
Abstract
The aim of this study was to provide a specific review of current medical literature regarding the lipid profile during prostate carcinoma (PCa) treatment. The main aim was to analyze the results presented by different authors and to find a commonality in the changes occurring during the treatment—hormonotherapy. The levels of total cholesterol (TC), triglycerides (TG), high-density lipoprotein (HDL) cholesterol, and low-density lipoprotein (LDL) cholesterol were measured before and after the follow-up treatment. The manuscripts reviewed came from the period between 2008 and 2016. The size of the studies ranged from 16 participants to 310. The mean age was from 65 to 74 years in all studies. The Q test was used to attain all lipid parameters and to specify heterogeneity (p < .0001). After 12 months of androgen deprivation therapy (ADT), the patients had a significantly higher level serum TC and TG.
Keywords
Prostate carcinoma (PCa) is the main cause of mortality among men and the second most common cause of cancer-related mortality (Grubb & Kibel, 2007). The methods of treating PCa patients differ and depend on the age of the patient and the progress of the disease. Radical treatment methods include surgery, radiotherapy (RT), and combinations of both, sometimes combined with hormonotherapy. The androgen dependence of PCa was first described by Huggins (1941) who proved that castration decreases the growth of PCa. Self-contained hormonotherapy is used as neoadjuvant and adjuvant therapy before and after RT, as palliative treatment or with the biochemical prostate-specific antigen (PSA) recurrence. Androgen deprivation therapy (ADT) is carried out by the administration of luteinizing hormone–releasing hormone (LHRH) agonist or antiandrogens. ADT is the standard palliative treatment for metastatic PCa patients and is used as an adjunct to RT in patients with locally advanced disease and in unfavorable intermediate-risk or high-risk disease cases. This kind of treatment is very often used to alleviate the symptoms or to prolong survival. ADT may also promote the development of some changes in metabolism—side effects such as skeletal complications, metabolic and cardiovascular complications, sexual dysfunctions, hot flashes, and mood disorders (Alibhai, Gogov, & Allibhai, 2006; Green et al., 2004; Shahinian, Kuo, Freeman, & Goodwin, 2006). Cholesterol plays an important role in steroidogenesis in which androgens are produced, which in turn stimulate the proliferation of prostate cancer (PCa) cells (Murai, 2015). There are some epidemiological studies that report a positive correlation between hypercholesterolemia or dyslipidemia and PCa (Ahn et al., 2009; Hayashi et al., 2012; Kitahara et al., 2011; Mondul, Clipp, Helzlsouer, & Platz, 2010; Moses et al., 2009; Platz et al., 2009; Van Hemelrijck et al., 2011). One epidemiological meta-analysis showed a negative correlation—higher levels of TC, HDL, or LDL were not associated with the risk of development of PCa (YuPeng et al., 2015). The aim of this study was specifically to review the current clinical study–based medical literature regarding the lipid profile in PCa treatment. The plan was to analyze the results presented by different authors and to identify the commonality between changes occurring during treatment.
Materials and Methods
This is a review of all the studies found on the PubMed platform (www.pubmed.com) as a result of a search done with the use of the following keywords: lipid profile in cancer patients; prostate cancer and lipids change; lipid profile in cancer patients after radiotherapy; and lipid profile in prostate cancer patients after chemotherapy. Fifteen studies were found. In these studies the following lipid parameters were compared: TC, HDL, LDL, and TG before and after hormonal therapy. Because the results of two different studies by the same authors were identical, only one of them was included in the review (Study 8—the same authors presented the same data of lipids for two topics in two different journals). One study was omitted in the analysis due to incomplete data (Study 5 had no standard deviation). Two more studies, 2 and 3, were also incomplete due to the lack of full clinical data; however, they were included in the study. Therefore, 13 studies were left (Hamilton et al., 2011; Henriksson, Angelin, & Berglund, 1992; Morote et al., 2015; Nguyen et al., 2015; Oka et al., 2016; Sağlam, Köse, Kumsar, Budak, & Adsan, 2012; Salvador et al., 2013; Smith et al., 2002; Smith, Lee, & Nathan, 2006; Smith et al., 2008; Torimoto et al., 2011; Yuan et al., 2012; Ziaran, Goncalves, & Breza, 2013). The manuscripts came from the period between 2008 and 2016. There were 12 prospective studies and 1 retrospective study. The size of those studies ranged from 16 participants to 310. The mean age was from 65 to 74 years in all studies. All subjects were clinically diagnosed with PCa and the diagnosis was confirmed by histopathological examination and categorized as an advanced clinical stage. The lipid profiles were measured in the blood and monitored at different stages in different studies. The two common monitoring points for all the studies were before the initiation of ADT and 12 months after the treatment. Clinical characteristics of the studies are presented in Table 1.
Clinical Characteristics of the Studies.
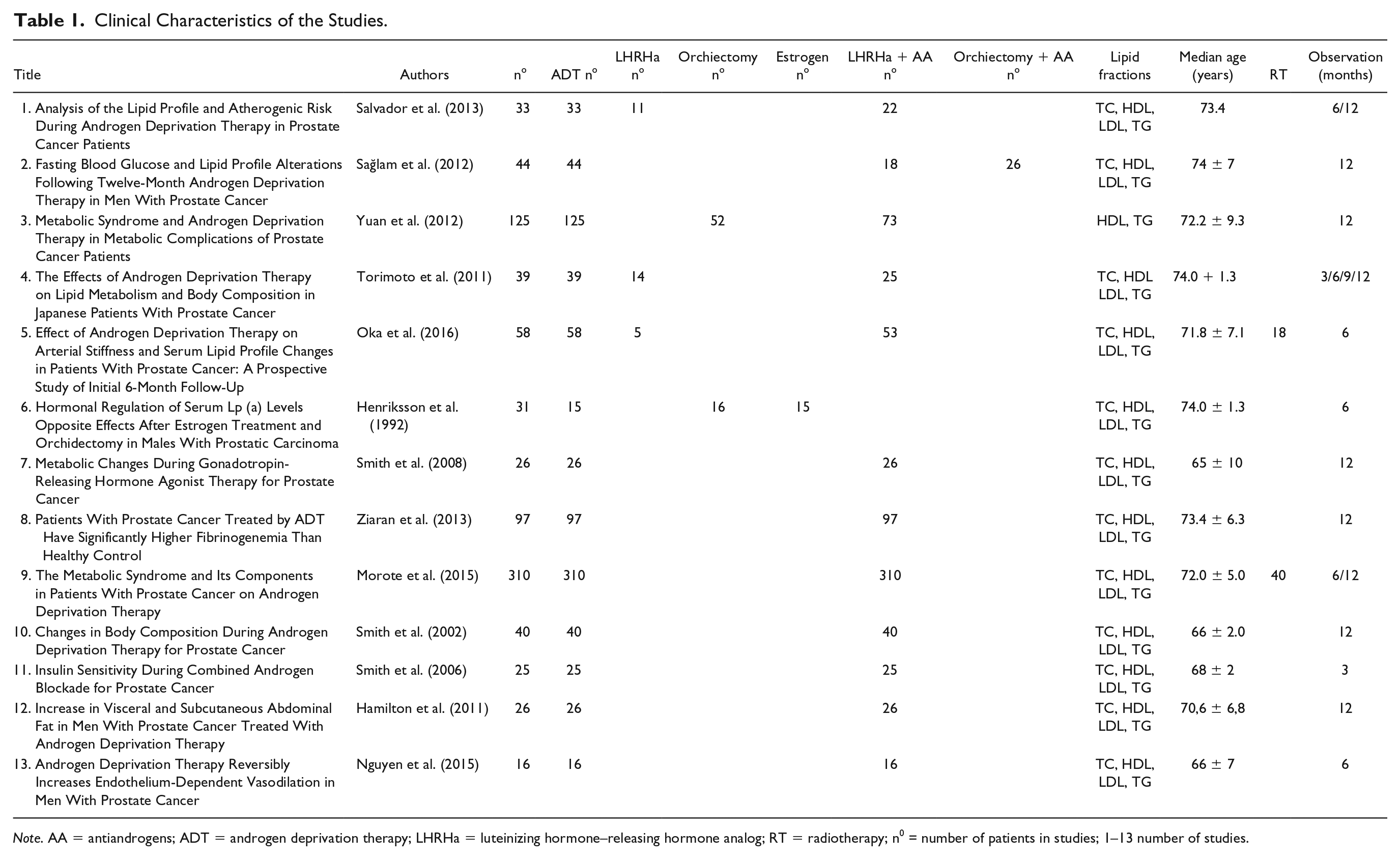
Note. AA = antiandrogens; ADT = androgen deprivation therapy; LHRHa = luteinizing hormone–releasing hormone analog; RT = radiotherapy; n0 = number of patients in studies; 1–13 number of studies.
Statistical Analysis
To synthesize the relevant results from each study, we used meta-analysis. This is an analytical method where the goal is to aggregate and contrast the findings using statistical functions for calculating various effect size or outcome measures. In the conducted meta-analysis, standardized mean differences (SMDs) were estimated between the studies based on the random effects model. Additionally, the Q test was applied to specify heterogeneity of the data. The computation was performed with the metafor R package (Viechtbauer, 2010). Using meta-analysis, the estimates of the standardized mean differences and heterogeneity of the data are reported in Table 2.
Meta-Analysis of the Aggregated Studies for Calculating Effect Size for Lipids Models Before Hormonotherapy and After 12 Months Therapy (SMD and Q Test).

Note. CI = confidence interval; HDL = high-density lipoprotein; LDL = low-density lipoprotein; SMD = standardized mean differences; TG = triglyceride.
Results
The mean difference between baseline concentrations of plasma lipids and the levels after hormonotherapy in the PCa patients is presented in Figures 1–4. It can be seen in Table 2 that for the TC model, the SMD is −0.81, ranging from −1.39 to −0.24, and the p value = .0056. It means that in all aggregated studies we observe a significant increase of TC concentration after RT compared to that before the treatment. However, the tested Q = 140 andp < .0001 provide evidence of a considerable amount of heterogeneity in these findings. For HDL and LDL measures, the obtained p values for SMDs are both >.05, which indicates an insignificant difference in the lipid concentrations before and after treatment. Similarly the Q test values in HDL and LDL models testify strong heterogeneity of the data. For the final TG lipid, following the synthesized studies, the model indicates statistically significant increase of TG after 12 months therapy compared to that before hormonotherapy. The conducted meta-analysis is displayed graphically in Figures 1–4. Due to lack of data, some studies were excluded from the meta-analyses (see Materials and Methods section).
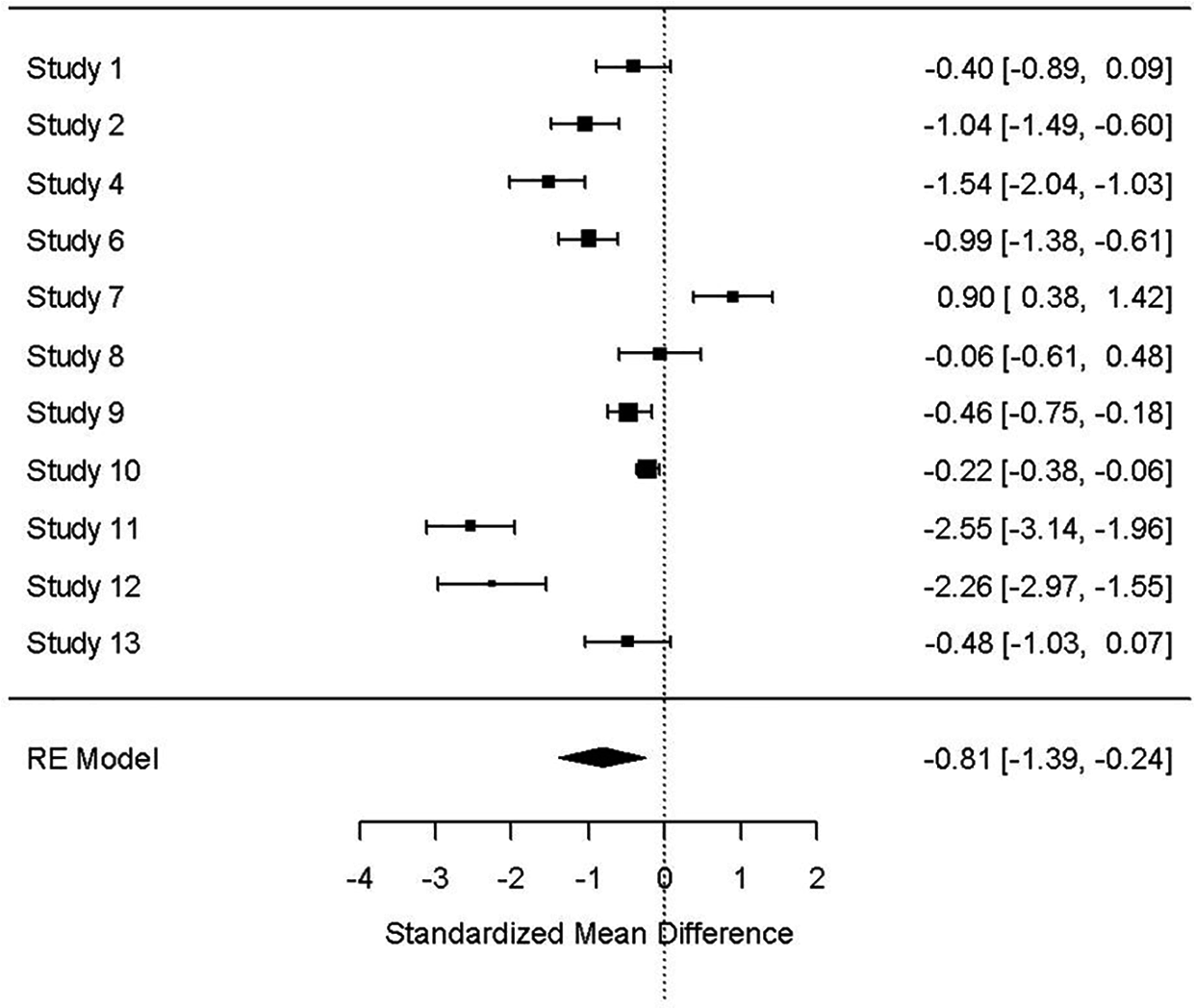
TC: baseline results and 12 months follow-up result for all studies (p = .0056).

HDL: baseline results and 12 months follow-up result for all studies (p = .3542).

LDL: baseline results and 12 months follow-up result for all studies (p = .3784).
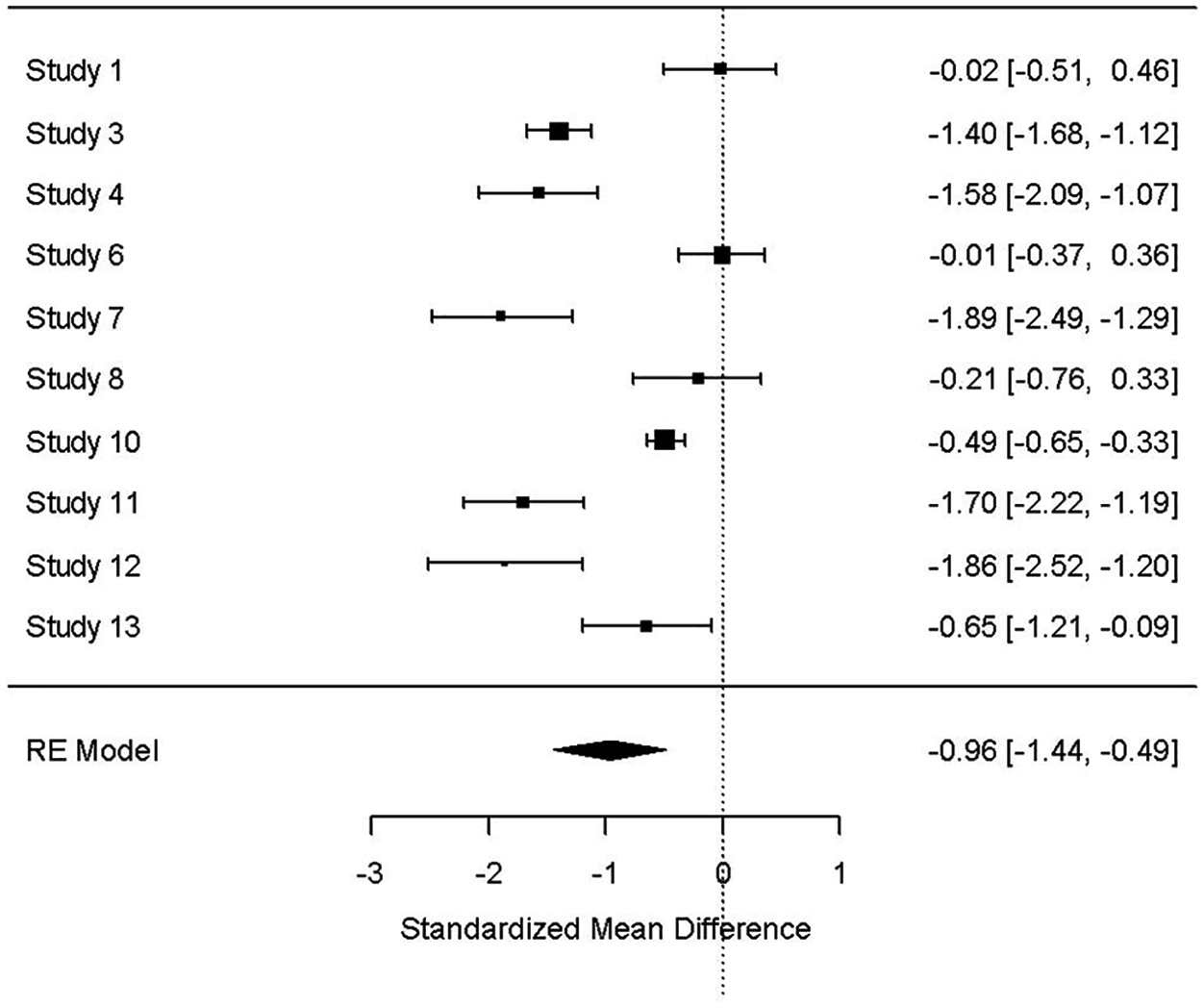
TG: baseline results and 12 months follow-up result for all studies (p = <.0001).
Discussion
The patients with PCa underwent different treatment modalities, which might have had an influence on the lipid parameters. After hormonal therapy (LHRH analog + antiandrogen bicalutamide or flutamide = maximal androgen blockade [MAB]), prostate cells are deprived of androgen, which decreases proliferation and progression of prostate cancer cells (Pfitzenmaier & Altwein, 2009). Certain studies point to a continuous ADT treatment in older men as the cause of an increased risk of diabetes and fragility fracture but not acute myocardial infarction or sudden cardiac death (Alibhai et al., 2009). There are studies that stand in opposition to the above and state that LHRH agonists do not seem to increase cardiovascular mortality in men with locally advanced prostate cancer (Efstathiou et al., 2009). In a recent epidemiology study, high TC and high HDL levels were presented to be a positive prognostic factor in increasing the overall survival (OS) and disease-free survival (DFS) among patients with cancer. There was no visible effect of low TG and low LDL on cancer survival. The authors presented certain lipid metabolic markers (high level of TC and LDL and a low level of HDL) as an increased risk factor for the incidence and the progression of cancer (Zhou, Li, Liu, Chen, & Xiao, 2018). TC is an important compound in the human body, especially for transporting proteins in the plasma (Hughes-Fulford, Chen, & Tjandrawinata, 2001) and is used in the synthesis of new cell membranes—including in cancer cells (Banker et al., 2004). Low cholesterol can be a cause of the increased sensitivity to oxidative stress (Muldoon, Kritchevsky, Evans, & Kagan, 1996) and of the loss of immune cells (T cells and CD8+) (Muldoon et al., 1997). In the low serum TC environment, the interleukin-6 level is elevated (an inflammatory protein related with cancer development and progression) (Kuroda et al., 2007). Hypocholesterolemia could occur due to an increased LDL receptor activity in cancer cells (Hughes-Fulford et al., 2001; Vitols, Björkholm, Gahrton, & Peterson, 1985). Long-term use of ADT is known to cause changes in the lipid profile during and after treatment (Alibhai et al., 2009). The results obtained in this analysis reported significantly higher concentrations of total TC and TG after using ADT. The serum lipid levels can be potentially modified by RT: TC was decreased after RT but its reduction was slower in patients with a higher PSA compared to those with a lower PSA and TG decreased after RT only in the patients ≥70 years (Wolny-Rokicka, Tukiendorf, Wydmański, Brzezniakiewicz-Janus, & Zembroń-Łacny, 2019; Wolny-Rokicka, Tukiendorf, Wydmański, & Zembroń-Łacny, 2017). This review aimed to assess the lipid profile in PCa patients during ADT. An overview of medical literature reveals that combining treatment methods works best for PCa patients. Palliative RT when used with ADT contributes to changes in plasma lipids. This is mainly due to changes in the activity of enzymes, their synthesis, and catabolism of lipid membranes, and thus leads to modifications in the composition of lipids (Simons & Sampaio, 2011). PCa cells are reported to have a higher cholesterol and sphingomyelin content when compared with healthy cells (Freeman & Solomon, 2004). The evidence shows that PCa cells produce androgen by intratumoral steroidogenesis, leading to their enhanced proliferation (Locke et al., 2008). LDL and HDL stimulate androgen production in steroidogenic tissues (Azhar & Reaven, 2002). In the study on metastatic prostate adenocarcinoma cell lines, LDL induces proliferation of castration-resistant bone-derived cells, but not lymph node metastatic prostate (Sekine et al., 2009). In conclusion, to the best of our knowledge, this is a systematic analysis of the influence of ADT on the lipid profile (TC, TG, HDL, and LDL) in PCa patients. This analysis focused only on examining the correlation between ADT and its effect on the lipid profile in patients. The results showed significantly higher concentrations of total TC and TG after 12 months of the use of ADT. The analysis did not identify any significant differences for HDL and LDL between baseline and after treatment. As the survival rate of cancer patients increases, frequent control of the lipid profile gains importance. In the authors opinion, cholesterol may play multiple roles in promoting PCa. To describe the complete role of lipids in, potential correlation between lipoproteins changes after ADT and progression to castration-resistant prostate cancer should be studied.
Study Limitations
This analysis, however, has certain limitations such as a short follow-up period and the lack of homogeneity in groups and in the methods of treatment. This analysis had different sample sizes of participants involving different populations across the world. In 13 studies, 2 were pooled with RT; hence, hormonotherapy was not the only method of treatment. These studies have no clinical groups of the tumor according to local or advanced stages or clinical tumor, nodes, and metastasis (TNM) stages. Some of the studies had control groups and the time of observations was short—only up to 12 months.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.