
Abstract
African American men have the highest prostate cancer-related mortality nationally. In response to this disparity, targeted interventions are emerging to enhance African American men’s prostate cancer (PrCA) knowledge to ensure they are equipped to make informed decisions about PrCA screening with health-care providers. African American men’s PrCA knowledge has been measured inconsistently over time with limited psychometric evidence. The factor structure of this construct in African American men is relatively unknown. This study describes the development and psychometric evaluation of an 18-item Prostate Cancer Knowledge Scale among 352 African American men. Exploratory factor analysis (EFA) was conducted using weighted least square mean and variance estimation with Geomin rotation. EFA yielded three factors: PrCA Anatomy and Screening (6 items), Risk Factors (5 items), Warning Signs (7 items) with good internal consistency reliability at KR-20 = .80 for the total scale and .64, .66, and .75, respectively, for each subscale. Factor loadings ranged from .31 to .86. The standardized root mean square residual (0.08) indicated that the factor structure explained most of the correlations. The three-factor, 18-item Prostate Cancer Knowledge Scale demonstrates that PrCA knowledge is a multidimensional construct and has utility for reliably measuring PrCA knowledge among African American men. Future research is required to confirm this factor structure among socio-demographically diverse African Americans.
Prostate cancer (PrCA) is the number one nonskin cancer among men with an estimated 174,650 men who will be diagnosed and 31,620 men who will die from the disease in 2019 (Siegel et al., 2019). African American men have PrCA morbidity and mortality at more than two times the rate of their White counterparts (Siegel et al., 2019). Myriad factors contribute to these disparities, including health beliefs and behaviors and having access to health care. None of these factors have definitive associations with PrCA morbidity or mortality (Mordukhovich et al., 2011; Taksler et al., 2012). PrCA disparities are further complicated by the ongoing debate regarding the efficacy of the prostate-specific antigen (PSA) screening exam (Kim & Andriole, 2015), which led to mixed clinical recommendations from health-care providers about screening (Fleshner et al., 2017) and an increase in patients who elect to forego screening (Gibson et al., 2016). PrCA disparities are partly explained by African American men’s lower PrCA knowledge (Dhillon et al., 2017; Owens et al., 2018). To reduce the burden of PrCA, the American Cancer Society (ACS; Wolf et al., 2010), American Urological Association (AUA; Carter et al., 2013), and the United States Preventive Services Task Force (USPSTF; Bibbins-Domingo et al., 2017) recommend that men make an informed decision with their health-care provider about whether to receive PrCA screening. Informed decision-making is when an individual understands a disease as well as risks, benefits, uncertainties, and alternatives to screening and is involved in the decision-making process to the extent that he or she desires (Briss et al., 2004). Based on this definition, many researchers identify knowledge as critical to informed decision-making (Mullen et al., 2006). PrCA knowledge is a focal point for PrCA interventions promoting informed decision-making (Ilic et al., 2015; Riikonen et al., 2018). PrCA knowledge has been measured inconsistently over time with limited psychometric evidence, particularly among African Americans, which limits generalizability across studies. Below is a review of measures used to assess PrCA knowledge among African American men.
A Review of Prostate Cancer Knowledge Measures
The Knowledge and Attitude Survey (Demark-Wahnefried et al., 1993, 1995) is a 24-item, multiple-choice questionnaire that assesses PrCA knowledge and beliefs. Scoring was based on the percentage of questions answered correctly. After administration of the Knowledge and Attitude Survey to 286 African American and White men in nine PrCA Awareness screening events in the southeastern United States, Denmark-Wahnefried et al. (1993, 1995) discovered that African American men were less likely to (a) have a regular doctor, (b) ever have a digital rectal examination (DRE) or PSA test, (c) report that a man with PrCA can lead a normal life, or (d) that men can have PrCA without symptoms. A substantial number of both African American and White men did not know race and/or heredity are risk factors for PrCA, although this number was higher in African American men (Demark-Wahnefried et al., 1993, 1995). No psychometric properties were reported for this scale (Demark-Wahnefried et al., 1993, 1995).
The Prostate Cancer Knowledge Inventory (Boehm et al., 1995) is a 11-item questionnaire designed to assess African American men’s PrCA knowledge and screening behaviors. Response categories for each item is true–false. Scores range from 0 to 11 (correct or incorrect) with higher scores indicating higher PrCA knowledge. When administered as part of a PrCA education and screening program in African American churches, the internal consistency reliability using the Kuder–Richardson Formula 20 (KR-20) at pretest and posttest in a subsample of African American men (n = 123) was .45 and .58, respectively (Boehm et al., 1995). Content and face validity were enhanced by a literature review, clinician’s expert review, and focus groups with African American men.
Smith et al. (1997) asked 556 African American men seven questions about PrCA knowledge (e.g., risk factors) based on measures developed by Boehm et al. (1995) and Demark-Wahnefried et al. (1995). Responses were grouped by low, medium, and high PrCA knowledge categories based on the number of correct items. Similar to prior studies, Smith et al. (1997) reported African American men’s PrCA knowledge was inadequate. No internal consistency reliability was reported for the scale.
Abbott et al. (1998) used a pretest–posttest design to compare PrCA knowledge in African American (n = 388) and Caucasian (n = 566) men (N = 944) as a part of a PrCA screening and education intervention in a senior health clinic. An unspecified number of questionnaire items measured three constructs: (a) etiology, (b) risk factors, and (c) clinical factors. The total score for the full questionnaire is 7. PrCA knowledge increased overall following the intervention. However, African American men were less likely than Caucasian men to correctly identify early symptoms of PrCA and the basic components of prostate screening. In the same sample, this questionnaire was used to evaluate the effectiveness of an educational PrCA screening program and identified that African American men had lower levels of knowledge about prostate etiology and clinical factors (Barber et al., 1998). No psychometric properties of the questionnaire used in studies by Abbott et al (1998) or Barber et al. (1998) were reported.
The Knowledge of Prostate Cancer Screening Questionnaire (Weinrich et al., 1998) is a six-item questionnaire developed to assess men’s knowledge about PrCA screening, symptoms, and risk factors. This questionnaire was developed by interviewing 99 primarily low-income African American men about their existing PrCA knowledge. Five cancer health professionals were used to establish content validity and the measure was pilot tested on 17 occasions. Dichotomous responses were agree or disagree and scores ranged from 1 to 6 based on the number of items answered correctly. After administration to 56 men, the total score mean was 3.75 (SD = 1.5) and the reliability was 0.61. In a sample of men (n = 319; 82% African American), Weinrich et al. (1998) assessed PrCA knowledge prior to implementation of an educational program and discovered PrCA knowledge predicts participation in PrCA screening. Internal consistency reliability of the scale using Cronbach’s α was 0.73. Content validity was established using nine subject-matter experts and construct validity was examined using factor analysis.
Steele et al. (2000) developed a 13-item PrCA Risks, Knowledge, Attitudes and Screening Practices Scale to measure self-perceived risk and knowledge, attitudes, and screening practices of older men (≥50 years). Only 2 of 13 items on the scale measured PSA screening knowledge and the second question assessed men’s awareness of PSA screening. No detailed description of the measure was provided, including the scale’s development, response options, and scoring. The PrCA Risks, Knowledge, Attitudes and Screening Practices Scale was administered via phone to two populations of men in New York: a statewide sample of 631 men (84% White) and 742 African American men (Steele et al., 2000). African American men were discovered somewhat less likely than White men to recognize their higher PrCA risk and significantly less likely to be aware of the PSA screening. No psychometric properties of this scale were reported.
To examine correlates of actual and perceived PrCA knowledge among African American men, Agho and Lewis (2001) developed an original questionnaire based on recommendations from several health authorities (e.g., ACS). The questionnaire consisted of 31 items designed to measure actual PrCA knowledge, perceived PrCA knowledge, use of prostate screening services, and demographic characteristics. The Actual Prostate Knowledge Scale (Agho & Lewis, 2001) was a 21-item self-report measure designed to determine African American men’s factual PrCA knowledge and was similar to PrCA knowledge scales developed prior to 2001 (see measures reviewed above). The Perceived Prostate Cancer Knowledge Scale (Agho & Lewis, 2001) was developed to measure participants’ subjective PrCA knowledge (e.g., I am very knowledgeable about PrCA). The authors do not report the number of items on this scale. Dichotomized responses of both scales were true–false and scored based on the percentage of correct items. In a convenience sample of 108 African American men in Florida, the men had low PrCA knowledge, actual and perceived PrCA knowledge were positively correlated, and actual knowledge was negatively correlated with age and income. Cronbach’s α for the Actual and Perceived Prostate Knowledge Scales was .87 and .81, respectively. Validity of the scales was not reported.
The Prostate Cancer Knowledge Scale (Wilkinson et al., 2003) is a 12-item self-report measure developed to assess men’s knowledge of PrCA risk factors, symptoms, prevention, screening, and treatment. Response options were multiple choice or true/false with each question also including an I don’t know response option. Scoring was based on the percentage of questions answered correctly and ranged from 0 to 100. In a sample of 835 African American men (n = 696) and women (n = 139), the Prostate Cancer Knowledge Scale was used to assess the effectiveness of a PrCA education program to improve PrCA awareness and knowledge using a pretest–posttest design. Women were included in the study because of their influence on the PrCA screening decisions of African American men. Findings identified that the education program improved PrCA knowledge. No psychometric properties of this scale were reported.
A revised Knowledge of Prostate Cancer Screening Questionnaire (Weinrich et al., 2004) was expanded from 6 (Weinrich et al., 1998) to 12 items, which measured PrCA limitations, symptoms, risk factors, side effects of PrCA treatment, and PrCA screening age guidelines. Response options were true/false or I don’t know. Total scores ranged from 0 to 12 based on the number of correct items. In 2002, the scale was administered to nine men to assess face validity (Weinrich et al., 2004). In a sample of 81 low-income men (60 African Americans, 21 Caucasians), the total mean score was 6.6 (SD = 3.0), the median score was 7, and the internal consistency reliability using the KR-20 was 0.77 (Weinrich et al., 2004). In a sample of 27 men, test–retest reliability using Cohen’s κ was 0.55. Construct validity of the 12-item questionnaire using factor analysis resulted in a unidimensional 12-item factor structure by retaining items loading at 0.35 or greater (Weinrich et al., 2004).
Cormier and colleagues created the PrCA Knowledge Scale (Cormier et al., 2002) by combining 20 items from three aforementioned scales (Boehm et al., 1995; Demark-Wahnefried et al., 1995; Weinrich et al., 1998). Eleven items were from the PrCA Knowledge Screening Questionnaire (Weinrich et al., 2004). Six items were from the PrCA Knowledge Inventory (Boehm et al., 1995). Three multiple-choice items were from the Knowledge and Attitude Survey (Weinrich et al., 1998), which also assessed beliefs (three items on screening, three items on treatment, one item on perceived risk). Constructs include Prostate anatomy and function (two items), PrCA risk factors (six items), PrCA screening (nine items), and PrCA symptoms (four items). Response categories for each item are true, false, and I don’t know. Scoring was calculated by summing item scores (i.e., 1 point per correct item) for a total of 20 points (ranging 0–20). Response categories for the perceived risk item included being less than, equal to, or more than the risk of the average man (Cormier et al., 2002). When administered to 139 men (92% White) who were brothers and sons of PrCA survivors, PrCA knowledge was high overall, but race as a risk factor and PrCA warning signs were poorly understood (Cormier et al., 2002). No psychometric properties of Cormier et al.’s PrCA Knowledge Scale were reported.
Magnus (2004) developed a five-item Prostate Cancer Knowledge Scale with guidance from educational information released by the ACS. Items specifically focused on risk factors for multi-ethnic African American men, contained dichotomous response options, and scored based on the percentage of questions answered correctly. Face validity was determined by academicians and public health practitioners. This Prostate Cancer Knowledge Scale was administered to 528 African American, English-speaking Caribbean, Haitian-American, and African men in the United States. Overall, PrCA knowledge among these Black men was moderate to high with mean correct responses at 68%. Although no significant differences in knowledge between the ethnic groups was identified, men with higher incomes and family histories of PrCA had the highest knowledge scores. No psychometric properties of the scale were reported.
Radosevich et al. (2004) developed and systematically evaluated the reliability and validity of the PROCASE Knowledge Index, a 10-item scale measuring PrCA history and risk factors (five items), PSA accuracy and follow-up tests (three items), and PrCA treatment efficacy (two items). Four additional items were included that measured knowledge of the likelihood of death from PrCA, predictive value of PSA tests, natural history of PrCA, and experts’ agreement on validity of the PSA test. Response options were true/false, and two of four additional items were multiple choice. Scoring was based on the percentage of items answered correctly. To assess psychometric properties, the PROCASE Knowledge Index and the four single items were administered to 1,152 male veterans (57% White), aged 50 and older. Internal consistency reliability using the KR-20 was 0.68 and had robust construct and criterion validity. However, the four single-item questions combined with the PROCASE Knowledge Index had weak validity.
The Cancer Knowledge Survey, developed by Powe et al. (2009), is a 23-item measure that assesses men’s knowledge of PrCA (11 items) and colorectal cancer (12 items), including risk factors, signs, symptoms, and screening recommendations for the two diseases. Response options for all questions were true/false and were scored by calculating the percentage of correct answers (i.e., 1 point per correct item). The survey was administered to 119 men (72 African Americans, 47 Hispanics) who were patients at qualified health centers and one hospital-based primary care clinic in a southern state and reported that African American men, who were older and had higher education attainment, had significantly higher PrCA and colorectal cancer knowledge than Hispanic men. Internal consistency reliability using Cronbach’s α was 0.75, but reliability estimates were not reported for each subscale. Validity information was also not reported.
To assess the impact of a spiritually-based PrCA informed decision-making intervention, Holt et al. (2009) developed two scales: the Knowledge of Prostate Cancer Scale and the Knowledge of the Screening Controversy Scale. The Knowledge of Prostate Cancer Scale is a nine-item measure that assessed PrCA knowledge and risk factors. The Knowledge of the Screening Controversy Scale is a four-item measure developed to assess knowledge of the PrCA screening controversy. One additional, original item assessed men’s knowledge about the relationship between PrCA screening and mortality. Scoring was determined by calculating the percentage of correct responses on each scale. In a sample of 49 men, Holt et al. (2009) discovered that knowledge on the Knowledge of Prostate Cancer Scale and their one, original item increased significantly whether the men received a spiritually-based or non-spiritually based education program. Only men in the spiritually-based intervention (n = 31) had significant increases on the scale for knowledge of the screening controversy. Internal consistency reliability for the Knowledge of Prostate Cancer Scale and Knowledge of the Screening Controversy Scale using Cronbach’s α were 0.66 and 0.43, respectively. Scale validity was not reported.
Ogunsanya et al. (2017) added two items to the Knowledge of Prostate Cancer Screening Questionnaire (Weinrich et al., 2004), which expanded it to a 14-item scale. The two additional items assessed the effects of diet on PrCA and the screening controversy (i.e., efficacy of the PSA test). Response categories were true, false, and I don’t know and scoring was based on the number of items answered correctly. This 14-item Knowledge of Prostate Cancer Screening Questionnaire was administered to 267 African American men, aged 18 to 40 years, to determine the intention of young African American men to screen for PrCA when it is recommended and relevant correlates. An additional 33 survey items measured attitudes toward PrCA screening, social influence, comfortability with prostate examinations, cues to action, health screening experiences, and intention to screen. African American men had low PrCA knowledge scores and PrCA knowledge had a positive correlation with intention to receive PrCA screening. No psychometric properties on the scale were reported (Ogunsanya et al., 2017).
Owens et al. (2018) modified Cormier et al.’s (2002) PrCA Knowledge Scale by adapting it for computer administration. Items were modified or eliminated if they were (a) unclear or inconsistent with current screening recommendations or (b) inconsistent with the iDecide PrCA education program, which was developed based on focus groups with African American men and educational information from the National Cancer Institute (National Cancer Institute, 2012; Blinded). Specifically, the ACS, AUA, and the USPSTF (American Cancer Society, 2013; Bibbins-Domingo et al., 2017; Carter et al., 2013) do not support routine screening, but suggest that men make informed decisions with their health-care provider based on their PrCA risk. The ACS, in particular, recommends that African American men, a high-risk population, begin having conversations about PrCA screening with their health-care provider at age 45 or as early as age 40 if they have a family history of PrCA (American Cancer Society, 2013). Items that referred to routine screening practices or ages that are inconsistent with current screening guidelines were eliminated (see Table 2; Q4, Q12–Q14). Items were added to clarify the efficacy of PSA and DRE exams, which included adding that neither are 100% accurate and neither test can be used to diagnose PrCA because a PrCA diagnosis is validated via biopsy (see Table 2; Q9, Q17, Q18). Only the scale by Radosevich et al. (2004) included items about prostate biopsy to measure knowledge about PrCA screening and diagnosis. One item on the original scale (see Table 1; Q22) regarding PrCA warning signs was separated into multiple items and two questions were added to capture other common symptoms (Table 2; Q23–Q26). Furthermore, an assessment of face validity resulted in the rewording of two questions (Q1, Q7) to increase clarity. Two additional questions were eliminated based on PrCA subject matter expert review (Q10, Q11) by the lead author (O.O.) and two additional PrCA experts with training in health communications. Content validity was assessed by pilot testing the survey containing the PrCA Knowledge Scale and 45 additional items used to evaluate the iDecide PrCA screening decision aid. Two African American men were asked to complete a paper survey, noting if there were questions, words, or concepts on the survey that might be difficult to interpret for themselves or men with low reading levels. After survey completion, they were also asked verbally by the lead author about these difficulties following survey completion. Both participants did not suggest additional changes to the survey. Table 2 presents original and modified versions of the PrCA Knowledge Scale. Items are scored based on the percentage of items correct.
Review of Prostate Cancer Scales.

Note. PrCA = prostate cancer; KR-20 = Kuder–Richardson Formula 20.
Prostate Cancer Knowledge Scale Modifications.
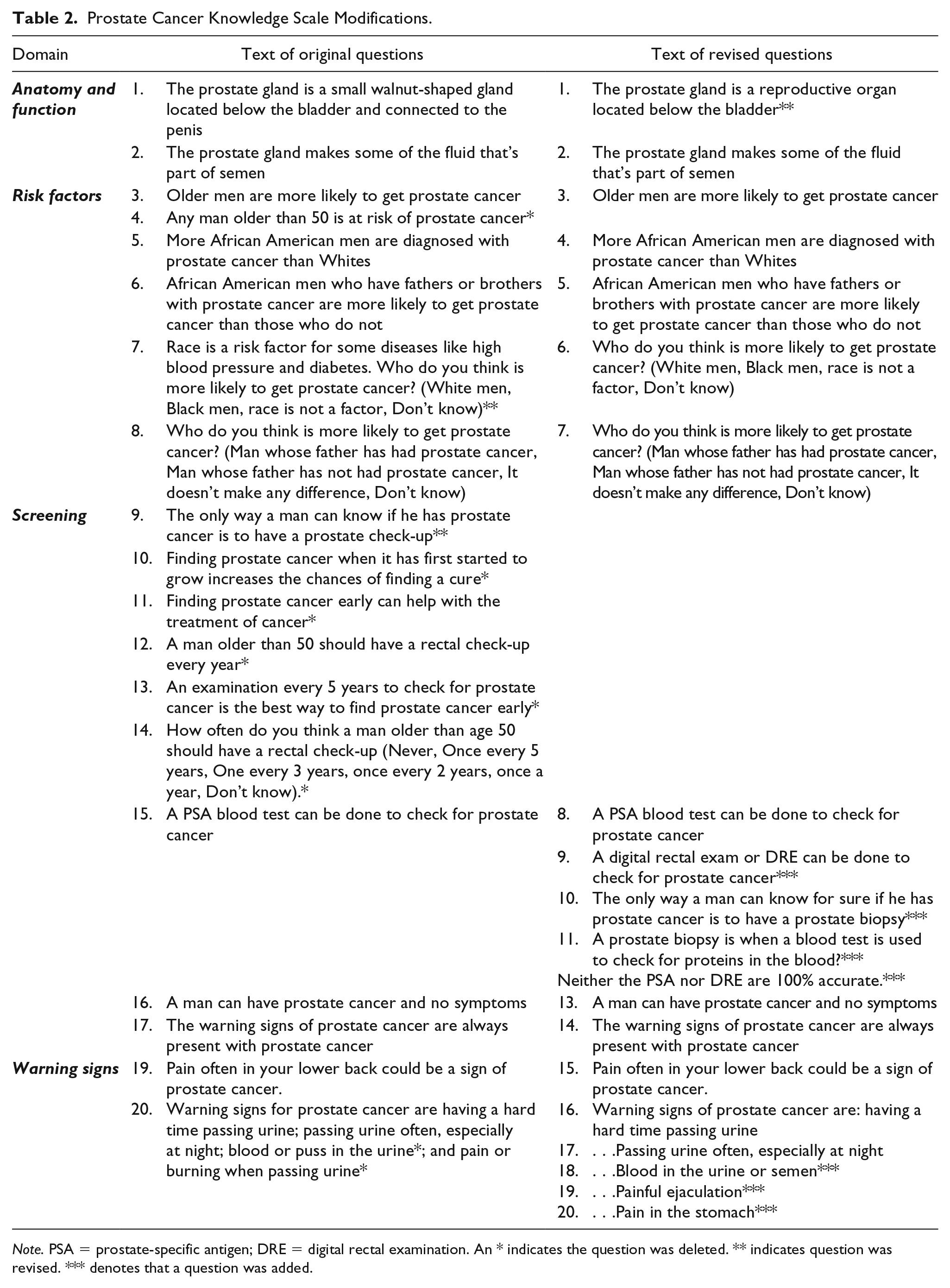
Note. PSA = prostate-specific antigen; DRE = digital rectal examination. An * indicates the question was deleted. ** indicates question was revised. *** denotes that a question was added.
In a sample of 352 African American men, the modified 20-item PrCA Knowledge Scale was administered to evaluate the effectiveness of a computer-based PrCA screening decision aid, iDecide, to increase PrCA knowledge, informed decision-making self-efficacy, and technology use self-efficacy. iDecide used an African American embodied conversation agent (i.e., a human-like character) to guide users thorough the basic information about prostate anatomy and a series of key topics that one should consider when making informed decisions about PrCA (e.g., risks and benefits of screening). To reiterate key points during the education session, users were engaged in question and answer exercises. These responses were not recorded, but prompted the system to provide users with the opportunity to choose other responses until a correct response was selected. Within the decision aid, users had the control to repeat information, repeat quizzes, and so forth. Following receipt of basic PrCA education, users were encouraged to participate in short role-play exercise with a second African American embodied conversational agent who was dressed like a health-care provider. The goal of this section was to prepare the user for a conversation with his health-care provider. In this section, users had limited onscreen questions that they could pose to the embodied conversational agent and it would respond accordingly. Some questions were included that are commonly asked, but may not be the best questions to ask in the context of a PrCA screening discussion. For example, while some providers may discuss PrCA during a conversation about an annual check-up, others will not because PrCA screening is not recommended on an annual basis. Therefore, if a user chose the basic checkup option in iDecide, the decision aid would inform them why this was not the best selection and encourage them to choose another option. The conversation between the user and the embodied conversation ended when the user indicated that he was ready to make an informed decision. At this point, the user was provided with informational resources both through the decision aid and the research associate. iDecide was about 10 minutes in duration and administered on a tablet computer. Men received paper-based surveys prior to and after using iDecide. Overall, PrCA knowledge, informed decision-making self-efficacy, and technology use self-efficacy increased significantly. However, the psychometric properties of the modified PrCA Knowledge Scale were not reported (Owens et al., 2018).
Although multiple studies have measured PrCA knowledge among African American men, most either do not report psychometric properties of their PrCA knowledge measure (Abbott et al., 1998; Demark-Wahnefried et al., 1993, 1995; Magnus, 2004; Smith et al., 1997; Steele et al., 2000; Wilkinson et al., 2003), have low representation of African American men (Demark-Wahnefried et al., 1993, 1995), or have small sample sizes (Powe et al., 2009). For the vast majority of studies reporting the reliability of their PrCA knowledge measure, internal consistency reliability was consistently low (i.e., ranging from .45 to .66; Boehm et al., 1995; Holt et al., 2009; Ogunsanya et al., 2017; Ross et al., 2011). Two studies reporting moderate to high reliability (i.e., α = .77, α = .87) among African American men had small sample sizes and no validity evidence was reported (Agho & Lewis, 2001; Weinrich et al., 2004). Agho and Lewis (2001) also used Cronbach’s α instead of KR-20 to assess internal consistency reliability. The current study evaluated the psychometric properties of the modified PrCA Knowledge Scale (Cormier et al., 2002) in African American men, who have the highest PrCA mortality risk in the world (Siegel et al., 2019). Having a reliable and valid measure of PrCA knowledge is critical for determining whether interventions are effectively informing African American men about PrCA screening options, as recommended by the ACS, AUA, and the USPSTF. See Table 1 for a summary of the review of measures.
Conceptual Framework for the Operationalization of the Prostate Cancer Knowledge Scale in Informed PrCA Decision-Making
Social cognitive theory emphasizes the dynamic interplay between individuals, their physical and social environments, and their behaviors (Bandura & Walters, 1977). In the context of PrCA screening, multiple social and environmental influences determine whether an individual is able to make an informed decision about PrCA screening. Two key individual factors that influence whether an individual has the capacity to engage in informed decision-making about PrCA screening are PrCA knowledge and self-efficacy. PrCA knowledge refers to the information necessary for an individual to understand PrCA (including the prostate’s anatomy and function, PrCA risk factors, types of PrCA screening, and PrCA warning signs) and the risks, benefits, uncertainties of, and alternatives to PrCA screening (basis of the scale). Self-efficacy is the level of confidence an individual possesses to actively involve himself, to the extent that he desires in screening decisions. At the environmental level, several factors influence whether a man engages in informed decisions about PrCA screening, but the most common are access to: PrCA information and a provider. While the measures reviewed in this manuscript focus on PrCA knowledge (one construct associated with PrCA screening decision-making), many of the interventions that utilize PrCA knowledge measures also work to enhance a man’s comfort with speaking with a health-care provider. For example, [Blinded author] sought to enhance PrCA knowledge and self-efficacy, which is consistent with social cognitive theory.
Methods
This cross-sectional study examined the psychometric properties of a modified version of the PrCA Knowledge Scale (Cormier et al., 2002) used in a pretest–posttest design to evaluate PrCA knowledge before and after the administration of iDecide, a computer-based decision aid in African American men. Detailed information about iDecide is in {Blinded}. Only posttest data are used in the current study. Human subjects approval was received from the {Blinded} Institutional Review Board.
Participants
A purposive sample of 352 African American men aged 40 and older were recruited from multiple venues in South Carolina between July 2015 and February 2016 to participate in a pilot study. Eligible participants were men who (a) self-identified as African American; (b) spoke and comprehended English; (c) had no personal history of PrCA; and (d) had no self-reported history of cognitive decline. All men were provided with study details immediately prior to their study participation through a written informed consent document. Men were asked to sign the consent after asking clarifying questions. Detailed study information is reported in {Blinded}.
Data Analysis
Descriptive statistics were conducted to describe to the sociodemographic characteristics of the men in the sample. Pearson’s correlation assessed the association between factors and subscale items. Internal consistency reliability was assessed using KR-20 for the total scale and each of the four subscales. KR-20 is an alpha used when response categories on a measure are dichotomously scored with 1 for correct responses and 0 for incorrect responses (Waltz et al., 2005).
Exploratory factor analysis (EFA) is a data-driven exploratory technique and that does not require a priori specification of the relationships between latent and observed variables (Brown, 2014; Harrington, 2009; Kline, 2005). Thus, a priori model specification is not required because factor structure and factor loadings are assumed to be unknown. The purpose of EFA is to identify the most parsimonious number of interpretable factors that explain the correlations between observed variables (Thompson, 2004). In this study, EFA was conducted to identify the number of latent constructs (factors) and underlying factor structure of the modified PrCA Knowledge Scale. The number of participants to item ratio is 14:1, which is above the recommended 10:1 often used to determine a priori sample size for EFA (Costello & Osborne, 2005).
EFA was conducted using weighted least square mean and variance (WLSMV) estimation with Geomin rotation. WLSMV is a robust estimator which does not assume normally distributed variables and provides the best option for modeling categorical or ordered data (Brown, 2014). The modified PrCA Knowledge Scale (Cormier et al., 2002) has true/false response categories. Factor structure was assessed by eigenvalues and proportion of eigenvalues on the scree plot. An eigenvalue greater than one and the cumulative proportion of eigenvalues of the reduced covariance matrix greater than one determined if a factor was retained in the factor structure. A factor with less than three item loadings was considered weak and unstable (Costello & Osborne, 2005), and was dropped from the analysis. Factors with three or more items loading onto them were retained. Factor loadings were assessed using item communalities, cross-loadings, and item statistics. An item was determined to load on a factor if the loading score was 0.30 or greater (Shultz et al., 2013). Cross-loading occurred if an item loaded onto multiple factors at 0.30 or above.
Fit indices used to assess model fit included the model chi-square, normed chi-square (χ2/df), root mean square error of approximation (RMSEA), Bentler’s comparative fit index (CFI), the standardized root mean square residual (SRMR), and the Tucker–Lewis Index (TLI). Model fit criteria were a normed chi-square of less than 3, RMSEA between 0.05 and 0.08 with a confidence interval of less than or equal to 0.05 lower bound and less than or equal to 0.10 upper bound, CFI greater than or equal to 0.90, SRMR less than 0.10, and TLI greater than or equal to 0.95 (Kline, 2005). Descriptive statistics, Pearson’s correlation, and KR-20 were performed using SAS/STAT®, version 9.4 (SAS Institute, 2015) and EFA was conducted using Mplus v. 8.2 (Muthén & Muthen, 2017).
Results
The frequency distribution for each item of the modified PrCA Knowledge Scale is shown in Table 3. An overwhelming majority (85%, n = 301) of African American men correctly answered that a PSA test can be used to check for PrCA (Q8) and that African American men are more often diagnosed with PrCA than Whites (Q4; 83%, n = 291). The lowest frequencies for incorrectly answered questions were for Q20, which asked whether warning signs are always present with PrCA (16%, n = 56) and Q21, which asked if pain in the lower back is a symptom of PrCA (26%, n = 92).
Frequency Distribution of Items for the PrCA Knowledge Scale.

Note. PrCA = prostate cancer; PSA = prostate-specific antigen; DRE = digital rectal examination.
Using WLSMV, scree plot and eigenvalues suggested six factors for the modified 20-item PrCA Knowledge Scale, but the RMSEA (.03), CFI (.98), TLI (.96), and SRMR (.06) suggested a five-factor solution may provide the best fit (Table 4). In the five-factor solution, 20 items loaded positively on five different factors at 0.30 or above with factor loadings ranging from 0.34 to 0.94. Three items (5, 8, 16) cross-loaded. Seven items (1, 2, 5, 8, 9, 12, 13) loaded on PrCA Anatomy and Screening (Factor 1) with item 8 (.34) cross-loading less strongly on Factor 2 and item 5 cross-loading more strongly on Factor 3 (.76). Four items (4, 6, 8, 16) loaded on Probability of PrCA (Factor 2) with items 8 (.44) and 16 (.68) cross-loading more strongly on Factors 1 and 4 respectively. Three items (3, 5, 7) loaded on Risk Factors (Factor 3) with item 5 cross-loading less strongly (.32) to Factor 1. Six items (15, 16, 17, 18, 19, 20) loaded onto Warning Signs (Factor 4). Two items (11, 14) loaded on PrCA Diagnosis (Factor 5). Based on the loading pattern, Factor 5 does not have enough items to be considered a subscale (<3 items; Brown, 2014). Factor 2 also has less than the three items. In addition, items 4 and 6 (Factor 2) fit better conceptually with items on Factor 3. Similarly, items 11 and 14 (loaded on Factor 5) fit better conceptually on Factors 1 and 4, respectively.
Model Fit for 19 and 20-Item Prostate Cancer Knowledge Scales.

Note. RMSEA = root mean square error of approximation; CFI = Bentler’s comparative fit index; TLI= Tucker–Lewis index; SRMR = standardized root mean square residual. All model chi-square estimates were significant at a level of .05. Cutoff criteria for fit indices are as follows: RMSEA <.05, CFI > .90, TLI > .95, SRMR < .08. Cross-loadings occurred if items loaded on two or more factors at .40 or above.
Because the fit indices of Factors 1, 2, and 3 were below standard cutoffs in the five-factor model (Table 4), a four-factor model was examined, which resulted in better loading patterns and no cross-loadings. Factor loadings ranged from .31 to .86. Seven items (1, 2, 8, 9, 12, 13) loaded on PrCA Anatomy and Screening (Factor 1). Five items (3, 4, 5, 6, 7) loaded on Risk Factors (Factor 2). Six items (15, 16, 17, 18, 19, and 20) loaded on Warning Signs (Factor 3). Two items (11, 14) loaded on PrCA Diagnosis (Factor 4), though items 11 and 14 would fit better conceptually on Factors 1 and 3, respectively. Item 10 did not load onto any factor.
Exploring a 19-Item Factor Structure for the Prostate Cancer Knowledge Scale
To improve factor structure, item 10 was dropped from the four-factor model. Item 10 was related to prostate biopsy, a diagnostic test used to validate whether cancer is present beyond screening. After item 10 was dropped, the EFA yielded slightly higher fit indices for the four- and five-factor models on the 19-item PrCA Knowledge Scale. However, the 19-item, four-factor model had the best factor loading pattern conceptually. In the four-factor model, five items (1, 2, 8, 9, 16) loaded on PrCA Anatomy and Screening (Factor 1), with item 16 cross-loading less strongly (.32 versus .62) on Factor 3. Five items (3, 4, 5, 6, 7) loaded on Risk Factors (Factor 2). Six items (14, 15, 16, 17, 18, 19, 20) loaded on Warning Signs (Factor 3), with item 14 loading more strongly (.42 versus .76) on Factor 4. Two items (11 and 14) loaded on PrCA Diagnosis (Factor 4). Items 12 and 13 did not load.
Exploring an 18-Item Factor Structure for the Prostate Cancer Knowledge Scale
Because PrCA Diagnosis (Factor 4) consistently had too few item loadings to constitute a subscale, two items (11, 14) were considered for removal. Item 11 was removed because it was the only question remaining that was conceptually related to PrCA diagnosis (i.e., biopsy). Item 14, however, also cross-loaded on Factor 3 (.42), to which it was more conceptually related so it was retained. Items 12 and 13 were also retained in the 18-item factor structure although they were not in the 19-item factor structure analyses. Both items loaded (.32 and .41) in the 20-item, five-factor structure analyses. EFA was re-run with 18 items.
EFA of the 18-item factor structure resulted on 18 items loading onto a factor. While the four- and five-factor models yielded the best fit indices (Table 5), both models did not have enough items loading onto at least one factor to constitute a subscale. The three-factor model had reasonable model fit based on RMSEA (.05), CFI (.95), and SRMR (.08). For the three-factor model, five items (1, 2, 5, 7, 8, 9, 12, 13) loaded on PrCA Anatomy and Screening (Factor 1), with items 5 (.49 versus .56) and 7 (.39 versus .61) cross-loading more strongly onto Factor 2. Five items (3, 4, 5, 6, 7) loaded on Risk Factors (Factor 2), with items 5 and 7 cross-loading on Factor 1. The remaining seven items (14, 15, 16, 17, 18, 19, 20) loaded onto Warning Signs (Factor 3) with no cross-loading (Table 6). Each of the three factors were positively correlated (Table 7) and the total scale had good internal consistency reliability (KR-20 = .80).
Factor Loadings for 18-Item Prostate Cancer Knowledge Scale.
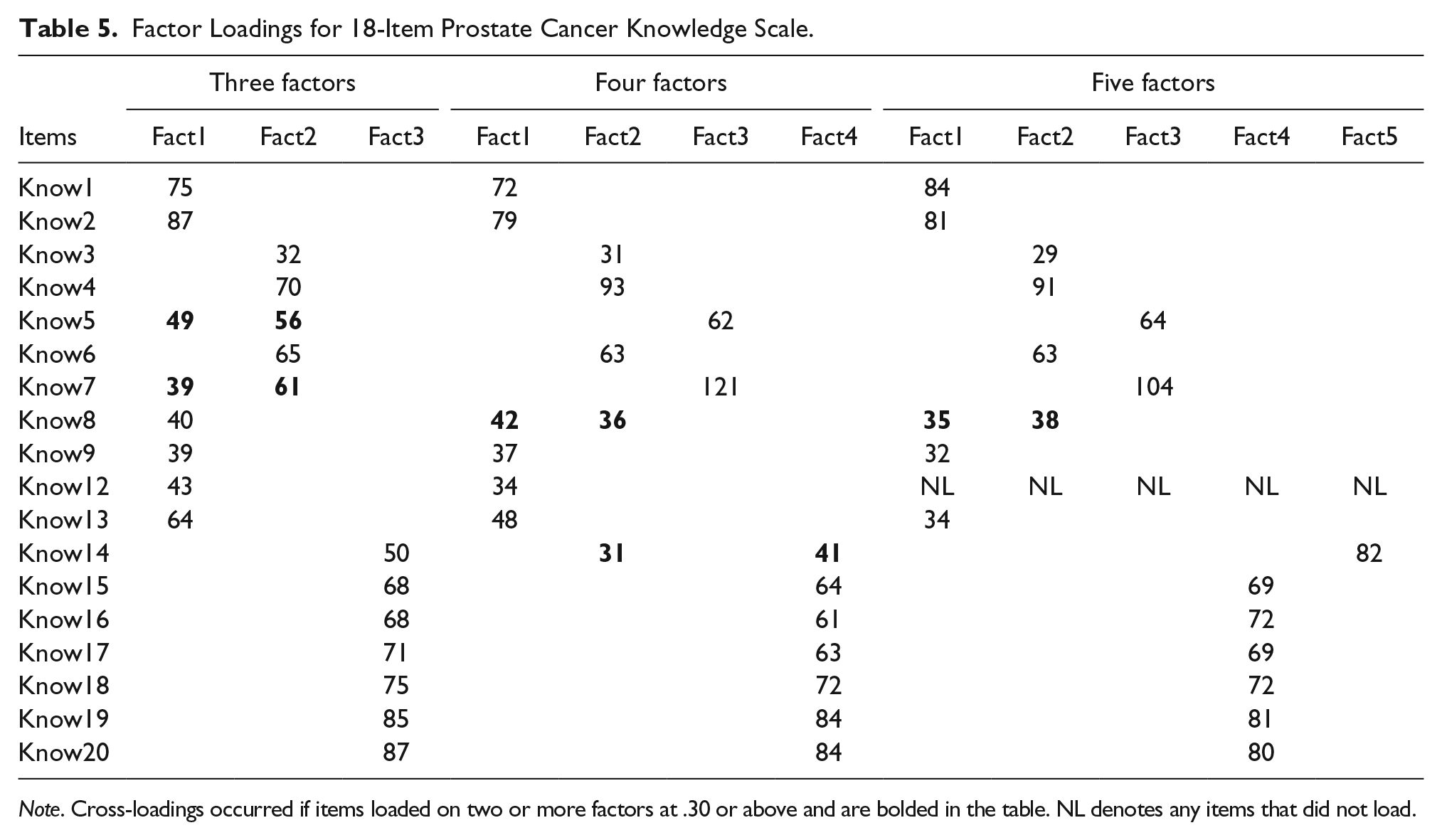
Note. Cross-loadings occurred if items loaded on two or more factors at .30 or above and are bolded in the table. NL denotes any items that did not load.
Model Fit for 18-Item Prostate Cancer Knowledge Scale.

Note. RMSEA = root mean square error of approximation; CFI = Bentler’s comparative fit index; SRMR = standardized root mean square residual. All model chi square estimates were significant at a level of .05. Cutoff criteria for fit indices are as follows: RMSEA < .05, CFI > .90, TLI > .95, SRMR < .08. Cross-loadings occurred if items loaded on two or more factors at .40 or above.
Means, Standard Deviations, Reliabilities, and Pearson Correlations for the Total Scale and Three Subscales of PrCA Knowledge.

Note. PrCA = prostate cancer. Kuder–Richardson Formula 20 (KR-20) is the reliability coefficient in the diagonal reported. KR-20 is 0.80 including all items.
Discussion
Using EFA, this study employed a multi-step process to determine the most parsimonious and interpretable factor structure for a modified PrCA Knowledge Scale using WLSMV estimation. EFA yielded an 18-item, three-factor structure (Anatomy and Screening, Risk Factors, and Warning Signs) PrCA Knowledge Scale as the best solution for measuring PrCA knowledge among African American men. This 18-item, three-factor structure is substantiated by moderate to high (.39–.87) factor loadings, adequate fit indices, a good internal consistency reliability, and strong conceptual relationships between items on each subscale. Model estimates and fit indices were used conjunctively to choose the best overall factor structure and model fit. Fit indices and scree plots provided the strongest evidence for a five-factor solution, but an assessment of the factor loading patterns in tandem with conceptual relationships between items indicated that a three-factor solution was ideal. All three factors of the three-factor structure were positively correlated. Thus, the 18-item, three-factor structure of the PrCA Knowledge Scale was most parsimonious and conceptually-relevant for measuring PrCA knowledge among African American men.
The psychometric evidence of the 18-item, three-factor model of the PrCA Knowledge Scale may be greatly improved compared to evidence on previous versions of the PrCA Knowledge Scale because of methodological differences. The current study had a sample of 352 African American men whereas most prior studies had small samples and subsamples of African American men ranging from 11 to 123, which resulted in low reliability estimates or none reported. Studies with larger sample sizes (286–835) reported minimal or no psychometric evidence. Other PrCA knowledge scales had fewer scale items, and used various factor analytic methods and internal consistency reliability estimates to assess factors structure and reliability for a measure with dichotomous response categories. Factor structure and model fit indices can be sensitive to sample size and number of scale items, and using inappropriate estimation procedures and reliability estimates can bias results (Shultz et al., 2013; Waltz et al., 2005). Overall, this study’s three-factor, 18-item PrCA Knowledge Scale extends prior PrCA psychometric evidence by identifying a measure with more conceptually-relevant scale items, better domain coverage, and a more parsimonious factor structure that includes the most recent PrCA screening recommendations. Additional psychometric tests are needed to confirm this factor structure.
To the author’s knowledge, this is the first study to examine the psychometric properties of a PrCA knowledge scale that includes recent recommendations from the ACS, AUA, and the USPSTF, suggesting men make an informed decision, considering both potential benefits and harms of screening, with their health-care provider before undergoing PrCA screening. Based on the conceptual framework guiding this study, men who have lower knowledge of PrCA (in addition to low decision self-efficacy) may be less prepared to engage in informed decisions with their providers about PrCA as recommended by the ACS, AUA, and the USPSTF. In absence of the informed decisions about PrCA screening, men could receive later diagnoses or undergo unnecessary treatment, both of which can lead to decision regret (Gökce et al., 2017; Orom et al., 2015). Having a knowledge scale that is culturally appropriate for African American men can facilitate the evaluation of culturally targeted interventions for educating African American men about PrCA screening.
Dropping Prostate Cancer Biopsy Items
Item 10 did not load in the 20-item, four-factor structure of the PrCA Knowledge Scale and was consequently dropped. Item 10, which reads “The only way for a man to know for sure if he has PrCA is to have a prostate biopsy” was expected to load with items on Anatomy and Screening (Factor 1). By removing item 10, items 11 (“A prostate biopsy is when a blood test is used to check for proteins in the blood”) and 14 (“The warning signs are always present with prostate cancer”) were expected to load onto Anatomy and Screening (Factor 1) and Warning Signs (Factor 3), respectively. This new factor loading pattern eliminated the PrCA Diagnosis (Factor 4), which did not have enough loadings to constitute a subscale. However, EFA of the 19-item revealed that Q11 and Q14 still loaded together, but 14 cross-loaded less strongly (.42 versus .76) onto Factor 3, to which it was conceptually related. Removing Q11 resulted from this item being the only item loading strongly onto Factor 4.
Both items 10 and 11 asked about prostate biopsy. A biopsy is a diagnostic test used to diagnose PrCA, unlike screenings that indicate general abnormalities that could be attributed to factors other than PrCA. For example, the PSA screening can be falsely lowered by medications to treat a swollen prostate or falsely elevated through vigorous physical activity (Cary & Cooperberg, 2013; Smith et al., 2016). The fact that Q10 and Q11 did not load with other screening items can potentially be explained by three rationales: (a) African American men lack biopsy knowledge, (b) prostate biopsy is not clinically or conceptually related to PrCA screening informed decision-making, and (c) question wording lacked clarity. Though some researchers support the notion that men should be informed about the potential next steps in the decision continuum (biopsy, treatment) prior to making a screening decision {Blinded}, most researchers have focused their interventions on empowering men to make each of these decisions separately (Ankerst et al., 2012; Ilic et al., 2015; Violette et al., 2015). Biopsy may not typically be discussed in conversations about PrCA screening or included in decision aids about PrCA screening. For example, Radosevich et al.’s (2004) PROCASE Knowledge Index was the only scale reviewed that measures biopsy knowledge. Consequently, healthy African American men’s knowledge about prostate biopsy may be significantly limited. Further, it is possible, based on poor performance on Q11 at pre- and post-intervention (Table 3), that men may have confused the prostate biopsy and PSA screening procedures. Findings suggest future research assess prostate biopsy and PSA screening as independent constructs and prostate biopsy specifically with more than two scale items.
Cross-Loading Items
Interestingly, Q5 (“African-American men who have fathers or brothers with prostate cancer are more likely to get prostate cancer than those who do not”) and Q7 (“Who do you think is more likely to get prostate cancer?. . ...”) both cross-loaded on Anatomy and Screening (Factor 1) and Risk Factors (Factor 2) with lower loadings on Factor 1. While it is unclear why Q5 cross-loaded onto Factor 1 (which is conceptually unrelated), Q7 cross-loading onto Factor 1 may be attributed to question composition. Unlike most questions on the scale which have true, false, and I don’t know response options, Q7 had four multiple response options (“Man whose father has had prostate cancer, Man whose father has not had prostate cancer, It doesn’t make any difference, Don’t know”) and only 55% of the participants chose correctly. Therefore, this multiple-choice option may have increased the likelihood of response bias.
Study strengths included a large community sample of African American men, which exceeded the minimum recommended sample size for EFA (>200; MacCallum et al., 1999). The African American men were from one mid-sized city in a southeastern state and may not be generalizable to African American men who reside in other United States regions or men of younger ages, and other races and ethnicities. Cross-loadings of two items onto a factor to which it was conceptually unrelated suggest that some scale items may need further refinement prior to future scale administration. Despite these limitations, this study provides valuable psychometric evidence, which can contribute to the future development and evaluation of culturally appropriate interventions to facilitate PrCA screening decisions of African American men who are at the highest risk for PrCA mortality. Confirmatory factor analysis is warranted to confirm convergent and discriminate validity of the PrCA Knowledge Scale.
Conclusion
The robust psychometric evidence on the 18-item, three-factor PrCA Knowledge Scale demonstrates the utility of this instrument for measuring PrCA knowledge among African American men, who have the highest mortality rates nationally. Because current PrCA screening recommendations suggest that men make informed decisions with their provider about PrCA screening, there is an emergence of decision aids to enhance men’s PrCA knowledge. However, there is a lack of evidence-based, culturally appropriate scales for evaluating the effectiveness of these decision interventions for enhancing knowledge among African American men. Determining whether African American men are adequately equipped with knowledge about PrCA screening is critical to ensuring that they understand the risk, benefits, and uncertainties of screening; are able to participate in this decision at the level they desire; and ultimately avoid decision regret. Furthermore, engaging in PrCA screening decisions early could ultimately reduce their mortality risk. Therefore, the PrCA Knowledge Scale shows promise not only for being instrumental in reliably evaluating decision interventions among African American men, but also in contributing to the elimination of PrCA disparities among this racial group. The PrCA Knowledge Scale can be used with any PrCA interventions with African Americans. Future psychometric testing including confirmatory factor analysis is warranted to confirm convergent and discriminate validity of the PrCA Knowledge Scale. Future research should also confirm the factor structure of the PrCA Knowledge Scale using a larger and more demographically diverse sample of African Americans.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by the Office of Vice President for Research and School of Pharmacy at the University of South Carolina through an American Cancer Society Institutional Research Grant (PI: Bennett).