
Abstract
Cardiovascular disease is the leading cause of mortality in the United States, accounting for one fourth of deaths. Higher rates of obesity put Hispanic and Black men at increased risk. The American Heart Association cites diet quality, physical activity, and body weight as alterations responsive to health promotion intervention. Prevention strategies need to begin in adolescence and the emerging adulthood years to impact cumulative risk factors. A scoping review identified search terms and this was followed by a systematic review of Cumulative Index to Nursing and Allied Health Literature (CINAHL) and PubMed databases for articles published in English from January 1, 2002, through May 11, 2017. This review explores community-based content, delivery, recruitment, or retention strategies used with young men of color aged 15 to 24 years. Of 17 articles describing 16 individual interventions and 1 describing multiple interventions (with samples ranging from 37 to 4,800), 13 reported significant results in one or more domains. No studies specifically targeted the needs of young men and only three had more than 50% male participants. There was a gap in studies that addressed young men in the ages of interest with most interventions reaching participants aged 11 to 19 years. Cultural tailoring was addressed through recruitment setting, interventionist characteristics, community involvement, and theoretical frameworks such as motivational interviewing that allow individual goal setting. Because young men seek access to preventive health services less than young women, it is suggested that interventions that are community based or use push technology (send information directly to the user) be increased.
Background
Cardiovascular disease, a range of conditions including heart disease and stroke, represents a significant health burden in the United States (Mozaffarian et al., 2016). Heart disease is the leading cause of death (Kochanek, Murphy, Xu, & Tejada-Vera, 2016), accounting for almost one fourth (23.4%) of deaths in Americans in 2014. Men have higher rates of both cardiovascular morbidity and mortality compared to women (Kochanek et al., 2016; Mozaffarian et al., 2016). Hispanic and Black men have higher rates of obesity, and are, in turn, at increased risk of cardiovascular disease compared to non-Hispanic White men (Daviglus et al., 2012; Mozaffarian et al., 2016). Racial and ethnic disparities in all-cause (i.e., death attributed to any cause) and heart disease–specific mortality, while narrowing, continue to persist (Beydoun et al., 2016; Gilbert et al., 2016). These disparities reflect documented differences in access to and use of health-care services as well as structural and community-level factors, including inequalities in social and built environments (housing, poverty, discrimination, and racism; Adler & Rehkopf, 2008; Douglas, Grills, Villanueva, & Subica, 2016; Gilbert et al., 2016; Jones, Crump, & Lloyd, 2012; Martin, Harris, & Jack, 2015; Shelton et al., 2009; Vega, Rodriguez, & Gruskin, 2009; Williams & Jackson, 2005).
There is strong evidence that regular physical activity has numerous physical and mental health benefits, including reduced obesity, leading to improved cardiovascular and metabolic health (Reiner, Niermann, Jekauc, & Woll, 2013). Dietary changes, specifically decreased consumption of sugar and increased fruit and vegetable consumption, have also been shown to reduce the prevalence of obesity and, in turn, obesity-related morbidity and mortality (Hu, 2013; Wang et al., 2014). The American Heart Association identifies diet quality, physical activity, and body weight as the three alterable elements with the greatest potential for improvement, and therefore these should be the primary focus of health promotion interventions (Mozaffarian et al., 2016), with health promotion, in this inquiry, being defined as the process of enabling people to increase control over and improve their health.
Recognizing that critical factors accumulate and interact to increase the risk of obesity, health promotion interventions to prevent, rather than treat, obesity that begins in adolescence and early adulthood are key to reducing the health burden of cardiovascular disease across the life span (Johnson, Gerstein, Evans, & Woodward-Lopez, 2006). Weight gain in adolescence has been shown to be associated with elevated occurrence of heart disease (Tirosh et al., 2011). Furthermore, there are few behavioral weight loss interventions that have been shown to be effective in the long term (Curioni & Lourenco, 2005; Douketis, Macie, Thabane, & Williamson, 2005; Diabetes Prevention Program Research Group, 2009; Wing & Phelan, 2005).
To reduce disparities in cardiovascular disease, culturally competent interventions that acknowledge and address context, values, and the root causes of obesity and related health risks are needed (Jones, Crump, & Lloyd, 2012; Osei-Assibey & Boachie, 2012). Interventions must be responsive to age-, gender-, race-, and ethnicity-specific needs. Young men (including both adolescents [15–19 years] and young adults [20–24 years]) have specific health needs and goals (Bell, Breland, & Ott, 2013; Jones et al., 2012; Martin et al., 2015), yet very few behavioral weight loss interventions (5% in a recent review) are specifically designed for men (Pagoto et al., 2012). Research has identified systematic differences in physical activity and diet by gender, race, and ethnicity among both adolescents (Kim, Grimm, Harris, Scanlon, & Demissie, 2012; Taber, Chriqui, Vuillaume, Kelder, & Chaloupka, 2015) and adults (Hiza, Casavale, Guenther, & Davis, 2013; Newton, Griffith, Kearney, & Bennett, 2014). Some studies have found that engagement and outcomes in behavioral weight interventions differ by race and gender (Jelalian et al., 2008; West, Prewitt, Bursac, & Felix, 2008; Wing & Anglin, 1996), although these findings are not consistent (Newton et al., 2014). Recent systematic reviews have examined the programmatic features and outcomes of behavioral weight loss or weight maintenance interventions for multiethnic adults in general (Osei-Assibey, Kyrou, Adi, Kumar, & Matyka, 2010; Seo & Sa, 2008; Yancey, Ory, & Davis, 2006): Black adults (Osei-Assibey & Boachie, 2012), Black men (Newton et al., 2014), and Hispanic adults (Whittemore, 2007). Each of these reviews called for tailored interventions that address the specific needs, values, cultural orientations, baseline health states, and community contexts of the participants and noted small sample sizes and heterogeneity of study populations in the studies reviewed.
The developmental stage of adolescents and young adults is particularly relevant for healthy weight and cardiovascular health promotion and interventions. Diet and physical activity behaviors established in adolescence persist into later adulthood (Sanchez et al., 2007; Zahran, Zack, Vernon-Smiley, & Hertz, 2007), and addressing these behaviors early can have beneficial effects on health status later in life (Patton et al., 2016). Recent systematic reviews of health promotion interventions for adolescents and young adults (Ashton et al., 2015; Laska, Pelletier, Larson, & Story, 2012; Stoner et al., 2016), including one specifically among young men between the ages of 18 and 25 years (Poobalan, Aucott, Precious, Crombie, & Smith, 2010), identified age- and life stage–related dramatic shifts that affect both diet and physical activity. In this life stage, sometimes referred to as emerging adulthood (Arnett, 2007), physical activity patterns change as young adults enter college or transition to the workplace, and diet changes as a result of doing one’s own food shopping and cooking. Reviews of health promotion interventions for adolescents and young adults (Ashton et al., 2015; Poobalan et al., 2010) also identified postintervention increases in mental health and quality of life outcomes, such as self-esteem.
To date, however, no reviews have been identified that address the intersection of gender, age, and race and ethnicity as they relate to healthy weight and cardiovascular health promotion interventions for Black or Latino men in adolescence and young adulthood. To guide the development and implementation of such interventions for young men of color, we conducted a systematic review to examine: (a) what the content, features, and approaches of behavioral health promotion interventions to promote healthy diet and physical activity that are designed specifically to reach male adolescents (aged 15–19 years) and young adult men (aged 20–24 years) of color are; (b) how such interventions are culturally or developmentally tailored; and (c) what outcomes are reported specifically for young men or young men of color.
Methods
Overview
The current systematic review was undertaken as a first step to guide the development and refinement of a health promotion intervention for young men of color who are between the ages of 15 and 24 years. The focus of this inquiry is to identify approaches to content, delivery, recruitment, or retention that have been used by other interventions. Specifically, we examine the following key questions:
To what extent are published health promotion interventions specifically addressing the needs or experiences of young men of color between the ages of 15 and 24 years?
What are the key characteristics of interventions aimed at increasing physical activity and improving diet conducted with young men of color?
How were intervention content, setting, or delivery tailored to meet the specific cultural needs (as defined by gender, race, and/or ethnicity) of their participants?
How was intervention content, setting, or delivery tailored to meet age-related or developmental needs of their participants?
What recruitment and retention strategies were employed at the start of the intervention, and how were these strategies adapted to address challenges that were encountered?
Which intervention elements are most effective for subgroups identified by gender, race, and/or ethnicity in this age group?
Methods for this systematic review were guided by the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA; Moher, Liberati, Tetzlaff, Altman, & Group, 2009), as outlined in Figure 1. The systematic review protocol was not registered.

Summary of literature search.
Search Strategy
To assist in the articulation of the key questions and inform search strategies, a scoping review was first conducted to identify review articles and systematic reviews. The scoping review facilitated the articulation of the key concepts underpinning the research question, refining of the research question to avoid overlap with existing evidence, mapping of the research question to specific search terms, and identification of the main sources and types of evidence available (Arksey & O’Malley, 2005). This approach has recently been used by others studying health promotion interventions for men (Gavarkovs, Burke, & Petrella, 2016; Seaton et al., 2017). Working from the scoping review findings, the key questions mentioned earlier were operationalized, identifying populations, interventions, comparators, and outcomes (PICO) to clearly delineate the parameters of the research question (Table 1).
Eligibility Characteristics of Studies Included in Review (PICO).

Note. MeSH = Medical Subject Headings; PICO = populations, interventions, comparators, and outcomes.
Because this systematic review was intended to inform the development and implementation of interventions in primarily nursing-delivered health-care settings, the following electronic databases were identified prior to specifying the search terms: PubMed and Cumulative Index to Nursing and Allied Health Literature (CINAHL). Electronic database searching methods were supplemented with identification of articles through manual review and hand-searching references within the references of reviewed papers. The electronic database search was conducted in May 2017, encompassing articles published in English from January 1, 2002, through May 11, 2017. Search terms (Table 1) were identified through an initial scoping review of previously published review articles on correlates of diet and physical activity in racially and ethnically diverse populations (Harley et al., 2014; McMurray et al., 2000) and review articles on health promotion interventions in child and adult populations (Fitzgibbon et al., 2005; Flynn et al., 2006; Kong, Tussing-Humphreys, Odoms-Young, Stolley, & Fitzgibbon, 2014).
Articles that met the criteria of describing community-based (not hospital-based or physiology laboratory–based) interventions including at least 10 male participants between the ages of 15 and 24 years and addressing physical activity, diet, weight, and/or body size were included in the review. Interventions that included only populations defined by a health condition other than obesity, diabetes, or cardiovascular disease (e.g., cerebral palsy), that compared the relative performance of two different types of exercise, or that included directly observed exercise using specific exercise equipment were excluded. No limits were placed on the duration of the intervention or follow-up period. Title and abstract review were conducted consecutively by two reviewers (KH, SG), using independent spreadsheets to track exclusion reasons. Full article review for inclusion was conducted by three reviewers (KH, SG, MF), with consensus achieved for all exclusions (see Figure 1). After review of manuscripts was initiated, and challenges were encountered in synthesizing results by race and ethnicity for non-U.S. countries (e.g., multiple country settings or with indigenous populations), non-U.S. interventions (n = 8) were excluded.
Data Synthesis
To synthesize findings, each article was reviewed to summarize the extent to which gender, age, or race or ethnicity (or the intersection across several of these factors) was planned for, addressed, or encountered by interventions in terms of recruitment or retention strategies; theoretical framework or approach; intervention content; delivery setting, mechanism, or format; subgroup outcome differences; and/or recruitment or retention challenges.
Results
A total of 17 articles describing 16 individual interventions and 1 article describing the effects of multiple ongoing interventions in Charlotte, North Carolina, were included for review. A variety of outcomes were measured and categorized as being related to diet, physical activity, anthropomorphic measurements, biological measurements, and knowledge and attitudes about diet and physical activity.
Participants
Participant characteristics are described in Table 2 (Part A). Sample sizes per intervention ranged from 37 (Carcone et al., 2013) to 1,600 (Bleich, Herring, Flagg, & Gary-Webb, 2012). The analysis of multiple interventions involved in the Charlotte REACH Projects used a population-based sample of 4,800 survey respondents (Plescia et al., 2008). While the inclusion criterion was that interventions must have included at least 10 male participants between the ages of 15 and 24 years, the ages of participants in included studies ranged from 2 to 35 years, with the majority of interventions (71%, 12/17) having participants exclusively in the age range of 11 to 19 years. Nine interventions (53%) included parents or other adult family members in the intervention along with their children or adolescents (Bean et al., 2015; Dolinsky, Armstrong, Walter, & Kemper, 2012; Jones et al., 2008; Mackey et al., 2015; Patrick et al., 2013; Rieder et al., 2013; Wieland et al., 2016). The percentage of male participants ranged from 20% (Macdonell, Brogan, Naar-King, Ellis, & Marshall, 2012) to 67% (Covelli, 2008). The synthesis revealed few interventions that included predominantly young men of color. Three had samples comprised of predominantly (>50%) male and exclusively Black and Latino adolescents (Bleich et al., 2012; Covelli, 2008; Schnall et al., 2013), but none of these interventions included young adult men over age 19 years. Conversely, one intervention (James, Adams-Huet, & Shah, 2015) included young adults, with an average age of approximately 22 years, but the sample was predominantly female (56%) and non-Latino White (only 4% Black and 12% Latino).
Part A: Population and Sample Characteristics.

Part B: Intervention Description.

Note. *Intervention setting (region, state, city/town) as specified in the manuscript.
Part C: Study Findings.

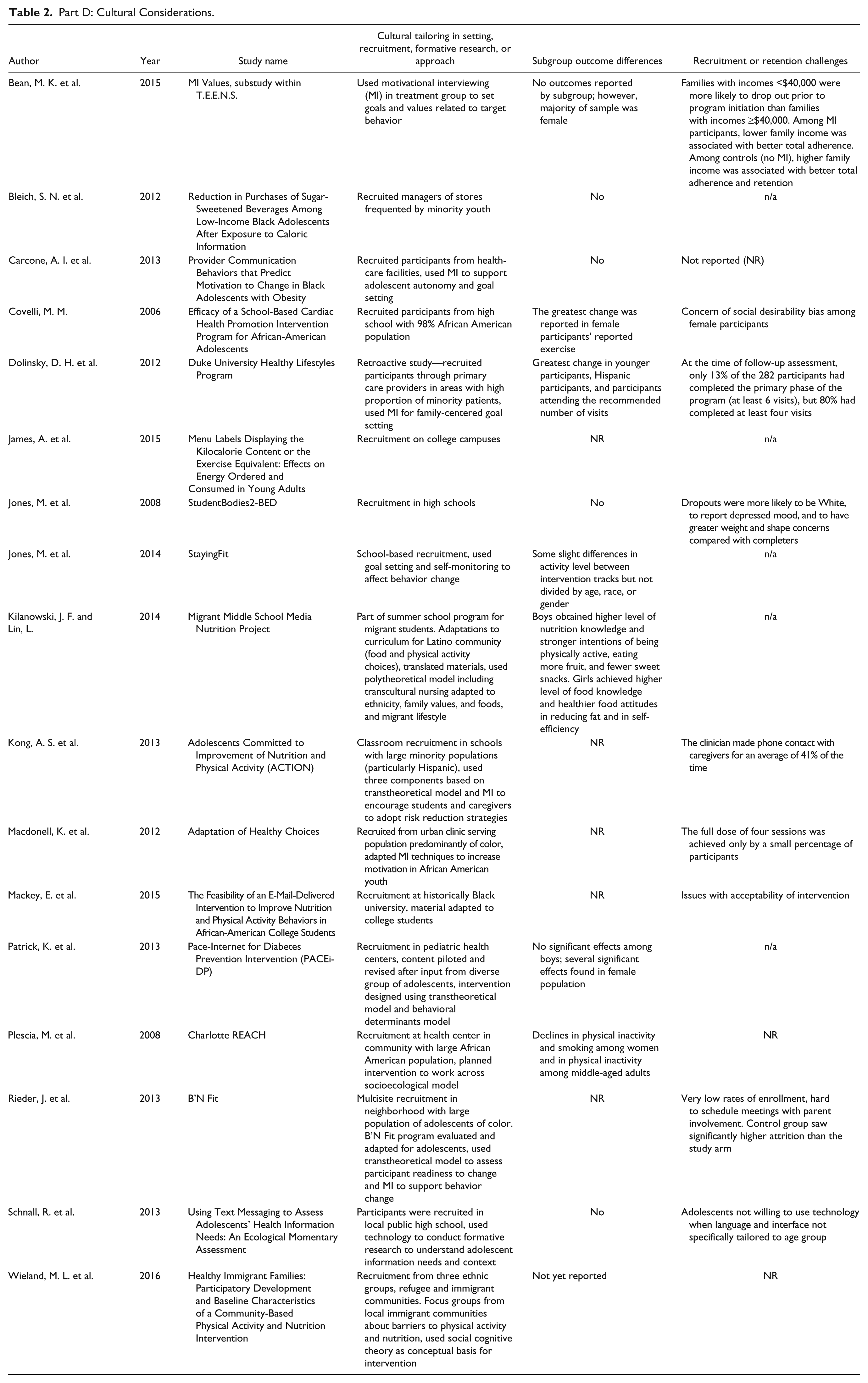
Part D: Cultural Considerations.
Interventions
The interventions (described in Table 2, Part B) ranged in intensity, from posting caloric information (Bleich et al., 2012; James, Adams-Huet, & Shah, 2015) or specific messaging used in encounters (Carcone et al., 2013) to multiple sessions occurring over a 6-month period (Bean et al., 2015). The majority (11 of 17) of interventions were theory based, most commonly (n = 4) using motivational interviewing (MI) alone (Bean et al., 2015; Carcone et al., 2013; Dolinsky et al., 2012; Macdonell et al., 2012) or using MI in combination with a transtheoretical (Stages of Change) framework (Kong et al., 2013; Rieder et al., 2013). Seven of the interventions were for the treatment of obesity, only enrolling participants who were overweight or obese (Bean et al., 2015; Carcone et al., 2013; Dolinsky et al., 2012; Kong et al., 2013; Macdonell, Brogan, Naar-King, Ellis, & Marshall, 2012; Patrick, et al., 2013; Rieder, et al., 2013). Nine interventions focused on obesity prevention, although they did not state the exclusion of overweight or obese participants (Bleich et al., 2012; Covelli, 2008; James, Adams-Huet, & Shah 2015; Jones et al., 2008; Kilanowski & Lin, 2014; Mackey et al., 2015; Plescia et al., 2008; Schnall, et al., 2013; Wieland et al., 2016). One intervention (Jones et al., 2014) recruited participants who were normal weight as well as those who were overweight or obese, and delivered different tracks of a similar Internet-based intervention, aimed at either prevention or treatment of overweight/obesity. The majority of interventions (n = 11) took place in urban areas (Bleich et al., 2012; Carcone et al., 2013; Covelli, 2008; Dolinsky et al., 2012; Jones et al., 2008; Jones et al., 2014; Kong et al., 2013; Mackey et al., 2015; Patrick et al., 2013; Plescia et al., 2008; Rieder et al., 2013; Schnall et al., 2013; Wieland et al., 2016). The delivery setting varied, with four delivered in a school setting, three at home, three exclusively in a clinic setting, two exclusively in a community setting, and one in both clinic and community settings. Fewer than half (n = 6) used technology to deliver intervention content, including DVDs (Kong et al., 2013), videotaping of sessions (Carcone et al., 2013), or text messaging (Patrick et al., 2013; Schnall et al., 2013). Two of the interventions were online only (not including eligibility, enrollment, or outcome measurement processes), using web-based videos and discussion boards (Jones et al., 2008) and e-mail messaging (Mackey et al., 2015).
Four articles (Carcone et al., 2013; Mackey et al., 2015; Schnall et al., 2013; Wieland et al., 2016) were feasibility or pilot studies not statistically powered to report impacts. Of the remaining 13 interventions, all reported significant results in at least one domain (Table 2, Part C). One intervention (Bean et al., 2015) tested MI as an adjunct to obesity treatment for adolescents (predominantly African American females) and only examined treatment adherence, observing significantly higher adherence to gym visits and nutritional consults compared to the arm without MI. Of those remaining, eight reported significant changes in diet (Bleich et al., 2012; Covelli, 2008; James, Adams-Huet, & Shah, 2015; Jones et al., 2008; Jones et al., 2014; Macdonell, Brogan, Naar-King, Ellis, & Marshall, 2012; Plescia et al., 2008; Rieder et al., 2013). Of these, three reported decreases in sugar-sweetened beverage (SSB) consumption (Bleich et al., 2012; Jones et al., 2014; Macdonell, Brogan, Naar-King, Ellis, & Marshall, 2012). Three interventions reported increases in fruit and vegetable consumption (Covelli et al., 2008; Jones et al., 2014; Rieder et al., 2013). Jones and colleagues (2008) reported a decrease in episodes of binge eating among participants, and James, Adams-Huet, and Shah (2015) reported decreased caloric consumption during a meal in participants in the intervention group compared to controls.
Six intervention studies reported a significant change in physical activity, with three reporting increases in physical activity, reported as general increases in “exercise per week” (Covelli et al., 2008), having reported “at least one day of 60 or more minutes of exercise in the last 7 days” (Jones et al., 2014) and increases in “vigorous physical activity” (Rieder et al., 2013). Four other interventions reported significant decreases in sedentary behavior, as measured by weekday screen time (Kilanowski & Lin, 2014), “episodes of sedentary behavior” (Jones et al., 2008), and average hours of sedentary behavior per day (Patrick et al., 2013). Plescia and colleagues (2008) reported a “decrease in physical inactivity” among female but not among male participants. Possible explanations for positive effects among female but not male participants may be attributed to higher social desirability of reporting positive change among females and/or differences by gender in the type and frequency of physical activity (Covelli et al., 2008).
Six intervention studies reported significant changes in body mass index (BMI) as an anthropomorphic measurement (Dolinsky et al., 2012; Jones et al., 2008; Jones et al., 2014; Lin, 2014; Kong et al., 2013; Rieder et al., 2013). While Kilanowski and Lin (2013) found only changes across BMI categories, Kong and colleagues (2013) reported decreases in waist circumference in addition to absolute decreases in BMI.
In total, four studies examined biological outcomes. Of these, only one, a university clinic-based intervention for families using an MI approach (Dolinsky et al., 2012), found statistically significant impact. This intervention, the Healthy Lifestyles Program, was based in a pediatric setting in which the health-care provider provided medical management of obesity-associated comorbidities. It integrated interviews in the initial visit to facilitate family-centered goals for lifestyle change, while later visits included a provider and dietician for nutrition therapy. The results reported significant changes in biological measurements, including serum triglycerides, cholesterol, and blood pressure. Two interventions (Covelli et al., 2008; Kilanowski & Lin, 2014) reported increases in physical activity and nutrition knowledge.
Five studies reported gender-based differences in outcomes, frequently (but not consistently) with female participants showing greater change in physical activity (Covelli, 2008; Patrick et al., 2013; Plescia, Herrick, & Chavis, 2008). Only one study (Plescia et al., 2008) reported significant findings only in a gender subgroup, reporting that smoking and physical inactivity decreased among female but not male participants.
Cultural Considerations
The extent to which the interventions were tailored to address contextual factors, health concerns, or health behaviors by gender, race, or ethnicity, or to take into account various cultural considerations in their design, recruitment, or retention is summarized in Table 2 (Part D). None of the interventions studied was specifically designed to reach men in general or more specifically men of color. The most common strategy described in the studies was targeted recruitment, with eight interventions (Covelli, 2008; James, Adams-Huet, & Shah, 2015; Jones et al., 2008; Jones et al., 2014; Kilanowski & Lin, 2013; Kong et al., 2013; Mackey et al., 2015; Schnall et al., 2013) targeting enrollment through schools to reach their targeted demographic. Another five interventions recruited from health-care settings. Of the 11 interventions that were specifically designed to reach populations of color, not all described conducting planning work or formative research or testing with members of their target communities before intervention rollout. Those that did used approaches such as conducting a feasibility study (Mackey et al., 2015; Schnall et al., 2013) or formative research and pilot testing (Patrick et al., 2013) with diverse members of the target community to guide improvements in intervention content and messaging. Others carried out needs and asset assessment of the community (using it to design and refine the intervention; Plescia et al., 2008) or used a participatory approach (including community advisory boards) to involve the community in all aspects of the intervention, including intervention content (Kilanowski & Lin, 2013; Kong et al., 2013; Plescia et al., 2008; Wieland et al., 2016). Some had the intervention carried out by staff whose cultural background (Kilanowski & Lin, 2013) or age group (Rieder et al., 2013) mirrored that of participants.
Some studies used a theoretical framework on which the intervention was built to tailor the intervention to meet specific population needs or concerns. MI, used by six of the interventions studied, elicits from participants their personal goals and potential identified barriers to change. These MI-based interventions were therefore considered to be well suited to address person-centered outcomes with specific populations defined by age group, race, ethnicity, or culture (Bean et al., 2015). Supporting this approach, a meta-analysis of 72 MI interventions found larger effect sizes among ethnic minority populations (Hettema, Steele, & Miller, 2005). Transcultural nursing (Kilanowski & Lin, 2013) is another theoretical approach used to explicitly guide the incorporation of cultural considerations in intervention content.
Discussion
This review identified several commonalities across interventions. All of the interventions that examined diet or physical activity outcomes found significant positive effects, although it should be acknowledged that effect sizes were small. Most of the interventions used schools or clinics as a way to target recruitment, and more than half included parents or caregivers in the interventions. Interventions designed to specifically reach specific communities defined by race, ethnicity, or life stage followed best practices of engaging community members in the intervention planning and conduct through participatory approaches, conducting formative work, or using a theoretical underpinning that builds in person-centered approaches. Using participatory approaches has been shown to be an effective way to address adolescents’ specific barriers to behavior change (Goh et al., 2009).
Cultural sensitivity in health promotion interventions involves addressing two dimensions (Resnicow, Baranowski, Ahluwalia, & Braithwaite, 1999): surface and deep structure. The surface structure matches materials and messages to observable, “superficial” characteristics of a target population, such as by using the language, food, or locations familiar to and preferred by the target audience. However, culturally sensitive interventions must also address the deep structure, by acknowledging and incorporating cultural, social, historical, and psychological forces that influence the target health behavior in the target audience. Attention to deep structure must also acknowledge social determinants of health (the conditions in which people are born, grow, live, work, and age), specifically racism and discrimination, which have been solidly linked to racial and ethnic health disparities overall and in cardiovascular health (Braveman & Gottlieb, 2014; Paradies et al., 2015; Williams & Jackson, 2005; Jones, Crump & Lloyd, 2012). This review suggests that deep structure can be addressed by using theory-driven communication approaches such as MI to guide interventions by encouraging participants to identify their personal goals, values, and beliefs, and set their own context-specific goals, while taking into account forces, both internal and external, that may serve as facilitators or barriers to planned behavior change.
Some limitation in this review, and in the underlying studies, must be acknowledged. The aim of this study was to synthesize information on the approach used by the intervention designers and implementers, rather than to draw conclusions on the relative effect sizes yielded by the different approaches, an examination precluded by the heterogeneity of outcomes covered by the underlying studies. Publication bias must be considered here; likely, given the inclusion of terms that map to outcomes (e.g., BMI), the approach and search terms used here may have overlooked interventions that were culturally tailored but did not yield significant changes or differences in outcomes. Finally, not all of the studies that observed significant differences in anthropometric outcomes also observed significant changes in mediating factors such as diet and physical activity, placing a limit on one’s ability to draw causal claims.
Several unanswered questions remain about how health promotion interventions can effectively engage adolescent and young adult men of color to yield health behavior change that ultimately will affect chronic disease risk and address disparities. This review revisited an inquiry (Flynn et al., 2006) over a decade ago, which found that “few programmes for children and adolescents are gender-specific and . . . programmes specifically addressing boy’s needs are rare (p. 36).” This review indicates that this gap still persists for adolescents and young adults: Of the 17 interventions in this review, none was specifically designed for young men, and only three of them had more than 50% male participants. Outside the context of interventions, related qualitative work suggests that young men have specific conceptualizations and definitions of health that could be utilized when developing content for interventions that seek to reduce sedentary behaviors and increase healthy eating (Wright, O’Flynn, & Macdonald, 2006). Previous research on health disparities in men of color has called for an examination of the intersection of race and ethnicity with gender (Griffith, Metzl, & Gunter, 2011), and the need for interventions to address the ways in which these factors intersect, for example, as ideals about masculinity assigned by mainstream White society may lead to internal conflict. There do exist a number of interventions specifically for adult African American males (Treadwell et al., 2010), as covered in some key reviews (Newton et al., 2014; Osei-Assibey & Boachie, 2012).
This review sought to identify interventions that address the additional intersection of the age- and life stage–specific needs of young men as they transition from school age to adulthood, but found scant guidance on interventions that addressed all factors. This review uncovered only one study (James, Adams-Huet, & Shah, 2015) that included young adults, yet with few (16%) participants of color. Emerging adulthood, a term sometimes used to describe the transitional period between adolescence and adulthood (Arnett, 2007), is a developmental stage that presents specific needs, capabilities, and contexts that directly affect a health promotion intervention’s approach and potential for positive impact. The best practices identified for conducting childhood obesity prevention interventions (Flynn et al., 2006) do not necessarily hold here. Intervention strategies for adults have been shown to be less effective for young adults (Gokee-LaRose et al., 2009), with trials showing lower rates of participation and attendance. Attrition and low dose, a barrier to many interventions that seek to reach adolescents (Crutzen et al., 2011), was addressed in more than half of the interventions studied here by including parents or other adult caregivers in the intervention, an approach that would not be appropriate for young adults. In the emerging adulthood age range of interest here (between the ages of 15 and 24 years), new independence and self-reliance for health care and well-being that previously would have been encouraged by parents, teachers, or other adult caregivers, is in the hands of young adults.
Because young men have been shown to access preventive health services less frequently than young women (Rand et al., 2007), community-based or technology-based interventions that do not require engagement with a health-care provider have the potential to reach young men in need of guidance and support around developing and maintaining healthy behaviors. Technology that enables push-out engagement that sends information directly to participants through e-mail contacts (Mackey et al., 2015; Patrick et al., 2013), text messages (Schnall et al., 2013), or push notifications in apps (messages that appear even when the participant is not using the app)—rather than a pull-in approach that requires participants to seek out a website or app—can reduce documented challenges in delivering sufficient exposure to intervention content for young adults; Crutzen et al., 2011). In this review, however, only six of the studied interventions used technology-based interventions, and of these, only three (Jones et al., 2014; Kong et al., 2013; Patrick et al., 2013) measured changes in diet, physical activity, or anthropometry.
Future work should develop and test interventions specifically designed for young men of color. While this review suggests that theory-guided or technology-based approaches would show the most promise, additional evidence is needed.
Footnotes
Acknowledgements
The authors acknowledge Anna Getselman, director of the Augustus C. Long Health Sciences Library, and Meghana Shamsunder for their contributions to the literature search methodology.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.