
Abstract
The number of cases of aggressive prostate cancer is increasing. Differentiating between aggressive and indolent cases has resulted in increased difficulty for the physician and patient to decide on the best treatment option. Due to this challenge, efforts are underway to profile genetic risk for prostate cancer aggressiveness, which may help physicians and patients at risk for developing aggressive prostate cancer to select an appropriate treatment option. This study explores patients’ interest in receiving genetic results, preference for how genetic risk information should be communicated, and willingness to share results with adult male first-degree relatives (FDRs). A nine-item survey was adapted to assess their beliefs and attitudes about genetic testing for prostate cancer aggressiveness. In addition, participants (n = 50) responded to hypothetical scenarios and questions associated with perceived importance of risk disclosure, preferences for receiving genetic risk information, and sharing of results with FDRs. As the hypothetical risk estimate for aggressive prostate cancer increased, patients’ willingness to receive genetic risk information increased. This study found that most patients preferred receiving genetic risk education in the form of a DVD (76%), one-page informational sheet (75%), or educational booklet (70%). Almost all patients (98%) reported that they would be willing to share their test results with FDRs. The results of this study highlight prostate cancer patients’ desire to receive and share genetic risk information. Future research should focus on assessing the long-term benefits of receiving genetic information for prostate cancer patients and implications of sharing this information with FDRs.
Prostate cancer is the leading cause of cancer incidence and second leading cause of mortality among men in the United States (Cancer Facts & Figures, 2018).The incidence of metastatic prostate cancer has increased from 702 cases in 2004 to 1,345 in 2013 (92% increase) among men between the ages of 55 and 69 years (Weiner et al., 2016). The number of cases of aggressive prostate cancer, which refers to prostate cancer that rapidly develops, grows, and spreads, are on the rise (Weiner et al., 2016). Identifying which prostate cancers are aggressive remains difficult, thus complicating treatment decisions (Punnen et al., 2015). Unfortunately, the prostate-specific antigen (PSA) test cannot reliably distinguish aggressive from indolent (i.e., slow-growing, low-risk) cases (De La Calle et al., 2015). Efforts are underway to profile genetic risk for prostate cancer aggressiveness, which will help physicians and patients most at risk for developing aggressive prostate cancer select an appropriate treatment option. Currently, there are a few clinical biomarkers for aggressiveness, such as PSA, Gleason score, and clinical stage. However, these combinations are not accurate enough to determine treatment plans. Genetic variations, also known as risk single nucleotide polymorphisms (SNPs), appear to have limited clinical value for prognosis (Shui et al., 2014). However, RNA-based gene expression profiles from tumor tissue are more commonly used for predicting outcomes of prostate cancer.
Studies published in the past 5–10 years have emphasized the importance of informed decision making to help patients make scientifically sound treatment decisions that align with their preferences and values (Bowen et al., 2011; Hoffman et al., 2017; Leader et al., 2012; Owens et al., 2016). Examples of sound treatment options for early prostate cancer include watchful waiting (i.e., active surveillance), radical prostatectomy, radiation therapy, chemotherapy, and hormone therapy. Radiation and hormone therapy are especially common for aggressive prostate cancer that has spread beyond the prostate (Rusthoven et al., 2016). Informed decision making also requires awareness of treatment options, the associated risks and benefits, and patient–provider communication to ensure the decision is consistent with the patient’s/family’s values (Braddock et al., 1999; Volk et al., 2013). Ensuring informed and shared decision making about treatment options is critical due to possible decisional regret that some patients may feel about their choice and subsequent treatment (e.g., unpleasant side effects, which may negatively impact their quality of life; Hoffman et al., 2017).
Until the past few years, prostate cancer patients only received information about treatment options and the associated risks and benefits, with limited precision information about disease aggressiveness. Biomarkers are a promising tool to help identify whether patients have a clinically significant predisposition for aggressive prostate cancer. Using this information, patients can be stratified by risk to better determine the appropriate treatment. A number of studies reported that SNPs in genes such as AKT3 (minor allele frequency or MAF of 0.18), CYP17A1 (0.40), LHCGR (0.49), ESR2 (0.03), PRKCQ (0.15), HIF1A (0.04), MMP16 (0.12), and EGFR (0.39) may be biomarkers for aggressive cases (Fraga et al., 2014; Lavender et al., 2012; Lin et al., 2013; Robles-Fernandez et al., 2017). However, as already mentioned, these SNPs appear to have limited clinical value for prognosis. RNA-based gene expression profiles from tumor tissue are more commonly used for predicting prostate cancer outcomes. There are three gene expression-based tests for prognosis of prostate cancer available: Decipher (GenomeDX, Vancouver, Canada), Oncotype DX Prostate (Genomic health, CA), and Prolaris (Myriad Genetics Inc., UT; Cullen et al., 2015; Cuzick et al., 2011; Erho et al., 2013). These tests are designed for clinically low-risk prostate cancer patients.
As the use of clinical genetic data increases, questions about how to use this information to best improve patients’ health and decision making have been raised (Kaphingst et al., 2018). For information to be useful, it should be delivered with clinically actionable steps that facilitate well-informed decisions about treatment approaches. Clinically actionable information in this setting refers to information that leads to a specific course of action associated with choosing an appropriate treatment regimen for prostate cancer that is right for the individual. Incorporating and understanding individual patient preferences for receiving this information may guide the development of decision support tools and assist patients and physicians in making an informed decision about treatment.
At least five studies have examined cancer patients’ interest in and the perceived psychosocial and behavioral impact of receiving genetic test results (Andrykowski et al., 2010; Aspinwall et al., 2018; Lipkus et al., 2004; O’Neill et al., 2008; Sanderson et al., 2009). For instance, Andrykowski et al. (2010) reported women were less enthusiastic about receiving genetic information about breast cancer risk that did not provide a specific course of action for treatment and believed this information could be harmful by increasing anxiety and decisional conflict among patients. Aspinwall et al. (2018), however, reported the potential benefits of receiving genetic test results, such as patients being better prepared to manage their cancer risk and more motivated to improve their prevention behavior. Specifically, the information that patients received from the genetic test results presented to them via a counseling session empowered them to manage their cancer risk. Lipkus et al. (2004) explored the extent to which genetic test results associated with lung cancer susceptibility received by smokers affected perceived risk of lung cancer and whether the results increased motivation for smoking cessation. Results showed that there was no association between receiving the genetic test result and engaging in written materials/telephone counseling, which included information on susceptibility to lung cancer, risks of smoking/benefits of quitting, and discussion of test result. O’Neill et al. (2008) found a high level of interest among smokers who were blood relatives of patients with lung cancer in receiving information about genetic susceptibility testing for lung cancer via the internet. Similarly, Sanderson et al. (2009) found genetic test results for lung cancer risk delivered via internet to be reasonably well accepted among smokers.
No published studies have assessed patients’ interest in receiving genetic test results for aggressive prostate cancer risk. Whether and how patients share this information with their unaffected first-degree relatives (FDRs; e.g., male biologic siblings and adult biologic sons) is unknown. Considering FDRs is important because family history contributes to the increased risk for prostate cancer among men. Men who have a father, brother, or son who has had prostate cancer are at increased risk for prostate cancer. Understanding patients’ preferences for receiving genetic results for aggressive prostate cancer risk and their plans to share results with FDRs may lead to increased genetic testing and well-informed treatment decisions. Since FDRs are most impacted by genetic testing information, we decided to limit the sharing of risk information to them. The current pilot study sought to explore prostate cancer patients’ interest in receiving genetic results, preference for how genetic risk information should be communicated, and their willingness to share results with unaffected adult male FDRs.
For the current study, a series of hypothetical scenarios were developed to assess patients’ preferences for receiving genetic risk information regarding prostate cancer aggressiveness. Hypothetical scenarios have been used in previous studies as a tool for examining cancer treatment decision making and decisions regarding uptake/use of genetic information (Andrykowski et al., 2010; Brewer et al., 2009; O’Neill et al., 2007). Based on the benefits of genetic testing identified in previous studies, it was expected that prostate cancer patients would be more receptive toward receiving risk information associated with aggressive prostate cancer when they perceived the risk to be substantive and that they would be willing to share this information with FDRs if they thought the genetic risk information would be useful for their family members.
Methods
Recruitment
This study was approved by the University of South Florida Institutional Review Board (Study # CR4_100796). A total of 50 patients participated in this study. Participants for this pilot study were prostate cancer patients who were treated at Moffitt Cancer Center in Tampa, FL, and consented between February 2003 and October 2009. These patients were recontacted between 2012 and 2013 from a larger prostate cancer epidemiological study (Das et al., 2016). As background, the larger study included prostate cancer patients (n = 1,218) recruited at the genitourinary (GU) clinic at Moffitt Cancer Center. Eligibility criteria included males (a) between the ages of 18 and 90 years, (b) with a clinical diagnosis of prostate cancer within the past 12 months, and (c) no previous history of other cancers with the exception of basal and squamous skin cancer. Participants were enrolled after signing an informed consent form for study participation and future contact. The first 50 patients who agreed to be recontacted were participants for this pilot study and were given an additional survey to complete.
Study Instrument
A nine-item survey from a prior study of breast cancer patients, which focused on genetic risk for cognitive impairment (CI) following chemotherapy (Andrykowski et al., 2010), was adapted to assess beliefs and attitudes about genes and genetic testing for prostate cancer aggressiveness. The survey can be found in Appendix A. The relevant survey questions that were used for this study included Questions 2, 3, 4, 7, and 8. The original survey included two different hypothetical clinical scenarios varying in genetic-related risk of CI and severity of CI after chemotherapy. Information on the importance of being told this genetic information and the impact on the decision to receive chemotherapy was obtained in that survey. The hypothetical scenarios used in this study were created by the research team leveraging literature on breast cancer (Andrykowski et al., 2010) and lung cancer/tobacco (Lipkus et al., 2004; O’Neill et al., 2008; Sanderson et al., 2009). These hypothetical risk scenarios were presented to the patients after treatment.
Sociodemographic and clinical information
Participants reported their age, race/ethnicity, education, and family history of prostate cancer.
Perceived importance of risk disclosure
Three items used a hypothetical scenario to assess participants’ interest in receiving genetic risk information about the chances of developing an aggressive form of prostate cancer in the future. For each item, participants were asked to imagine that their doctor knew that they possessed a genetic profile that made it likely to have a 10%, 30%, or 50% higher chance of having the aggressive form of prostate cancer compared to a patient without the genetic profile. Participants were asked how important it would be for the doctor to tell them this information before beginning treatment, using a scale ranging from 1 (not important at all) to 5 (extremely important). Each of the three scenarios was identical other than the risk percentage presented.
Preferences for receiving genetic risk education
Participants also reported their preferred format for receiving genetic risk information. Participants could select as many of the following formats as they desired: one-page informational sheet, detailed educational booklet, brief DVD, in-person consult with a health professional, and information session with a health professional by phone.
Dissemination of results to FDRs
One question assessed participants’ willingness to share genetic test results with their unaffected adult male FDRs if the results provided information about the chances their relatives may develop the aggressive form of prostate cancer in the future (response options: yes, no). A separate question assessed whether the participant would be willing to share contact information of male FDRs with researchers for future studies (response options: yes, no).
Data Analysis
A repeated measures analysis of variance test was conducted to examine the variability in the perceived importance of receiving information about varying levels of risk for aggressive prostate cancer (10%, 30%, and 50%). Wilcoxon rank sum tests were conducted to examine sociodemographic and clinical characteristics associated with the perceived importance of receiving information at each level of risk. Descriptive statistics were conducted to characterize preferences for each educational tool format as well as to determine whether participants would share genetic test results with their FDRs.
Results
Demographics
Participant characteristics are presented in Table 1. Participants’ average age was 61.3 years. Most participants were White (86%), had at least some college level education (64%), and did not have a family history of prostate cancer (72%).
Demographic Characteristics of Respondents (n = 50).

Perceived Importance of Risk Disclosure
When presented with hypothetical scenarios about possessing a genetic profile that increased their risk for an aggressive form of prostate cancer, patients generally reported that it would be important for a doctor to disclose this information. The full hypothetical scenarios can be seen in Appendix A (Questions 2, 3, and 4). Mean scores were 4.27 (SD = 0.87) for a 10% risk, 4.60 (SD = 0.57) for a 30% risk, and 4.75 (SD = 0.48) for a 50% risk. Overall, for the entire sample, perceived importance of information significantly increased (p < .001) as the risk estimate increased at all three risk levels (10%, 30%, and 50%). African American men were more likely than White men to perceive information at the 10% risk level only as more important (p = .03). No other significant associations by sociodemographic or clinical characteristics were identified at each of the other risk levels. There were no racial/ethnic differences at the higher risk levels, 30% and 50%. Figure 1 compares the perceived importance of receiving genetic information at varying risk levels for men by race.
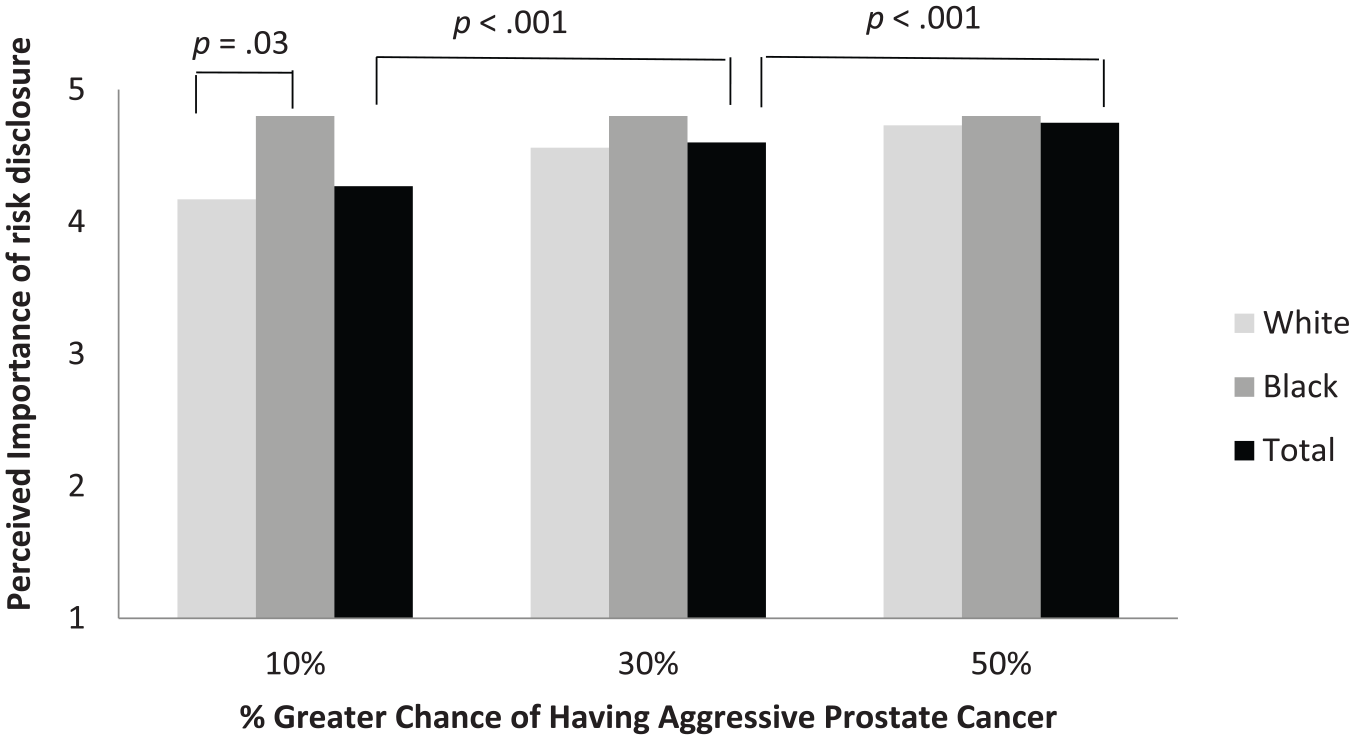
Mean perceived importance of receiving genetic profile information before initiation of treatment.
Preferences for Receiving Genetic Risk Education
As presented in Figure 2, a majority of prostate cancer patients preferred to receive genetic risk education in the form of a brief DVD (76%), a one-page information sheet (75%), or a detailed educational booklet (70%). Consultations with health professionals via phone or in person were less desired by patients (49% and 46%, respectively). Patients were also asked if there were additional ways they would like to receive this information. The majority of the patients who responded (17 of 19) did not have any additional preferences. One patient identified the internet and one patient identified email as their preferred method for receiving genetic risk information.

Preferences for receiving genetic risk education.
Dissemination of Results to FDRs
Most prostate cancer patients reported that they would share their genetic test results with their unaffected adult male FDRs (43 of 44 respondents; 98%) and would share contact information of adult male FDRs with researchers for future studies (40 of 43 respondents; 93%). Table 2 summarizes the results of patients’ willingness to share genetic risk information with others.
Receptivity to Sharing of Results With First-Degree Relatives.

Note. Table includes data for nonmissing responses only.
Discussion
This study explored prostate cancer patients’ interest in receiving genetic test results, preference for how genetic risk information should be communicated to them, and their willingness to share their results with other adult male FDRs. Findings highlighted that patients expressed interest in and understood the value of receiving genetic risk information associated with aggressive prostate cancer. As the hypothetical risk estimate for aggressive prostate cancer increased, patients’ willingness to receive genetic risk information increased. Andrykowski et al. (2010) reported similar results when evaluating hypothetical situations posed to breast cancer survivors and healthy women who had not had breast cancer. Women’s interest in genetic information about risk for CI from chemotherapy was greater when there was information that suggested the likelihood and severity of CI were high. Other studies have also reported individuals’ willingness to receive genetic risk information associated with cancer (Cruz-Correa et al., 2017; Pasacreta, 2003; Quinn et al., 2010; Schwartz et al., 2005; Sussner et al., 2015; Vadaparampil et al., 2011; Wang & Miller, 2008). Individuals may be willing to receive genetic risk information because they believe that it will reduce uncertainty about cancer treatment options or because of their desire to help family members become more aware of the risks. In addition, the results from this study found that, among African American patients, perceived importance of receiving genetic information was comparably high at all three hypothetical risk levels. This differential finding may reflect the perceived importance of or perceived susceptibility to prostate cancer among African Americans.
This study found that more patients preferred receiving genetic risk education in the form of a DVD, one-page information sheet, or detailed educational booklet compared to receiving education from a health professional. This finding may be due to these resources being available at a lower cost compared to the cost of an appointment with a health-care provider. Another reason for this finding could be the possibility for patients to view a DVD or written information on their own time. These findings are consistent with previous studies that have suggested the use of education materials to help individuals make decisions regarding treatment options (Andrykowski et al., 2010). As such, these findings support the use of education materials, a less resource-intensive approach compared to in-person education by health providers.
Almost all patients in this study reported that they would share their test results with unaffected FDRs. FDRs are interested in genetic testing for cancer susceptibility due to wanting to learn about their children’s risk, increase use of cancer screening tests, and take better care of themselves (Cormier et al., 2002; Gwede et al., 2015; Lerman et al., 1995).These perspectives suggest FDRs would be receptive to receiving information associated with genetic susceptibility for prostate cancer. FDRs’ willingness to receive genetic testing information could make them more likely to undergo genetic testing themselves, which would allow doctors to identify these high-risk individuals and offer specific screening guidelines to increase the possibility of early curative treatment for prostate cancer.
The results from this study have implications for prostate cancer treatment decisions and screening decisions among unaffected FDRs. Since patients want to be made aware of genetic risk for aggressive prostate cancer, potential treatment options for aggressive prostate cancer may be more likely considered. The development of educational tools can be used to help doctors and patients make an informed or shared decision regarding treatment. These tools can especially be targeted toward African American men due to their increased awareness of their risk for prostate cancer and their desire to be informed. Information from genetic test results must be presented in a format that is easy to understand and preferred by patients. This information also can help FDRs when making an informed decision about getting screened for prostate cancer (Davis et al., 2014). Patients’ willingness to share test results with their FDRs shows that patients are willing to provide any information to FDRs that may be helpful to them in the future (Gwede et al., 2015).
This study has multiple strengths. First, the majority of the patients in this study were between the ages of 55 and 69 years, which is the age range where metastatic prostate cancer is seen to increase the most (Weiner et al., 2016). This group of patients may have heightened potential disease progression and as such have high interest in sharing genetic risk information. Second, these findings provide support to move forward with the development of a decision aid as genetic risk information for prostate cancer aggressiveness becomes clinically actionable. Limitations for this study include (a) limited diversity of sample (86% White), (b) use of hypothetical scenarios, (c) a small sample size (n = 50), (d) patients being drawn from a single institution (cancer center), and (e) lack of a web-based option for receiving genetic risk information. The use of hypothetical scenarios is less than ideal since we are not able to assess the patients’ actions. However, understanding how patients might perceive these scenarios is important since it adds to the knowledge base of perceived importance of risk disclosure among this population. As noted, one limitation for this study is the lack of an internet-/web-based option for preferences for receiving genetic risk information among patients. However, one patient did identify the internet as an additional preferred method of receiving this information when asked to provide additional modalities. Given the increased use of web-based decision aids for prostate cancer, patients may prefer to receive information through this avenue as well if given the option.
Nevertheless, taken together with other literature, the results of this study emphasize the desire of prostate cancer patients to obtain genetic risk information to help determine the best treatment option for their condition. Future research should focus on assessing the long-term benefits of receiving genetic risk information for prostate cancer patients. Future research associated with prostate cancer genetic testing should also include more African American patients to better understand the attitudes and beliefs of the most at-risk group affected by prostate cancer.
Supplemental Material
PCa_Genetic_Beliefs_Manuscript_Clean_suppl – Supplemental material for Exploring Prostate Cancer Patients’ Interest and Preferences for Receiving Genetic Risk Information About Cancer Aggressiveness
Supplemental material, PCa_Genetic_Beliefs_Manuscript_Clean_suppl for Exploring Prostate Cancer Patients’ Interest and Preferences for Receiving Genetic Risk Information About Cancer Aggressiveness by Siddhartha Roy, Clement K. Gwede, Teri L. Malo, Courtney L. Scherr, Selina Radlein, Cathy D. Meade, Susan T. Vadaparampil and Jong Y. Park in American Journal of Men’s Health
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.