
Abstract
This paper reports on results from research conducted on health behaviors undertaken of men. Health behavior is one of the determinants of our health. The way in which people care for their health affects not only their health, but also their well-being, quality of life, and work ability. The lifestyle and health behavior have a significant impact on health, whereas a lack of pro-health behavior may cause the risk of many diseases and mortality, especially among men. The aim of the study was to define the determinants of positive health behaviors among men aged 20–65, active on the labor market.
To check the attitudes of men toward health and health behavior, a questionnaire-based research has been carried out among 600 men active on the labor market. Several tools were used: Positive Health Behaviour Scale (Woynarowska-Sołdan & Węziak-Białowolska, 2012), Work Ability Index (Tuomi et al., 1998), work–life balance—with the Copenhagen Psychosocial Questionnaire (subscale “Work-home conflict”) (Kristensen & Borg, 2005), Multidimensional Health Locus of Control (Wallston & Wallston, 1978, in polish adaptation Juczyński, 2001), Inventory for Psychological Sex Assessment (Kuczyńska, 2012) and Personal Values (Juczyński, 2001), and questionnaire “Work conditions” (developed in CIOPPIB).
These studies have shown which factors determine their health behavior. The positive health behaviors of men were associated with good economic status, high self-assessment of care for health, positive opinions about life and work, and masculinity. They were also white-collar workers with good work ability.
Keywords
Health behaviors are an important factor shaping and directly affecting health, alongside genes, living environment (including the work environment and conditions), and medical care and are defined as activities undertaken by humans in order to maintain, achieve, or recover good health as well as prevent disease. Health behaviors reflect the health-related beliefs of an individual. Some of the typical health behaviors are regular physical activity, balanced diet, and vaccinations (Short, Mollborn, 2015)
The method in which individuals take care of their health (i.e., whether they engage in health-promoting behaviors—including rational nutrition, physical activity, and avoidance of unhealthy behaviors—smoking, excessive alcohol consumption) affects not only their health, but also their general well-being—physical and mental condition, quality of life, work–life balance, and ability to engage in professional activity (Hildt-Ciupińska, 2017).
Men perceive health and care for them a bit differently than women. According to women, care for health manifests itself, for example, in healthy nutrition, regular preventive examinations, and observation of their body. According to men, care for health is strongly associated with high socioeconomic status, and good work and life satisfaction. Caring for health is also often understood as going to the doctor, but only when symptoms appear that they cannot cope with, e.g., using the Internet (Cianciara, 2012).
The change of lifestyle to a health-promoting lifestyle enables slowing down the development of many diseases, particularly cardiovascular diseases, which are one of the leading causes of death in the world, particularly in men (White, 2011).
Men rate their health better than women, even though they use health care less often and are also more likely to adopt behaviors related to unhealthy lifestyle, which are associated with the risk of developing noncommunicable diseases, such as cardiovascular diseases, cancer, diabetes, and respiratory diseases (Zwolinsky et al., 2016).
Men are more likely to adopt unhealthy behaviors such as smoking, unhealthy eating patterns, higher alcohol consumption, and higher injury and interpersonal violence rates compared to women. Male risk behavior and underutilization of health-care services (e.g., failure to take advantage of periodic health examinations) are similar in many countries and are linked to socioeconomic factors as well as to standards of masculinity and hegemonic 1 ideals (WHO, 2018a).
In all age groups, men in Poland die more often than women. In 2017, men’s life expectancy was 74 years, and for women it was 7.8 years longer and was 81.8 years. Men’s mortality rate in Poland is higher than the average in the European Union (EU) countries in all age groups. The largest difference occurs among men aged 30–44 and 45–59, in which the threat to life in Poland is about two-thirds higher than the average in EU countries in general. Among women, differences in mortality in Poland and the EU in age groups are lower than in men and the largest surplus, around 29%, is in the age groups 45–59 and 60–74 (Statistics Poland, 2015 Wojtyniak & Goryński, 2016). Among the most dangerous “killers” of Polish men are listed: cardiovascular disease (40.9% of causes of death) and malignant tumors (25.9%).
Among the reasons for this state of affairs are mentioned factors that are related to lifestyle. Among men aged 18–79, as many as 5.2 million people are smokers. Overweight is close to 10 million people, or almost 70%, and obesity affects nearly a quarter of men. Almost 9 million men have hypercholesterolemia, but only about every third of them know about it, and only 1 million men cure it. Almost 35% men (5 million) have hypertension, but they are treated by slightly more than half of them (Wojtyniak & Goryński, 2016).
Investing in men’s health through properly planned and implemented health education can bring a variety of benefits, especially for men with the lowest socioeconomic status, doing physical work, and often shifting work (including night work) and thus exposed to many noxious factors, both inside and outside the workplace. The research results presented will be used to develop a health education program for men.
In this paper, it has been assumed that engaging in positive health behaviors proves that men take care of their health (they present “healthy lifestyle”). Thus, “care for health” is defined as healthy eating, physical activity, taking care of mental health (sleep, relaxation), maintaining safety, and avoiding risky behaviors. The objective of the study was to identify the determinants of positive health behaviors among men aged 20–65, active on the labor market in Poland.
Methods
The method used was a quantitative study. The SPZZ Positive Health Behaviour Scale (Woynarowska-Sołdam & Węziak-Białowolska, 2012) was used to measure health behaviors, including rational nutrition, physical activity, taking care of sleep, rest, and safety, as well as avoiding unhealthy behaviors—smoking, excessive alcohol consumption (the full-scale Cronbach’s α coefficient was .825, for individual subscales it ranged from .603 to .708). In addition, the respondents were asked several questions, such as regarding self-assessment of health, self-assessment of own care, and understanding of what taking care of health is (open question).
Several standard questionnaire tools were used: LWO List of Personal Values, by Z. Juczyński (2001); it consists of two parts: Symbol of happiness and Personal values (Cronbach’s α coefficient is, respectively, .78 and .76), MHLC Multidimensional Health Locus of Control Scale (Wallston et al. (1978) in the Polish adaptation by Z. Juczyński (2001)) (Cronbach’s α coefficient is .74 for external control, .69 for case impact, and .54 for influence of other people), Work Ability Index by Tuomi K, et al. (1998) (Cronbach’s α: .78), IPP Psychological Gender Inventory (Kuczyńska, 2012) (Cronbach’s α is .78 for feminity scale and .79 for masculinity scale), subscale of the COPSOQ questionnaire (Copenhagen Psychosocial Questionnaire [COPSOQ II] “Work–Life Balance” [Kristensen & Borg, 2005]), “Working conditions” questionnaire developed in CIOP-PIB Central Institute for Labour Protection – National Research Institute (https://m.ciop.pl/CIOPPortalWAR/appmanager/ciop/pl?_nfpb=true&_pageLabel=P16600139261348474174014&html_tresc_root_id=19958&html_tresc_id=300002137&html_klucz=19958&html_klucz_spis=).
In addition, for the needs of the project, a questionnaire was developed, which included personal data and questions concerning, among others, self-assessment of health and taking care of it, ailments, understanding of the term “taking care of health,” and sources of information about health.
The Study Sample
The study group consisted of polish men (N = 606) of working age (20–65 years), with different levels of education, doing physical, mental, or mixed work, from several enterprises in Poland, who agreed to participate in the study. The men represented several industries: shipbuilding, uniformed services, construction, as well as housekeeping and security services.
The selection of the study group was intentional, it was made on the basis of age (20–65 years), gender (men), and type of work (mental, physical, mixed mental and physical).
Appropriate Ethics Approval and Informed Consent/Animal Welfare Statements
Research was anonymous. Only men who voluntarily joined them took part. The research was conducted with respect for human dignity (Code of ethics for the researcher. Ethics Committee in Science. National Academy of Sciences 2017).
There is a Bioethical Commission in Poland, which is an independent institution that provides opinions and controls clinical trial projects created to ensure proper protection of human dignity during research (medical experiments) (Regulation of the Minister of Health and Social Welfare of May 11, 1999 regarding the principles of appointing and financing as well as the mode of operation of bioethics committees. http://prawo.sejm.gov.pl/isap.nsf/download.xsp/WDU19990470480/T/D19990480L.pdf). This commission checks the validity, feasibility, and plan of the clinical trial, analysis of expected benefits and risks, and correctness of the clinical trial protocol. Questionnaire research, surveys, interviews, and database analysis on health and illness are not a medical experiment. There are no relevant regulations regarding such surveys. CIOP-PIB does not have own IRB.
Statistical Analysis
To analyze the results obtained from 606 men, the following analyses were carried out:
Regressions
The model predicting the determinants of the Positive Health Behaviour Scale (SPZZ) was created using a multivariate linear regression analysis, in which the predictors were introduced by backward elimination. It is a classic regression model in which one dependent variable is predicted on the basis of several independent variables (predictors). The backward elimination method is a way of creating a model, in which the analysis is carried out first taking into account all the predictors selected by the researcher, and then eliminating from it successively those that do not affect the dependent variable in a statistically significant way. Consecutive steps involve eliminating a single predictor—the one that is statistically least important. Ultimately, this leads to a model in which all the predictors significantly predict the dependent variable.
Significance of Differences
The significance of differences between groups was determined using fraction tests (if response rates were compared) or t tests for independent study groups (if averages were compared). A fraction test is, in other words, a Z-test of the proportions between independent groups.
Reliability
The reliability of the Positive Health Behaviour Scale and all its subscales was checked using the Cronbach’s α coefficient. The reliability of the entire scale was .933. For the subscales nutrition, physical activity, safety, sleep and mental health, and caring for the body, the Cronbach’s α value ranged from .648 to .952.
Results
Characteristics of the Study Sample
The highest proportion (38%, N = 230) of the 600 men surveyed were aged 36–45; the second largest group were individuals aged 27–35 (34%, N = 206); the average age was 38.0. The average body mass index (BMI) among the respondents was 27.5; most of the men were overweight (52%, N = 315). The correct value of this index, presented by only 26% (N = 158) of the respondents, is 18.5–24.99 (25–29 is overweight, 30–34.99—first-degree obesity, 35–40—second-degree obesity).
The majority of respondents were in a relationship (83%, N = 502) and had children (70%, N = 424). The vast majority of men assessed their material situation as average or good (70%, N = 424). Nearly one-fourth of men had higher education, almost one-fifth of the respondents had bachelor’s degree, and one-fourth had secondary vocational education. Most of the men lived in cities.
The largest group of men (44%, N = 266) performed mixed work (mental and physical), and about 15% were employed in a managerial role. Shift work was carried out by about 80%, most of which were in continuous plant operation, in the 8-hr system (45%, N = 272).
The Concept of Taking Care of Health (Open Question)
According to the men surveyed, taking care of their health is first of all: healthy nutrition, physical activity, active rest, periodic medical examinations, avoiding/provoking diseases, safety (including the use of personal protection equipment during work), and avoiding noxious factors, stress, excess alcohol, and smoking.
Self-Assessment of Health
Most men (57%) rated their health as good. Very good health was presented by less than 16%; only 3% of the respondents declared bad or very bad health (Figure 1).

Self-assessment of men’s health (N = 600, in %).
Self-Assessment of Taking Care of Health
The vast majority of men (85%) declared that they took care of their health, and 15% were of the opposite opinion. With five answers to choose from (on a scale from no care at all to very good care), the highest number of men (62.4%) admitted that they “mostly take care” of their health. Undecided were less than 20%, and “not caring at all” only 1.3% (Figure 2).
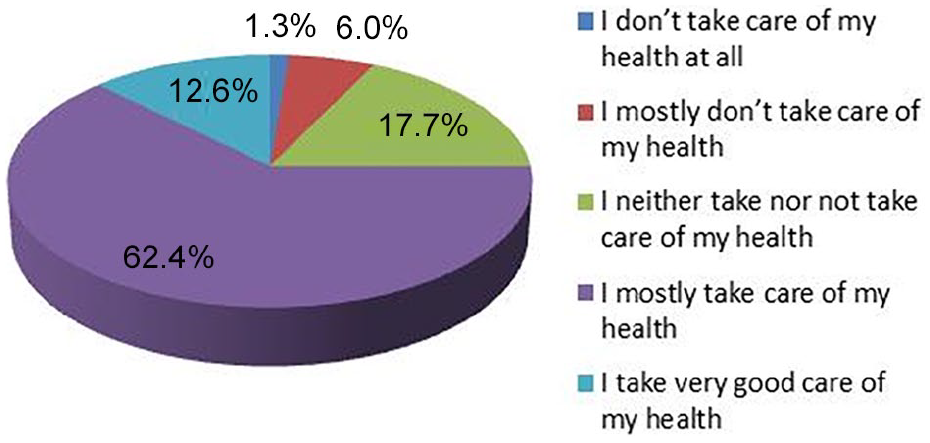
To what degree do you take care of your health? (N = 600, in %).
The answers “I mostly take care” and “I take very good care” were more often chosen by men, who were younger, assessed their health well, and were with the correct body weight.
Positive Health Behaviors
The Positive Health Behaviour Scale included 32 statements concerning health-promoting behaviors related to nutrition, body care, sleep/rest, safety, physical activity, and not engaging in unhealthy behaviors related to smoking, excessive alcohol consumption, and taking medicines without consulting a physician.
Within the entire scale, the men could obtain 111 points; the average score was 70.98 points, minimum 8, maximum 111 points. The remaining average results for each subscale are presented in Table 1.
Descriptive statistics for the Positive Health Behaviour Scale (SPZZ) (in points).
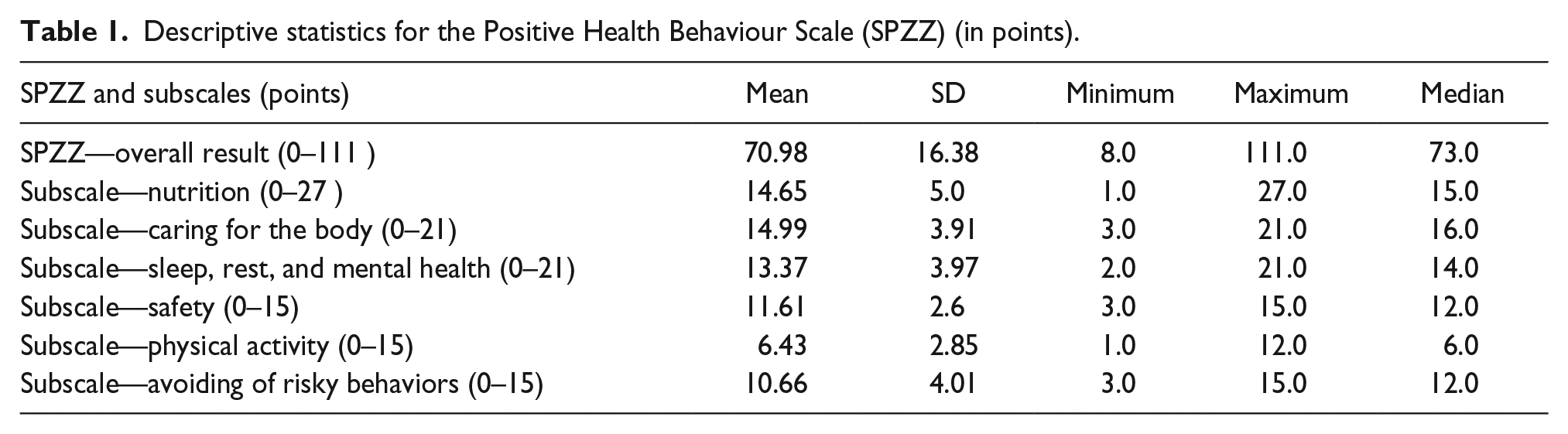
The results obtained by the respondents were divided into low (0–62 points), medium (63–79 points), and high (80–111 points). Points are divided by average and SD within the studied group. A high level of taking care of health expressed in terms of points within the range of 80–111 points with a maximum of 111 points was achieved by less than one-third of the respondents (Figure 3).

Level of taking care of health expressed by the result on the SPZZ Scale (N = 600, in %).
The men differed on the basis of certain socioeconomic and personality factors (place of residence, type of work, material situation, ability to work, gender), as well as factors such as self-assessment of health and declarations regarding physical activity and rational nutrition. A high level on the Positive Health Behaviour Scale was significantly more often achieved by men (Table 2):
Relationships (significance of differences) between selected variables and the Positive Health Behaviour Scale (SPZZ) in groups of men (N = 606, in % [N]).

p < .05.
– inhabiting cities (vs. villages),
– mental workers (vs. physical workers),
– with at least good material situation (vs. bad and very bad),
– with good and very good self-assessment of their health (vs. bad),
– declaring to spend at least 150 min per week on moderate physical activity (vs. not declaring),
– declaring rational eating (vs. not declaring),
– with good and excellent working ability (vs. poor and moderate),
– types: male and androgynous of psychological gender (vs. unspecified persons and feminine men).
Of the 32 health-promoting behaviors (Table 3), it is worth noting that only 37% of men “almost always” start the day with breakfast, which as the most important meal during the day reduces the risk of diabetes, obesity, and many other modern-age diseases.
Positive health behavior (N = 606, in % [N]).

Only 8% reduce the consumption of animal fats, which, in terms of statistics regarding mortality from heart disease, atherosclerosis, and infarctions, is a cause for concern. The oldest group of respondents do it significantly more often compared to younger ones.
Slightly more than 40% measure blood pressure once a year; men aged 46 and above do it significantly more often than their younger colleagues (Table 3).
To identify the strongest determinants for taking care of health among men, expressed by engaging in positive health behaviors, a linear regression analysis was carried out, in which the general result of the SPZZ survey was a dependent variable and independent variables (predictors) were as follows:
– age of the respondents,
– education,
– marital status,
– shift work,
– type of work (mental, physical, mixed),
– self-assessment of material situation,
– self-assessment of health,
– self-assessment of taking care of health (the level of care from very good to no care at all),
– BMI,
– health locus of control (MHLC survey scale),
– risk factors at work (harmful and noisome factors at work—CSU survey scale), stereotypical femininity and masculinity (IPP survey scale),
– intensity of the work–home and home–work conflict (COPSOC survey scale),
– list of personal values,
– Psychological Gender Inventory
– SPZZ survey scale—not engaging in risky behaviors.
The results of the regression analysis show that only four predictors significantly influence the overall health care. They are the degree of taking care of one’s own health (I do not take care at all to take great care of myself), scale of masculinity, general life optimism expressed by the scale of opinions about work and life of the questionnaire “Harmful and noisome factors at work,” and a good material situation (R2 is .468, corrected R2 is .454). This means that health is taken care of by “male” men who declare that they take good or very good care of their health, have a positive attitude toward life and work (including its conditions and safety), and believe that their material situation is at least good (Table 4).
Predictors of the Positive Health Behaviour Scale.

SE, standard error.
Discussion
The survey conducted among 606 men confirms the general trends in men’s approach to health (in Poland and worldwide). The surveyed men, similar to other reports (Public Opinion Research Center, 2016; Cianciara, 2012; Polish Central Statistical Office, 2015; White, 2011; WHO, 2018a; Wojtyniak & Goryński, 2016), rated their health and caring for it highly; their health occupies a high place in the hierarchy of values, and disease is associated mainly with powerlessness, suffering, and pain.
The most noticeable and, at the same time, worrying is the discrepancy between declarations and knowledge about health care and specific health behaviors of men, concerning nutrition, physical activity, caring for the body (including disease prevention), safety or mental health, sleep, and rest. High results in most of these areas (testifying to high care in these aspects) were reported only by about 1/3 of the respondents; the exception was the subscale of body care—here a high result was achieved by 40% of men.
Studies conducted among men identify that few of the examined men follow the basic recommendations related to nutrition (e.g., eating breakfast, limiting the consumption of animal fats or salt) and physical activity, i.e., the two most important areas related to the prevention of cardiovascular diseases, which are the main cause of premature mortality among men. Skipping breakfast is associated with an increased risk of weight gain and obesity in young adults, probably due to increased daily snacking (Baum et al., 2017). Worldwide, about 20% of young men (18–39 years old) do not meet the national recommendations for physical activity (Bauman et al., 2009). The quality of their diets is also unsatisfactory. In a study by Fryer and Ervin (2013), the percentage of calories from fast food was the highest (15.5%) among young men (20–39 years old) compared to women and men in all other age groups. Low physical activity combined with poor dietary choices result in excess weight or obesity, with estimates showing that about 37% of men aged 20–24 and 47% of men aged 25–29 in developed countries were overweight or obese (Ng, Fleming, et al., 2014).
The prevalence of risk factors for chronic diseases, including smoking, poor quality of nutrition, excessive alcohol consumption, lack of physical activity, and obesity in men, mainly young men, is high (Bauman et al., 2009, Fryer and Ervin, 2013, Ng, Fleming, et al., 2014, Ng, Freeman, et al., 2014, World Health Organisation, 2014). There is a need to reduce these risk factors, especially among young men, in order to prevent the emergence of many diseases at a later stage, including cardiovascular disease, cancer, and obesity (Ashton et al., 2015).
A large prospective cohort study in the USA (CARDIA) reported that maintaining a healthy lifestyle from adolescence to middle age (i.e., mean BMI ≤ 25 kg/m2, moderate alcohol consumption, higher healthy diet results, higher physical activity, nonsmoking) was strongly associated with a low cardiovascular risk profile at middle age (Liu et al., 2012).
According to a report by the World Health Organization (WHO [2018a]), the greatest emphasis in the group of men nowadays should be on healthy eating habits, at home, at work, and in all environments where men live; reducing smoking; consumption of alcohol and all other psychoactive substances; as well as mental health.
The factors determining the care for the health of the polish man to the greatest degree included good financial situation, positive opinions about work and life, high self-assessment of health care, and male psychological gender. Similar results were obtained by Public Opinion Research Center (2016); these studies identify that opinions on the popularity of health-promoting behaviors in Polish society were more often expressed, among others, by respondents who assessed their material situation well (70%) and individuals who declared taking care of their own health (67%).
Men who support traditional masculinity beliefs or dominant masculinity standards engage in poorer health-related behaviors and have a higher health risk than men who have a less traditional approach to gender roles (Hooker et al., 2012). The most recent WHO report (2018) emphasizes the need to change the approach to women’s and men’s health, primarily because of the huge role played by gender and the associated social roles and stereotypes in this area.
Low scores in the Positive Health Behaviour Scale in own research were more often obtained by men: in the group of 27–35 years old, living in villages, physical workers, assessing their material situation and health as bad, with obesity, assessing their health as bad or very bad, not spending about 150 min a week on moderate physical activity, not declaring rational nutrition, smoking, with poor or moderate ability to work, of feminine type, and undefined as far as the psychological gender is concerned. Health behaviors are influenced by socioeconomic capital as well. Several studies have shown socioeconomic differences in leisure-time physical activity (Lindström et al., 2001). Demographic and socioeconomic factors are among the main determinants of health, health behaviors, and health-related inequalities; these factors determine men’s health more than women’s (WHO, 2018b). There is a lot of evidence of associations between levels of economic capital (e.g., low income and self-reported financial stress) and various health outcomes (Ahnquist et al., 2012; Courtneay, 2003).
It should also be emphasized here that social factors also include industrialization, globalization, and technical progress (apart from low pay and low standard of living), which also affects lifestyle and health behavior. People move less and eat more processed food, which further worsens their health (Graham & White, 2016).
According to the WHO European Health Region Review (2013) on social determinants of health, the poorer survival rates for men are also reflected in several other factors—higher levels of occupational exposure to physical and chemical hazards, behavior related to male risk-taking standards, male health behavioral paradigms, and the fact that men visit physicians less frequently and report symptoms of disease less frequently. Low scores in the Positive Health Behaviour Scale in own research were more often obtained by men who were physical workers.
Polish physical workers with a low level of education and low health awareness are a community threatened by social exclusion in the sphere of health, and as a consequence they may have a worse position on the labor market, which indicates the need to extend the range of measures aimed at equalization of their opportunities. One of the ways to achieve this goal can be properly conducted health education and health promotion. This research allowed us to draw the appropriate conclusions and develop a health education program for men for use in enterprises.
Conclusions
Based on the conducted questionnaire research, it is stated that the surveyed men highly assess their health and care for them and they are characterized by average health care, measured by undertaken health behaviors. Men are divided into more or less caring about health in terms of demographic and socioeconomic, personality traits, in terms of health self-assessment and care, declarations of care, and also because of the ability to work.
There is a great need to implement a health education program for men—blue collar workers, less educated, and not undertaking healthy behaviors in polish enterprises.
Study Limitations
The limitation of this research is the lack of representativeness of the studied group of men and, therefore, the inability to draw more general conclusions or the possibility of a fair comparison with other studies from other countries. It would also be good to examine the control group—nonworking men—in order to compare their health behaviors depending on the amount of free time. An additional limitation is the fact that people (in their anonymous survey) overestimate themselves (want to look better). In the future, it would be better to conduct observations or case studies to better understand men’s health behaviors.
Footnotes
Authors’ Note
This paper has been based on the results of a research task carried out within the scope of the third stage of the National Programme “Improvement of safety and working conditions” partly supported in 2017–2019—within the scope of research and development—by the Ministry of Science and Higher Education/National Centre for Research and Development. The Central Institute for Labour Protection – National Research Institute is the program’s main co-ordinator.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by the Ministry of Science and Higher Education/ National Centre for Research and Development.