
Abstract
The aim of this study is to explore the social support of male breast cancer patients (MBCP) in Germany. In particular, three aspects of social support focus on (a) the used resources within the social environment, (b) the received support, and (c) the differences of used social support between MBCP. A mixed-methods design is applied including data of qualitative interviews (N = 27 MBCP) and a written questionnaire (N = 100 MBCP). MBCP use different resources of support from their social environment like partners, family, friends, colleagues, other breast cancer patients, and medical experts. Mostly, MBCP receive emotional and informational support. They often receive emotional support from their partners and informational support from medical experts. Different types of social support usage can be identified dependent on age, occupation, and severity of disease. The older the patients and the less the disease severity, the less social support MBCP use. Within cancer care, partners and the closer social environment should be included more as they are a key resource for MBCP. As health-care professions might also be an important resource of support for MBCP, further research should examine this resource.
Breast cancer is the most common type of cancer in women (Bray et al., 2018) and is often treated as a typical women’s disease in Western societies. Nevertheless, with a rising number (Giordano, 2018; White et al., 2011), 1% of new breast cancer diagnoses in Western societies occur in men (Miao et al., 2011). The disease is rare in men and because of its feminization, patients experience psychosocial burdens such as emasculation (da Silva, 2016; Donovan & Flynn, 2007; France et al., 2000; Iredale, Brain, Williams, France, & Gray, 2006; Swergold, Murthy, & Chamberlain, 2014), stigmatization (Andrykowski, 2012; Bunkley, Robinson, Bennett, & Gordon, 2000; da Silva, 2016; Midding et al., 2018), and isolation (Bunkley et al., 2000; Iredale et al., 2006). Some male breast cancer patients (MBCP) experience clinical burdens, as many health-care providers are never confronted with an MBCP. Because of the rareness of disease (Fentiman, 2018), it can be assumed that experiences in dealing with MBCP are missing among health-care providers. Since clinical studies of breast cancer are mostly based on clinical studies and needs of female breast cancer patients, needs of MBCP are hardly represented (Giordano, 2018; Gómez-Raposo, Zambrana Tévar, Sereno Moyano, López Gómez, & Casado, 2010). Because of these aspects, social support is important for MBCP, as it may buffer the burdens. For cancer patients in general, social support positively affects the mindset and the healing process (Helgeson & Cohen, 1996) and coping (Kim, Han, Shaw, McTavish, & Gustafson, 2010). Social support is associated with less depression (Hann et al., 2002). Kulik and Mahler (1993) state that male cardiac patients were released from the hospital faster if they received social support. Especially for (female) breast cancer patients, social support reduces the stress of cancer diagnosis (Israel & Schurman, 1990) and enhances emotional well-being (Dukes Holland & Holahan, 2003; Dunkel-Schetter, 1984).
Former studies identify that it is important to investigate social support of MBCP in particular, as men are different from women with regard to this dimension in many ways: MBCP without support of a partner experience more psychological distress and are less able to fight. In contrast, for women, partner support has no effect on psychological support and coping (Taniguchi, Akechi, Suzuki, Mihara, & Uchitomi, 2003). Several studies report that MBCP receive less social support than female breast cancer patients (da Silva, 2016; Donovan & Flynn, 2007; Iredale et al., 2006; Robinson, Metoyer, & Bhayani, 2008). Moreover, MBCP often do not talk about their diagnosis beyond their closest social environment to prevent stigma and embarrassment (Andrykowski, 2012; Bunkley et al., 2000; da Silva, 2016; Midding et al., 2018).
Social support describes the interaction between two or more people with the aim to change or to make a problem of a person more bearable if nothing can be changed (Schwarzer, 1996). There are three dimensions of social support: emotional support like caring, compassion, spending consolation, warmth and physical affection; instrumental support like tangible assistance or material goods; and informational support like imparting information or giving advice (Knoll, Scholz, Rieckmann, & Schwarzer, 2011; Schwarzer, 1996). The sources of support can be extensive. However, most processes of social support take place in closer social relationships, such as in a partnership, with family, or in friendships (Schwarzer, 1996). Accordingly, referring to this concentration, the present study concentrates on this (closer) social environment of MBCP. As studies of the state of research report, MBCP receive mainly support from their partners (France et al., 2000; Iredale et al., 2006; Pituskin, Williams, Au, & Martin-McDonald, 2007), both in terms of doctor visits as well as in the course of the disease (Williams et al., 2003). France et al. (2000) also identify that female friends suffering from breast cancer can be a resource for receiving informational support, and some MBCP have the feeling that no professional support is needed. Concerning support groups as a source of social support, MBC-specific support groups are rare (Bunkley et al., 2000; da Silva, 2016) and men often do not want to attend female breast cancer support groups (da Silva, 2016; Iredale et al., 2006; Robinson et al., 2008; Smolin & Massie, 2002).
Keeping those aspects in mind, the state of research gives an idea of available support resources of MBCP, but not in a satisfying way. It further remains unclear what dimensions of social support MBCP use (emotional, informational, instrumental) and which specific resource they use for the different dimensions of support. Therefore, the aim of this study is to investigate (a) what resources of social support MBCP in Germany use within their social environment, (b) what kind of social support (dimensions) they use, and (c) if different types of support-seeking and support-using behavior in MBCP concerning the heterogeneity of used resources can be identified.
Methods
Study Design
This study is part of the N-MALE project conducted between 2016 and 2018 in Germany. It was funded by the German Cancer Aid and approved by the Ethics Committee for Bonn (Germany).
A mixed-methods analysis was used to explore and understand the needs of MBCP. Within this triangulation, both methods, qualitative and quantitative, were treated equally (Carell, 2005). Therefore, semistructured interviews and a postal survey were conducted. The postal survey was conducted before the interviews. For further information on the methods used in the N-MALE project, please have a look at Midding et al. (2018; open access publication).
Study Inclusion and Participants
To take part in the study, MBCP had to have a confirmed breast cancer diagnosis (C50.x or D05.x) and a written declaration of consent. Exclusion criteria comprised a missing or withdrawn written declaration of consent or aspects that complicate interviewing (e.g., speech or comprehension problems, advanced cancer, psychosis, and dementia).
Access to the field was given through certified breast cancer centers, the Men with Breast Cancer Network (Netzwerk Männer mit Brustkrebs e.V.), and personal contacting of interested MBCP.
For qualitative data, sampling was carried out using the strategy of theoretical sampling of Glaser, Strauss, and Paul (2008) to find as significant and contrastive cases as possible. Therefore, the postal survey was used to find participants who varied in sociodemographic aspects, facts of disease, experiences during treatment, and contact with support groups. Patients were included into the study until theoretical saturation was reached.
Data Collection
Collection of data was between April 2016 and October 2017.
Qualitative data
For the semistructured face-to-face interviews, an interview guideline structured along the steps of cancer therapy was created and pilot tested. The interviews lasted between 1 and 2 hours and were audio recorded and anonymized transcribed following approved standards (Fuß & Karbach, 2014).
Quantitative data
Social support was measured by the validated Modified Medical Outcomes Study Social Support Survey short scale (mMOS-SS) by Moser, Stuck, Silliman, Ganz, and Clough Gorr (2012). It refers to social support within the private social environment and has two subscales: emotional support and informational support. The scale contains eight items (four items for each subscale) to be answered on a five-point scale from 1 (never) to 5 (always).
The questionnaire included instruments of support accomplished by self-generated factual items. The first instrument measures the contact of MBCP with other breast cancer patients (BCP) with three dichotomous (yes/no) items: (1) “Do or did you have contact with other men with breast cancer?” (2) “If no, have you wished to have contact with other men with breast cancer?” (3) “Do or did you have contact with women with breast cancer?” A fourth item measures MBCPs’ needs of support from support group: (4) “Do you need support from support groups since your breast cancer diagnosis?” with the answer categories: (a) “Already taking part in support group”; (b) “No I do not need the support of a support group”; and (c) “Yes I need the support of a support group” (unmet need).
Aspects of the disease (time since breast cancer diagnosis, first time or relapse, received cancer treatment) and sociodemographic data (age, family status, children, education, and occupation) were collected with factual single items.
Data Analysis
Analysis of qualitative data
The transcripts were analyzed using summarizing qualitative content analysis 1 (Mayring, 2016). Coding was done deductively and inductively using MAXQDA software version 12.2.1 (VERBI GmbH, 2016). An alternating interviewing and analyzing process was applied, where categories were developed and tested within the following interviews to make purposeful sampling possible (Helfferich, 2011).
Statistical analysis of quantitative data
For statistical analysis, SPSS version 25 (IBM SPSS Statistics, 2017) was used and descriptive statistics (cross-tables, quantities) were applied. The social support scale was analyzed according to the “Social Support Survey Instrument Scoring Instructions” (RAND Health). A score for each item and a score index for each subscale were computed. A higher score indicates a higher amount of support (RAND Health).
Mixed-methods analysis
For mixed-methods analysis, data of N = 27 MBCP with both available qualitative and quantitative data were included. The data were merged, containing codes of qualitative analysis (dimensions of social support) and data of quantitative analysis such as sociodemographic aspects (age, family status), disease-related aspects (breast cancer for the first time/relapse, treatment in cancer care system), and contact with other BCP (contact with support group, contact with male/female BCP). Scores of the social support scale (emotional and instrumental support) per person and per type were included.
Findings
Sample Characteristics
N = 100 MBCP sent back an evaluable questionnaire (cleared response rate = 85.5%). N = 27 interviews with MBCP were conducted from this sample. Sociodemographic and clinical characteristics of the quantitative sample and the (qualitative) subsample are presented in Table 1.
Demographic and Clinical Characteristics of Participants.

Note. Quantitative sample N = 100; qualitative sample (subsample) N = 27. Numbers of qualitative sample in brackets.
Resources of Social Support in Social Environment
Findings of the qualitative interviews demonstrate that MBCP use different resources of social support in their social environment (nonprofessional support; Figure 1). Within the close social environment, they use their partner, family, and friends. Within their wider social environment, resources like colleagues 2 and other male or female BCP or support groups are used. Some MBCP have personal contact with medical experts who can be a source of social support for them. Medical experts can be classified into closer and wider social environment, as they can be part of both (e.g., a family member with a medical background or colleagues/other BCP with a medical background).

Resources of social support of male breast cancer patients.
Basic requirements to use resources are availability and access. Most participants have a partner (quantitative sample = 87.2% (qualitative sample = 79.2%)) and children (84.0% (76.9%); Table 1). Support from colleagues depends on the occupational position. Since participants are 66.9 (64.8) years on average and only 30.9% (30.5%) are still working (full-time and part-time), the resource of colleagues for social support is not available for most participants. Concerning other BCP, most men have contact with female BCP (63.2% (73.1%); Table 2). In comparison, 24.2% (46.2%) of the participants have contact with other MBCP. The majority of participants who had not had any contact with other BCP so far do not want to have contact with them (contact with MBCP 82.4% (64.3%) and contact with female BCP 90.0% (75.0%)). As it is known from personal interviewing, medical experts are not available for every participant, as not everyone knows a person working in the medical system within their social environment.
Contact of Male Breast Cancer Patients With Other Breast Cancer Patients.
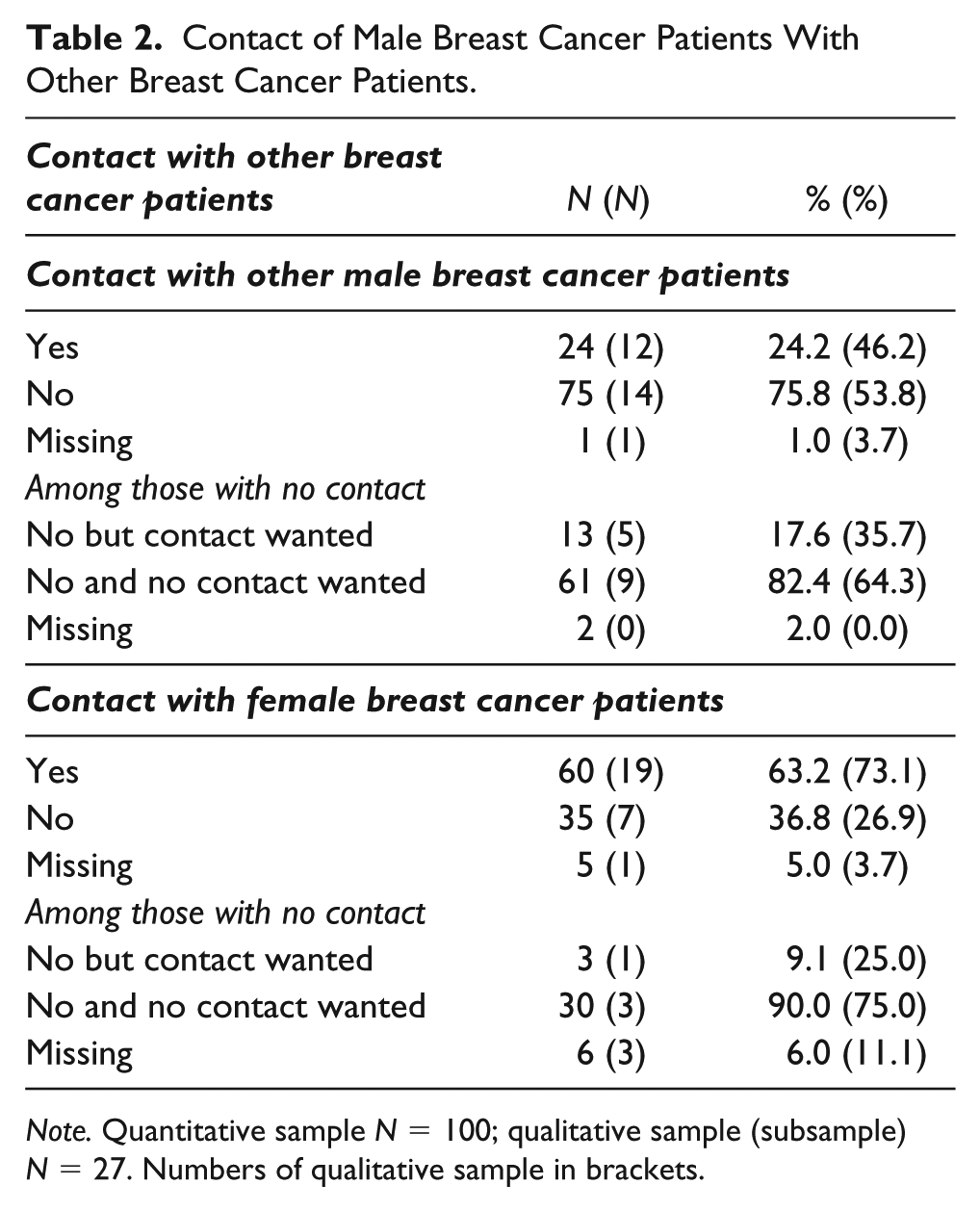
Note. Quantitative sample N = 100; qualitative sample (subsample) N = 27. Numbers of qualitative sample in brackets.
Regarding contact with other BCP within a support group, 15.3% (40.0%) of the participants are part of a support group; the majority of participants are not (84.7% (61.5%); Table 3). Further, most participants state that they do not wish to be part of a support group (96.3% (93.8%)).
Male Breast Cancer Patients’ Needs of Support From Support Group.
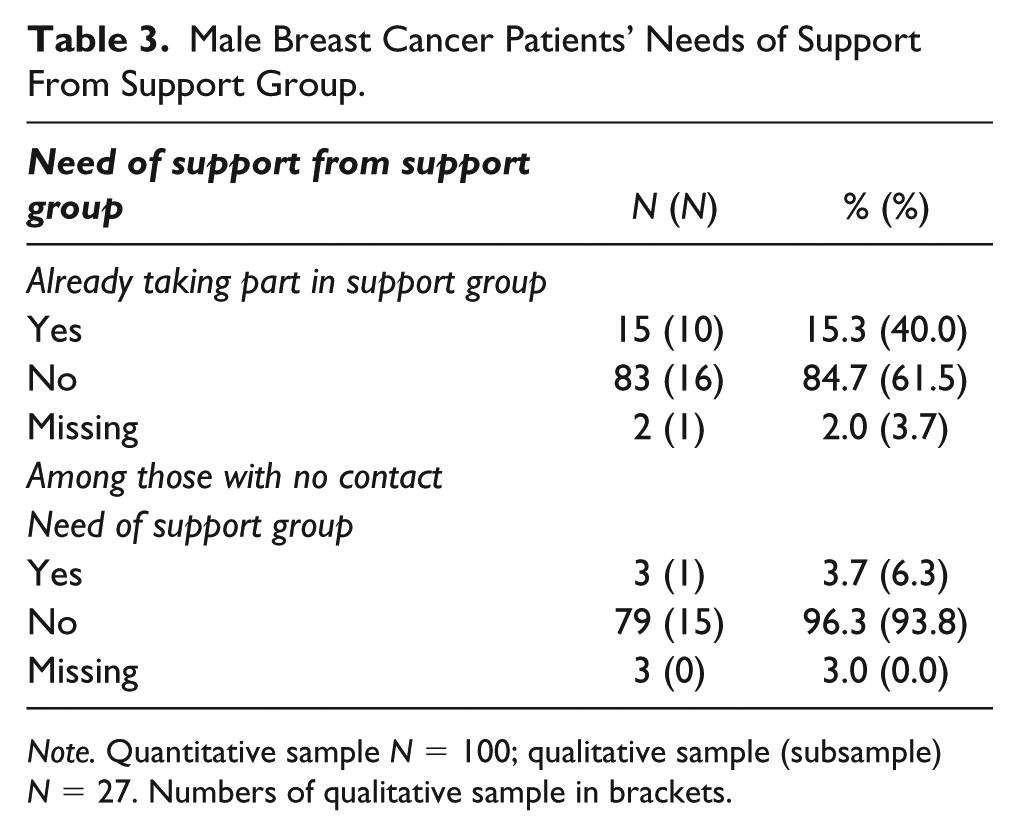
Note. Quantitative sample N = 100; qualitative sample (subsample) N = 27. Numbers of qualitative sample in brackets.
Qualitative results suggest that there are different reasons why participants do not want support from a support group: They may feel no personal need to have contact with other BCP or they are afraid of depressing talk and do not want to be confronted with the disease any more: “I had no interest in that. [..] I said: Okay I had it, but it’s over. Basically, I don’t want to [..] always be confronted with it. […] they partly described their complaints there.” (ID no. 91)
Dimensions of Social Support
Emotional support
As the results of the qualitative analysis identify, emotional support is the support the participants receive the most. The key resources of this support are widely spread over the close social environment such as partner, family and friends, colleagues, and other BCP. The resources differ in functions.
Many participants state their partner is the key resource of support, when it comes to talking about the disease and emotional or personal aspects: “My wife is also the first contact person for me, of course.” (ID no. 43)
Furthermore, they spend emotional support by being present, backing, creating an everyday atmosphere, and giving confidence and hope: “Everything went on as before. It wasn’t a huge thing: “And you are sick.” […] Everything was going on. I knew the disease was a burden for the family. But they somehow dealt well with it. So I did not get the impression that this would be a thing for the family that took their joy in life. [..] And of course that’s something that helped me a lot.” (ID no. 16)
Friends are also there for talking and being around but also “to blow away the cobwebs” or to be insightful: “How they contacted me, how OFTEN they contacted me. They just came over and knocked at the door: “We just wanted to check on you.” ” (ID no. 19)
Colleagues spend emotional support by understanding the patient’s situation or if the relationship is more intense even as conversation partners: “The reactions were extremely positive. So JUST from my students, that was really great and gave me a lot of power.” (ID no. 99)
Other male or female BCP or other patients of support groups send recovery wishes, give confidence, and keep them grounded. They are further a resource for communication about the disease and disease-related aspects, as they are in a similar situation: “So now I have written again that I’m in the clinic now. And they’ve answered briefly and wished me all the best.” (ID no. 11)
Some participants completely avoid emotional support and do not want to talk about their disease: “I’m not like that, […] that I absolutely need someone to talk to.” (ID no. 67).
Informational support
Informational support is the second most received form of support (after emotional support). It is more often provided by persons who are experts because they have either a medical background or experience with the disease and therefore can provide MBCP with information.
Partners and family members can give informational support independent of their medical or breast cancer experiential background, as they are often the ones who send the men to the doctor: “And then my wife actually said: “Your left nipple looks a bit different than the right one.” Pulled in so easily inside. The edge of the nipple. I didn’t even think about that […]. But still, that was actually the trigger then. And then I actually went to my family doctor.” (ID no. 55)
In the personal surrounding, family members with a medical background can play an important role. They have a special position because they belong to both systems, the personal surrounding and the health-care system. In this case, they can give advice, for example, to health-care facilities or act as medical counselors and explain ambiguous medical statements (also being translators) to the participants or give information on breast cancer: “My sister is a doctor. That’s also my best guide. She isn’t a medical specialist. She’s an anesthesiologist, but of course has contacts. And of course, then can enlighten directly.” (ID no. 99)
Other BCP play a key role for MBCP if they have and want to have contact with them: For some men they are the first person of contact when it comes to breast cancer specific aspects, not at least because of their availability compared to providers. Moreover, they are important for MBCP to inform themselves about experiences of the disease and to get some advice (e.g., concerning health-care facilities). They also have a function as translators for medical information: “It was a bit like that, you just think, when you talk to an AFFECTED guy, that’s quite different from talking to doctors. And that has really been good for me.” (ID no. 43)
Other participants avoid informational support, as they do not want to have too much information: “I’m not the person who reads everything in particular. I’ve already said in the beginning. But I take things the way they come. And it doesn’t help me if there is a lot of information [..]. I have to help myself.” (ID no. 63)
Instrumental support
The third dimension of social support is the least used by participants and is mainly focused on the private surrounding—mostly on the partner. However, the participants also use support of colleagues and other BCP.
Instrumental support is usually given by the partner, for example, by providing a shuttle service, joining medical consultations, providing body care, caring for the participants, taking care of everything, subordinating themselves, and providing social security: Wife: “He can’t wash himself properly. So I washed him. I also put some cream at him at the moment, I cut his fingernails and toenails.” (ID no. 82)
The family has the role of providing shuttle service, being present at medical consultations and taking care: “As the diagnosis was breast cancer he said [father]: “I drive you, I support you, I’m with you.” And so he got involved very, very much and later on to chemotherapy. He always picked me up here, drove me there, then at noon, when I was through, then I could call him and he picked me up.” (ID no. 12)
Friends are there as well for shuttle service and offer support, which the men often did not make use of: “Yes, so I was asked from my [..] friends if there is something to do somewhere, where I just can’t do physically or anywhere, or I need support: “If you need someone or something”—that actually worked.” (ID no. 55)
Colleagues offer flexibility within the job or concerning working conditions: “Within the therapy, I always went back to work when I felt better. So I talked to my employer and he said it’s okay for him, I can do that.” (ID no. 16)
Other BCP provide instrumental support, as they help accelerate the processes within the health-care system or help with the transfer to the breast cancer center: “In fourteen days or three weeks, the result was there. [..] That was fine, it was fast. It’s not as long as some women do. Okay, I just put pressure, that’s logical. And the [naming chairman self-help], of course, too.” (ID no. 67)
The role of medical experts concerning instrumental support is to connect MBCP with providers, to select a rehab center, or to offer medical and cosmetics support: “So fortunately, she is a doctor herself, an internist. She’s working with a health insurance company as a consultant doctor has since contact with rehab clinics. WITHOUT her, I wouldn’t have done it that way.” (ID no. 77)
On the other hand, some MBCP state that they do not need any instrumental support: “I didn’t have any physical limitations. I was immediately completely active in life again. I think that’s a bit different between people. There are many who, I say in quotation marks, who care for their illness and are affected by their illness. And for me is actually […] I’ve felt no impact because after the surgery, after three, four days you have no pain anymore.” (ID no. 87)
Social Support Scale
Scores for the availability of social support range from 1 to 5 within the two subscales of emotional and informational support. The mean of emotional support is 4.39 (4.49) and that of informational support is 4.42 (4.41) (Table 4).
Availability of Social Support of Male Breast Cancer Patients (N = 100).

Note. Reference of the subscales: Moser et al. (2012).
Types of Used Social Support
The participants (N = 27) can be divided into different types concerning their usage of social support resources within the dimensions of social support (emotional, informational, instrumental). Table 5 presents this mixed-method matrix. 3 Sociodemographic and disease-related characteristics of the types in total are presented in Table 6. 4
Mixed-Methods Matrix – Types of Used Social Support.


Note. First time = breast cancer for the first time; Relapse = relapse of breast cancer. S = surgery; C = chemotherapy; A = adjuvant radiation; R = rehabilitation; H = hormone therapy; BCP = breast cancer patient; FBCP = female breast cancer patient; MBCP = male breast cancer patient.
Qualitative results of social support per patient; x = received social support within this dimension; As sociodemographic and disease-related aspects were collected with different methods (questionnaire and interview), there are some deviations (if comparing data of qualitative sample within Tables 1 and 5).
Quantitative results of availability of social support (Table 4) per patient and per type (results of the subscales emotional support and instrumental support).
The four different types are marked by different colors (type 1: white; type 2: green; type 3: orange). Total scores: Type 1 = 0; Type 2 = 1.0–3.0; Type 3 = 3.1–5.0.
Age groups: 1 = 40–44 years; 2 = 45–49; 3 = 50–54; 4 = 55–59; 5 = 60–64; 6 = 65–69; 7 = 70–74; 8 = 75–79; 9 = 80–84; 10 = 85–89.
Demographic and Clinical Characteristics of Types.

Three different types can be identified: Type 1 does not use any social support during the breast cancer disease. Nevertheless, the added group score of the mMOS-SS support scale identifies that the participants within this group mostly have someone who offers them emotional (mean = 4.4) and instrumental support (mean = 4.5). With an average age of 78 years, it is the oldest type and consists of two participants. Concerning aspects of disease, both participants within this type have breast cancer for the first time and have just received cancer care in the form of surgery (100%) or surgery and hormone therapy (50%; Table 6). Concerning their occupational situation, the men within this type are certified sick or are retired.
The second type uses different resources of social support from one to three categories of social support during the process of disease. They use a minimum of two resources and the number of used supports falls between those of the two other types. The total score of the social support scale indicates that they mostly have someone who offers them social support, but the mean value of support is the lowest among the groups (mean emotional support = 4.2, mean instrumental support = 4.4). With 17 participants, it is the biggest type, with a younger age on average compared to Type 1, 66.6 years. Regarding aspects of the disease, these men have breast cancer for the first time (94.2%) or are experiencing a relapse (5.8%). In cancer care, the treatment is widespread, as some men had only surgery, while others also had chemotherapy (52.9%), adjuvant radiation (58.8%), hormone therapy (94.2%), and rehabilitation (58.82%). Most men within this group are not working (retired 52.9% or certified sick 23.5%).
The third type receives social support from two or all three categories of social support. This type uses the most different resources of support and has the highest amount of used support. The availability of social support has the highest mean value of the types (mean emotional support = 4.7, mean instrumental support = 4.8). There are eight men within this type. It is the youngest type with an average age of 57.5 years. All participants within this group have breast cancer for the first time (87.5%) or are experiencing a relapse (12.5%) and are being given a high amount of cancer care on average, as most of the participants received several steps of cancer treatment (chemotherapy 87.5%, adjuvant radiation 75.0%, hormone therapy 100.0%) Regarding the occupational situation, half of the men within this group are working (full-time 37.5%, part-time 12.5%) and the other half are not (retired 25.0% or certified sick 25.0%).
Discussion
The aim of this study was to determine the social support of MBCP within their social environment: What resources do they use? Within which dimensions do they receive support? Are there different types among MBCP concerning the heterogeneity of used resources?
Resources
MBCP use a variation of resources for social support. Within their closer and wider social environment, they “use” their partner, family, friends, colleagues, other BCP, and medical experts. Concerning the partner, most participants have a partner, who is the key source of social support for some of them. This is congruent with the findings of Iredale et al. (2006) and France et al. (2000), who state that MBCP mostly use their partner and female friends for social support. Regarding medical experts within the social environment, they are of particular importance for social support, as they involve a trust-based relationship and provide information. As Ernstmann et al. (2017) report, a close and trusting relationship between patient and provider leads to patient enablement for oncology patients. Furthermore, if there is a medical expert within the social environment, the access and availability is much easier than contacting an unknown professional within the cancer care system. Because of this double role of medical experts, it might be easier for them to explain difficult medical topics to the patients, as they can also speak on a personal level, not only the professional one. In addition, medical experts are very important because of the rareness of the disease. Often, there is not very much information available for MBCP about the disease and many men do not know about breast cancer in men before they get the disease.
Whether the working environment can be used as a source of support depends on the occupation and the atmosphere within the working place of the individual participant and if it is established there or possible to talk about personal problems. As former studies report, social support within the working environment can improve the health of employees (Jung et al., 2012; Liukkonen, Virtanen, Kivimäki, Pentti, & Vahtera, 2004).
Regarding other BCP, most participants have contact with female BCP, while contact with MBCP is quite rare. This might be connected with the rareness of the disease. In social surroundings as well as within the cancer care system, MBCP often only meet female BCP. Furthermore, the majority of the participants do not want to have contact with a support group. That is congruent with the results of Pituskin et al. (2007). Concerning rare diseases, support groups are often the only option to meet other patients—in this case MBCP. There is a specific support group for men, but it is not clear how well known this support group is for MBCP. Within the interviews, some men stated that they did not know about a male-specific support group for breast cancer, although it can be found on the Internet. Maybe knowledge of the existence of this support group would increase the interest of some MBCP to have contact with a support group. As former studies report, MBCP would prefer support groups only for men (Brain, Williams, Iredale, France, & Gray, 2006; da Silva, 2016; Farrell et al., 2014; Iredale et al., 2006). Patients who experienced a male breast cancer (telephone) support group recommend it to other patients for coping with the disease (Farrell et al., 2014). It needs to be taken into account that some participants state that they do not want personal contact with other BCP because they are afraid of depressive talk and do not want to be confronted with the disease anymore. So, it might also be an issue of coping whether someone wants to attend a support group or not. As a study by Batenburg and Das (2014) reported, (female) BCP who cope with their emotions more actively have more benefit from a support (online) group than patients who cope less actively with their emotions.
Dimensions
The availability of social support is generally high for MBCP as the social support scale demonstrates. Qualitative and quantitative data identify that emotional support is the most used and most available resource for the participants. It is mostly provided within the closer social environment such as family and friends, but also by other BCP and colleagues who can spend emotional support to the patients. This usage of different resources is in contrast to the results of Pituskin et al. (2007), as they reported that there is no emotional support outside the family. Maybe family means privacy. This private atmosphere and trust can also be created within other social relationships such as other BCP or colleagues. But not every patient wants to be emotionally supported; there are men who avoid emotional support. It can be assumed that this avoidance is an aspect of gender, as Quincey, Williamson, and Winstanley (2016) discussed: Expressing emotions is seen as a feminine characteristic (Moynihan, 2002) and especially men following “traditional hegemonic masculinities” do not want to assume a “feminine” practice of coping (Quincey et al., 2016).
The necessity of informational support might be related to the low information level of male breast cancer. As it is information based, this dimension is more focused on experts of (male) breast cancer who can provide information on the disease, such as persons with a medical background (medical experts) or people who have personal experiences with the disease, such as other BCP. Thaxton, Emshoff, and Guessous (2005) support those results, as they identified that for prostate patients, men benefit from the information exchange of support groups. MBCP differ in the level of information needs, as there are MBCP who do not want to receive too much information. This might also be associated with an avoiding coping style (Brain et al., 2006).
Within instrumental support, there is the largest variance, as some men receive instrumental support and others do not. Qualitative data reveal that instrumental support is less used by MBCP. This might be explained by the fact that some of the participants were in an early stage of the disease and they do not yet feel the need for instrumental support. If instrumental support is used, it is mostly focused on the private surroundings, such as the partner. Friends provide it, but men do not make use of it very often. Nevertheless, the majority of the participants state that instrumental support is available for them if needed (quantitative data).
Typification
The three types of social support usage demonstrate the variance of social support between MBCP. Since the types differ in age, occupational situation, and received cancer therapy, there might be an association between age, occupational situation, severity of the disease, and social support. Concerning age, the older the patients are, the less (resources of) support they use. Therefore, Meléndez, Mayordomo, Sancho, and Tomás (2012) reported that coping strategies in problem solving and social support seeking decrease with age. Reasons for this might be that the resources of support become less, as the family gets smaller (death of partner and other family members, children moving out) and the social contact points often decrease (e.g., no colleagues in retirement). In addition, studies report that life satisfaction increases with age (starting from middle age; Wolff & Tesch-Römer, 2017). Even with health restrictions, life satisfaction can be high in old age (Staudinger, 2000). This could be another reason for less support seeking of elderly MBCP. Nevertheless, all patients within this group (and within other groups as well) state that they have the availability of social support if they need it (emotional, emotional/informational, and instrumental). Another reason might be the image of masculinity of this generation of men, as they do not want to talk about personal problems and emotions. As Meléndez et al. (2012) identify, older men especially use a more problem-solving, coping style, which is less emotional than the coping style women of this age use. Furthermore, woman look more intensively for social support. With increasing age and beginning retirement, one is not any longer within a working environment, which is why the occupational situation might have an influence on the availability of the resource of other colleagues.
Regarding severity of disease, there are indications that patients who receive a higher amount of therapy often use more resources of social support. As a disease gets more serious, more topics and worries arise that need to be handled or coped with by the patients. For example, they cannot do daily routines anymore and therefore they need (instrumental) support from others. Corbin and Strauss (1991) state in their trajectory model that more social support is needed especially in severe cases of chronic disease within phases of transition (e.g., from stable to unstable phase).
Furthermore, the use of social support also depends on one’s need of support and coping style. As Type 1 demonstrates, the patients mostly have the availability to use social support, but they do not use it during their breast cancer journey. Quincey et al. (2016) state that some MBCP stay away from several coping strategies to protect their masculinity, as the disease is feminized itself. It can be assumed that patients from this sample who totally reject social support want to protect their masculinity, as seeking social support is associated with a female coping style, since women are more socialized for seeking support (Moynihan, 2002; Quincey et al., 2016). Also, this avoidance of social support may cause stigmatization, as some MBCP want to hide their diagnosis (Midding et al., 2018).
Reflection and Study Limitations
Reflecting on the relationship between the interviewer and participants of this study, taking part in the study, and doing a personal interview was also some kind of social support (especially emotional support) for some of the participants. This was confirmed by statements of the patients or by concluding their behavior within or after the interview as a feeling of “There is someone who is interested in me and my worries.” It can be concluded that social support is missing somehow for some MBCP.
Within this study, it was not possible to differentiate between actual and personally felt support, as suggested in the literature (Schwarzer, 1996). The support could only be measured by a personal estimation of the participants. For a measurement and a comparison of the actual and personal felt support, an observation would have been necessary.
Practical Implications and Further Research
As the partner and the close social environment (family and friends) play an important role for the social support of many MBCP, it should be included more in cancer care. Currently, relatives of cancer patients can be involved in the discharge management in the hospital or rehabilitation stay in Germany (Deutsche Vereinigung für Soziale Arbeit im Gesundheitswesen, 2013).
As the specific support group for MBCP in Germany is not known to all patients, health-care professionals should provide the patients with this information. As support groups provide a lot of informational and emotional support, they can be useful for patients who look for that kind of support. Furthermore, social support groups can be recommended to MBCP who are confronted with the disease and are willing to talk about the disease and share experiences with other MBCP.
Following the results of this explorative cross-sectional study, they can be considered within longitudinal studies or interventional designs to find out what effect social support or support groups have for coping with the disease or for life satisfaction of MBCP.
Previous research identifies that social support by health-care providers can be an important resource for cancer patients (e.g., Dunkel-Schetter, 1984). In the future, social support from health-care professionals needs to be examined, as it can be assumed that they are also an important resource of support for MBCP.
Footnotes
Acknowledgements
We would like to thank all the patients who participated for sharing their experiences. Also, we are thankful for the help of Christian Heuser, Hannah Nakata, Sherin Christmann, and Lydia Chorus.
Please contact the corresponding author for additional research materials and further information.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: CK is an employee of the German Cancer Society.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The N-MALE project was funded by the German Cancer Aid (Grant Number: 111742).