
Abstract
The aim of this study was to evaluate mental health issues related to attention-deficit/hyperactivity disorder (ADHD) in young adult male prisoners.
The study was performed in the Pravieniškės Correction House-Open Prison Colony and represents the first study on adult ADHD in Lithuania. The sample consisted of 100 young males imprisoned for mild to moderate crimes. ADHD symptoms were assessed using the Adult Self-Report Scale v1.1 (ASRS v1.1) and Wender Utah Rating Scale (WURS) self-rating scales. Related mental health issues were evaluated using the DSM-5 Level 1 Cross-Cutting Symptom Measure, the Personality Inventory for DSM-5, and data from both medical files and offenses-incentives lists.
Clinically significant ADHD symptoms were found in 17% of the respondents. Prisoners with ADHD were younger and had shorter incentives lists. Personality traits of negative affect, antagonism, disinhibition, and psychoticism with increased personality dysfunction were more prevalent in the respondents with ADHD. Medical files of prisoners with ADHD more frequently included data on substance abuse, psychiatric diagnoses, and psychopharmacological treatment. None of the respondents had been diagnosed or treated for this disorder.
Clinically significant ADHD symptoms were highly prevalent among imprisoned males, but ADHD was not diagnosed or treated correctly. These findings show that the problem of ADHD in young male adults with increased risk for criminal behavior needs recognition by the politicians and professionals responsible for health care in Lithuania in order to better care for prisoners with this psychopathology.
Keywords
Prevalence of adult attention-deficit/hyperactivity disorder (ADHD) varies widely between different studies and methodologies. The World Mental Health Survey Initiative screened 11,000 people aged 18–44 years from 10 countries of Europe, America, and the Middle East. Estimated average prevalence of ADHD in this adult population was reported to be 3.4% with a range from 1.2% to 7.3% (Fayyad et al., 2007). A recent meta-analysis of 42 studies found a fivefold increase in the prevalence of ADHD in youth prison populations (30.1%) as compared with published prevalence rates in the general population. In the same analysis, a tenfold increase was found in adult prison populations (26.2%) in comparison with the general population (Young, Moss, Sedgwick, Fridman, & Hodgkins, 2015). Similar ADHD prevalence findings were reported by Young et al. (2015) in a recent meta-analysis of 42 international studies.
Studies of children and adolescents report that ADHD is related to the increased risk of poor social relationships (Moyá, Stringaris, Asherson, Sandberg, & Taylor, 2014), involvement in delinquent behavior, and substance use disorders (SUDs; Chang, Chen, & Huang, 2007; Kaye et al., 2016; Selinus et al., 2015; Zulauf, Sprich, Safren, & Wilens, 2014). In both adults and children, ADHD is associated with some psychiatric conditions, most frequently mood and anxiety disorders, SUDs, and personality disorders, particularly antisocial personality disorders (Cuffe et al., 2015; Notzon et al., 2016; Young et al., 2017). Affective disorders and anxiety disorders were respectively found to be five times and three times more prevalent among adult prisoners with ADHD than among non-ADHD prisoners (Young et al., 2015). ADHD is associated with substantial personal and individual burden as well as criminality (Katzman, Bilkey, Chokka, Fallu, & Klassen, 2017; Machado, Rafaela, Silva, Veigas, & Cerejeira, 2017; Muld, Jokinen, Bölte, & Hirvikoski, 2013; Taşkıran, Mutluer, Tufan, & Semerci, 2017). Studies have revealed that mild and moderate ADHD symptoms were significantly associated with repeated violence. British researchers found that most cases of violence were related to co-occurring psychopathology (González, Kallis, & Coid, 2013). A study in Sweden reported that association between character maturity and aggressive behavior or psychopathic personality traits remained even when ADHD was controlled (Nilsson et al., 2016). There is a definite association between ADHD and suicidality in both sexes and all age groups (Balazs & Kereszteny, 2017). Treatment guidelines recommend that when ADHD coexists with other psychopathologies in adults, the most impairing condition should be treated first (Katzman, Bilkey, Chokka, Fallu, & Klassen, 2017).
There is a lack of research in this area, largely due to the challenges involved in obtaining the necessary permissions from prison authorities and ethics commissions to investigate this vulnerable population. In Lithuania, ADHD has only gained recognition in the last 16 years. Only in the last 4 years have child and adolescent psychiatrists started comprehensive treatment of patients with ADHD in Lithuania. The first study on the prevalence of and burden associated with ADHD in primary school age children was conducted in Lithuania in 2003 (Leskauskas, Kuzmickas, Baranauskiene, & Daskeviciene, 2004). The prevalence of ADHD was 5.2%, similar to the 5.26% found in other countries. One of the factors which increased the illness burden was reported to be the unavailability of treatment with effective first choice psychostimulant drugs. Methylphenidate was only approved by the State Medicines Control Agency for the treatment of ADHD for the age group 7–18 years in 2015. In the same year, specification for the drug treatment of ADHD in children was approved by the Lithuanian Ministry of Health Care. However, adult psychiatrists in Lithuania are still neglectful about ADHD in adults. This leads to the omission of diagnosis and treatment of older patients, resulting in numerous problems in their health and psychosocial adjustment. One of the possible explanations for this phenomenon is the use of ICD 10 AM (the International Statistical Classification of Diseases and Related Health Problems, Tenth Revision, Australian Modification) classification of mental disorders in Lithuania, which does not provide diagnostic criteria or guidelines for adult ADHD (in contrast with DSM 5 classification which provides specifications for diagnosing ADHD in people older than 17). The goal of this study was to enhance knowledge about the relationship of ADHD symptoms and other mental health issues in incarcerated young adult males.
Methods
The study was performed in Pravieniškės Correction House-Open Prison Colony (PCH-OPC) with the permission of the PCH-OPC director. This study was approved by the Biomedical Research Ethics Committee of the Lithuanian University of Health Sciences (No. BEC-LSMU (R)-02). The invitation to participate in the study was extended to all male prisoners sentenced to 3–4 years for minor to moderate crimes (robbery, violence, defamation, fraud, damage to property, illegal disposition of drugs or psychotropic substances) where the remainder of their prison sentence was greater than 1 year. Prisoners who had been conditionally discharged or released on probation were excluded from the study, along with those who did not wish to take part. Twenty-three prisoners chose not to participate for reasons were not analyzed. The research team administered the self-reporting instruments to six groups of 20–22 participants. Participants were provided with essential information about the study, such as its goal, what the process involved, free choice to participate, any confidentiality issues, and possible benefits of participation. A sample of 100 male prisoners agreed to participate. Each of them was officially invited under the prison rules. Participants who signed the informed consent form and participated in the inquiry received a diploma of gratitude that was beneficial for the future evaluation of their activity in the prison. Participation in the research could be an advantage in their consideration for parole. Individuals who showed motivation to participate in the study could be separated from criminal offenders and accommodated in a safer part of the prison. Participants also got an opportunity to attend a group oriented towards correcting problems related to their personalities. The average age of participants was 28.8 ± 8.6, with a range from 18 to 55.
Prevalence and manifestation of ADHD symptoms were assessed with the Adult ADHD Self-Report Scale v1.1 (ASRS v1.1) and the Wender Utah Rating Scale (WURS). These are the two self-report scales that are widely used internationally and in Lithuania. A respondent was considered as having clinically significant ADHD symptoms if his score was positive on either one of these scales.
(1) The Adult ADHD Self-Report Scale v1.1 (ASRS v1.1) is a standardized and well-validated tool for assessing current ADHD symptoms in adults. The Symptom Checklist consists of 18 questions matched with DSM-IV-TR criteria. Six of 18 items are determined to be the most predictive symptoms consistent with ADHD diagnosis. These six items are the basis for the ASRS v1.1. Four or more items marked in this part of the scale identify that the respondent has symptoms highly consistent with ADHD in adults (Kessler et al., 2007).
(1) The Wender Utah ADHD Rating Scale (WURS) is a 61-item retrospective self-report scale used to evaluate adults for ADHD. In completing the WURS, the adult reports on their recollection of how they were as children. The WURS had been reported to be a valid retrospective screening and a dimensional measure of childhood ADHD symptoms (Ward, Wender, & Reimherr, 1993). Responses to the 25 questions regarding ADHD symptoms count as a 0 to 100 score. The total score increases as the severity of ADHD responses increases. A score ≥50 indicates that ADHD symptom responses are consistent with a definite diagnosis of ADHD.
The presence of other psychiatric symptoms was assessed using the DSM-5 Level 1 Cross-Cutting Symptom Measure. This is a self-rated (or informant-rated) measure that evaluates mental health domains important across different psychiatric diagnoses. This adult version of the measure consists of 23 questions that assess 13 psychiatric areas, including depression, anger, mania, anxiety, somatic symptoms, suicidal ideation, psychosis, sleep problems, memory, repetitive thoughts and behaviors, dissociation, personality functioning, and substance use. Each item inquires how much (or how often) the individual has been affected by the specific symptom during the past 2 weeks (Clarke & Kuhl, 2014).
The Personality Inventory for DSM-5-Brief Form-Adults (PID-5-BF) was used to assess the presence of problematic personality traits. It evaluates 25 specific personality facets residing in five higher order domains (negative affect, detachment, antagonism, disinhibition, and psychoticism). The individual is required to rate how well each item on the PID-5-BF describes him or her. The common domain and overall personality dysfunction scores were reported to be reliable, easy to use, and clinically useful to the clinicians in the DSM-5 Field Trials (Hopwood, Thomas, Markon, Wright, & Krueger, 2012).
Data about health problems, alcohol and substance abuse, diagnosis, and treatment were collected from the medical files of the participants. Offenses and incentives were tallied from the offenses and incentives lists. The average of good and poor behavioral events during the year was calculated and compared among groups.
Descriptive statistics and logistic regression analysis were performed, using Categorical Variables Coding and Crosstabs. Student’s t-test was used to calculate the difference of age distribution in ADHD and non-ADHD subgroups. Pearson’s chi-squared test for categorical data was used to calculate the difference in the distribution of the characteristics between the subgroups of prisoners with and without ADHD. IBM SPSS Statistics Version 21.0. was used to analyze the data.
Results
Prevalence
Twelve out of one hundred respondents (12%) scored ≥50 on the WURS, indicating the probability of ADHD diagnosis. Eleven respondents (11%) marked four or more out of six primary questions on the ASRS v1.1 scale, suggesting that they had symptoms highly consistent with ADHD in adults. Seventeen of the assessed prisoners (17%) had clinically significant scores on either of the ADHD symptoms rating scales and were regarded as the ADHD subgroup in further analysis.
Prisoners in the ADHD group were younger (M = 23.9, SD = 4.4) than those in the non-ADHD subgroup (M = 29.8, SD = 8.6; p < .05, t = 2.75). There was no significant difference between the subgroups regarding education or family status.
Analysis of Medical Files
Analysis of medical records revealed that sleeping disorder and unspecified phobic anxiety disorder were more frequently diagnosed in the ADHD subgroup than in the non-ADHD subgroup (χ2 = 11.594; p < .05; Table 2). It is worth mentioning that ADHD has not been officially diagnosed in any of these people. Prisoners with clinically significant ADHD symptoms were prescribed psychotropic drugs 1.7 times (35.3% vs. 20.5%) more frequently than the ones in the non-ADHD subgroup. This difference did not reach statistical significance, χ2 = 1.748. Antipsychotics were most frequently prescribed (23.5%), but treatments were never ADHD specific with stimulants or noradrenergic drugs.
Other Psychiatric Symptoms
Evaluation with the DSM-5 Cross-Cutting Scale showed that substance use was more prevalent among prisoners within the ADHD subgroup when compared to the non-ADHD subgroup: alcohol 41.2% vs 21.7%, tobacco 70.6% vs 51.8%, illegal and under-the-counter drugs 23.5% vs 14.5%. However, the difference did not reach statistical significance. No significant difference was found in other DSM-5 Cross-Cutting Scale domains.
The Personality Inventory for DSM-5-Brief Form and Offenses and Incentives List
Data derived from the PID-5-BF personality inventory and offenses and incentives list were analyzed using Categorical Variables Coding (Table 1) and Crosstabs (Tables 1 and 2). Traits of personality dysfunction (negative affect, antagonism, disinhibition, and psychoticism) were more prevalent in the ADHD subgroup than in the non-ADHD group (χ2 = 12.617 for negative affect, χ2 = 10.277 for disinhibition, χ2 = 5.876 for antagonism, and χ2 = 9.684 for psychoticism, p < .05; Table 1). Prisoners in the ADHD group had fewer encouragements per year on average (24%) than in the non-ADHD subgroup (52%), as was reported in their offenses and incentives lists (χ2 = 4.529; p < .05).
Personality Dysfunction Traits of Imprisoned Men With and Without Clinically Significant ADHD Symptoms.
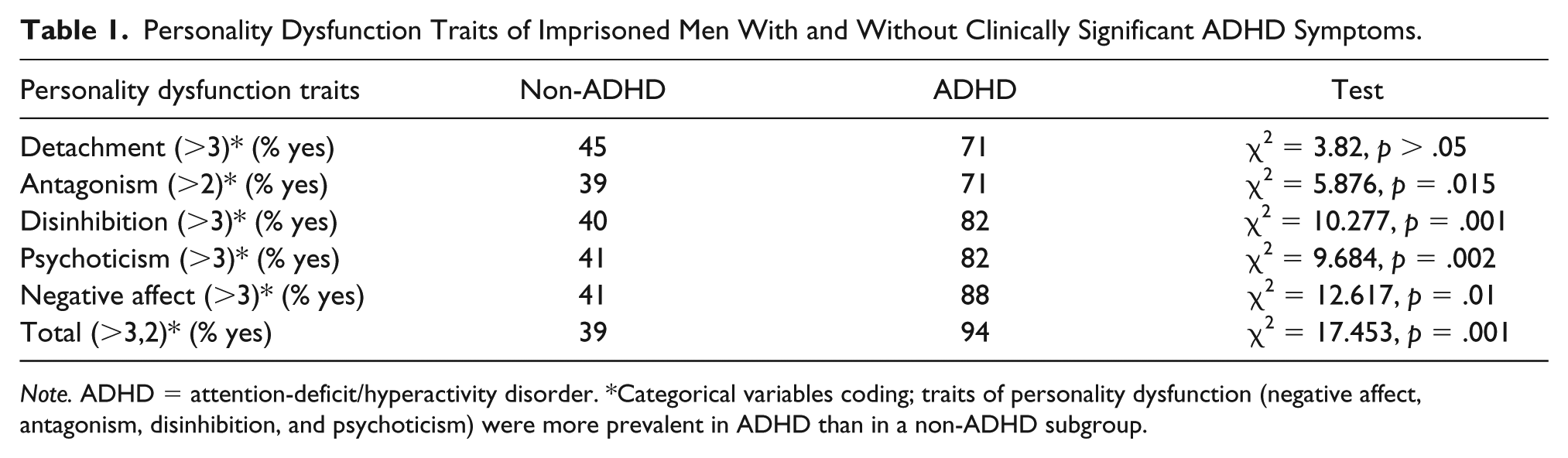
Note. ADHD = attention-deficit/hyperactivity disorder. *Categorical variables coding; traits of personality dysfunction (negative affect, antagonism, disinhibition, and psychoticism) were more prevalent in ADHD than in a non-ADHD subgroup.
Data From Medical Files Analysis of Imprisoned Men With and Without Clinically Significant ADHD Symptoms.

Notes. ADHD = attention-deficit/hyperactivity disorder. Analysis of medical files revealed that sleeping disorder and phobic anxiety disorder unspecified were more frequently diagnosed in ADHD than in non-ADHD subgroup (χ2 = 11.594; p < .05).
The following independent variables were included in the multidimensional logistic regression analysis to predict whether a subject would be in the ADHD subgroup: age, detachment, antagonism, disinhibition, psychoticism, and negative affect. The responses of all subjects were analyzed. A selective stepping regression was used to eliminate variables, thus leaving only those the model used to predict the clinically relevant symptoms of ADHD. Using this method, 88% of respondents were correctly classified. Results of the multidimensional logistic regression model showed that the significant indicators of ADHD symptoms include age (OR = 0.875, CI [0.828, 0.925], p = .00), antagonism (values >2, OR = 5.382, CI [1.354, 21.396], p = .017), and disinhibition (values >3, OR = 3.832, CI [1.012, 14.513], p = .048). The model predicted the presence of ADHD symptoms with 88% accuracy (model suitability − determination ratio R2 = 0.679).
Discussion
The prevalence of ADHD is consistently found to be higher in the prison population than in the general population. Results of other studies report that many adults with ADHD are treated poorly or remain undiagnosed and untreated (Gajria et al., 2014; Ginsberg, Quintero, Anand, Casillas, & Upadhyaya, 2014). Hence, the goal of this study was to evaluate mental health issues among young adult male prisoners who present ADHD symptoms. Clinically significant ADHD symptoms were found in 17% of the respondents. The main findings of this study are first, that none of the participants with obvious ADHD symptoms had been diagnosed with ADHD and properly treated before. Second, prisoners with ADHD had more comorbid psychiatric and behavioral problems. Third, ADHD in young prisoners was related to increased personality dysfunction and the traits of negative affect, antagonism, disinhibition, and psychoticism. Furthermore, prisoners with ADHD symptoms in this study more frequently had anxiety, sleep disorders, and traits of personality disorders. This finding concurs with other studies on ADHD diagnosis in adults (Cuffe et al., 2015; Notzon et al., 2016) and behavioral problems (Stoel, Houtepen, van der Lem, Bogaerts, & Sijtsema, 2018). The current study has shown that young adult male prisoners with ADHD symptoms have complex mental health issues, which in turn indicates the need for proper diagnosis and treatment of adult ADHD in this population. The major findings of this study suggest the need for increased education among Lithuanian psychiatrists, especially those that work in prisons with this population. In addition, policy-makers need to be aware of this issue to effectively allocate funding to support therapeutic services in prisons for young adult males.
It is noteworthy that prisoners in the ADHD subgroup were younger. This finding demonstrates the need for more reliable diagnosing of ADHD among youth prison populations to prevent future mental health problems and antisocial behavior (Langley et al., 2010). In Lithuania, there is better diagnosing and treatment of ADHD among children and adolescents. It would be valuable to assess ADHD prevalence among the adolescent population in the juvenile correction system and to make a prospective study how adequate treatment affects further delinquencies.
The main contribution of this study was the evaluation of mental health problems related to ADHD symptoms in imprisoned male population and comparison between the subgroups of prisoners with and without ADHD symptoms.
The main limitations of this study were the relatively small sample size and the lack of a locally sampled comparison group. Another limitation was that all interviews were based entirely on self-reports. As with any study, these findings require replication, which could decrease the risk of false positive results. Further research with larger populations is needed to evaluate and clarify the prevalence of ADHD (not only ADHD symptoms) and coexisting mental health problems.
Conclusion
Clinically significant ADHD symptoms were highly prevalent among imprisoned males but ADHD was not diagnosed or treated correctly. Prisoners with ADHD were younger, and they had more psychiatric and behavioral problems than other prisoners did. ADHD in young prisoners was related to increased personality dysfunction and the traits of negative affect, antagonism, disinhibition, and psychoticism. These findings show that the problem of ADHD in young male adults with increased risk for criminal behavior needs recognition by the health-care politicians and professionals in Lithuania. With this knowledge, they would be more likely to provide better care for prisoners with this psychopathology. Effective means for the diagnosis and treatment of adult ADHD need to be developed and made available for health-care specialists working with this vulnerable population.
Footnotes
Acknowledgements
Authors would like to thank Egle Sepetauskiene for the help with statistical analysis and David Harrison for his language review and comments on an earlier version of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Article Processing Charge was paid by Lithuanian University of Health Sciences Hospital Kauno klinikos (Department of Psychiatry).
Ethical Approval
This study was approved by the Biomedical Research Ethics Committee of the Lithuanian University of Health Sciences (No. BEC-LSMU (R)-02).