
Abstract
To understand prostate cancer (PCa) specialists’ views about prostate cancer support groups (PCSGs), a volunteer sample of Canada-based PCa specialists (n = 150), including urologists (n = 100), radiation oncologists (n = 40), and medical oncologists (n = 10) were surveyed. The 56-item questionnaire used in this study included six sets of attitudinal items to measure prostate cancer specialists’ beliefs about positive and negative influences of PCSGs, reasons for attending PCSGs, the attributes of effective PCSGs, and the value of face-to-face and web-based PCSGs. In addition, an open-ended question was included to invite additional input from participants. Results showed that PCSGs were positively valued, particularly for information sharing, education and psychosocial support. Inclusivity, privacy, and accessibility were identified as potential barriers, and recommendations were made for better marketing PCSGs to increase engagement. Findings suggest prostate cancer specialists highly valued the role and potential benefits of face-to-face PCSGs. Information provision and an educational role were perceived as key benefits. Some concerns were expressed about the ability of web-based PCSGs to effectively engage and educate men who experience prostate cancer.
Introduction
In Western countries, prostate cancer (PCa) is the most common male cancer (Australian Government, 2013; Canadian Cancer Society, 2013; Centers for Disease Control and Prevention, 2013). Affecting 1 in 7 men, the incidence of PCa is increasing with an aging male population and improved screening (Canadian Cancer Society, 2013). Men are also living longer with PCa, and the death rate continues to be low amid increases in the number of men being diagnosed (Australian Government, 2013; Canadian Cancer Society, 2011; Centers for Disease Control and Prevention, 2013). In the absence of a known modifiable cause, for many men, PCa will be a chronic illness (Canadian Cancer Society, 2013; Jemal et al., 2009; Remzi, Waldert, & Djavan, 2004). Diverse morbidities can accompany PCa and its treatments, including erectile dysfunction and urinary incontinence; psychosocial supports are thus integral to the well-being of men who have PCa and their families (Arrington, 2010; Chapple & Ziebland, 2002; Charmaz, 1995; Fergus, Gray, & Fitch, 2002a, 2002b; Gannon, Guerro-Blanco, Patel, & Abel, 2010; Meuleman & Mulders, 2003; Navon & Morag, 2003a, 2003b; Oliffe, 2005, 2006; Wall & Kristjanson, 2005). Among an array of psychosocial oncology options, prostate cancer support groups (PCSGs) have prevailed as important community-based resources in Canada and other Western countries (Arrington, 2010; Arrington, Grant, & Vanderford, 2010; Gray et al., 1999; Gray, Fitch, Davis, & Phillips, 1996; Gray, Fitch, Davis, & Phillips, 1997; Gray, Fitch, Phillips, Labrecque, & Fergus, 2000b; Matsunaga & Gotay, 2005; Steginga et al., 2001; Zanchetta, Cognet, Xenocostas, Aoki, & Talbot, 2007). However, the sustainability of volunteer-run PCSGs have been challenged by recruitment and leadership succession issues (Oliffe et al., 2008). Relatedly, PCSGs diverse connections to cancer agencies and health care providers can influence group viability. For example, health care providers who share information at PCSGs and/or refer patients to group meetings can advance the effectiveness and reach of PCSGs. While PCa specialists are an important health care provider subgroup, well positioned to link with PCSGs in a variety of ways the perceptions and practices of PCa specialists regarding PCSGs are poorly understood. In addressing the research question, what are Canada-based PCa specialists’ views about PCSGs? This study and article offers some empirical insights to address this knowledge gap and thoughtfully consider avenues for maximizing the potential of PCSGs.
Background
In contrast to the diversity in clinical psychosocial PCa programs, PCSGs are somewhat uniform in their provision of support, with both face-to-face and virtual groups focusing on (1) educational presentations from medical experts and/or (2) group discussions about treatment options, disease management, and/or health promotion (Oliffe, Gerbrandt, Bottorff, & Hislop, 2010; Seale, Ziebland, & Charteris-Black, 2006; Thaxton, Emshoff, & Guessous, 2005). Research indicates that men attend PCSGs to learn about their disease and treatment options and side effect management from other men who have direct experience, as well as from an array of health care providers (Arrington et al., 2010; Gray et al., 1997; Klemm, Hurst, Dearholt, & Trone, 1999; Manne, 2002; Oliffe et al., 2010; Seale et al., 2006; Smith, Crane, Byers, & Nelson-Marten, 2002; Thaxton, Emshoff, & Guessous, 2005). Women partners also attend PCSGs (Bottorff et al., 2008; Thaxton et al. 2005) and the group leaders can comprise health care providers and survivors. Compared with information provision, some have argued that PCSGs are less equipped to support men’s emotional distress (Arrington et al., 2010; Coreil & Behal, 1999; Weber & Sherwill-Navarro, 2005). Although experiencing significant psychosocial concerns in relation to being diagnosed, it has also been reported that men typically adopt an “instrumental” coping style oriented to action and focus on “functionality” more than “feelings” in the context of in-person and online PCSGs (Klemm et al., 2003; Oliffe et al., 2010, Seale et al., 2006). So while many men do share ordinarily private illness experiences at PCSGs (Oliffe et al., 2010), research indicates that emotional supports are secondary motivations for attendance (Thaxton et al. 2005; Voerman et al., 2007).
The vast majority of PCSG research has focussed on the benefits and barriers to attending group meetings. Previous work detailing benefits includes an interview study of 12 men—most of whom had leadership roles in PCSGs located at Winnipeg, Toronto, and Ottawa—reporting that men derived a sense of meaning and purpose through attending PCSGs (Gray et al., 1997). Similarly, a survey of men who attended a professionally led, Montreal-based PCSG reported that the sharing of PCa experiences gave men reassurance, helped alleviate anxiety, and provided a positive outlook and perception of being involved in their treatment (Gregoire, Kalogeropoulos, & Corcos, 1997). The benefits described in these studies are confirmed elsewhere wherein PCSGs have been reported as useful in mitigating the psychosocial aspects of cancer by conveying information, empowering men with PCa, enhancing and facilitating psychosocial adjustment, and helping men and their partners cope with life after a diagnosis and treatment of cancer (Arrington, 2003; Arrington et al., 2010; Cordova et al., 2003; Gray et al., 1997; Katz et al., 2002; Manne, 2002; Steginga et al., 2001; Voerman et al., 2007; Walker, 2005; Weber et al., 2004; Zhang et al., 2008).
In terms of barriers to attending PCSGs, an interview study with 34 Canadian men and their partners led Gray, Fitch, Phillips, Labrecque, and Fergus (2000a) to suggest PCSGs were poorly attended because men typically avoid disclosure due to low perceived need for support, fear of stigmatization, the need to minimize the threat of illness to aid coping, practical necessities in the work place, and the desire to avoid burdening others. Related to this, US-based and Australian-based men’s misperceptions that PCSG meetings were geared toward emotional support of the terminally ill (Krizek, Roberts, Ragan, Ferrara, & Lord, 1999; Walker, 2005) and a sense of shame and embarrassment about sharing personal information (Smith et al., 2002; Weber, Roberts, & McDougall, 2000) were identified as barriers to attending support groups.
There is also evidence that health care providers strongly influence men’s interest in attending a “support” group. For example, health care providers’ lack of awareness of PCSGs can be a barrier (Smith et al., 2002). A survey questionnaire study of 1,224 attendees at Australian-based PCSGs confirmed that the clinician’s level of endorsement for men’s participation in PCSGs strongly influenced them to attend (Steginga, Pinnock, Gardiner, Dunn, & Gardiner, 2005). This finding led researchers to conclude that clinicians are integral to the development and implementation of support services for men with PCa (Steginga et al., 2005). A subsequent study of 36 clinicians (27 urologists and 9 radiation oncologists) by Steginga et al. (2007) identified that participants were reluctant to refer patients to PCSGs, fearing that biased viewpoints and misinformation within the groups might contribute to men’s uncertainty and decisional regret.
In summary, there is consensus that PCSGs provide important resources to men and their families; however, group sustainability can be challenged by failing to attract new attendees, which in turn reduces the capacity for group leadership succession planning (Oliffe et al., 2008). Related to this it seems that men’s resistance to attending PCSGs might stem from concerns about how the groups operate and the legitimacy of the resources that they provide. In this regard, PCa specialists are well positioned to inform men about the availability of PCSGs. While PCa specialists’ reliability for reporting what may or may not motivate PCa patients to attend a support group is debatable, their collective views about PCSGs provide important insights to thoughtfully consider avenues for maximizing the potential of PCSGs.
Subjects and Method
This study was approved by the University of British Columbia’s Behavioural Research Ethics Board Committee. The survey instrument to solicit the PCa specialists’ views was developed as a web-survey composed of a 56-item questionnaire based on Steginga et al.’s (2007) study tool. The survey items were first developed from in-depth expert stakeholder interviews with 36 clinicians (27 urologists and 9 radiation oncologists) who had provided care to men with PCa for a mean of 16 years. To confirm item relevance in an iterative approach a follow-up paper-based survey applying a 5-point Likert-type scale was completed by 30 of these participants from which key themes were identified. For the current study incorporated were five demographic questions and six sets of attitudinal items to measure beliefs about: positive influences of PCSGs, negative influences of PCSGs, reasons for attending PCSGs, the attributes of effective PCSGs, and the value of face-to-face and web-based PCSGs. Each set of attitudinal items included five to nine questions that were rated by respondents using a 5-point Likert-type scale (where 1 = strongly disagree and 5 = strongly agree). An open-ended question to provide additional information was also included. Reliabilities for the current study ranged from .72 to .94. This instrument is available on request.
In all, 150 PCa specialist respondents were recruited via existing professional contacts and the Canadian Urological Association. There was a nominal honorarium of a $50 gift card of their choice, which was mailed to respondents on receipt of the completed survey. Descriptive statistics are reported. Median scores are reported for ordinal Likert data. Responses to the open-ended questions were coded and content analyses performed to inductively derive broad descriptive categories. Respondents included 100 urologists, 40 radiation oncologists, and 10 medical oncologists. Table 1 presents descriptive data on the demographic and professional characteristics of the sample. Of 150 respondents, 82.7% (n = 124) were male and the majority of respondents practiced in British Columbia (38.0%) and Ontario (33.3%). Respondents worked in a variety of settings, including hospitals and/or cancer centers. They ranged in age from 26 to 86 years (mean age = 44.7 years) and had an average of 13.8 years’ experience working with PCa patients. The majority (62.0%) reported formally presenting information at PCSGs, and 78% indicated that they had referred patients to PCSGs.
Demographic & Professional Characteristics of the Study Sample.
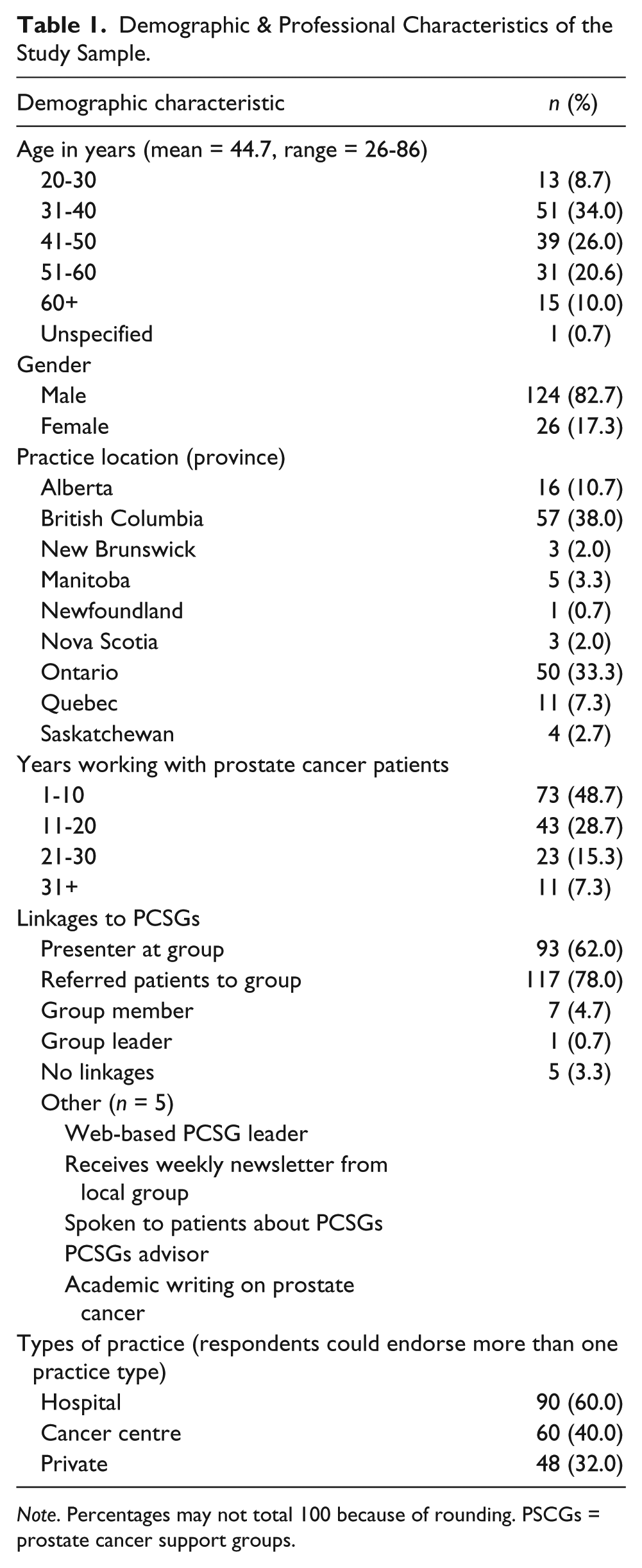
Note. Percentages may not total 100 because of rounding. PSCGs = prostate cancer support groups.
Results
Features of PCSGs That Positively Influence Men’s Adjustment to PCa
Respondents provided ratings of seven features of PCSGs that were potentially positive influences on men’s adjustment to PCa (Figure 1). Ratings of these features were uniformly high (median of five). All seven characteristics (i.e., community support, reassurance, social identity, sharing experiences, emotional support, and providing information) were identified as important benefits. While friendship was rated the lowest of the items, sharing experiences and emotional support were highlighted as the strongest factors positively influencing men’s adjustment to PCa.

Positive factors how prostate cancer support groups influence men’s adjustment to prostate cancer.
Features of PCSGs That Negatively Influence Men’s Adjustment to PCa
Specialists rated nine items related to possible negative influences of PCSGs including, meeting with dominant members who push their own views, dissemination of inaccurate information, hearing negative experiences, creating conflict over treatment decisions, promoting a specific clinician, creating confusion, supplying irrelevant information, causing confrontation, and promoting a single therapy (Figure 2). PCSG meetings with dominant members, dissemination of inaccurate information, and hearing negative experiences were identified as the three leading negative influences of PCSGs affecting men’s adjustment to PCa. The median response for the other six items was 3 (neutral) with no specific negative factors being identified as particularly influential. In addition, some negative influences were apparent in the open-ended responses discussed below.

Negative factors how prostate cancer support groups influence men’s adjustment to prostate cancer.
Reasons for Attending PCSGs
The items most strongly endorsed by PCa specialists as the reasons that men attended PCSGs were to discuss PCa treatments and to gain information (median of 5; see Figure 3).

Reasons why men choose to attend a prostate cancer support group.
Reasons for Not Attending PCSGs
Perceived reasons for not attending PCSGs were assessed with seven items. Privacy issues was the most clearly endorsed reason for not attending PCSGs (median of 5), followed by ignorance of PCSGs (Figure 4). Items including “no need,” “having enough information,” and “a desire to move past the PCa experience,” were also highly endorsed by PCa specialists (median of 4) as reasons why some men might prefer not to attend PCSGs.
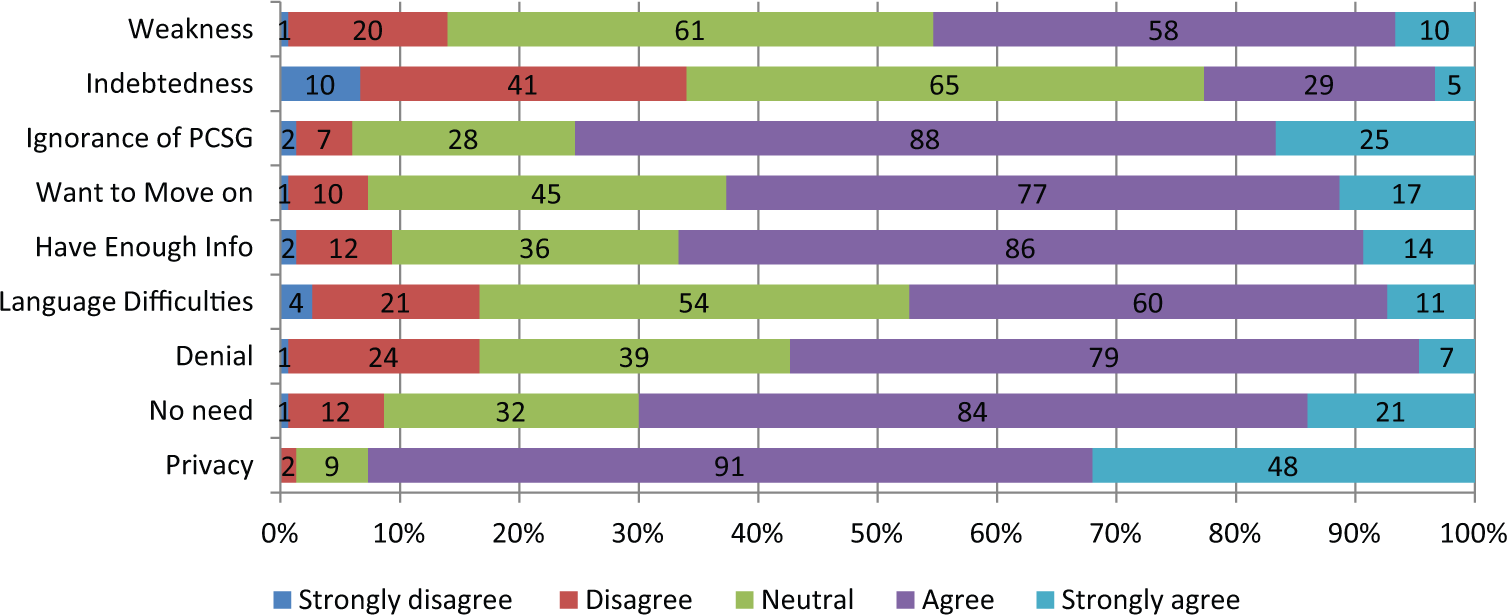
Reasons why men choose not to attend a prostate cancer support group.
Characteristics of Effective PCSGs
Respondents rated items to assess their views on the characteristics of effective face-to-face PCSGs. Avoiding bias by not promoting one view of treatment, a range of different health care providers’ input, being patient-driven, and diversity of therapies discussed were the most highly endorsed characteristics of effective PCSGs (median rating of 5; Figure 5). Supported by other health care providers, having a trained facilitator, and support from health organizations were also generally agreed as keys to success (median rating of five).

Key factors for the effectiveness of an in-person prostate cancer support group.
Characteristics of Effective Web-Based PCSGs
Provision of summarized PCa information, the use of multimedia evidence-based health care provider presentations, and the facilitation of camaraderie were identified as the most essential features of effective web-based PCSGs (Figure 6). The findings suggest that specialists are most concerned with the accuracy and interactive capacity of the information made available online.

Key factors for the effectiveness of a web-based prostate cancer support group.
Additional Commentary
Thirty-four respondents shared additional insights via written comments. Table 2 presents the results from the content analysis of the open-text comments. In summary, the main cautions related to online PCSGs and prostate specific antigen advocacy. Online PCSGs were predicted to encounter similar shortcomings, and they were suggested to augment rather than replace face-to-face meetings for a variety of reasons including older men’s reduced access to online resources. In terms of endorsements and suggestions for promoting the work of PCSGs, respondents offered a range of ideas, including messaging individual clinicians about the groups and supplying brochures to clinics that patients could take with them.
Main Endorsements and Cautions From Open-Ended Question.

Discussion
The results from the current study provide important insights to PCa specialists’ awareness of the benefits of PCSGs for men with regards to emotional support underpinned by the sharing of personal experience. Men are typically underrepresented as seekers of psychological support after cancer (Steginga et al., 2008) and a recent U.S. study indicated that PCa patients are approximately 30% less likely than breast cancer patients to have discussed emotional and social concerns with their health care provider (Forsythe et al., 2013). In light of these findings it may be that although PCa specialists appear to understand and endorse the benefits of face-to-face PCSGs, emotional and social care, and therefore raising patient awareness about support groups is not necessarily a priority. That said, given that many men with PCa report unmet needs for support with regards to fears about the cancer returning or spreading and worry about “significant” others (Lintz et al., 2003; Smith et al., 2007; Steginga et al., 2001), PCSGs present as a valuable but potentially underused support program.
Contrasted within the current study findings that sharing experiences and emotional support were the most positive influences of PCSGs on men’s adjustment, PCa specialists rated information as men’s primary motivation for attending groups. Interestingly, the key reasons endorsed as potentially negative effects of support groups including online groups, centered on misinformation. This may reflect the uncertainty that persists about the optimal treatment approach for PCa, the expanding array of treatment options and regimes, and from this, clinicians concerns about supporting men’s decision making in the clinical encounter. Men with PCa often report high decisional conflict that for some persists over time (Steginga, Occhipinti, Gardiner, Heathcote, & Yaxley, 2004), and men do report others cancer experiences, both positive and negative, as influencing their treatment choices (Steginga et al., 2002). Hence, this is a highly salient clinical issue for specialists in these men’s care.
There was less agreement on the value of PCSG in terms of social interaction and helping other men with PCa, suggesting that some PCa specialists believe the group format of PCSGs may be unappealing to men and dissuade them from attending. These views may also suggest that PCa specialists do not anticipate men to be long-term attendees.
The overarching endorsement of specialists for face-to-face PCSGs suggest some shifts to Steginga et al. (2007) findings which highlighted specialists’ concerns about the potential for misinformation. Such subtle changes are likely influenced by an array of factors including specialists’ direct exposure to PCSGs, increased clinical emphasis on shared treatment decision-making, and the growth and research fundraising activities of groups more generally. While specialists’ concerns about misinformation may be more focused on web-based resources including online PCSGs, face-to-face groups may need to dissect out and better define and focus their role in decision and information support if they are to further build specialist support and referral to their groups and programs.
Although this study is explorative, identified were some variations with respect to PCa specialist views about PCSGs. These findings as well as views that a lack of knowledge about PCSG might obscure PCSGs as a potential resource for men indicate that efforts are needed to raise awareness about PCSGs and its potential value in targeted and tailored communications to PCa specialists and men in the community. Engaging PCa survivors who have attended PCSGs to challenge assumptions and misconceptions about PCSGs that are barriers to attendance is likely to be helpful. The positive experiences of other men can provide powerful examples to overcome fears among potential attendees. However, a parallel educational initiative to ensure that PCa specialists are well informed about PCSGs is also needed. The consideration of PCa specialists’ personal perspective is essential in the planning and implementation of this type of initiative.
The current study limitations include recognition that the reliability of PCa specialists to report what may or may not motivate patients to attend a PCSG is debatable. Moreover, PCa specialists’ perspectives about PCSGs are one among many potentially diverse health care provider views. Therefore, acknowledged also are the limits in terms of generalizability in describing the viewpoints of a small Canada-based sample of a PCa specialists. Nonetheless, these limitations provide important direction for future studies, which might include large international multisite studies integrating qualitative interviews to more fully contextualize the findings offered in the current study.
While the PCSG sustainability issues raised by Oliffe et al. (2008) talked to the challenges connecting to non-profit cancer agencies, the findings from the current study reveal the PCa specialists as allies with significant potential for advancing PCSGs, especially by raising awareness with potential attendees. In this regard, formalizing collaborations might be mutually beneficial whereby a steady flow of new PCSG attendees can be mustered and the burden on clinical psychosocial oncology services further reduced.
Footnotes
Acknowledgements
Special thanks to Canadian Urological Association for their assistance with recruitment.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was made possible by the Canadian Institutes of Health Research (Grant No. 11R06913).