female factor of infertility, respondents with the mixed factor of infertility, and respondents with the idiopathic factor of infertility. The analysis of the stress outcomes after diagnostic disclosure revealed a statistically significant increase in the prevalence of clinically significant distress in the subgroups of respondents with the male and mixed infertility factor (p values = .00), while lower proportions of significantly distressed patients were observed in the subgroups with the female and with the idiopathic infertility factor. One may note that at the second assessment, after the diagnostic disclosure, the analyzed percentage of distressed males with male and mixed infertility factors significantly exceeded not only their respective baseline values but also markedly differed from the corresponding percentages of distressed males in the couples with the female and idiopathic infertility factors. These data confirm the conclusions of other studies indicating that males with the male factor of unwanted childlessness may experience elevated distress when they receive their diagnoses ((Fisher & Hammarberg, 2012; Gameiro et al., 2012; Hanna & Gough, 2015; Holter, Anderheim, Bergh, & Möller, 2007; Kumbak et al., 2010; Martins et al., 2016; Pook & Krause, 2005; Schmidt et al., 2012; Wischmann et al., 2009; Wischmann & Thorn, 2013; Wincze, 2015).
There are investigations of psychological effects of diagnostic disclosure of the male infertility factor, which generated discordant results, for example, Kumbak et al.’s (2010) study of Turkish males could not find any significant differences in measures of anxiety, anger, or depression that could be attributed to respondents’ factor of infertility.
Holter’s team (2007) reported that subjects reacted to their infertility experiences similarly, regardless of their diagnostic category. They also demonstrated that the male factor of infertility did not adversely affect their respondent’s well-being or outlook on life.
Pook and Krause (2005), who explored the course of infertility distress in a group of males who twice visited an andrological clinic for workups, demonstrated distress was associated with an interaction of factors such as a recent treatment failure and duration of treatment of ≥17 months. These authors could not indicate that subjects’ distress was directly or indirectly associated with the diagnosis of the male fertility factor.
The aforementioned studies used different designs, for example, the respondents were assessed before starting or while undergoing their ART treatment. In this observation psychological tests were carried out after a considerable period of time since the last visit so the respondent’s psychological status and distress levels could stabilize and reach a plateau. A question may arise about the reasons for the differences between subgroups of respondents with various infertility factors. It may be suggested that during diagnostic evaluation, male patients are affected by a number of factors such as an unfulfilled child wish and the effect of the ability to father a child on their self-esteem or sense of manliness (Fisher & Hammarberg, 2012). It may be concluded that the ability to father a child goes beyond a biomedical problem because in all cultures male fertility is associated with masculinity, so male factor infertility can be perceived as stigmatizing. Other psychological agents influencing males undergoing fertility evaluation may include guilty feelings or feelings of inadequacy that may arise, wife’s reaction, perceived social support, keeping hope in fertility treatments, the subject’s coping skills, or self-efficacy (Boivin & Gameiro, 2015; Culley et al., 2013; Hanna and Gough, 2015; Kumbak et al., 2010; Marci et al., 2012; Navid, Mohammadi, Vesali, Mohajeri & Omani Samani, 2017; Song, Kim, Yoon, Hong, & Shim, 2016; Sylvest, Christensen, Hammarberg, Schmidt, 2014; Volgsten & Schmidt, 2017; Volgsten, Svanberg, & Olsson, 2010; Wischmann & Thorn, 2013).
In the current study the proportion of distressed respondents with mixed infertility factor significantly increased at the second visit but then at the fourth visit the percentage of distressed respondents significantly dropped (p value = .00). In this context, it is noteworthy that both males with the mixed factor and males with the male factor of unwanted childlessness suffer from impaired fertility. However, males with the mixed factor share a similar health problem with their wives. Consequently, they may be more likely to receive their wife’s support and may experience less guilty feelings over not being able to conceive. Social support and acceptance may have advantageously affected coping skills of some participants of the study, so they were ready to reconcile with their circumstances and move forward. At the fourth visit (T4) these males had already been in treatment for some time and knew their medical problem was challenging because both partners needed treatment (Kumbak et al., 2010; Marci et al., 2012; Martins et al., 2016; Sylvest et al., 2014; Wincze, 2015).
This study revealed that the percentage of female factor of infertility respondents with an increased risk for psychiatric morbidity and clinically significant distress remained stable between T1 and T2, but then it rose significantly at T3 (p value < .046). This finding can be related to the fact that the majority of female factor of infertility respondents asked for fertility evaluation because their wife had already been in treatment. It may be suggested that at the time of the third assessment they had realized their chances of having a biological baby were dwindling. That might have resulted in their deteriorated well-being. Publications maintain that males in couples with female infertility factor pursuing medical treatment display distress due to forced timing of sexual activity, psychological pressure to conceive, or because they worry about the side effects of treatment. In the present study, however, the subjects manifested a marked rise in stress levels after they had already been in treatment for some time (Marci et al., 2012; Schaller et al., 2016; Song et al., 2016).
The investigation demonstrated that the subgroup of respondents with idiopathic (unexplained) infertility factor was characterized by a stable percentage of distressed individuals, which remained well below reference values during the entire follow-up time. This problem was also analyzed in investigations of males undergoing ART treatment; for example, Navid and colleagues (2017) observed that males with unexplained fertility factor who were undergoing ART treatment were more satisfied with their life than other unintentionally childless male respondents. On the contrary, Volgsten and colleagues (2017) indicated the unexplained infertility factor was an independent determinant for depression in undesirably childless males in couples undergoing in vitro fertilization procedures. Another study by Volgsten et al. (2010) indicated that 3 years after undergoing unsuccessful in vitro fertilization treatment, individuals with unexplained infertility suffered from compromised well-being and were frustrated over not knowing the causes of their inability to conceive. Unexplained infertility was also difficult to understand, accept, and deal with. The inconsistency in the study findings may be, in part, related to the fact that the respondents of the Volgsten et al. (2010) study were investigated at various stages of their infertility experience. Consequently, they differed in the ability to keep hope in treatment effects and to cope with an uncertain diagnosis. Individuals participating in the current study, in turn, were characterized by a relatively short waiting time to conception, so they could have believed the problem was minor and only temporary. Still, psychological implications of unexplained infertility should be further explored in order to improve the understanding of patients’ difficulties in dealing with the diagnosis and treatment (Boivin & Gameiro, 2015).
Of further interest were changes in the prevalence of clinically significant distress during the follow-up. Here, the analysis demonstrated the percentage of respondents with high levels of distress and an increased risk for psychiatric morbidity decreased in the final stage of the testing. The decrease was most prominent in the subgroup of respondents with the mixed factor but it was the least prominent in respondents with male factor of infertility. The decrease may by associated with factors. These factors may include patients’ adjustment to the diagnosis of infertility, their readiness to make decisions about initiating in vitro fertilization treatment, or finding alternative ways to fulfill parenthood goals (e.g., the decision to start adoption procedures). However, the observed mechanisms seem to be diverse and appear to be related to the diagnostic category of unwanted childlessness. Adequate support directed at helping individuals who are treated for unwanted childlessness may be very helpful. The support interventions should consider the diagnostic category of infertility and its effect on patient’s distress and psychological strain. Infertility treatment specialists or other health-care professionals should be provided education training programs to help them understand how learning of one’s role in inability to conceive influences distress and risk of psychiatric morbidity. Infertility staff should integrate the knowledge into practice so that they will be able to provide adequate emotional support to males treated for unwanted childlessness.
The present study has some limitations that should be considered while interpreting the results. First, respondents came from a single setting and covered the costs of andrological procedures at the clinic. Second, it is acknowledged that the questionnaires were retrospective and self-administered. Third, respondents’ stress outcomes could have been affected by other factors such as age or their religious background. However, the longitudinal nature of the study provides valuable indicators for physicians, counselors, and other professionals working with males with unintended childlessness.
Conclusion
The study implies that male course of distress and risk of psychiatric morbidity is significantly affected by the factor of infertility and changes across the pathway of treatment-related/follow-up andrological appointments. The risk for psychiatric morbidity significantly surges after the diagnostic disclosure, particularly if male or mixed factor of infertility is diagnosed; then it decreases but remains significantly elevated during the follow-up.
Footnotes
Acknowledgements
The author thanks the infertility staff of the andrological outpatient clinic for their kind and unconditional support in gathering the data for this study. The author would also like to acknowledge and thank the participants who generously shared their time and answered the questionnaires.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.