
Abstract
To investigate the correlation of prostatic calculi (PC) with semen parameters in men with fertility intention, this retrospective case–control study enrolled 1,303 participants ranging from 20 to 59 years old; 725 were diagnosed with PC using abdominal ultrasonography. Patients with PC were classified into the type A calculi group (discrete and small echoes) and type B calculi group (coarse and large masses of multiple echoes). Five hundred and seventy-eight men without PC were recruited for the control group. The clinical data of each group were collected and analyzed. The total motility was significantly lower for subjects with type B calculi (41.84% ± 17.50%) than for subjects in the type A calculi (51.78% ± 20.84%; p < .001) and control (54.47% ± 20.74%; p < .001) groups. The percentage of progressively motile was significantly lower for the type B calculi (31.66% ± 14.68%) group than the type A calculi (40.17% ± 17.09%; p < .001) and control (41.83% ± 17.05%; p < .001) groups. The results of the hypo-osmotic swelling test yielded significantly lower percentages in the type B calculi group (59.88% ± 17.13%) than the type A calculi (65.28 ± 14.43%; p = .005) and control (66.92 ± 16.12%; p < .001) groups. The type B calculi group had a significantly higher percentage of round cell concentration than control (4.5% vs. 1.0%; p = .007) did. Small and discrete PC may not influence semen quality among adult men with fertility intention, but larger and coarser PC are associated with decreased sperm motility.
First described by Donatus in 1586 (Klimas, Bennett, & Gardner, 1985), prostatic calculi (PC) are incidentally discovered during imaging examinations in men evaluated for other medical reasons. According to the echo features of PC using ultrasonography, PC are divided into type A calculi (discrete and small echoes) and type B calculi (coarse and large masses of multiple echoes; Harada, Igari, & Tanahashi, 1979). Although the precise mechanism of PC formation remains elusive, there are two main hypotheses. One hypothesis is that PC form by urinary intraprostatic reflux. The other hypothesis is that the precipitation of prostatic secretions and calcification of the corpora amylacea in the state of inflammation lead to PC formation (Sfanos, Wilson, De Marzo, & Isaacs, 2009). The prevalence of PC ranges widely from 7.35% to 88.6% according to different definitions and in different populations (Cao et al., 2018). It is reported that PC are seldom detected in children, unusual in young men, and common in middle-aged and elderly men (Klimas et al., 1985). PC are mostly regarded as a physiological result of aging in elderly men but have been correlated with inflammation in young men (Geramoutsos et al., 2004). In addition, PC are more commonly found in men with prostatitis, benign prostate hyperplasia (BPH), or prostate cancer (Gu et al., 2015; Park, Nam, Lee, & Chung, 2010).
A prospective study indicated that patients with PC had more inflammation or bacterial colonization within the prostate than those without PC (Zhao, Xuan, Zhang, He, & Zeng, 2014). Animal experiments with rats proved that a chronic inflammatory state of the male reproductive system could impair semen quality irreversibly even after sufficient antibiotic therapy (Ludwig et al., 2002). At a molecular level, men with PC were reported to have significantly higher concentrations of interleukin (IL)-8 and IL-1β than those without PC (Soric et al., 2017). Expressed by stromal and epithelial cells of the prostate, IL-8 is the most reliable marker for diagnosing prostate inflammation (Penna et al., 2007) and it plays an important role in damaging spermatogenesis (Gruschwitz, Brezinschek, & Brezinschek, 1996). In addition, a negative association between total number of progressively motile (PR) sperm and concentration of IL-1β in semen has been revealed. All these findings have underlined that PC might cause immune-mediated damage to semen quality. An animal experiment with dogs suggested that the addition of normal prostatic fluid (PF) to fresh epididymal sperm was able to activate sperm motility (Korochkina, Johannisson, Goodla, Morrell, & Axner, 2014). It was demonstrated that PF is associated with male fertility by triggering molecular pathways involved in ejaculation, sperm activation, and capacitation (Gilany, Minai-Tehrani, Savadi-Shiraz, Rezadoost, & Lakpour, 2015; Tena-Sempere, 2013). Positive pathogen culture and elevated white cell counts of expressed prostatic secretions (EPS) are more likely to arise in patients with PC (Shoskes, Lee, Murphy, Kefer, & Wood, 2007).
The presence of PC represents an indication of inflammation and/or infection within and outside the prostate. The inflammatory state and metabolic status alteration of the male reproductive system might have the potential to impair semen quality. No prior study has evaluated the clinical significance of PC in male fertility to date. To explore the clinical characteristics of men with PC as well as the correlation of PC with semen parameters, a total of 1,303 adult men with fertility intention were enrolled in this retrospective case–control study.
Materials and Methods
Patient Enrollment
Between March 2018 and August 2018, the transabdominal ultrasonography (TAUS) records of the male reproductive system of 9,657 adult men with fertility intention who visited the andrology department of the hospital were retrospectively identified. Patients with acute urinary tract infection, pyuria, bacteriuria, history of lower urinary tract irradiation or surgery, symptoms of lower urinary tract symptoms (LUTS), or history of urinary neoplasms, or those taking medications for BPH were excluded. According to the ultrasonography records, patients diagnosed with PC were enrolled in the current study. Patients in the control group were randomly selected from the patients who underwent TAUS during the same period but were not diagnosed with PC. Medical records of these participants, including sociodemographic characteristics, ultrasonography findings, and laboratory investigations, were identified and analyzed. This study design was reviewed and approved by the medical research ethics committee of the Center for Reproductive Medicine, Shandong University. The study approval number was [2019]IRB No.(33). All patients in the present study signed informed consents.
Assessment of PC
In the andrology department of the hospital, TAUS of the male reproductive system was routinely conducted in men with fertility intention. Prostate volume was evaluated using TAUS and computed as 4/3 π × the height × width × length (Roehrborn, Chinn, Fulgham, Simpkins, & Peters, 1986). According to the echo patterns of PC, patients were further divided into two groups, namely, type A calculi (discrete and multiple small echoes, often diffusely and individually distributed throughout the entire gland; Figure 1A) and type B calculi (large masses of multiple echoes, much coarser, linear pattern, occasionally associated with an ultrasonic shadow trailing behind; Figure 1B; Harada et al., 1979).
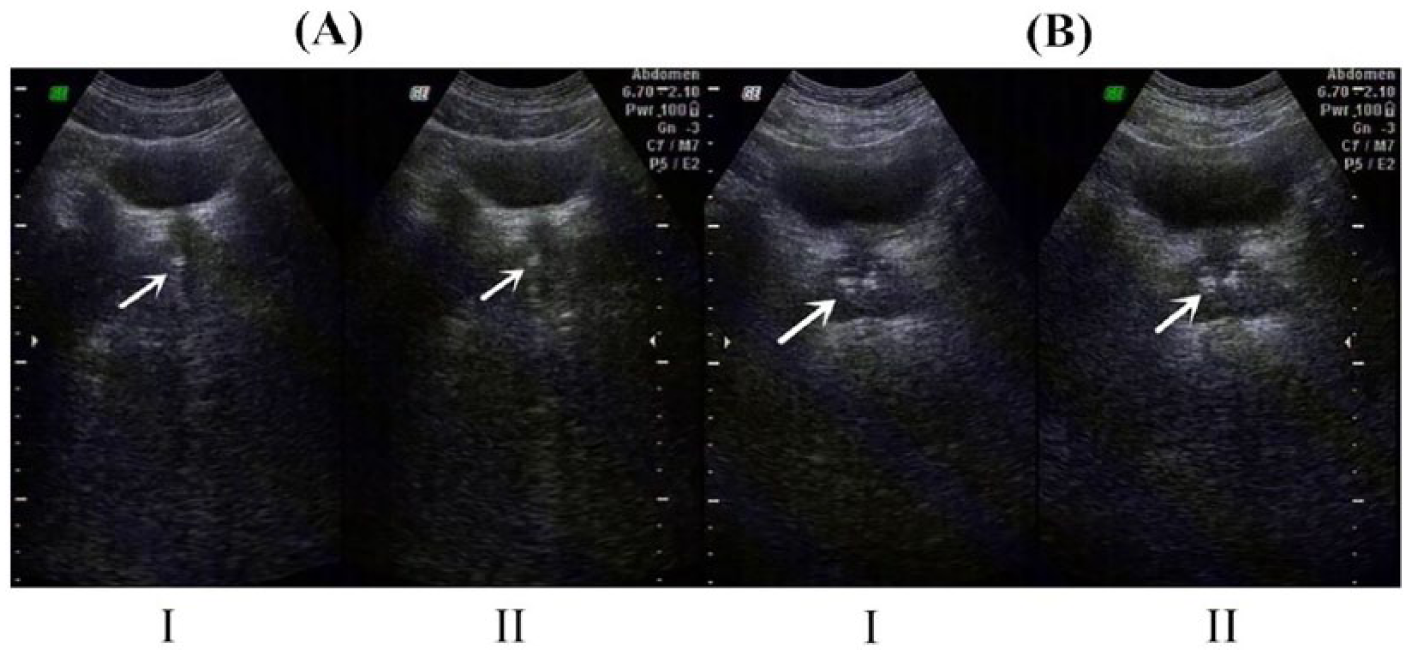
Typical echo features of the patients with PC. (A) Multiple and small PC (type A) in one participant. (B) Coarse echoes representing larger and discrete PC (type B). PC = prostatic calculi.
Semen Analysis
In the andrology department of the hospital, semen analysis was routinely performed in men with fertility intention and was conducted in the laboratory department of the hospital. Semen analysis was conducted based on the fifth edition of World Health Organization (WHO) guidelines (Cooper et al., 2010). Semen samples were obtained through masturbation after sexual abstinence within 2–7 days and were processed within 1 hr of collection. Appearance, liquefaction, semen volume, concentration, total sperm number, and the percentage of sperm motility, including total motility, PR, nonprogressively motile (NP), and immotile (IM), were evaluated. Sperm morphology and round cell concentration were also assessed, and the hypo-osmotic swelling test (HOST) was performed. If the sperm could not be found in a routine analysis of the semen, centrifuge analysis of the semen was conducted at least twice.
Hormone Profile
The measurements of follicle-stimulating hormone (FSH), luteinizing hormone (LH), prolactin (PRL), total testosterone (T), and estradiol (E2) were completed by Roche 601 (Roche Diagnostics, Germany) through electrochemiluminescence methods in the laboratory department of the hospital. Before sampling the participants were asked to maintain a sitting posture for at least 30 min. Blood samples were then collected for plasma hormone profiling in a fasting condition between 7 a.m. and 9 a.m. The hormones explored were FSH (normal level [nl]: 1.5–12.4 IU L−1), LH (nl: 1.7–8.6 IU L−1), PRL (nl: 4.04–15.2 ng ml−1), T (nl: 249–836 ng dl−1), and E2 (nl: 28–156 pmol L−1).
Statistical Analysis
For the data analyses in this study, SPSS (version 22.0, Chicago, USA) and MedCalc (version 15.2, MEDCALC Inc., Ostend, Belgium) were used. The results are expressed as the mean and standard deviation (SD) for continuous variables or N and the percentage for categorical variables. Kolmogorov–Smirnov analysis was performed for normality testing of all parameters. The groups were compared with variance analysis for continuous variables or the Pearson χ2 test for categorical variables. To determine differences between two groups, Student’s t test was applied for the analysis of average values. A two-sided confidence level p < .05 was considered statistically significant.
Results
Seven hundred and twenty-five men (7.51%) were diagnosed with PC. Specifically, type A calculi were found in 563 participants (77.66%) and type B calculi were detected in 162 patients (22.34%). In addition, 578 patients without PC were recruited in the control group. The principal characteristics of patients with PC, including age, body mass index (BMI), prostate volume, comorbidities, and sexual hormones, are listed in Table 1. In addition, 631 patients received semen analysis, whereas 94 patients did not accept semen examination due to sexual dysfunctions or other reasons. Ejaculate sperm was found in 506 patients (80.19%). Semen parameters among groups are presented in Table 2. Based on centrifuge analysis of the semen, 23 men (3.65%) were diagnosed with cryptozoospermia. The HOST results in the type B calculi group (59.88% ± 17.13%) were significantly lower than those in the type A calculi (65.28% ± 14.43%; p = .005) and control (66.92% ± 16.12%; p < .001) groups. Compared with the control group, the type B calculi group had a significantly higher percentage of round cell concentration, at over 5 million per milliliter (4.5% vs. 1.0%; p = .007). The means and 95% confidence interval (CI) of total motility, PR, NP, and IM among groups are plotted in Figure 2. The percentage of patients with asthenozoospermia in the type B calculi group (61 of 110; 55.45%) was significantly higher than those in the type A calculi (124 of 396; 31.31%; p < .001) and control (112 of 578; 19.38%; p < .001) groups. Compared with the control group, the type A calculi group had a significantly higher percentage of patients with asthenozoospermia (19.38% vs. 31.31%; p < .001). One hundred and twenty-five patients (19.81%) had azoospermia. Among the patients with azoospermia, 94 patients (75.20%) were diagnosed with type A calculi and 31 patients (24.80%) were diagnosed with type B calculi. Seventy-three patients (58.40%) received testicular sperm aspiration (TESA) or testicular sperm extraction (TESE). Forty-nine patients were diagnosed with nonobstructive azoospermia (NOA). Twenty-four subjects also had obstructive azoospermia (OA).
The Comparison of Demographic and Clinical Characteristics Among Groups.
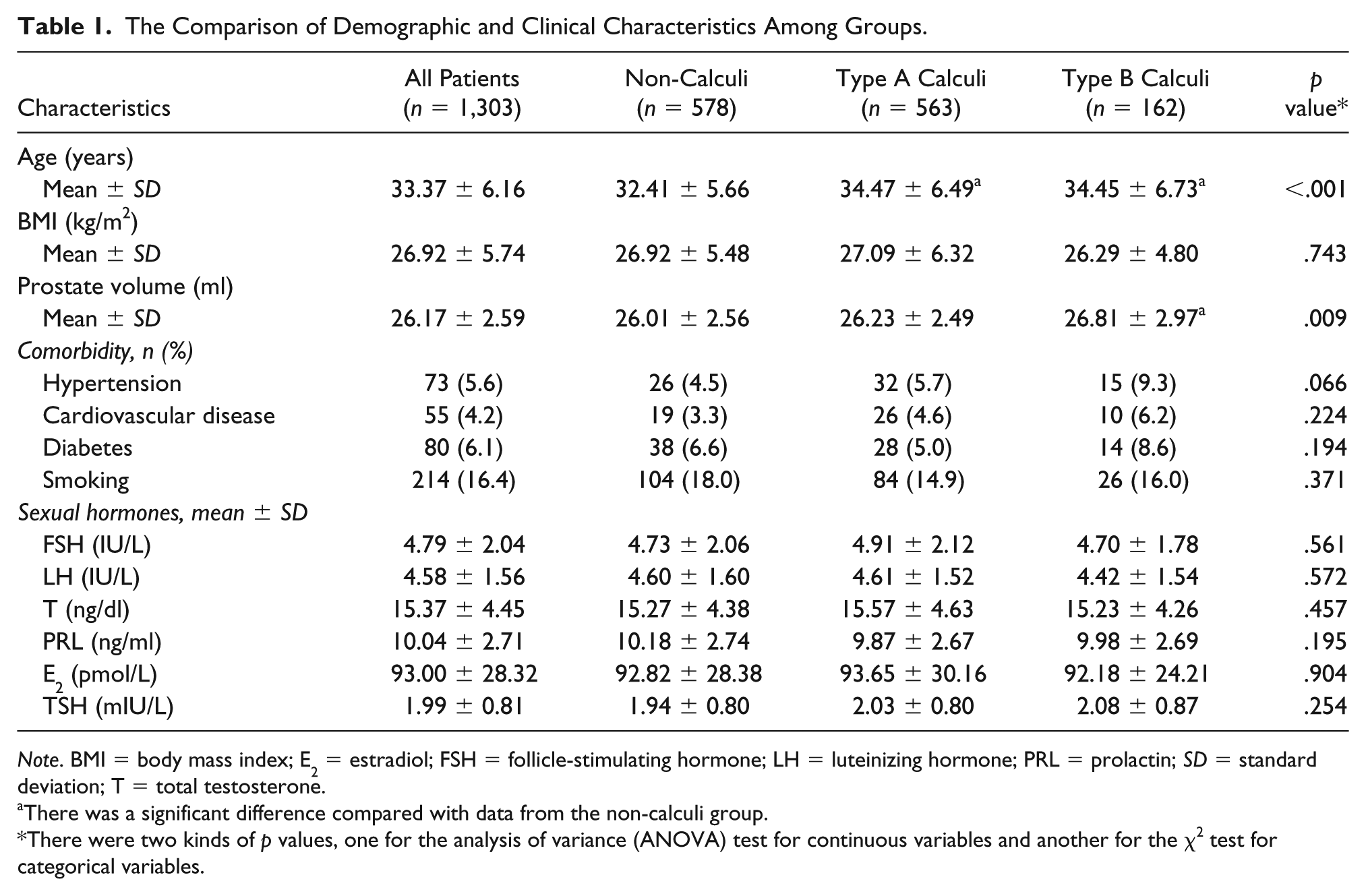
Note. BMI = body mass index; E2 = estradiol; FSH = follicle-stimulating hormone; LH = luteinizing hormone; PRL = prolactin; SD = standard deviation; T = total testosterone.
There was a significant difference compared with data from the non-calculi group.
There were two kinds of p values, one for the analysis of variance (ANOVA) test for continuous variables and another for the χ2 test for categorical variables.
The Comparison of Semen Parameters Among Groups.

Note. Values are means ± SD. HOST = hypo-osmotic swelling test; IM = immotile; NP, nonprogressively motile; PR = progressively motile; VAP = average path velocity; VCL = curvilinear velocity; VSL = straight-line velocity.
There was a significant difference compared with data from the non-calculi group. bThere was a significant difference compared with data from the type A calculi group.
There were two kinds of p values, one for the analysis of variance (ANOVA) test for continuous variables and another for the χ2 test for categorical variables.

Error bar charts of total motility, PR, NP, and IM among groups. (A) The means and 95% CI of total motility among groups; (B) the means and 95% CI of PR among groups; (C) the means and 95% CI of NP among groups; and (D) the means and 95% CI of IM among groups. CI = confidence intervals; Cont = control; IM = immotile; NP = nonprogressively motile; PR = progressively motile.
Discussion
In the current study, the mean age of all participants was 33.37, ranging from 20 to 59 years, and 82.69% were below 40 years of age. Most of the participants in this study were of a young age, and 7.51% of the subjects were diagnosed with PC using TAUS. Geramoutsos et al. (2004) reported that 7.35% of 1,374 young men under 50 years were diagnosed with PC using TAUS. A retrospective study including 68,705 participants reported that the incidence of PC increases as age increases. Nine percent of men aged 18–29 years were diagnosed with PC using TAUS (Tang, Wu, Wei, & Wu, 2018). The prevalence of PC in the population of the present study was comparable to that in previous studies (Geramoutsos et al., 2004; Tang et al., 2018). Type A calculi represent a consequence of physiological aging and both types of PC form in proportion to age (Lee, Akin-Olugbade, & Kirschenbaum, 2011). Multiple studies (Park et al., 2010; Yang, Huang, Wang, Chang, & Yang, 2013) concluded that age is an independent predisposing factor for PC. The current study demonstrated that the mean age of patients with PC was significantly higher than that of men in the control group, regardless of the type of PC.
Another modified predisposing factor for PC is prostatic volume (Park et al., 2010). Transrectal ultrasonography (TRUS) has been proposed to be superior to TAUS regarding volume measurement (Loch et al., 2007). However, due to the invasiveness and discomfort, an elevated level of resistance is correlated with TRUS (Park et al., 2000). Unlike TRUS, TAUS is more convenient and widely accepted by patients as well as urologists. Huang and associates (Huang Foen Chung et al., 2004) concluded that no significant difference in the measurement of prostatic volume had been identified between TAUS and TRUS. TAUS, instead of TRUS, was selected to examine the prostate in the current study. As is generally known, a minor statistically significant difference should be detected when the sample size is more than 100, or even less. The statistically significant difference obtained from the comparison between prostate volume in the non-calculi group and that in the type B calculi group was mainly caused by the large sample size. Therefore, it could hardly have clinical significance, especially considering the margin of error when measuring prostate volume by ultrasound.
Although considerable attention has been paid to the clinical significance of PC recently, the understanding of PC in male fertility has not yet progressed. In the present study, lower PR was found in the type B calculi group than in the type A calculi and control groups. Patients with type B calculi had significantly lower total sperm motility than men in the type A calculi and control groups. The current study collectively demonstrated that type B calculi had a significantly detrimental effect on sperm motility. Multiple reasons account for this finding. Formed by chemical, bacterial, or immunologic stimulation, type B calculi are primarily located in the prostatic ducts. Increased intraprostatic pressures in turn give rise to loss of epithelium, atrophy, or fibrosis of certain areas within the prostate (Torres Ramirez, Aguilar Ruiz, Zuluaga Gomez, del Rio Samper, & Issa Khozouz, 1979). Patients with PC possessed significantly higher concentrations of IL-1β and IL-8 in seminal plasma than patients without PC (Soric et al., 2017). In addition, IL-1β was associated with the number of PR sperm (Gruschwitz et al., 1996). Cytokines, including IL-8, were able to damage structural and metabolic components of the sperm motility apparatus (Penna et al., 2007).
Apart from immune-mediated effects, PC were also associated with bacterial colonization (Shoskes et al., 2007). Bacterial imprints were detected in PC, suggestive of chronic infection characterized by lymphocytes and histiocytes (Torres Ramirez et al., 1979). Bacterial infection within the male reproductive system had the potential to impair the secretory ability of the prostatic epithelium, which may in turn cause decreased semen quality (Domes et al., 2012). Even after eliminating pathogens by antibiotics, semen parameters were not able to return to normal in half of the patients (Ludwig et al., 2002). One possible reason was that asymptomatic and chronic inflammation may lead to germ cell loss or duct obstruction, which could continuously influence both sides of the testes and impair fertility (Lu et al., 2013). Patients with PC were more vulnerable to positive results of pathogen culture and elevated white cell counts in EPS (Shoskes et al., 2007). Sperm motility requires the coordination of factors within the seminal plasma. The first fractions of the semen expelled during ejaculation are dominated by sperm-rich PF. Multiple components of PF had the capacity to control ejaculation and regulate proteins for the activation of sperm maturation (Gilany et al., 2015). An animal experiment with dogs suggested that the addition of normal PF to fresh epididymal sperm could activate sperm motility (Korochkina et al., 2014). Patients involved in this study were consulting for fertility intention rather than prostatitis-related problems; the collection of EPS was therefore not easily accepted by the patients due to the invasiveness and uncomfortable feelings. As a supplement, round cells in the ejaculate are mainly composed of leukocytes together with immature germ cells, and the total number of round cells may reflect the severity of the inflammation or spermatogenesis (Cooper et al., 2010). In this study, the type B calculi group had a significantly higher round cells concentration, over 5 million per milliliter, than the type A calculi and control groups. The current study provided crucial evidence that the inflammatory or spermatogenic condition of the semen in the type B calculi group was more severe than in the type A calculi and control groups. This finding underlined that the correlation of type B calculi with decreased sperm motility might be attributable to the inflammatory state within the reproductive system.
Biochemical damage of the sperm membrane, even when structurally intact, may cause failure of sperm–oocyte fertilization. Based on the evaluation of sperm membrane integrity, HOST is widely used as a valuable detection of semen quality and sperm fertilizing capacity. In the present study, the mean percentage of sperm swelling in the type B calculi group was significantly decreased compared with that in the type A calculi and control groups. It revealed that larger and coarser calculi might damage the membrane integrity of the sperm. Further studies are needed to explore the mechanism concerned in this finding.
There were several limitations in the current study. A relatively small sample size at a single institution with a retrospective study design constituted the primary limitation of this study. Additionally, the relationship between type B calculi and decreased sperm motility might be due to immune mediators that were not measured. Furthermore, the criteria for classifying PC have yet to be well established. We are looking forward to larger studies, especially randomized controlled trials, to further evaluate the association of PC with semen parameters and to better characterize the types of PC. Despite these limitations, this was the first case–control study to assess PC in male fertility, and it provided novel insights in a previously uncharted field.
Conclusions
The current study demonstrated that larger and coarser PC are associated with decreased sperm motility in adult men with fertility intention. However, small and discrete PC may have no effect on semen quality.
Footnotes
Acknowledgements
We would like to express the depth of our gratitude to Demin Fan from the Department of Urology, Shandong Provincial Qianfoshan Hospital, for the proofreading of our manuscript.
Tong Chen and Linlin Tian contributed equally to this study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was supported by the grant from Shandong Province Key Research and Development Program (No.2017GSF218070).