
Abstract
Studies evaluating the effects of narghile use on the periodontium present conflicting conclusions. This study aimed to compare the periodontal status of exclusive narghile smokers (ENSs, n = 74) to that of exclusive cigarette smokers (ECSs, n = 74). Males aged 20–40 years were recruited to participate in this comparative study. Information concerning oral health habits (number of yearly visits to the dentist, daily toothbrushing frequency) and tobacco exposure were obtained. Clinical measurements were performed on all the existing teeth, except the third molars. The number of remaining teeth and decayed/missing/filled teeth (DMFT) were noted. The plaque levels were recorded using the plaque index of Löe and Silness. The gingival index modified by Löe was used to evaluate gingival inflammation. Teeth mobility was measured using bidigital mobility. The probing pocket depth was measured using a periodontal probe. Periodontal disease was defined as the presence of at least 10 sites with a probing depth ≥5 mm. Student’s t and chi-square tests were used to compare, respectively, the two groups’ quantitative and qualitative data. The two groups were matched for quantities of used tobacco, age, daily toothbrushing frequency, teeth mobility, number of remaining teeth, plaque index, and DMFT. Compared to the ECS group, the ENS group had a significantly lower number of yearly visits to the dentist (mean ± SD: 0.2 ± 0.5 vs. 0.1 ± 0.2), lower probing pocket depth (mean ± SD: 2.33 ± 0.63 vs. 2.02 ± 0.80 mm), and gingival index (median [interquartile]: 0.46 [0.10–0.89] vs. 0.00 [0.00–0.50]), and it included significantly lower percentages of smokers with periodontal disease (24.3% vs. 9.5%). In conclusion, chronic exclusive narghile smoking has fewer adverse effects on the periodontium than chronic exclusive cigarette smoking.
Narghile is one of the ways of tobacco smoking, which has increased worldwide over the past 2 decades (Ramôa, Eissenberg, & Sahingur, 2017; World Health Organization [WHO], 2005, 2015). A systematic review (Akl et al., 2011), aimed at evaluating the prevalence of narghile use among general and specific populations, reported its high prevalence among adults as well as school and university students. In North Africa, 3.5% of the general population were reported to use narghile with a male predominance (82.0%; Alzaabi et al., 2017). This smoking habit poses great health threats and, with its increasing use, these threats are becoming more and more significant. It is therefore very important to investigate its effects on health in order to better inform the public.
Narghile use is frequently associated with several diseases. Hence, numerous studies were published concerning the general effects of narghile use on health (Awan, Siddiqi, Patil, & Hussain, 2017; Ben Saad, 2010; Bou Fakhreddine, Kanj, & Kanj, 2014; Chaouachi, 2015; El-Zaatari, Chami, & Zaatari, 2015; Waziry, Jawad, Ballout, Al Akel, & Akl, 2017; WHO, 2005, 2015). As inhalation of the toxic substances included in narghile smoke may affect the integrity of the oral cavity (Amer, Waguih, & El-Rouby, 2019) and as dentists may have narghile smokers as their patients, it is essential to inform them of the significantly damaging impacts of its use on some components of the oral cavity, such as the periodontium. The adverse impacts of cigarette smoking on the periodontium are well documented (César Neto, Rosa, Pannuti, & Romito, 2012; Laxman & Annaji, 2008). Some authors demonstrated that exclusive cigarette smokers (ECSs) had more severe periodontal disease (PD) with increased bone loss, greater periodontal attachment loss, and more gingival recession and periodontal pocket formation (Bergström, Eliasson, & Dock, 2000; Calsina, Ramón, & Echeverría, 2002). For young ECSs, the odds ratio (OR) for PD was as high as 14.1 (Linden & Mullally, 1994). However, to the best of the authors’ knowledge, specific reviews evaluating the effects of narghile use on oral health are scarce (Awan et al., 2017; Khemiss, Rouatbi, Berrezouga, & Ben Saad, 2015, 2016; Ramôa et al., 2017; Warnakulasuriya, 2011). A 2017 systematic review and meta-analysis of the health outcomes of narghile use reported that the latter is not associated with PD (Waziry et al., 2017). At the time, the aforementioned systematic review included only five studies (Al-Belasy, 2004; Baljoon, Natto, Abanmy, & Bergström, 2005; Natto, Baljoon, Abanmy, & Bergström, 2004; Natto, Baljoon, & Bergström, 2005a, 2005b; Natto, Baljoon, Dahlén, & Bergström, 2005) with only two related to PD (Natto et al., 2004, 2005b). By the end of 2018, almost 10 studies had evaluated the effects of narghile use on the periodontium, and their results were controversial (Al-Alimi et al., 2018; Al-Mufti & Saliem, 2018; Bibars, Obeidat, Khader, Mahasneh, & Khabour, 2015; Javed et al., 2016; Khemiss, Ben Khelifa, Ben Rejeb, & Ben Saad, 2016; Khemiss, Ben Khelifa, & Ben Saad, 2017; Malik, Khan, Rahman, & Malik, 2012; Mokeem et al., 2018; Natto et al., 2004, 2005b). According to Malik et al. (2012), the worst nightmare for narghile smokers is PD. The authors reported an increase in gingival index (GI), calculus formation, and probing pocket depth (PPD; Malik et al., 2012). While some studies revealed that exclusive narghile smokers (ENSs) and healthy nonsmokers (HNSs) were matched for plaque index (PI; Bibars et al., 2015; Khemiss et al., 2017), GI (Bibars et al., 2015), and decayed/missing/filled teeth (DMFT; Khemiss et al., 2017), others reported that compared to HNSs, ENSs had compromised oral health in terms of PI (Javed et al., 2016; Mokeem et al., 2018; Natto et al., 2004, 2005b), GI (Natto et al., 2004, 2005b), PPD (Bibars et al., 2015; Javed et al., 2016; Mokeem et al., 2018; Natto et al., 2005b), and PD (Bibars et al., 2015; Natto et al., 2005b). Compared to cigarette smoking, narghile use was identified to induce similar effects in terms of GI (Natto et al., 2004, 2005b), PI (Javed et al., 2016; Natto et al., 2005b), PPD (Javed et al., 2016; Natto et al., 2005b), and PD (Bibars et al., 2015; Natto et al., 2005b), and it was identified to be more harmful in terms of PI (Khemiss, Ben Khelifa, et al., 2016; Natto et al., 2004). A case control study including 100 males (50 free of PD [25 HNSs and 25 ENSs] and 50 having PD [25 nonsmokers and 25 ENSs]) concluded that the groups free of PD had similar PI but different GI (higher in the HNS group; Al-Mufti & Saliem, 2018). The authors also stated that in the groups with PD, PI and GI were higher in nonsmokers (Al-Mufti & Saliem, 2018). Finally, in a Yemeni population of adults aged 30–60 years (150 periodontitis cases and 150 healthy controls), narghile use was identified as a risk factor for periodontitis (OR between PI score and narghile use was 10.2; Al-Alimi et al., 2018). The divergence in conclusions can be related to some methodological limitations/differences, to diverse study designs (Berry, 1974; Mann, 2003), and to some characteristics of the included smokers (e.g., socioeconomic and/or schooling levels [Shafagoj, Mohammed, & Hadidi, 2002], geographical regions with a wide use of miswak [an antimicrobial agent used to prevent and to treat PDs; al-Otaibi, 2004] in Saudi Arabia), which may affect the outcomes. Four examples can be highlighted. First, the lack of sample size calculation in some studies (Bibars et al., 2015; Malik et al., 2012; Natto et al., 2004, 2005b) is a statistically central argument since determining its optimum size for a study guarantees enough power to differentiate statistical significance. The sample size calculation is a serious step in the design of a planned research procedure (Kang, Ragan, & Park, 2008). Second, the inclusion of the elderly aged more than 60 years (Natto et al., 2004, 2005b) may introduce a bias because the prevalence of PD increases with age (R. E. Persson, Rollender, Laurell, & Persson, 1998). Third, the lack of information concerning the different types of narghile tobacco used (Javed et al., 2016; Malik et al., 2012; Mokeem et al., 2018; Natto et al., 2004, 2005b) makes comparison difficult. In fact, in the case of tombak or jurak, in comparison to tabamel, the pattern is different (Ben Saad, 2009). Fourth, different methods of narghile use quantification (not reported [Natto et al., 2004], run-years [Natto et al., 2005b], units/day [Malik et al., 2012], narghile/week [Bibars et al., 2015], narghile daily frequency and session duration [Javed et al., 2016; Mokeem et al., 2018], and narghile-years [NY; Khemiss, Ben Khelifa, et al., 2016; Khemiss et al., 2017] were applied. The means of narghile tobacco exposure, mentioned in some studies (Bibars et al., 2015; Javed et al., 2016; Khemiss, Ben Khelifa, et al., 2016; Khemiss et al., 2017; Malik et al., 2012; Natto et al., 2005b), were very extended (from 3.4 narghiles/week [Bibars et al., 2015] to 36 run-years [Natto et al., 2005b]). This situation makes comparison between studies problematic. Five biological mechanisms were advanced to explain the effects of narghile use on the smokers’ periodontal health: inhalation of toxic substances (e.g., nicotine); increase of matrix metalloproteinases’ expression; overstimulation of the host response; release of collagenase, elastase, and other enzymes from inflammatory cells; and alteration of the buffering capacity (Boström, Linder, & Bergström, 1999, 2000; Cryer, Haymond, Santiago, & Shah, 1976; Kalra, Chaudhary, & Prasad, 1991; Khemiss et al., 2017; McGuire & Nunn, 1999; Natto et al., 2004, 2005b; Palmer et al., 1999; Pauletto, Liede, Nieminen, Larjava, & Uitto, 2000; L. Persson, Bergström, Gustafsson, & Asman, 1999; Ryder, 1994; Ryder et al., 1998). However, since the toxic substances and the chemical profile of narghile smoke are completely different from those of cigarettes (e.g., the mean blood nicotine level in ENSs sitting for a narghile session [~45 min] was lower than that identified in ENSs having smoked 1 cigarette [~5 min] or corresponding to that of 1.7 cigarette when applying a pharmacokinetics model; Ben Saad, 2009; Chaouachi, 2009, 2015; Eissenberg & Shihadeh, 2009; Primack et al., 2016), these two methods of tobacco smoking are hypothesized to induce different health effects in ENSs and ECSs. For instance, one Tunisian study concluded that narghile smoking has less adverse effects on pulmonary function tests than cigarette smoking (Ben Saad, Khemiss, Nhari, Ben Essghaier, & Rouatbi, 2013).
Research on narghile use still has a lot of limitations that need to be further studied. According to WHO (2005, 2015) consultative notes on narghile use, research with regard to narghile-associated disease risk is required. Taking into account the aforementioned methodological limitations/differences, the WHO recommendations, and the different chemical profiles of narghile and cigarette smoke, this study aimed at comparing some clinical data related to the periodontal status in ENSs with those in ECSs involving young adults. The null hypothesis was that there is no difference between the mean values of their periodontal data (e.g., number of remaining teeth, DMFT, PI, GI, PPD).
Population and Methods
Study Design
This was a comparative cross-sectional study, carried out over 2 years (from October 2016 to February 2018) in the Department of Oral Medicine at Fattouma BOURGUIBA University Hospital (Tunisia). The present study is the third part of a project aimed at the evaluation of narghile use effects on oral health. The first study aimed at comparing the periodontal bone height in 60 ENSs with that in 60 ECSs (Khemiss, Ben Khelifa, et al., 2016). The second one aimed to compare some salivary characteristics of 36 ENSs and 36 HNSs (Khemiss et al., 2017).
Permission from the ethical committee of Farhat HACHED University Hospital of Sousse (approval number: 17052013) was obtained. The study was conducted in accordance with the Declaration of Helsinki. Smokers were individually informed about the purpose of the study. They all signed an informed written consent prior to their participation. The smokers diagnosed with any oral pathology were given treatment or were referred to the right specialist.
Population
The smokers were recruited via flyers distributed in cafés in the city of Monastir. Only males aged 20 to 40 years and who were ENSs or ECSs were included, respectively, in the narghile or the cigarette groups. The following noninclusion criteria were applied: (a) tobacco use <5 NY for the ENS group; (b) jurak and/or tombak tobacco use; (c) known systemic medical conditions (e.g., diabetes mellitus); (d) previous head or neck radiation therapy; (e) number of remaining teeth <20; (f) tobacco use <5 pack-years (PY) for the ECSs group; and (g) consumption of drugs (antidepressants, anticonvulsants, cyclosporin A, calcium, and antagonists) known to have an effect on the periodontium.
Sample Size
The sample size was estimated using a predictive formula (Kang et al., 2008), detailed in the Appendix. The sample size for the study was 148 smokers (74 ENSs and 74 ECSs).
Process of Data Collection and Applied Definitions
The participants were interviewed using a nonstandardized questionnaire written in Arabic. Closed-ended questions were provided and they were often dichotomous. The socioeconomic level was defined according to the professional status. The schooling level was determined according to the highest level achieved by the participant in the Tunisian school system. Two socioeconomic and schooling levels (low/high; detailed in the Appendix) were arbitrarily defined. The levels of narghile use and cigarette consumption were quantified, respectively, in NY (1 NY is equal to 1 narghile per day for 1 year; Ben Saad, 2009) and in PY (1 PY is equal to 20 cigarettes per day for 1 year). The oral hygiene habits were evaluated through the number of yearly visits to the dentist and the daily toothbrushing frequency. Applying a “one daily toothbrushing frequency” as a cutoff, the smokers were classified arbitrarily into two groups: irregular (=0) and regular (≥1).
The equipment used in the basic dental examination consisted of a mouth mirror, cotton pliers, and an explorer–periodontal probe (number 6, 17, or 23). Water and air syringes were used to remove debris and fluids. The clinical examination was carried out to identify oral health indicators using a good light source in order to have an adequate view while performing any oral diagnostic procedures. The caries status was scored using DMFT index (D: tooth decayed; M: tooth missing; F: tooth or surface filled) in all the teeth except the third molars (Klein & Palmer, 1940). DMFT index measures the prevalence of dental caries and provides information on past and present diseases (Gaengler, Goebel, Kurbad, & Kosa, 1988). Some principles and rules in recoding DMFT, detailed in the Appendix, were applied. For each smoker, DMFT was calculated as follows: DMFT = D + M + F (Klein & Palmer, 1940).
The PI was evaluated according to the Silness and Löe (1964) system. This system assesses the plaque thickness at the tooth cervical margin (closest to the gum) and has four scores:
0: no plaque;
1: a film of plaque adhering to the free gingival margin which is nonvisible and it can be scraped from the tooth surface using a probe;
2: moderate accumulation of soft deposits within the gingival pocket or between the tooth and the gingival margin;
3: abundance of soft matter within the gingival pocket and/or on the tooth and the gingival margin.
A plaque indicator was used in order to demonstrate the bacterial plaque on teeth and to assist in PI evaluation. The presence of visible dental plaque was recorded on the four sites (vestibular, lingual, mesial, and distal) of all the teeth, except the third molars. As previously performed by some authors (Bibars et al., 2015; Khemiss, Ben Khelifa, et al., 2016; Khemiss et al., 2017), three PI classes (PI%; [0–1[; [1–2[; [2–3]) were arbitrarily defined.
The gingival status was evaluated using the method of Löe and Silness (1963), later modified by Löe (1967). The GI score perfectly evaluates the marginal and interproximal tissues separately on the basis of the following three criteria (Löe & Silness, 1963):
0: no inflammation, healthy gingiva;
1: mild inflammation, slight change in color, slight edema, no bleeding on pressure;
2: moderate inflammation, moderate glazing, redness, bleeding on pressure;
3: severe inflammation, marked redness and hypertrophy, ulceration, tendency to spontaneous bleeding.
The modified GI (score 2 was changed from bleeding on pressure to bleeding on probing) was used to evaluate gingival inflammation (Löe, 1967). The mesial, buccal, distal, and lingual sites of all the teeth, except the third molars, were scored. The arithmetic mean of the scores’ sum formed the smoker’s GI.
Tooth mobility, representing a combination of the periodontal bone height and the width of the periodontal ligament (Thomas & Kenneth, 2003), was measured using the bidigital tooth mobility. This measurement was performed by alternatively pressing on the tooth buccal and lingual surfaces using the nonworking ends of the two instruments’ handles (Thomas & Kenneth, 2003). Tooth mobility was recorded (Fleszar et al., 1980) as follows:
0: physiologic mobility, firm tooth;
1: slightly increased mobility;
2: definite to considerable increase in mobility but no function impairment;
3: extreme mobility, a loose tooth that is uncomfortable in function.
PPD is the distance between the gingival margin and the apical depth of the periodontal probe tip penetration (Proye, Caton, & Polson, 1982). The depth of the sulci or pockets was probed using a CP12 periodontal probe with markings 3, 6, 9, and 12 mm (0702L-12, ASA DENTAL, Italy). This is an accurate, well-defined, permanent, and easy-marking probe. The probe is thin (diameter = 0.5 mm), made of metal, and divided into three parts: handle, shank, and working end. Each smoker was represented by the arithmetic mean of all the probing depth values. The clinical measurements were based on the four sites (buccal, mesial, distal, and lingual) of all the teeth, except the third molars (Natto et al., 2005b). PD, an inflammatory disease characterized by the loss of the tooth-supporting tissues (Thomas & Kenneth, 2003), was defined by the presence of at least 10 sites with a probing depth ≥5 mm (Natto et al., 2005b).
Statistical Analysis
The Kolmogorov–Smirnov test was used to analyze the distribution of variables. When the distribution was normal and the variances were equal, the results were expressed by their mean ± standard deviation (SD) and by 95% confidence interval (95% CI). If the distribution was not normal, the results were expressed by their medians (interquartile). Student’s t test and chi-square test were used to compare, respectively, the two groups’ quantitative and qualitative data. Student’s t test was also used to compare the periodontal status data of the smokers divided according to their schooling and socioeconomic levels (low vs. high) and their brushing habits (regular vs. irregular). Spearman’s correlation coefficient (R) evaluated the associations between the periodontal status data (PI, GI, DMFT, number of remaining teeth, PPD) on the one hand and the smokers’ characteristics and oral health habits (age, level of tobacco exposure, daily toothbrushing frequency, number of yearly visits to the dentist) on the other hand. R was considered high when it was >0.70, good when it was between 0.50 and 0.70, fair between 0.30 and 0.50, and weak or no association if it was <0.30 (Hinkle, Wiersma, & Jurs, 2003). All mathematical computations and statistical procedures were performed using Statistica software (Statistica Kernel version 6; Stat Software, France). Significance was set at .05 level.
Results
Among the 157 smokers examined, only 148 were retained (74 ENSs and 74 ECSs). Nine smokers were excluded mainly because they were diagnosed with a systemic disease. Table 1 displays the characteristics and oral health habits of the smokers. The two groups were matched for age, quantities of tobacco used, and daily toothbrushing frequency. Compared to ECSs, ENSs included significantly lower percentages of smokers having high schooling or socioeconomic levels. Compared to ECSs, ENSs had a significantly lower mean of yearly visits to the dentist.
Characteristics, Oral Health Habits, and Clinical Data of the Smokers: Exclusive Narghile Smokers (ENSs) and Exclusive Cigarette Smokers (ECSs).

Note. NY = narghile-years; p = probability; PY = pack-years.
Data were amean ± SD (95% confidence interval); bmedian (interquartile); cnumber (%).
p < .05 (t test): ENSs versus ECSs. †p < .05 (chi-square): ENSs versus ECSs.
Table 1 displays also the periodontal status data of the smokers. The two groups were matched for PI, DMFT, and number of remaining teeth. Compared to ECSs, ENSs included a significantly lower percentage of smokers having PD. Compared to ECSs, ENSs had significantly lower means of PPD and GI. All the smokers had a physiological tooth mobility (mean ± SD = 0.00 ± 0.00) and the two groups were matched for PI% (Figure 1).
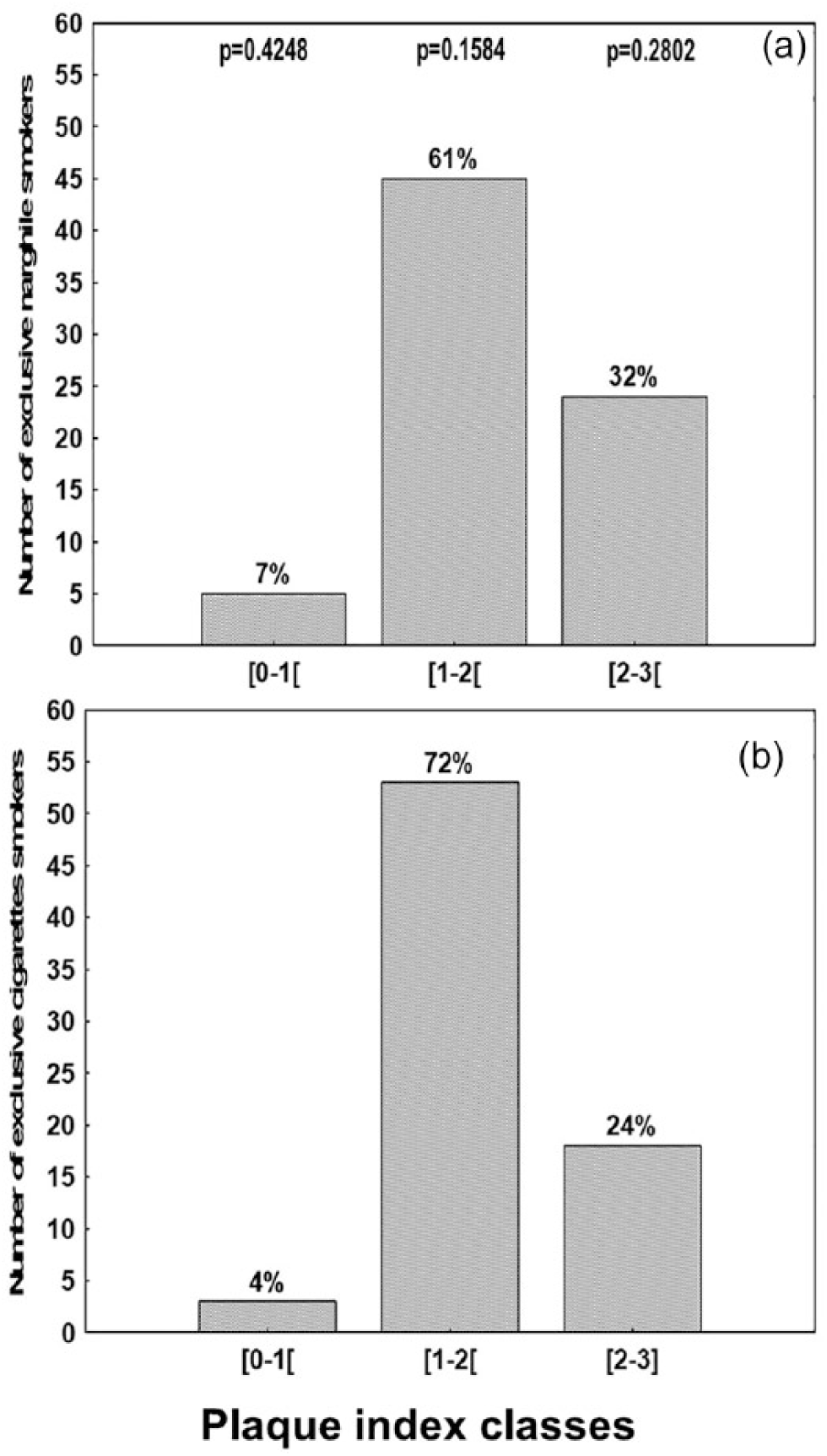
Repartition of the smokers according to the three plaque index classes and tobacco habits. (a) Exclusive narghile smokers (ENSs, n = 74). (b) Exclusive cigarette smokers (ECSs, n = 74). Data were percentages. Probability (p, chi-square): exclusive narghile smokers (ENSs) versus exclusive cigarette smokers (ECSs).
Table 2 presents the R between the periodontal status data and the smokers’ characteristics and their oral health habits. For ENSs, DMFT and PPD were correlated with age and DMFT, and number of remaining teeth was correlated with the daily toothbrushing frequency. For ECSs, DMFT, PPD, and number of remaining teeth were correlated with both age and the level of cigarette exposure, and DMFT was correlated with the daily toothbrushing frequency. All the above correlations were qualified as “weak” or “fair.”
Spearman’s Correlation Coefficient (R) Between the Periodontal Status Data and the Smokers’ Characteristics and Oral Health Habits: Exclusive Narghile Smokers (ENSs, n = 74) and Exclusive Cigarette Smokers (ECSs, n = 74).

Note. GI = gingival index; DMFT = decayed/missing/filled teeth; NY = narghile-years; p = probability; PI = plaque index; PPD = probing pocket depth; PY = pack-years; RT = remaining teeth.
Data were R (probability).
Correlations were as follows: ahigh: R > 0.70; bgood: R: 0.50–0.70; cfair: R 0.30–0.50; dweak or no association: R < 0.30.
Table 3 presents the periodontal status data of the smokers divided according to their schooling and socioeconomic levels as well as their brushing habits. The schooling level influenced the GI of ENSs, the DMFT of ECSs, and the number of remaining teeth of both groups. In smokers having a low schooling level, compared to ECSs, ENSs had a significantly lower DMFT. For the smokers having a high schooling level, compared to ECSs, ENSs had significantly lower GI and PPD. The socioeconomic level influenced the PI of ECSs and the GI of ENSs. For the smokers having a high socioeconomic level, compared to ECSs, ENSs had significantly lower GI, DMFT, PPD, and number of remaining teeth. Brushing habits had an influence on the DMFT of both groups and on the number of remaining teeth of only ENSs. For irregular brushers, compared to ECSs, ENSs had a significantly lower GI. Yet, for regular brushers, compared to ECSs, ENSs had significantly lower GI and PPD, but significantly higher number of remaining teeth.
The Periodontal Status Data of Exclusive Narghile Smokers (ENSs, n = 74) and Exclusive Cigarette Smokers (ECSs, n = 74) Divided According to Their Schooling and Socioeconomic Levels and Their Brushing Habits.

Note. GI = gingival index; DMFT = decayed/missing/filled teeth; NY = narghile-years; p = probability; PI = plaque index; PPD = probing pocket depth; PY = pack-years; RT = remaining teeth.
p < .05 (t test): low versus high or irregular versus regular for the same group of smokers. #p < .05 (t test): ENSs versus ECSs for the same level or habits.
Discussion
Two groups of smokers (74 ENSs and 74 ECSs) of the same age and consuming the same quantity of tobacco were compared. ENSs had significantly lower PPD and GI. They also included significantly lower percentages of smokers with PD. The two groups were matched for teeth mobility, PI, DMFT, and number of remaining teeth; they included similar percentages of smokers divided by PI%. Both narghile use and cigarette smoking alter the periodontal health. However, cigarette smoking had a more detrimental effect on the periodontium.
As dentists often encounter narghile smokers among their patients, they need to inform such patients of the significantly detrimental impacts of narghile use on their periodontal health and how it can lead to dental problems (Khemiss, Rouatbi, et al., 2016; Khemiss et al., 2015). However, studies analyzing the periodontal clinical data of ENSs are scarce. To the best of the authors’ knowledge, only 10 studies were published (Al-Alimi et al., 2018; Al-Mufti & Saliem, 2018; Bibars et al., 2015; Javed et al., 2016; Khemiss, Ben Khelifa, et al., 2016; Khemiss et al., 2017; Malik et al., 2012; Mokeem et al., 2018; Natto et al., 2004, 2005b). The study designs and the characteristics of the involved subjects in the eight comparative studies are displayed in the Appendix (Table 1S). The aforementioned studies had some methodological limitations and yielded contradictory results, as seen in the Appendix (Tables 2S and 3S).
Narghile is a way of tobacco smoking. Charcoal heats tobacco, producing smoke that passes through water before inhalation (Sameer-ur-Rehman et al., 2012). Humans began using narghile at least 7 centuries ago (van der Merwe, 1975). Its emergence in the Middle East dates back to the end of the 16th century and the beginning of the 17th century (Chaouachi, 2006a). This popularity coincided with the appearance of public coffeehouses and the adoption of tobacco in the Eastern societies (Chaouachi, 2006a). A modern narghile (Photo 1S, Appendix) is made up of six parts (head, body, bowl, hose, vase, mouthpiece). Depending on the region and the country, different synonyms were used to refer to narghile (Aslam, Saleem, German, & Qureshi, 2014). At least 35 names of narghile were used in the literature (Box 1S, Appendix; Bou Fakhreddine et al., 2014). At least 19 different names of tobacco used in narghiles were highlighted (Box 1S, Appendix; Bou Fakhreddine et al., 2014). There are three main smoking mixtures: mu‛assel (tabamel in Latin-based languages), tombak, and jurak. More information concerning narghile synonyms and components and the names of tobacco are detailed in the Appendix.
Compared to ECSs, ENSs had significantly lower PPD and GI. They also included significantly lower percentages of smokers with PD. However, the two groups had similar values of tooth mobility, number of remaining teeth, PI, and DMFT. They also included similar percentages of smokers divided by PI%.
The two groups of ENSs and ECSs were matched for PI and PI% (Table 1, Figure 1). The effects of narghile use on the aforementioned data are controversial (Table 3S). Consistent with this study findings, other studies reported no statistical differences between PI values of ENSs and those of ECSs (Natto et al., 2005b), mixed smokers (MSs; Natto et al., 2005b), and HNSs (Khemiss et al., 2017). However, in some other studies, PI mean values were significantly higher in ENSs compared to ECSs (Khemiss, Ben Khelifa, et al., 2016; Natto et al., 2004), MSs (Natto et al., 2004), or HNSs (Natto et al., 2004, 2005b). Comparable to the results of this study, other studies reported no statistical differences between the percentages of subjects having PI% in ENSs and ECSs (Bibars et al., 2015; Javed et al., 2016), MSs (Bibars et al., 2015), and HNSs (Bibars et al., 2015). The PI% seems to be higher in ENSs compared to HNSs (Javed et al., 2016; Mokeem et al., 2018). However, one study revealed no statistical differences between ENSs and ECSs, MSs, and HNSs concerning the frequency of surfaces having a plaque score equal to 1 or more (plaque %; Natto et al., 2004). Finally, it seems that 14% of ENSs had calculus (Malik et al., 2012).
The two groups had similar values with regard to the number of remaining teeth and DMFT (Table 1). The effects of narghile use on the smokers’ remaining/missing teeth are also controversial (Table 3S). Consistent with the results of this study, other studies reported no statistical differences between the number of remaining teeth values of ENSs and those of ECSs (Natto et al., 2005b), MSs (Natto et al., 2005b), and HNSs (Khemiss et al., 2017; Natto et al., 2005b). The number of remaining teeth mean values seem to be significantly higher in ENSs compared to those in ECSs (Khemiss, Ben Khelifa, et al., 2016). In the study of Javed et al. (2016), the two groups of ENS and ECS were matched for number of missing teeth. Compared to HNSs, ENSs had higher numbers of missing teeth. This study findings concerning DMFT are in line with another one (Khemiss et al., 2017), which reported no differences between DMFT mean values of ENSs and those of HNSs (Table 3S). In fact, the number of teeth influences the periodontal health (Thomas & Kenneth, 2003): More teeth per person is associated with greater severity of PD.
Compared to ECSs, ENSs had significantly lower PPD. They also included significantly lower percentages of smokers with PD (Table 1). These findings are not consistent with those of some similar studies (Table 2S). It seems that PPD mean values of ENSs were similar to those observed in ECSs (Bibars et al., 2015; Javed et al., 2016; Natto et al., 2005b) or in MSs (Bibars et al., 2015). However, they were higher than the data observed in HNSs (Bibars et al., 2015; Javed et al., 2016; Mokeem et al., 2018; Natto et al., 2005b), in MSs (Natto et al., 2005b), or in electronic cigarettes smokers (Mokeem et al., 2018; Table 2S). It seems that 6% of ENSs had PPD >4 mm (Malik et al., 2012). Moreover, the frequencies of PD among ENSs were similar to those observed in ECSs (Bibars et al., 2015; Natto et al., 2005b) or in MSs (Bibars et al., 2015; Natto et al., 2005b). However, they were higher than those observed in HNSs. The frequency of PD observed in this study (9.5%) was lower than that noted by Malik et al. (2012; 44%). Narghile use may have less influence on the smokers’ periodontal health than cigarette smoking.
Although both ENSs and ECSs exhibited the same PI and PI%, the GI mean value was significantly higher among ECSs than ENSs (Table 1). These findings are not in line with those observed in some comparable studies (Table 2S). It appears that GI mean values of ENSs were similar to those observed in ECSs (Natto et al., 2004, 2005b), in MSs (Natto et al., 2004, 2005b), or in HNSs (Natto et al., 2005b), but they were higher than the data observed in HNSs (Natto et al., 2004; Table 2S). In addition, 36% of ENSs had GI Score 2 (Malik et al., 2012). Moreover, when compared to ECSs, MSs, and HNSs, ENSs included similar percentages of smokers divided by GI% (Bibars et al., 2015).
The association between narghile use and gingival bleeding (GB, equal to the frequency of the gingival sites denoting GB on probing) is also controversial (Table 2S). It seems that GB mean values of ENSs were similar to those observed in ECSs (Bibars et al., 2015; Javed et al., 2016; Natto et al., 2004) or in MSs (Bibars et al., 2015; Natto et al., 2004). However, they were different from those observed in HNSs (Bibars et al., 2015; Javed et al., 2016; Mokeem et al., 2018; Natto et al., 2004). Some studies (Bergström & Boström, 2001; Lie, Timmerman, van der Velden, & van der Weijden, 1998; Mokeem et al., 2018) reported that the effect of cigarette smoking on the smokers’ gingival health is marked by a reduced inflammatory response in terms of GB. However, other studies reported increased GB in smokers (Baumert Ah, Johnson, Kaldahl, Patil, & Kalkwart, 1994; Linden & Mullally, 1994). Therefore, the influence of narghile use on the smokers’ gingival health needs to be further investigated.
The PPD of ENSs increases with age (Table 2). This result was in line with the findings of Natto et al. (2005b) who noted that “mean PPD increased with age.” The DMFT of ENSs increases with age and decreases with increase in the daily toothbrushing frequency (Table 2). These findings are in line with those reported in a large-scale multisite survey aiming at evaluating the dental conditions in patients with schizophrenia (n = 523, 33% were smokers; Tani et al., 2012), where older age and a low daily toothbrushing frequency were associated with a greater DMFT index. The number of remaining teeth of ENSs increases with increase in the daily toothbrushing frequency (Table 2). This result was in line with that observed in a Korean study (Song, Han, Choi, Ryu, & Park, 2016) where the number of remaining teeth means increased from 16.5 ± 0.5 in nonbrushers to 23.8 ± 0.1 in brushers of more than four toothbrushings per day.
The DMFT, PPD, and number of remaining teeth of ECSs were correlated with both age and level of cigarettes exposure. The DMFT of ECSs was correlated with daily toothbrushing frequency. This result was in line with that reported in the literature (Kassebaum et al., 2014; Kinane, Stathopoulou, & Papapanou, 2017).
Discussion of the methodology focused on the following points: inclusion and noninclusion criteria, recruitment methods, some aspects of narghile use (quantification, type and quantity of used tobacco, exposure level), comparison with control groups, and clinical examination. Discussion regarding some other points is reported in the Appendix.
The noninclusion criteria varied between the studies (Table 1S). This makes the comparison between data difficult. Since the prevalence and severity of PD are directly associated with age (PPD increases with age; Natto et al., 2005b; Thomas & Kenneth, 2003) and sex (males experienced greater levels than females; Thomas & Kenneth, 2003), only young males were included in this study. In similar studies, age varied from 17 (Natto et al., 2005b) to 70 (Natto et al., 2004) years. Some other studies included females (Bibars et al., 2015; Malik et al., 2012; Natto et al., 2005b). Among the 10 similar studies, only 2 did not report the “exclusive” character of narghile use (Al-Alimi et al., 2018; Malik et al., 2012). Ignoring the profile of smokers participating in the experiment is a methodological error (Chaouachi, 2006a). The smoker’s body preserves a memory of his physiological and behavioral practices (Chaouachi, 2009). For this reason, only ENSs should be evaluated in the group of narghile smokers (Ben Saad, 2009, 2010). In order to avoid additional sources of confusion, some important noninclusion criteria, known as risk factors for PD (e.g., diabetes mellitus, head and/or neck radiation therapy, use of certain medications; Thomas & Kenneth, 2003) were applied. Comparable to some local studies (Khemiss, Ben Khelifa, et al., 2016; Khemiss et al., 2017), only exclusive tabamel smokers were included. Lack of information regarding this important point makes comparison between the different studies complicated because when using another narghile tobacco (e.g., tombak or jurak, frequently used in Saudi Arabia) in comparison to tabamel, the pattern is different (Ben Saad, 2009; Chaouachi, 2009; Table 1S). It is established that schooling and/or socioeconomic levels affect the periodontal health. In fact, higher education and/or income were associated with lower levels (Shafagoj et al., 2002). In this study, despite the fact that compared to ENSs, ECSs had higher socioeconomic and schooling levels (Table 1), the two groups exhibited a marked alteration of PPD, GI, and PD. The lack of match between the two groups concerning the socioeconomic and schooling levels is certainly due to convenience sampling. However, the information that ECSs included significantly higher percentages of smokers having high schooling or socioeconomic levels when compared to ENSs reflects the “real life” as previously reported by Ben Hadj Mohamed and Ben Saad (2016). One important data that could be addressed as a noninclusion criterion, especially in the studies performed in Saudi Arabia (Javed et al., 2016; Mokeem et al., 2018; Natto et al., 2004, 2005b), is about chewing sticks, called miswak, widely used there (Chaouachi, 2006b). It appears that miswak use is at least as effective as toothbrushing in decreasing plaque and gingivitis. Besides, its antimicrobial effect is beneficial for the prevention and treatment of PDs (al-Otaibi, 2004). As done in some related studies (Bibars et al., 2015; Khemiss, Ben Khelifa, et al., 2016), smokers were recruited via flyers distributed in cafés. Other recruitment methods are reported (Table 1S). In this study, and similar to the majority of other ones, smokers were selected by a convenience sampling. As in any study using this recruitment method for its relative ease of access volunteers, availability, and the quickness with which data can be collected, there was a risk of volunteer bias (Ganguli, Lytle, Reynolds, & Dodge, 1998). Choosing volunteers during clinical studies leads to a selection bias since researchers may involuntarily approach some classes and avoid others. Thus, the sample might not represent the population as a whole (Lucas, 2014).
Similar to some local studies (Table 1S), narghile use was quantified in terms of NY. In the absence of a specific international codification, this method was preferred because it can be compared to the one used to quantify cigarette consumption. In similar studies, six additional methods of narghile use quantification were reported (Table 1S). This makes comparisons between studies very difficult.
As performed in some related clinical studies, the following seven data were collected: PI, PPD, number of remaining teeth, tooth mobility, DMFT, GI, and PD (Table 1S). Additional clinical data were evaluated in some studies: plaque %, GB, and the presence of calculus (Tables 1S and 2S). PI, the main outcome used to evaluate the periodontal health and to calculate the sample size, was evaluated via the Silness and Löe (1964) index, considered as the most commonly used index to evaluate oral hygiene (Silness & Löe, 1964). PPD, used to obtain information on the periodontium, especially the soft tissues, is the clinician’s most important diagnostic tool. PPD tells more about the gingival inflammation and the severity of PD than any other clinical diagnostic test (Thomas & Kenneth, 2003). However, PPD has some limitations. First, it depends on the probe angulation, pressure applied, tissue health, and probe diameter, and it is operator variable (Thomas & Kenneth, 2003). Second, the determinant of PPD is not only the connective tissue attachment location. The gingival health was assessed using GI modified by Löe (1967). GI, widely used in epidemiological studies to evaluate the gingival status (Thomas & Kenneth, 2003), was recommended by Lobene et al. (1989). The GI advantages are highlighted in the Appendix. PD is defined as “a disease with pocket formation and/or loss of periodontal attachment” (Thomas & Kenneth, 2003). Similar to other earlier studies (Bibars et al., 2015; Natto et al., 2005b), PD was defined as the occurrence of ≥10 sites with a probing depth of ≥5 mm per individual. This arbitrary definition was retained because PD is considered moderate at ≤5 mm with regard to attachment loss or pocket depth (Thomas & Kenneth, 2003). According to Natto et al. (2005b), “As the magnitude of prevalence is dependent on the definition of PD and the selection of a disease-specific criterion, comparisons with other studies may be difficult.” Tooth mobility was measured manually. This method is the simplest and the most practical in a clinical setting. However, mechanical devices should be used for research because they are more sophisticated and more precise (Mühlemann, 1951).
As previously conducted in some studies (Table 1S), a control group of ECSs was included. In some related studies, additional control groups of HNSs and/or MSs of narghile and cigarette were included (Table 1S). However, dealing with four groups of HNSs, ENSs, ECSs, and MSs (as done in four studies; Table 1S) or three groups of HNSs, ENSs, and ECSs [as done by Javed et al., 2016]) within a single study seems to be unprecedented in the literature. This raises some questions such as whether the prevalence of some epidemiological and/or clinical data (e.g., schooling and/or socioeconomic levels) in those groups is comparable.
This study had five limitations. First, the application of a nonvalidated medical questionnaire is a methodological limitation. Nowadays a standardized Arabic epidemiological questionnaire is available (Abou Arbid et al., 2017). Second, the fact that tobacco exposure quantification was based on an interview may have caused some over/understatement. This recall bias is likely to occur in cross-sectional studies where subjects are asked to remember exposure to risk factors (Berry, 1974). However, the reliability of self-reported tobacco use was considered high (Petitti, Friedman, & Kahn, 1981). Mokeem et al. (2018) quantified tobacco metabolites, (i.e., salivary cotinine) as a method for estimating tobacco exposure. Third, the nonevaluation of the smokers’ alcohol use can be a source of confusion. On the one hand, a greater risk of developing periodontal problems including gingival infection, increased pocket depth, and loss of attachment has been identified in alcoholics (Saini, Gupta, & Prabhat, 2013). On the other hand, it seems that among narghile smokers, 17%–31% were alcoholics (Hasni et al., 2019; Jawad, McEwen, McNeill, & Shahab, 2013). Fourth, the available evidence coming from cross-sectional and comparative studies does not establish causality (Raad et al., 2011). However, such studies allow researchers to compare different groups simultaneously since all the participants’ measurements were conducted at a single point in time (Mann, 2003). Cross-sectional and comparative studies are economic and easy to perform. They are informative, require less time than longitudinal ones, and provide evidence for any association (Berry, 1974; Mann, 2003). Fifth, this study sample size (n = 144) was intermediate compared with that of similar studies (Table 1S). However, this study sample size was calculated according to a predictive equation (Kang et al., 2008). It therefore seems to be satisfactory.
The discrepancy between results could be explained, in addition to the methodological limitations previously cited, by two additional factors. First is the different clinical approaches (e.g., clinical recordings in all the teeth, except the third molars; Javed et al., 2016; Khemiss, Ben Khelifa, et al., 2016; Khemiss et al., 2017; Malik et al., 2012; Mokeem et al., 2018; Natto et al., 2005b, or in only six representative teeth; Bibars et al., 2015). Second is the regional differences in the smokers’ oral health habits (Bibars et al., 2015; Khemiss, Ben Khelifa, et al., 2016; Natto et al., 2004). For instance, while in the Jordanian study of Bibars et al. (2015), the two groups of ENSs and ECSs did not differ significantly in the number of yearly visits to the dentist, in this study, and similarly in two previous North African and Saudi studies (Khemiss, Ben Khelifa, et al., 2016; Natto et al., 2004), ENSs were less regular in dental care. The regional differences in the daily toothbrushing frequency could not be advanced as a discrepancy factor since both ENSs and ECSs from Jordan (Bibars et al., 2015), Saudi Arabia (Natto et al., 2004), and Tunisia (present study; Khemiss, Ben Khelifa, et al., 2016) were matched for this data.
The underlying mechanisms responsible for the effects of narghile use on periodontal health are not elusive. Five mechanisms could be advanced. First, according to Natto et al. (2004, 2005b), the impact of narghile use on periodontal health is caused by the inhalation of toxic substances. Moreover, the levels of nicotine and its principal metabolite cotinine increase in the saliva of narghile smokers (Chaouachi, 2006b). Tobacco compounds may also affect the progression of PD by directly damaging the normal cells of the periodontal tissues. For example, nicotine can be stockpiled in and released from periodontal fibroblasts (Hanes, Schuster, & Lubas, 1991). These nicotine-exposed fibroblasts have an altered morphology and they have a weakened capacity to attach to root surfaces, to multiply, and to produce collagen (Cattaneo et al., 2000; Checchi, Ciapetti, Monaco, & Ori, 1999; Giannopoulou, Geinoz, & Cimasoni, 1999; James, Sayers, Drucker, & Hull, 1999; Raulin, McPherson, McQuade, & Hanson, 1988). In addition, nicotine can impregnate the root surface itself (Cuff, McQuade, Scheidt, Sutherland, & Van Dyke, 1989). These nicotine effects on both fibroblasts and root surfaces may in turn damage normal wound healing and renewal (Thomas & Kenneth, 2003). Moreover, it seems that narghile use results in increased volatile sulfur compound levels in the exhaled air (Al-Humaidi et al., 2017). These compounds were significantly associated with PD progression (Makino, Yamaga, Yoshihara, Nohno, & Miyazaki, 2012). Second, the increase of matrix metalloproteinase expression may be suggested (Cryer et al., 1976). Matrix metalloproteinases are the main enzymes that are associated with periodontal inflammation. They play an important role in the degradation of the host tissues supporting teeth (Cryer et al., 1976). Third, evidence demonstrates the effects of smoking on overstimulating the host response leading to the destruction of the periodontium. For example, tobacco smoke may stimulate the release of oxidative burst products and enzymes that could break down periodontal tissues (Kalra et al., 1991; Ryder, 1994). It may also promote an accumulation of neutrophils in periodontal tissues by stimulating a change in the level of adhesion molecules that control the migration and accumulation of neutrophils and other inflammatory cells in the tissue such as monocytes and lymphocytes (Palmer et al., 1999; Ryder et al., 1998). These cells secrete potentially destructive inflammatory cytokines such as interleukin 1β and tumor necrosis factor α. The latter is significantly higher in smokers’ gingival crevicular fluid (Boström et al., 1999, 2000). Furthermore, McGuire and Nunn (1999) identified that smokers with the genetic marker “elevated interleukin-1β production” have an increased probability of losing teeth and periodontal bone height when compared to HNSs who do not carry this genetic marker. Fourth, tobacco use may lead to a local release of collagenase, elastase, and other enzymes from inflammatory cells, which may destroy the periodontal tissues. The effect of smoke on the various enzymes remains unresolved. While one study identified an elevation of the elastase levels in the crevicular fluid, other studies reported no significant differences in the crevicular fluid elastase or collagenase levels (Pauletto et al., 2000; L. Persson et al., 1999). Finally, the alteration of the buffering capacity, one of the key factors that may affect individual caries’ risk, can be advanced since narghile use is responsible for a lower salivary buffering capacity (Khemiss et al., 2017).
In conclusion, both narghile and cigarette smoking alter the smokers’ periodontal health, but narghile use has a less detrimental effect than cigarette smoking. The results of this study do not provide clear evidence that narghile use is a safe way of smoking. Thus, global actions against this type of smoking are necessary. This should include regulating narghile products, increasing public awareness of its associated harmful effects on health, and providing support for narghile research activities to increase the knowledge of dentists about this type of smoking.
Supplemental Material
Appendix – Supplemental material for Comparison of Periodontal Status Between Male Exclusive Narghile Smokers and Male Exclusive Cigarette Smokers
Supplemental material, Appendix for Comparison of Periodontal Status Between Male Exclusive Narghile Smokers and Male Exclusive Cigarette Smokers by Mehdi Khemiss, Dalila Ben Fekih, Mohamed Ben Khelifa and Helmi Ben Saad in American Journal of Men’s Health
Footnotes
Acknowledgements
Authors wish to thank Professor Samir Boukattaya for his invaluable contribution in the improvement of quality of the writing in the present article. They also wish to express their sincere gratitude to all participants for their cooperation.
Abbreviations’ List
Authors’ Contributions
MK, DBF, and HBS: literature search, data collection, study design, analysis of data, manuscript preparation, and review of manuscript.
MBK: study design, analysis of data, manuscript preparation, and review of manuscript.
All authors read and approved the final manuscript.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: HBS reports personal fees from AstraZeneca, Teriak, and Chiesi.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.