
Abstract
As testicular torsion is a medical emergency, it requires quick diagnosis and treatment. Color Doppler ultrasound (CDUS) is useful for the diagnosis of testicular torsion. An accurate diagnosis can be difficult when CDUS indicates the preservation of blood flow in the testis. We examined the accuracy of testicular torsion diagnosis in patients with acute scrotum made by doctors on duty using CDUS. The subjects included 26 patients who visited our department between January 2016 and June 2018 presenting with acute scrotal pain. Patients were placed into one of three groups based on testicular blood flow evaluated by CDUS. The first group had no testicular blood flow, the second had diminished blood flow, and the last group had normal or increased blood flow. Patients were also diagnosed through scrotal exploration. Finally, patients were further divided into two groups identified by CDUS frequency utilized during diagnosis (12 MHz groups and ≤8 MHz groups), and the diagnostic accuracy of the two groups was compared. Characterizing torsion by either the absence of or diminished, testicular blood flow in the CDUS evaluation, the sensitivity and specificity of the CDUS performed by doctors on duty accounted for 69.2% and 53.8%, respectively. No improvement in diagnostic accuracy was evident despite the usage of a 12-MHz ultrasonic transducer. In this study, the sensitivity of CDUS performed by doctors on duty was about 70%, suggesting that scrotal exploration should be performed promptly even if testicular blood flow is observed and testicular torsion is suspected from medical history and body findings.
Trauma aside, torsion of the appendix testis, acute epididymitis, orchitis, testicular tumor, incarcerated inguinal hernia, and Henoch–Schönlein purpura are some of the conditions that may present as an acute scrotum. A differential diagnosis is particularly important for torsion of the appendix testis and acute epididymitis, as both appear with high frequency.
Color Doppler ultrasound (CDUS) is extremely useful in identifying testicular torsion and can be employed in a noninvasive bedside setting. An accurate diagnosis can be difficult, such as when limiting diagnosis to patient medical history and physical examination, or when blood flow is shown by CDUS to be preserved in the testis. If treatment is delayed, the testicle can undergo irreversible change producing damage. This becomes critical when diagnosis occurs in an emergency outpatient setting in which the doctor on duty must somehow perform a speedy and accurate diagnostic ultrasound followed by the appropriate treatment. We retrospectively compared the final diagnosis established by scrotal exploration with preoperative CDUS observation of testicular blood flow evaluated by doctors on duty.
Materials and Methods
The subjects included 26 patients who visited the Department of Urology of Dokkyo Medical University Saitama Medical Center between January 2016 and June 2018 presenting with acute scrotal pain. These patients had surgical treatment after the CDUS examination using a standard machine (TOSHIBA) equipped with high resolution and a color Doppler linear probe (>7.5 MHz). CDUS evaluation was conducted by the resident urologist (doctor on duty), who had no special ultrasound training. Some patients received these evaluations during after-hour visits. Determination of the presence/absence of testicular ischemia using ultrasound was made by at least two urologists. Patient age ranged from 3 to 26 years (average 10.5), with nine patients affected on the right scrotal side and 17 on the left. Patients were placed into one of three groups based on testicular blood flow evaluated by CDUS. The first group had no testicular blood flow, the second had diminished blood flow, and the last group had normal or increased blood flow. Patients were also diagnosed through scrotal exploration and accordingly classified into one of the following groups: testicular torsion, torsion of the appendix testis (appendage torsion), epididymitis, or some other condition.
Finally, patients were further divided into two groups according to the CDUS frequency utilized during diagnosis (12 MHz and ≤8 MHz), and the diagnostic accuracy of the two groups was compared. All the data were entered in Microsoft Excel format and then exported to SPSS21 (IBM, Armonk, NY). The correlation between the two groups was calculated using Cohen’s κ coefficient. Correlation values were determined to be very weak (0–0.19), weak (0.2–0.39), moderate (0.40–0.59), strong (0.6–0.79), or very strong (0.8–1.0).
Results
CDUS Diagnostic Accuracy of Testicular Torsion by Doctors on Duty
Final diagnosis established by scrotal exploration showed that testicular torsion accounted for 50% (13/26); torsion of the appendix testis (appendage torsion), 31% (8/26); and epididymitis, 12% (3/26). The median elapsed time between CDUS evaluation and scrotal exploration was 3 hr. As shown in Table 1, four out of four patients in the group without testicular blood flow were diagnosed with testicular torsion. Alternatively, testicular torsion was confirmed in five of the 11 patients (46%) in the group with diminished testicular blood flow, and in four of the 11 patients (36%) in the group with normal or increased testicular blood flow. Characterizing torsion by either the absence of or diminished, testicular blood flow in the CDUS evaluation, the sensitivity and specificity of the CDUS performed by doctors on duty accounted for 69.2% and 53.8%, respectively.
Comparison of Final Diagnosis by Scrotal Exploration with Preoperative Observation Using Color Doppler Ultrasound (CDUS).

Comparison of Diagnostic Accuracy for Testicular Torsion by Doctors on Duty Depending on CDUS Frequency
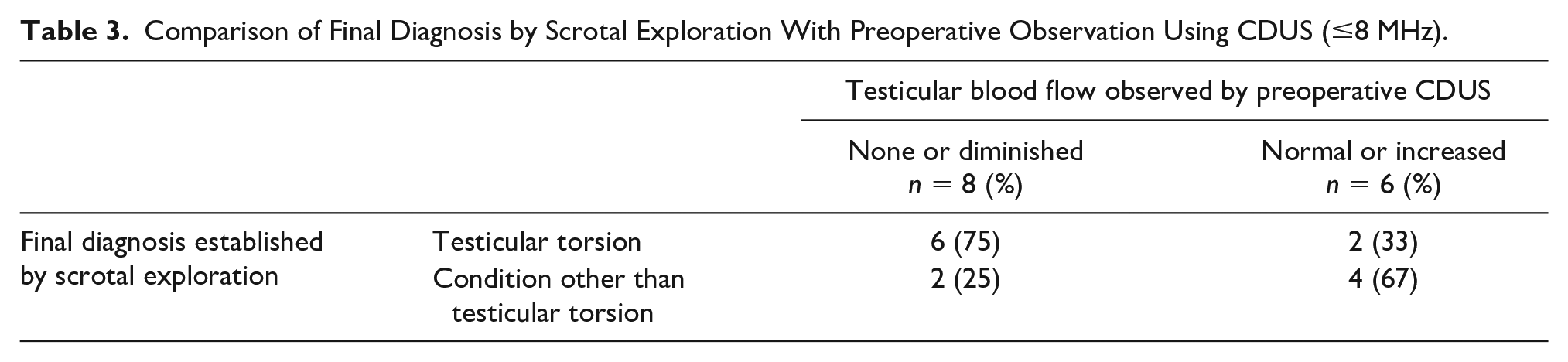
The sensitivity and specificity of the testicular torsion analysis, when compared by CDUS frequency, were 60% and 43%, respectively, for the 12 MHz group (Table 2), and 75% and 67%, respectively, for the ≤8 MHz group (Table 3). The agreement coefficient between the two groups was weak, with κ = 0.32 (p = .0215).
Comparison of Final Diagnosis by Scrotal Exploration With Preoperative Observation Using CDUS (12 MHz).

Comparison of Final Diagnosis by Scrotal Exploration With Preoperative Observation Using CDUS (≤8 MHz).
Discussion
Statistics show that the annual incidence rate for testicular torsion in the United States is 4.5 cases per 100,000 males (Mansbach et al., 2005), whereas a survey in Bristol in the UK pointed to one case among 4000 males aged 25 or under (Williamson, 1976).
Underlying diseases producing acute scrotum are wide-ranging, but testicular torsion, torsion of the appendix testis, and epididymitis account for some 80%, with each, reportedly accounting for 20%–30%, 40%–60%, and 5%–15%, respectively (Anderson & Giacomantonio, 1985; Makela et al., 2007; Murphy et al., 2006; Mushtaq et al., 2003; Sidler et al., 1997; Van Glabeke et al., 1999).
Rabinowitz (1984) reported that among 245 cases of the pediatric acute scrotum that they examined, testicular torsion accounted for 56 cases (23%), torsion of the appendix testis for 77 cases (31%), and epididymitis for 47 cases (19%). Pogorelic et al. (2016) reported that among 558 cases of the pediatric acute scrotum that they treated surgically, testicular torsion accounted for 142 cases (25%), torsion of the appendix testis for 344 cases (62%), epididymitis for 54 cases (10%), and testicular trauma for 10 cases (2%), with other causes accounting for eight cases (1%). At our hospital, testicular torsion accounted for 50% of the 26 cases of the acute scrotum for which scrotal exploration was performed. Surgery was performed in many cases even for torsion of the appendix testis and epididymitis—acute scrotum conditions for which conservative therapy is possible. Reports from many institutions (including our own) suggest that an accurate diagnosis of testicular torsion is difficult.
Amidst these circumstances, a variety of predictive factors in diagnosing testicular torsion has been reported. Barbosa et al. (2013) conducted a forward-looking investigation of 338 cases of the acute scrotum and utilized five clinical conditions and physical findings to develop the TWIST scoring system, with Sheth et al. (2016) subsequently validating the system’s usefulness. Shah et al. (2013) suggest that testicular torsion may be ruled out if the testicle is positioned normally, if neither nausea nor vomiting is a factor, and if the patient is aged 0–10 years. Meanwhile, Srinivasan et al. (2011) suggest that predictive factors of testicular torsion include the absence of a cremasteric reflex, the presence/absence of nausea and vomiting, and changes in the color tone of the scrotal skin. Such predictive factors contain subjective elements, rendering their ability to exclude testicular torsion debatably.
CDUS is the most effective and convenient test in diagnosing testicular torsion. Its diagnostic sensitivity is reported to be 88.9%–100%, and its specificity is 97%–98.8% (Hazeltine et al., 2017). The venous outflow is obstructed when the degree of spermatic cord twist is less than 360°, and arterial flow disturbance is further added when the testis twists 360° or greater, leading to testicular ischemia. As time passes, the testis becomes enlarged and appears heterogeneously hypoechoic, and a decrease in perfusion of the testis or complete absence of blood flow are observed by the Doppler examination (Figures 1a and 1b). In cases of intratesticular hypoperfusion, findings of testicular swelling and diffuse hypoechoic mass indicate that (surgical) scrotal exploration should be scheduled to examine for testicular torsion (Bandarkar & Blask, 2018). In this study, all cases within the group characterized by findings of no (or diminished) intratesticular blood flow had 360° (or greater) torsion and a diagnosis of testicular ischemia. On the other hand, in the group with normal or increased intratesticular blood flow, scrotal exploration led to a diagnosis of intermittent testicular torsion in two of the four cases of testicular torsion; among the remaining two cases, one had 360° torsion but yielded no finding of testicular ischemia. As intratesticular blood flow was noted in the one remaining case, the patient was observed for approximately 20 hr, after which scrotal exploration was performed in response to a deteriorating condition. In this case, torsion of 360° or greater was observed along with testicular necrosis. In early, partial, and intermittent testicular torsion, depending on the degree of torsion, the physician may find it difficult to differentiate between testicular torsion and another condition during a clinical examination. Moreover, testicular blood flow may be preserved in such cases (Figures 2a and 2b; Baker et al., 2000; Bentley et al., 2004; Kalfa et al., 2007).

Testicular torsion in a 13-year-old boy who presented with right scrotal pain. The right testis is enlarged and appears heterogeneously hypoechoic. Also, a complete absence of detectable flow is observed.

Intermittent testicular torsion in a 5-year-old boy who presented with left scrotal pain. (a) After spontaneous detorsion, the left testicular blood flow is increased. (b) Findings at scrotal exploration show traces of twisting.
Confirmation of a symptom such as a whirlpool sign in addition to an absence of testicular blood flow leads to a more accurate sonographic diagnosis (Bandarkar & Blask, 2018), but not all doctors on duty possess sufficient experience with echo findings. There are reports that the use of a 10–20 MHz probe in a high-resolution ultrasound examination can improve the diagnostic accuracy of spermatic cord torsion (Kalfa et al., 2004). Our study divided the patients into two groups by CDUS frequency (12 MHz and ≤8 MHZ) utilized during diagnosis to compare diagnostic accuracy; however, even the use of a high-frequency ultrasonic probe failed to improve diagnostic accuracy (Tables 2 and 3).
This study had several limitations. One such limitation was that multiple resident urologists conducted CDUS evaluations. Moreover, there were no restrictions on the machines utilized. We cannot rule out the possibility that achieving diagnostic accuracy depends on the investigator’s skill with ultrasonic equipment. The study employed a small sample size, negating the possibility for a statistical assessment of the difference in diagnostic accuracy dependent upon CDUS frequency. It is necessary to increase the sample size in future studies.
Even when testicular torsion is not present, the investigator’s lack of skill may play a role when determining intratesticular hypoperfusion through CDUS. Cases with appendage torsion and epididymitis were found to have marked inflammation upon scrotal exploration. CDUS may find increased blood flow in the epididymis, for example, suggesting relatively less intratesticular blood flow. It has been suggested that one way to avoid such diagnostic pitfalls is to compare the blood flow of affected and unaffected testicles, repeatedly checking blood flow in the parenchymal cells of the testis.
Dynamic contrast-enhanced MRI and diffusion-weighted MRI are also reported to be useful diagnostic tools (Makela et al., 2011; Maki et al., 2011). The drawback is that these tests cannot be performed readily in emergency outpatient settings.
Regarding prognosis for testicular preservation in cases of testicular torsion, reports indicate that testicular atrophy occurred following all surgical cases, either occurring gradually or else induced by a torsion of over 360° occurring more than 24 hr following the original onset of symptoms (Tryfonas et al., 1994). These reports indicate the need for extended follow-up.
Conclusion
The results of our study suggest that testicular torsion was present in about 30% of cases in which testicular blood flow was observed with CDUS performed by doctors on duty. We considered that these cases represented intermittent, or early-stage, testicular torsion. The length of testicular ischemia time greatly affects subsequent testicular function. In this study, the sensitivity of CDUS performed by doctors on duty was about 70%, suggesting that scrotal exploration should be performed promptly even if testicular blood flow is observed and testicular torsion is suspected from medical history, body findings, and/or urinalysis.
Scrotal exploration should be scheduled as quickly as possible when testicular torsion is suspected during clinical visits when there is no physician experienced in diagnostic ultrasound available to perform CDUS.
Footnotes
Consent for Publication
The reported approval was obtained from the Hospital Research Ethics Board of Dokkyo Medical University Saitama Medical Center (Approval number: 1881).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.