
Abstract
The objectives of this study were to examine the evolution of fathers’ long-term dyadic adjustment after the birth of a child and to analyze their evolution considering related factors. A total of 113 Spanish fathers with a mean age of 35.72 years (SD = 3.84 years) participated. In general, there was a decline in the dyadic adjustment of the fathers until 6–12 months after childbirth, after which their level of adjustment remained stable until 13–24 months. We observed different patterns when analyzing the evolution by subgroups formed based on these different variables, previous experience of paternity, and anxiety. The intrinsic differences between fathers should also be considered because these differences can influence the way in which men face the parental process as well as the evolution of the quality of their relationship with their partner.
The transition to parenthood (TTP) is considered a crucial moment for families, which requires them to adapt to the demands of the arrival of a new family member and to reorganize their lives on an individual, partnership, and family level (Cowan & Cowan, 2012). This process can last until the child is 2 or 3 years of age (Canàrio & Figueiredo, 2017). According to Kralik et al. (2006), the term “transition” is defined as a temporary process during which people must adapt to a new situation or circumstance; thus, the inclusion of a new child in the family structure would constitute a TTP, regardless of whether it were the first or a subsequent child (Cowan & Cowan, 2012).
Although the arrival of a child is a happy event, it is also recognized as a period of stress during which there are increased demands and responsibilities related to the care of the baby and the acquisition of new parental roles (Barimani et al., 2017; Cowan & Cowan, 2012). Saxbe et al. (2018) described how TTP implies changes at the biopsychosocial level among both men and women. For example, at the physical level, there is evidence of increased fatigue (Loutzenhiser et al., 2015) and sleep impairment (Hagen et al., 2013). At a psychological level, a meta-analysis by Cameron et al. (2016) recently reported that the prevalence of depression throughout TTP among men is nearly twice that of the adult population not in a TTP, and is directly related to maternal depression rates. In another systematic review, Leach et al. (2016) identified that anxiety among fathers is common during the pre- and postnatal period and that these levels increased and stabilized before the birth but declined throughout the postpartum period. In terms of relationships, decreases in sharing and independent leisure time (Claxton & Perry-Jenkins, 2008) as well as in relationship satisfaction (Doss et al., 2009; Mitnich et al., 2009; Mortensen et al., 2012; Trillingsgaard et al., 2014) have been reported.
The relationship satisfaction of couples is considered another relevant factor during the TTP. This construct is often used to describe the quality of relationships and is synonymous with the terms “quality,” “adjustment,” and “happiness” (Graham et al., 2011). Among other areas, its importance lies in its influence on personal well-being and mental health (Bower et al., 2013; Proulx et al., 2007) as well as its effect on relationships with children (Kouros et al., 2014). For example, in a study of Portuguese parents, Figueiredo and Conde (2011) concluded that the symptoms of postpartum depression in both men and women increased when the interactions between couples were poorer, while there was a lower risk of anxiety during the postpartum period among parents who assigned higher scores to their interactions with their partners.
Previous international studies have longitudinally examined the changes experienced during the TTP in terms of partnership satisfaction while considering other relevant variables. For example, in an 8-year prospective study conducted with 218 couples in the United States, Doss et al. (2009) reported negatively impacted the functioning of the partnership in both men and women, and indicated that lower incomes tended to predict more deterioration in fathers’ relationships after the birth. Doss et al. (2009) were unable to confirm whether this decrease was exclusively caused by the process of the TTP because there were no significant differences in the relationship function among new parents compared to the control group who had not become parents. In another meta-analysis, Mitnick et al. (2009) reported considerable heterogeneity in their results and concluded that there were small decreases in satisfaction among both men and women up to 11 months after childbirth. In studies that carried out evaluations up to 12 and 14 months postpartum, the decreases in partnership satisfaction had a moderate effect size. Finally, Trillingsgaard et al. (2014) reported that fathers experienced a decrease in satisfaction with their partner until 30 months postpartum.
In agreement with other theories, Don and Mickelson (2014) proposed that this variability in results may be because parents experience and face the challenge of the birth of a child in different ways. According to the vulnerability-stress-adaptation model (Karney & Bradbury, 1995), an individual’s adjustment to a stressful event may vary depending on individual variables, the couple, and the adaptive process itself. Similarly, DeHann et al.’s (2002) theoretical model focuses on levels of family stress and resilience. Based on the idea that not all families adapt in the same way to the process of change, Volling et al. (2015) proposed five patterns of marital relationship changes that may appear during the TTP process: the “honeymoon” (an increase in relationship satisfaction which then returns to pre-birth levels), “no change,” “adjustment and adaptation” (a return to pre-birth levels), “linear decline,” and “crisis” (a sudden decline in satisfaction, which persists over time without returning to the prenatal levels).
Because longitudinal studies in this field have reported mixed results, research in different contexts is useful for understanding both stress and adaptive changes in couples and to obtain helpful information about which types of support is required and will be most effective (Delicate et al., 2017; Volling et al., 2015). In addition, because of gender differences in relationships (Don & Mickelson, 2014), further studies are still needed to separately assess relationship satisfaction in each partner in order to develop a clearer understanding of these differences (Korja et al., 2016); in particular, we have far less knowledge about couples’ relationships and psychological adjustment during the TTP from the perspective of fathers (Figueiredo et al., 2018). Specifically, in the Spanish context, we were unable to find any publications that examined the relationship between men and women during the TTP. The current policies in place in Spain to support parenting are somewhat limited and are based on a traditional care model in which women are more involved in the family than men (Moreno-Mínguez et al., 2017).
The objectives of this present study were to examine the evolution of fathers’ long-term dyadic adjustment after the birth of a child and analyze their evolution, considering its related factors. In accordance with other results published in the literature (Mitnick et al., 2009), we expected the dyadic adjustments of fathers to decrease, on average, over the period we evaluated from childbirth up to 24 months postpartum. Research addressing the experience of fathers has the potential to significantly contribute to the literature on the TTP, because this population remains poorly studied. In this work, we hypothesized that the changes produced in the adjustment of couples would be related to whether the father already had children (Dyrdal & Lucas, 2013) as well as with their anxiety levels (Figueiredo & Conde, 2011).
Methods
Design, Setting, and Sample
This was a longitudinal observational study, which evaluated fathers at three different time points: at hospital discharge after childbirth, between 6 and 12 months (M = 8.27, SD = 1.39), and at 13–24 months postpartum (M = 19.47; SD = 2.22). We used a convenience study sample and the participants were recruited from October 2013 to March 2016. All the fathers that met the selection criteria on the day of hospital discharge after the birth of their child were asked if they were voluntarily willing to participate in this study. Fathers who were fluent in Spanish and able to speak and write without difficulty were included in this work. Men whose partner (a) had had multiple pregnancies; (b) had a serious complication after childbirth; or (c) whose newborn had had severe health problems requiring admission to an intensive care unit after birth, were not included in the study. The entire study cohort was collected from a total of 16 hospitals in different geographical areas of Spain: 13 from the Valencian Community, and one each from Castilla la Mancha, Catalonia, and Murcia.
Measures
The following sociodemographic variables were evaluated: age; nationality (Spanish/non-Spanish); current marital status (married or domestic partner; separated or divorced; single; widower); educational level (incomplete primary education; complete primary education; complete secondary education; or university-level education); and socioeconomic status (measured as the household income level per year, with eight response options ranging from less than €6,000 to more than €60,000). We collected the following data related to paternity and the experience of childbirth from the mother’s medical records at the time of hospital discharge: previous experience with paternity (dichotomous variable: first-child or previous children); the couple’s type of birth (categorical variable with four response options: normal vaginal birth; instrumented; scheduled caesarean section; or urgent caesarean section).
The brief version of the Dyadic Adjustment Scale (Santos-Iglesias et al., 2009), adapted from the translation of Bornstein and Bornstein into Spanish (1988), was used in this study. This scale evaluates the quality and adjustment of relationships and higher scores indicate greater adjustment in the couple; it comprises a total of 13 items grouped into three interrelated subscales (satisfaction, consensus, and cohesion) and its short version translated into Spanish had adequate psychometric properties and adjusted well according to the confirmatory factor analysis results (comparative fit index [CFI] = .95, adjusted goodness of fit [AGFI] = .93, and root mean square error of approximation [RMSEA] = .05). The overall scale had an internal consistency of .83 and the cut-off point for clinical interpretation was 44 for the low and high adjustment values.
The Spanish adaptation of the State-Trait Anxiety Inventory (Spielberger et al., 1982) evaluates two independent constructs of anxiety as a trait (the relatively stable tendency of people to perceive situations as threatening) and as a state (a situational condition that can vary with time and in intensity). This survey uses a Likert-type scale with four response options ranging from 0 (not at all) to 3 (a lot) and the total score of each subscale, comprising 20 items each, ranges from 0 to 60 points, with higher scores indicating higher levels of anxiety. The Spanish version of this scale had adequate psychometric properties both in terms of internal consistency (α = .90–.93 for the state subscale and α = .84–.87 for the trait subscale) and for construct validity (r = .73–.85), evaluated with the Taylor Manifest Anxiety Scale and Cattell’s Anxiety Scale.
Procedure
The participants completed the questionnaires at three different time points. The sociodemographic variables were collected and the dyadic adjustment and state-trait anxiety scales were administered in a paper-based format at the hospital at baseline (on the day of hospital discharge after the childbirth). The dyadic adjustment scale was completed online in the second and last periods between 6–12 months and 13–24 months, respectively. We sent four reminders about the completion of the surveys for the latter two time points at an interval of 10 days each to help increase the study participation rates. The individuals included in this study received no incentive for their participation.
The study was approved by the Clinical Research Ethics Committee at the General Direction of Public Health and Higher Public Health Research Centre, which both form part of the Valencian Community Health Council. Written informed consent for participation was collected from the fathers at baseline, at the time of their recruitment. The confidentiality of the data collected was ensured by using encrypted codes for each participant.
Analysis
SPSS (Version 26.0; IBM Corp., Armonk, NY) and R (version 3.4) software were used to perform the statistical analyses in this work. Descriptive analyses and correlations were carried out for the dyadic adjustment variables and sociodemographic, paternity-related, and state and trait anxiety variables (N = 113). We examined the differences between the means for the dichotomous variables, variances of the differences in the categorical variables, and correlations in the continuous variables. Non-parametric tests were used when the normality assumption was violated. In addition to statistically significant differences, we considered clinically relevant differences by analyzing Cohen’s d effect-size statistic (Cohen, 1988). The influence of the main outcome (dyadic adjustment) and the fathers’ age upon the drop-out rate over time was evaluated by binary logistic regression.
Finally, a longitudinal analysis of the dyadic adjustment variable was calculated (at baseline and at 6–12 and 13–24 months postpartum) by analyzing the variance with repeated measures (ANOVA generalized linear model [GLM]) by separately including the variables of having previously fathered children and state and trait anxiety into subsequent analyses (n = 113). We separately set the cut-off point at the 50th percentile (P50) of the state and trait anxiety subscale scores in order to distinguish individuals with lower and higher anxiety levels on each subscale. Next, we carried out longitudinal analyses separately for all the aforementioned father subgroups (already a father, no previous children, low state anxiety, high state anxiety, low trait anxiety, and high trait anxiety) to monitor the evolution of the fathers’ dyadic adjustment independently for each factor. Finally, the sphericity assumption was calculated using the Mauchly W test for all the analyses, and we implemented a post-hoc comparison between the different time points by using the Bonferroni test.
Results
Participants
The sociodemographic variables of the sample cohort are presented in Table 1. We obtained responses from 113 men aged between 25 and 49 years (M = 35.72, SD = 3.84); 85% (n = 96) were married, 12.4% (n = 14) were single, and 0.9% (n = 1) were separated/divorced from a previous partner. All of them (100%) were living with their current partner. In terms of nationality, 94.7% (n = 107) of the sample were Spanish and the socioeconomic level of the cohort (based on their total annual family income) varied considerably: 11.5% earned less than €11,999 per year, 53.1% had an income of €12,000 to €29,999, and 32.7% earned in excess of €30,000. A total of 25.7% had finished their primary education, 22.1% had completed a secondary education, and 44.2% had a university-level education. For 67.3% (n = 76) of the sample, the newborn related to this study was their first child; more than half the births in the sample had been normal vaginal births (71.7%, n = 81) and the remainder had been instrumented or caesarean section deliveries. Most of the fathers (69.9%) accompanied their partners in childbirth.
Sociodemographic Variables of the Fathers and Their Association With Dyadic Adjustment at Baseline (N =113).

Note. M = average; SD = standard deviation.
Spearman correlations for continuous variables. bKruskal–Wallis test for non-compliance with the assumption of data distribution normality. cMann–Whitney U test for the difference between the means of non-parametric data. dThe number of children was based on the parity of the mother.
p <.05.; **p < .001.
Differences at Baseline
Dyadic adjustment after hospital discharge was associated with having previously been a father (U = 987.5; p < .001). First-time fathers had higher dyadic adjustment scores (M = 53.42; SD = 5.66) compared to those that had previous children (M = 50.47; SD = 6.54; Table 1), with a Cohen d effect size of .48. However, no relationships with dyadic adjustment were observed for the other sociodemographic variables. Our analyses showed correlations between dyadic adjustment and trait anxiety (r = −.30, p < .001) and state anxiety (r = −.48, p < .001) measured at the time of hospital discharge, with an effect size of .15 and .23, respectively.
Attrition
A total of 1379 men initially participated at baseline, while the response rate at 6–12 months postpartum was 19% (n = 256), and at 13–24 months was 44.14% (n = 113; Figure 1). The binary logistic regression showed that the loss rate was not related to the study variable—dyadic adjustment (Exp (b) = 1.001; p = .93; 95% CI [.97, 1.03]) or the fathers’ age (Exp (b) = 1.02; p = .28; 95% CI [.98, 1.06]).

Flowchart for longitudinal design in dyadic adjustment variable.
Longitudinal Dyadic Adjustment Analysis
The longitudinal dyadic adjustment analysis was performed with a total of 113 participants. Table 2 presents the dyadic adjustment scores at the different time points. There was a significant decrease in dyadic adjustment at each time point (F = 20.18, p < .001) and the results adjusted well to a linear function (F = 44.53; p < .001; Figure 2). Post-hoc analyses showed that there were significant differences in dyadic adjustment between the immediate postpartum period (M = 52.50; SD = 6.07) and 6–12 months postpartum (M = 50.03; SD = 8.19; Bonferroni test = 2.48; p < .001), and that this adjustment stabilized between 6–12 and 13–24 months postpartum (M = 48.74, SD = 7.18; Bonferroni test = 1.28; p = .11).
Dyadic Adjustment Statistics for Overall Sample Based on Previous Experience With Paternity and State and Trait Anxiety Variables.
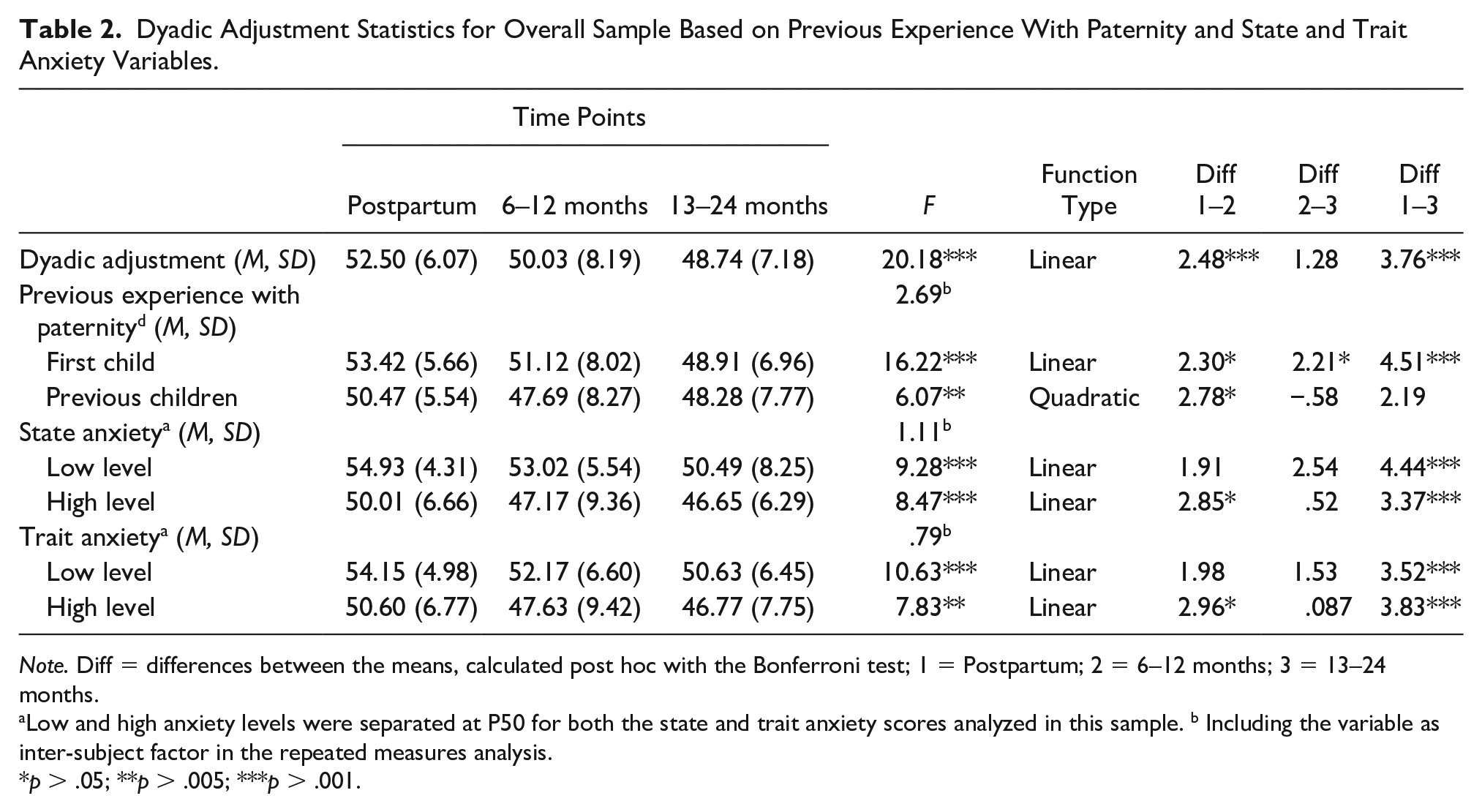
Note. Diff = differences between the means, calculated post hoc with the Bonferroni test; 1 = Postpartum; 2 = 6–12 months; 3 = 13–24 months.
Low and high anxiety levels were separated at P50 for both the state and trait anxiety scores analyzed in this sample. b Including the variable as inter-subject factor in the repeated measures analysis.
p > .05; **p > .005; ***p > .001.
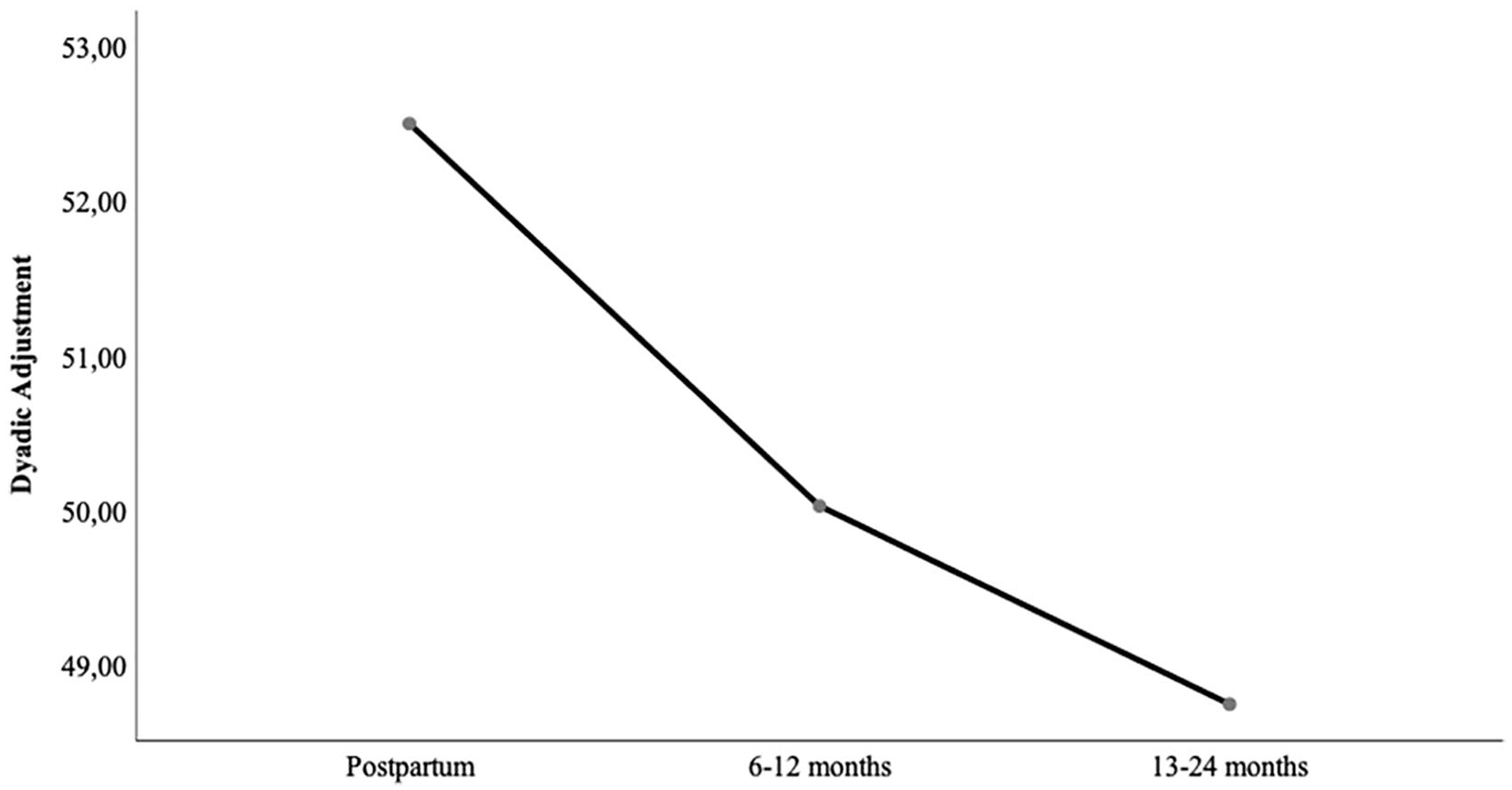
Longitudinal evolution of the fathers’ dyadic adjustment.
There were no significant interactions between dyadic adjustment and having previously fathered a child (F = 2.69; p = .07), indicating that this decrease is independent of this factor (Figure 3). Separate analyses for each group showed that fathers’ satisfaction with their relationship with their partner adjusted to a quadratic function (F = 5.60; p = .02) for those with previous children. There was a significant decline in satisfaction in this group between the immediate postpartum and 6–12-month time points (Bonferroni test = 2.78; p = .02), but by 13–24 months, this difference was no longer significant compared to the immediate postpartum scores (Bonferroni test = 2.19; p = .06), indicating that the dyadic adjustment had returned to its initial levels by the end of the study. In contrast, the changes experienced by first-time fathers adjusted well to a linear function (F = 40.05; p < .001) and there were significant differences in their satisfaction with their partnership between both the immediate postpartum and 6–12-month time points (Bonferroni test = 2.30; p = .02) and the 6–12- and 13–24-month time points (Bonferroni test = 2.21; p = .03; Table 2).

Changes in the fathers’ dyadic adjustment, depending on the previous experience with paternity variable.
We subsequently examined whether the decrease in dyadic adjustment over time was independent of fathers’ baseline state and trait anxiety levels. The P50 cut-off point used to distinguish individuals with higher or lower state or trait anxiety scores corresponded to 12 points for both subscales. The results indicated that the decreased dyadic adjustment did not significantly change between groups with different levels of state (F = 1.11; p = .4; Figure 4) or trait (F = .79; p = .73; Figure 5) anxiety. Significant declines in partner satisfaction were observed for fathers with low state or trait anxiety levels between baseline and the end of the study (low state anxiety: Bonferroni test = 4.44; p < .001 and low trait anxiety: Bonferroni test = 3.52; p < .001). There were also significant differences among fathers with high levels of state or trait anxiety immediately postpartum and at 6–12 months postpartum (Bonferroni test = 2.85; p = .02 and Bonferroni test = 2.96; p = .02, respectively), but this adjustment subsequently stabilized by 13–24 months in both cases (Bonferroni test = .52; p = 1.00 and Bonferroni test = .087; p = 1.00, respectively; Table 2).
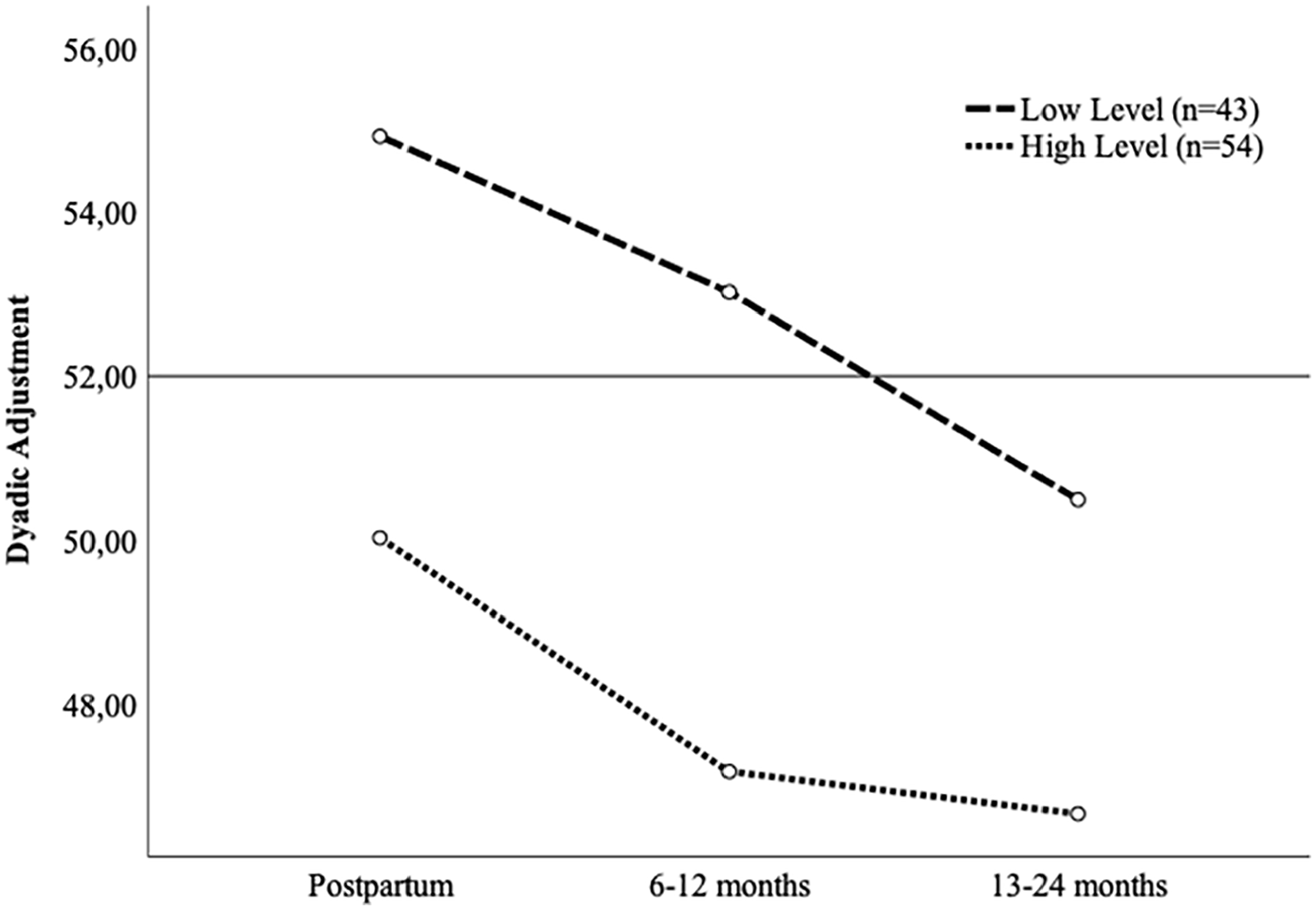
Evolution of the fathers’ dyadic adjustment, depending on the state anxiety variable.

Evolution of the fathers’ dyadic adjustment, depending on the trait anxiety variable.
Discussion
The main objective of this present study was to examine the changes experienced by fathers regarding the quality of their relationship with their partner after the birth of a child; to the best of our knowledge, this is the first research of this type to be carried out in Spain. The results showed a decline in the dyadic adjustment during the first 6–12 months after becoming a father. After this point, the deterioration in couples’ relationships tended to stabilize at the same levels until the end of the evaluation at 13–24 months postpartum. According to the patterns of change proposed by Volling et al. (2015), the overall dyadic adjustment of the fathers in this cohort followed a crisis pattern, meaning that by 18 months postpartum, the quality of fathers’ partnerships was inferior to its prenatal levels. This decrease was also independent of having already fathered a child (O’Brien & Peyton, 2002) or the levels of state or trait anxiety these men had experienced in the immediate postpartum period. Longer longitudinal studies will be required to clarify how long the impact of the TTP process lasts or indeed, whether reported changes in relationship satisfaction ever return to their baseline levels.
Based on different theories about stress and adaptation (De Haan et al., 2002; Karney & Bradbury, 1995) and parenthood-coping strategies (Don & Mickelson, 2014; Volling et al., 2015), it is insufficient to report the average scores for the evolution of the dyadic adjustment. Therefore, our second objective was to analyze the trajectory of these partnership dyadics according to whether these men had already fathered children and as a function of their baseline anxiety levels.
First, first-time fathers reported better dyadic adjustment in the immediate postpartum period compared to those who already had children. This may be because the fathers who already had children were more likely to have been impacted by the previous TTP, which could have reduced their reported relationship satisfaction levels at the outset of this study. In agreement with this, the decline in the satisfaction and functioning of partnerships reported in a previous study was greater in multiparous couples (Lindblom et al., 2014). Volling et al. (2015) suggested that the adjustment and adaptation of first-time fathers do not usually return to their reported prenatal levels, meaning that these men may start any subsequent TTP processes with an already “impaired” relationship quality. It is also important to consider that fathers with previous children must also assume their new postnatal-period parental roles alongside their responsibilities to their previous children, which could disproportionately affect the quality of their relationship dyadic.
Second, we found that fathers with previous children reported that, after 6–12 months, their dyadic adjustment had returned to levels similar to those immediately postpartum. According to Volling et al. (2015), fathers with previous children showed an adjustment and adaptation pattern while first-time fathers showed a linear decline pattern. These authors also suggest that parents who already had children adapted more effectively to a new child because they had already divided the parental tasks between themselves and their partner when they became parents for the first time. Continued longitudinal investigation of the long-term evolution of these dyadic adjustments in the context of potential cofactors could help to identify different patterns in this dyadic evolution during the pre-, intra-, and postnatal periods.
Finally, in agreement with previous studies (Rollè et al., 2017; Whisman et al., 2011), we observed that fathers with higher trait or state anxiety levels showed poorer dyadic adjustment in the immediate postpartum period. We concluded that men with higher baseline anxiety levels began their new parental role with a poorer relationship dyadic with their partner, which could have repercussions on a personal level as well as for their family and newborn (Bower et al., 2013; Kouros et al., 2014; Proulx et al., 2007).
We also investigated the evolution of the dyadic adjustment according to the initial state or trait anxiety of these fathers. Our results indicated that, among fathers with high anxiety levels in the immediate postpartum period, the relationship with their partner declined until 6–12 months, after which it stabilized, that is, a typical crisis pattern. This could perhaps be explained by the high demands associated with a new child combined with heightened state-trait anxiety levels in these men, causing a decline in adjustment until they begin to adapt to the new situation. In contrast, the dyadic adjustment of fathers with lower anxiety levels was not as affected, even though their adjustment had worsened 13–24 months after childbirth compared to the immediate postpartum period.
Given that the birth of a child is a time of considerable stress for families, fathers’ adaptation to the new situation is likely affected by the coping strategies they employ (Karney & Bradbury, 1995). It would be useful to include the mental healthcare considerations of fathers in prenatal care plans in order to address potential problems in the future functioning of couples’ relationships (Rollè et al., 2017; Trillingsgaard et al., 2014). Nonetheless, in our sample, less than 10% of the cohort had scores indicative of high anxiety levels (over 40 points), and hence future studies should explore the evolution of dyadic adjustment among fathers with more marked differences between low and high state-trait anxiety levels in order to confirm and better understand these patterns.
Limitations
The limitations of this research should be considered when interpreting these results. First, because we used a convenience sample, caution should be exercised regarding the external validity of the study. Second, more than 50% of the initially recruited cohort were lost to follow-up at the subsequent time points. Nonetheless, this loss was not associated with dyadic adjustment and therefore we assumed that the internal validity of the study had not been compromised. Future projects should be designed to maintain high participation rates over time in order to guarantee the internal validity of the work. Third, we used the parity of the mother as a proxy for the fathers’ previous number of children variable. Therefore, any children the participants had fathered with other partners were not considered, and so some men may have erroneously been categorized as first-time fathers. Fourth, the baseline dyadic adjustment evaluation was carried out at the time of hospital discharge after childbirth even though this corresponded to the midpoint in the TTP process. In contrast, the literature recommends evaluating any changes in couples’ relationships from the start of the TTP process—from the time parents first become aware of the pregnancy (Delicate et al., 2017; Don & Mickelson, 2014).
Conclusions
We concluded that fathers’ dyadic adjustments were usually affected by the birth of a child. Nevertheless, we must also consider preexisting differences between fathers and the evolution in the quality of their relationships, which can both influence the way fathers face the TTP. Future research should continue to deepen our knowledge from this perspective and aim to understand the profiles underlying different trajectories in couples’ relationships, thus facilitating the assessment of potential risk and protection factors for new parents. This work has important implications for clinical practice because it allows health professionals to understand the specific needs of couples and families during the TTP. This will allow health professionals to plan more effective pre-, intra-, and postnatal care while also considering parental diversity. Finally, it is important to avoid generalized activities and interventions, which assume that all fathers experience the birth of a child similarly.
Footnotes
Acknowledgements
The authors thank the institution and all the professionals who participated as well as all the fathers who contributed to the study.
Author Contributions
All listed authors meet the criteria for authorship
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The present study was granted by the General Sub-Directorate for Evaluation and Promotion of Research (Institute of Health Carlos III, ISCIII) and co-funded by the European Regional Development Fund (FEDER) (No. PI14/01549).