
Abstract
To identify individual and contextual factors contributing to overall mortality among men diagnosed with prostate cancer in Florida, a random sample of patients (between October 1, 2001, and December 31, 2007) was taken from the Florida Cancer Data System. Patient’s demographic and clinical information were obtained from the Florida Cancer Data System. Comorbidity was computed following the Elixhauser Index method. Census-tract-level socioeconomic status and farm house presence were extracted from Census 2000 and linked to patient data. The ratio of urologists and radiation oncologists to prostate cancer cases at the county level was computed. Multilevel logistic regression was conducted to identify significance of individuals and contextual factors in relation to overall mortality. A total of 18,042 patients were identified, among whom 2,363 died. No racial difference was found in our study. Being older at diagnosis, unmarried, current smoker, uninsured, diagnosed at late stage, with undifferentiated, poorly differentiated, or unknown tumor grade were significantly associated with higher odds of overall mortality. Living in a low-income area was significantly associated with higher odds of mortality (p = .0404). After adjusting for age, stage, and tumor grade, patients who received hormonal, combination of radiation with hormone therapy, and no definitive treatment had higher odds of mortality compared with those who underwent surgery only. A large number of comorbidities were associated with higher odds of mortality. Although disease-specific mortality was not examined, our findings suggest the importance of careful considerations of patient sociodemographic characteristics and their coexisting conditions in treatment decision making, which in turn affects mortality.
Introduction
Prostate cancer is the most common solid malignancy (excluding skin cancer) and the second leading cause of cancer-related death for American men. In the United States, an estimated 238,590 new cases of prostate cancer will be diagnosed in 2013, whereas an estimated 29,720 men will die of this disease (American Cancer Society, 2013). The State of Florida ranks second behind California for both incidence (17,330 estimated new cases) and mortality (2,200 estimated deaths) from prostate cancer in 2013 (American Cancer Society, 2013).
Prostate cancer mortality rate in the United States started declining steadily in the early 1990s. This decline is believed to be partly due to early detection and treatment (Howlader et al., 2012; Sarma & Schottenfeld, 2002). In spite of this decline, striking racial/ethnic differences in incidence and mortality still persist in the United States and the State of Florida. Reasons for the persistence of these racial disparities have been difficult to disentangle. Possible explanations include differences in screening leading to differences in the stage and size of tumors at diagnosis, tumor biology (aggressive disease), inadequate receipt of appropriate prostate cancer treatment, and underlying patient comorbidities and socioeconomic factors (Gilligan, Wang, Levin, Kantoff, & Avorn, 2004; Harlan, Brawley, Pommerenke, Wali, & Kramer, 1995; Haynes & Smedley, 1999; Smedley, Stith, & Nelson, 2003).
Stages at diagnosis and tumor characteristics have been consistently associated with mortality (Johansson, Holmberg, Johansson, Bergström, & Adami, 1997; Jonsson et al., 2006; Taksler, Keating, & Cutler, 2012). Black men tend to be diagnosed at an advanced stage and have a poorer clinical outcome than do Whites. It also has been documented that Black men living in the United States develop prostate cancer at an earlier age and have a higher mortality than do White men of similar clinical staging (American Cancer Society, 2013; DeLancey, Thun, Jemal, & Ward, 2008; Moul et al., 1995; Powell, Bock, Ruterbusch, & Sakr, 2010). However, it is unclear whether racial differences in stage at diagnosis are solely due to biologic factors (Hoffman et al., 2001; Jones et al., 2008).
Underutilization of screening services by Blacks and other minority groups may be a factor contributing to advanced stage at diagnosis (Jones et al., 2008; Ward et al., 2009), and subsequently to greater mortality. Indeed, research on screening reported that Black men were less likely to get prostate-specific antigen (PSA) screening than their White counterparts (Carpenter et al., 2010; Etzioni et al., 2008). Despite this argument, there is an ongoing debate over the extent to which PSA screening contributes to the decline in prostate cancer mortality (Andriole et al., 2009; Barry, 2009; Schröder et al., 2009; Schwartz et al., 2009). For instance, after completing an evidence review, the U.S. Preventive Services Task Force decided to recommend against screening for PSA, concluding that there is moderate or high certainty that the service has no net benefit or that the harms outweigh the benefits (Chou et al., 2011). However, due to notable underrepresentation of Blacks in these recent studies, our understanding of racial differences remains unclear.
Patients of lower socioeconomic status (SES) and with limited health insurance coverage are likely to be diagnosed at later stages and/or have worse mortality outcomes (Dall’Era, Hosang, Konety, Cowan, & Carroll, 2009; Major et al., 2012). Men with private health insurance are, in general, diagnosed with prostate cancer at a more favorable stage than do men who are insured through Medicare or Medicaid, or the uninsured, which allows them to have a more favorable mortality prognosis. Lack of facilities or availability of providers also persist in certain geographic areas, mostly in rural settings (Comer & Mueller, 2008; Joynt, Harris, Orav, & Jha, 2011), which may contribute to late-stage diagnosis and increased mortality in prostate cancer. SES differences explain a large portion of the racial disparity in prostate cancer mortality (Berglund et al., 2012; Taksler et al., 2012).
Studies have suggested that Black men are not receiving optimal treatment for prostate cancer and have also been experiencing delays in treatment (Schwartz et al., 2009; Shavers et al., 2004; Spencer, Fung, Wang, Rubenstein, & Litwin, 2004). Early tumor detection may reduce mortality by increasing the chances of successful curative treatments and decreasing the number of treatment-related complications. Prostate cancer treatments are also influenced by many other factors, some of which have a sound scientific basis, whereas others are based on highly personal opinions of physicians, patient preferences, availability of a broad range of treatment options, and on the type of hospital in which medical practice is conducted (Jayadevappa, Chhatre, Johnson, & Malkowicz, 2011; Pollack, Bekelman, Liao, & Armstrong, 2011; Pollack, Weissman, Bekelman, Liao, & Armstrong, 2012).
The existence of one or more comorbidity may have an impact on mortality. For instance, obesity was reported to be associated with an increased risk of cancer mortality (Calle, Rodriguez, Walker-Thurmond, & Thun, 2003; Rodriguez et al., 2007). However, findings of this association are still debatable (Mordukhovich et al., 2011).
To better understand overall mortality among patients diagnosed with prostate cancer, a comprehensive database is essential to capture potential factors at individual and contextual levels and elucidate their role in mortality among prostate cancer patients. To address this question, this study capitalized on a comprehensive database built from several existing data sets. Its objective was to investigate the relationship of multilevel factors with overall mortality among prostate cancer patients. Thus, the results may lead to long-term quantification of the benefits of current strategies for reducing the disproportionate mortality among minorities and the medically underserved in the United States.
Method
Population Studied
A random sample was taken from the data set. This study focused on Black and White men aged 40 or older, diagnosed with invasive prostate cancer in the state of Florida between the dates of October 1, 2001, and December 31, 2007. Other races were excluded from the study due to small population sizes.
Data Sources
Data for this study were assembled from four different sources. Individual-level prostate cancer incidence data for years 2001 to 2007 were obtained from the Florida Cancer Data System (FCDS) that is managed by the State of Florida Department of Health and operated by the University of Miami. The FCDS is the single largest population-based, cancer incidence registry in the nation.
Prostate cancer cases from FCDS contained information on patient’s demographics, type of health insurance at diagnosis, tumor characteristics, the first course of treatment, vital status, and tobacco use history. The patient residential address was geocoded by an independent geocoding firm contracted by the Florida Department of Health. Diagnosis information of all diseases, including prostate cancer, was obtained from the Florida Agency for Health Care and Administration (AHCA). AHCA data consist of two databases, namely, the Hospital Patient Discharge Data and Ambulatory Surgical Data, on all patient encounters within hospitals and freestanding ambulatory surgical and radiation therapy centers in Florida. Comorbidity was computed following the Elixhauser method based on diagnoses information from the AHCA data classified by the International Classification of Diseases, Ninth Revision (ICD-9) codes. ICD-9-CM diagnosis code 185 was used to identify the prostate cancer patient group. Prostate cancer, the outcome disease, was excluded from the comorbidity groups in this study. Elixhauser Index was used because it has been extensively validated and allows more disease states to be considered as comorbid conditions compared with the Charlson Index (Li, Kim, & Doshi, 2010; Mnatzaganian, Ryan, Norman, & Hiller, 2012; Southern, Quan, & Ghali, 2004; Stukenborg, Wagner, & Connors, 2001). The study used a total of 45 comorbidities, which includes 29 from the Elixhauser Comorbidity list and 16 additional comorbidities. None of the comorbidities in the database used for the analysis had frequency lower than 5. Details on the computation of the comorbidity measures are described in a methodology paper (Xiao et al.,2013).
Data from the U.S. Census Bureau (Census 2000, Summary File-3; U.S. Department of Commerce, U.S. Census Bureau, 2002) public files for the State of Florida were used to extract sociodemographic and farm house presence information at the census-tract level. Health providers to case ratios per 1,000 were computed using county-level information obtained from the Florida Department of Health Division of Medical Quality Assurance. Specifically, the number of urologists and radiation oncologists was divided by the number of prostate cancer cases diagnosed within each county during 2001 to 2007. This measure was used to capture provider availability.
Data obtained from the four sources were merged into a single data set by assigning each census-tract or county-level data to the individual cases located within these geographical units. Cases were excluded from the analyses if they could not be linked to census data or provider information.
Statistical Analysis
Multilevel logistic regression was conducted to assess significance of individual and contextual factors in relation to overall mortality among individuals diagnosed with prostate cancer. The dependent variable was overall mortality, which is simply referred to as mortality in the subsequent sections of this article. Explanatory variables were available at three levels (individual, census tract, and county). Individual-level characteristics included age, race, marital status, tobacco use history, health insurance, comorbidity, treatment type, tumor stage at diagnosis (early and late-stage), tumor grade, year of diagnosis, and medical facility characteristics. Using the primary payer code each case was allocated to one of the following three health insurance types: public, private, and uninsured. If the patient had more than one health insurance type, the first listed payer was used to derive the insurance type. If the primary payer was Medicare, Medicaid, Department of Defense (tricare), military personnel (military), Veteran Affairs, or Indian/Public health service then health insurance type was defined as public health insurance. Private insurance included managed care, health maintenance organization, preferred provider organization, or fee-for-services. If the patient did not have public insurance or private insurance at the time of diagnosis then this person was categorized as uninsured.
The classification of treatment variables was based on three major types of treatment: surgery, radiation, and hormone therapies. Patients who received surgery were classified into four groups: surgery plus radiation, surgery plus radiation plus hormone, surgery plus hormone therapy, and surgery only. Patients who did not receive surgery were grouped based on whether they received radiation and hormone therapy, radiation and no hormone treatment, hormone treatment only, and no definitive treatment (received neither radiation nor hormone treatment). Details on treatment classification are described in another methodology paper (Xiao et al., 2013).Surveillance Epidemiology and End Results (SEER) summary staging was used to classify prostate cancer stages based on FCDS coding. If the patient was diagnosed with localized prostate cancer, tumor stage was labeled as early-stage, whereas if the patient was diagnosed with regional or distant then tumor stage was labeled as late-stage. At the census-tract level, both median household income (expressed in thousands of dollars) and presence of farm house were included. Last, provider availability was considered at the county level as the ratio of urologists and radiation oncologist to prostate cancer cases.
To account for homogeneity within a county or a census tract and heterogeneity between counties or census tracts, county and census tract random intercepts were added to the logistic model. Therefore, if Yijk is the mortality indicator for the kth individual in the jth census tract from the ith county, and pijk = P(Yijk = 1) is the probability that this individual died, the multilevel logistic regression model is written as follows:

In the above model, are the explanatory variables for this person at three levels, β are the regression coefficients, vi is the random intercept accounting for homogeneity within each county, and uij is the random effect to model homogeneity within each census tract. County and census tract random effects were assumed to be independent. The random intercepts vi and uij were assumed to be independent realizations of normal distributions and respectively.
Likelihood ratio tests based on Laplace approximation method were used to assess significance of random intercepts. Odds ratios were calculated for explanatory variables. The statistical analyses were conducted using SAS/STAT® software, Version 9.3, of the SAS System for Windows.
Results
The sample consisted of 18,042 individuals diagnosed with prostate cancer in Florida during October 2001 to December 2007. Their age at diagnosis ranged from 40 to 100 years, with a median of 67 years. The majority of these individuals were White (87.61%), married (78.69%), non–current smoker (83.95%), and had public insurance (59.06%). The majority of these men were diagnosed at early-stage (88.25%) and had a tumor that was well or moderately differentiated (59.26%). In this sample, surgery was the most frequently received treatment (40.91%). Among the patients, 2,363 died (from any cause) during the study period. The study population characteristics are summarized in Table 1.
Characteristics of the Study Population (N = 18,042).
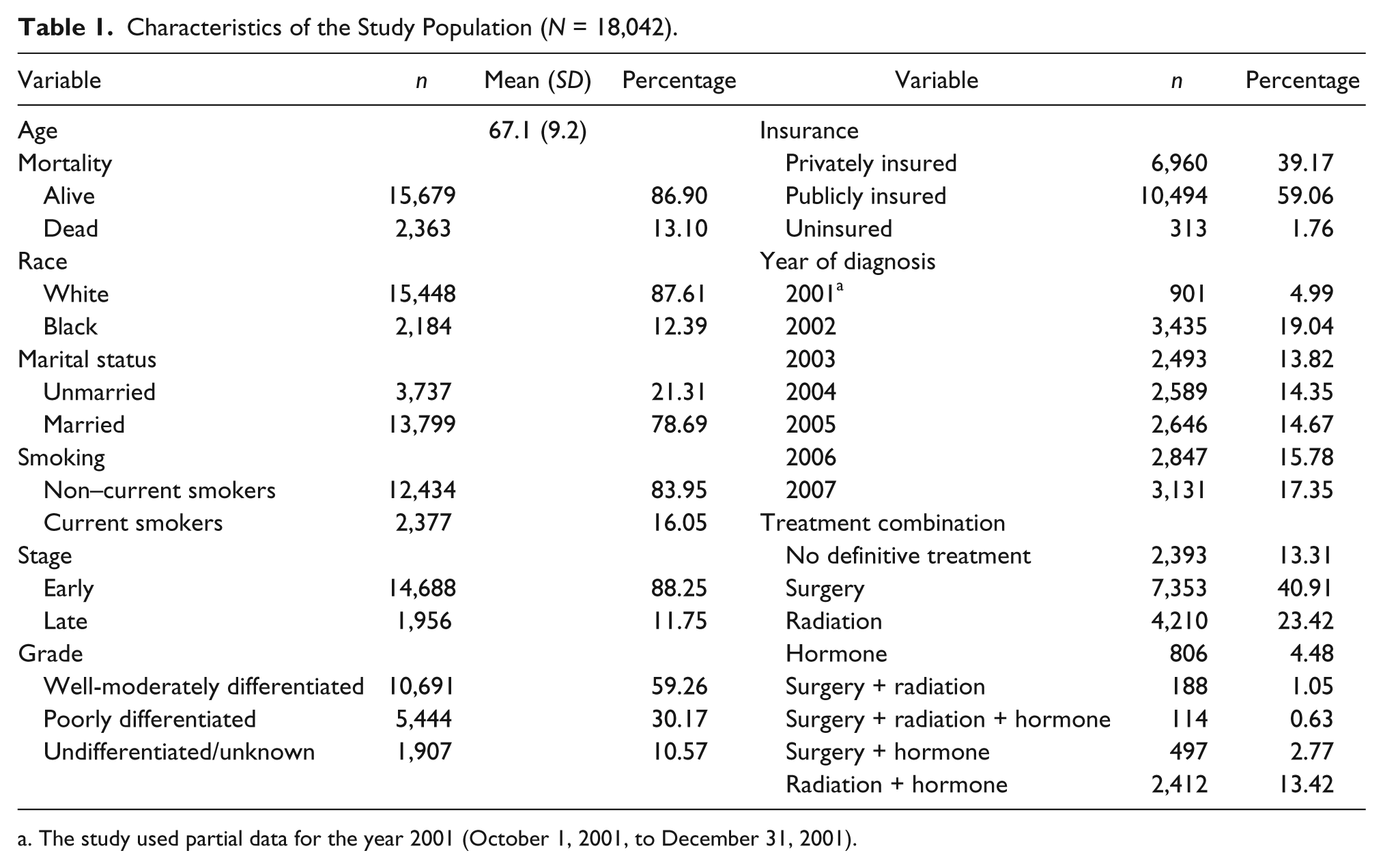
The study used partial data for the year 2001 (October 1, 2001, to December 31, 2001).
According to the joint test of random intercepts (p = .0114) individuals were not independent; hence, a logistic regression with independence assumption would not be suitable. The change in −2 log likelihood between model with only census tract random effects and that with both county and census tract random effects was only 0.11, meaning that the county random effects were not necessary if census tract random effects were already in the model. In addition, the estimate and standard error for the county random effects variance also suggest standard error of county variance estimate (0.01176) was relatively large compared with the variance estimate itself (0.003962). Therefore, only census tract random effects were kept in the final model.
The results of multilevel logistic regression are reported in Table 2. The following individual-level factors were significantly associated with higher odds of mortality: older age, unmarried, current smoker, uninsured, diagnosed at late-stage, having poorly or undifferentiated or unknown tumor grade. Cases diagnosed in more recent years had lower odds of mortality compared with those diagnosed in earlier years. Black men were around 18% more likely to die compared with White individuals, although the p value for this effect was .15. Compared with patients who received surgery only, those receiving no definitive treatment were about twice more likely to die. People who received hormonal therapy or a combination of radiation and hormone therapy had a higher risk of mortality compared with those who received surgery only. Among census-tract factors, living in a tract with lower median household income was associated with higher odds of mortality. There was not enough evidence to support the association between county-level providers-to-case ratio and mortality among patients who were diagnosed with prostate cancer in Florida.
Adjusted Odds Ratios of Major Factors to Overall Mortality Among 11,657 Prostate Cancer Patients, Florida, 2001-2007.

Significant at .01 level.
Significant at .05 level.
Several comorbidities were associated with higher odds of mortality. These included congestive heart failure, paralysis, other neurological disorders, chronic pulmonary disease, diabetes, renal failure, liver disease, metastatic cancer, solid tumor without metastasis, fluid and electrolyte disorders, chronic blood loss anemia, deficiency anemias, alcohol abuse, genitourinary system disease, respiratory disorders, other mental disorders, other anemias, and brain and other neurological disorders. The comorbidities that were not statistically significant according to the multilevel logistic regression are shown in the appendix.
Discussion
This study examined individual and contextual factors contributing to overall mortality among men diagnosed with prostate cancer in Florida during 2001 to 2007. There was no racial difference found in this study. The higher rate of mortality among Blacks might be explained by the difference of stage, treatment, and insurance. Older patients are reported to be more likely to have advanced stage and thus have a greater risk of mortality than younger patients (Bechis, Carroll, & Cooperberg, 2011). For older men, curative treatment is only indicated for selected patients as comorbidities can play a role in treatment decisions (Heinzer & Steuber, 2009; Scosyrev, Messing, Mohile, Golijanin, & Wu, 2012). The association between marital status and mortality benefit appears to be explained by the fact that married men are thought to have more socioeconomic resources, tend to have less risky behaviors, and benefit from social support, all of which contribute to overall better health practice (Du et al., 2012; Dupre, Beck, & Meadows, 2009). Smoking has been identified as the most preventable cause of prostate cancer morbidity and mortality (Giovannucci et al., 1999; Giovannucci, Liu, Platz, Stampfer, & Willett, 2007; Gong, Agalliu, Lin, Stanford, & Kristal, 2008). Studies on prostate cancer have suggested that patients of lower SES and with limited health insurance coverage may have less access to cancer screening services, subsequently leading to late-stage diagnosis, treatment delay, as well as worse mortality outcomes (Robbins, Whittemore, & Thom, 2000). This may explain the higher odds of mortality among uninsured men.
The recent advances in treatments, screening at early-stage, and receipt of prompt treatment may have contributed to lower the odds of prostate cancer mortality among men who are diagnosed early (Attard & de Bono, 2011; Lu-Yao et al., 2009; Xiao, Tan, & Goovaerts, 2011). Observation period used to be longer in past years, resulting in shorter time to treatment for cases diagnosed in later years. Our finding is consistent with a study that found that men undergoing surgery, specifically radical prostatectomy, had a reduced disease-specific mortality when compared with men not receiving treatment (Bill-Axelson et al., 2005). To reemphasize, the no definitive treatment category in our study includes active surveillance or treatment deferral for any reason. With regard to deferred treatment, it was suggested to be a reasonable alternative to immediate treatment, allowing for “watchful waiting” in select patients with early and low-risk prostate cancer (Patel et al., 2004). In contrast, active surveillance, a newer and more systematic approach that is usually indicated in men with early and low-risk prostate cancer (Dall’Era et al., 2012; Godtman, Holmberg, Khatami, Stranne, & Hugosson, 2013), allows for an active plan of monitoring disease status and includes predetermined treatment decision points and benchmarks mutually agreed between the patient and provider. Nevertheless, this newer approach also remains controversial, because it is not clear which patients are truly considered to have low-risk prostate cancer and could definitively benefit from this approach. The odds ratio was higher among patients without active treatments than patients with active treatments. We were not sure that the patients in our study were really under “active surveillance,” or just did not receive any treatment. Further studies are needed to separate patients without any active treatments. Consistent with a published study (Nanda, Chen, Braccioforte, Moran, & D’Amico, 2009), our study demonstrated that a combination of hormonal and radiation therapy for treating prostate cancer was associated with higher odds of mortality in men with moderate to severe comorbidity. These higher odds may be related to older age. Indeed, in our study population the majority of men receiving a combination of hormonal and radiation therapy were 65 years of age and older. Patients receiving combination of radiation and hormonal therapy may have overall poor health condition that does not allow surgical treatment. In a study by Pierorazio and colleagues, most of the men who underwent radical prostatectomy had favorable prostate cancer characteristics and excellent overall health status (Pierorazio, Humphreys, Walsh, Partin, & Han, 2010). Surgical treatment is reserved for patients with localized prostate cancer and who are projected to have a long life expectancy (Aus et al., 2005; Heidenreich et al., 2011; Zincke et al., 1994).
Men who are diagnosed with advanced stage of prostate cancer (Johansson et al., 1997; Jonsson et al., 2006; Taksler et al., 2012) and men with poorly differentiated prostate cancer (Albertsen, Hanley, & Fine, 2005; Schwartz et al., 2009) have a higher odds of mortality. This may be explained by the fact that men with poorly differentiated, undifferentiated, or unknown tumor grades tend to also have a more advanced stage of disease at the time of prostate cancer diagnosis (Enewold et al., 2011; Rapiti et al., 2009).
To disentangle factors associated with overall mortality among patients diagnosed with prostate cancer, area-level information (contextual factors) was included in the model. Patients residing in census tracts with higher median household income had lower odds of mortality. Lower median household income may be associated with limited education and lack of health insurance, which may constitute barriers to health care access (Basler, 2011; Hoffman et al., 2001; Patel et al., 2010).
Of the 45 comorbidities, 19 were significantly associated with higher odds of mortality. This finding is consistent with previous research (Albertsen et al., 2011; Hall, Jani, Ryu, Narayan, & Vijayakumar, 2005) and may have several explanations. First, individuals with comorbidities may not be treated aggressively for prostate cancer based on perceptions about their life expectancy, ability to tolerate therapy, and potential treatment side effects (Bechis et al., 2011; Post, Hansen, Kil, Janssen-Heijnen, & Coebergh, 2002). Second, side effects or complications are likely to cause interruptions in treatment, which may further lead to increased prostate cancer recurrence (Alibhai et al., 2005; D’Ambrosio et al., 2008).
The current study has a number of limitations. First, only cases diagnosed from 2001 through 2007 were analyzed. Thus, the observations made in this analysis may not necessarily reflect the most current trends. Second, mortality obtained from the FCDS database is all-causes mortality instead of prostate cancer–specific mortality. Third, severity data for comorbidities is not available, thus we are not able to suggest how clinicians should consider the presence of these comorbidities in their patients. Fourth, census tract and county-level data on SES were used to compensate for a lack of individual-level information, which would have provided richer information for the analyses. Finally, large databases like the FCDS are not without limitations. Registry data lack information about events and decisions leading up to screening. Follow-up information are often limited to vital status, and there are no detailed information on side effects of treatment or treatment compliance. Current cancer registry data may miss treatments provided by private physician offices. Bias may exist in the collection of information on cancer stage and may affect rates, particularly for unstaged cancers; accuracy of cancer registry data on stage at diagnosis is relatively low compared with other demographic variables. FCDS also fail to include location of treatment and diagnosis in the tumor registry.
Despite these limitations, the study was able to maximize the utility of current information by linking four data sources from different geographical levels and presented a comprehensive picture of patient outcomes. Specifically, patient comorbidity was taken into consideration, which is highly relevant to examining mortality among men diagnosed with prostate cancer.
In conclusion, patient’s demographics, tumor characteristics, comorbidity, and treatment received should be considered when studying clinical outcomes among prostate cancer patients. Thus, our findings direct attention to areas in which mortality outcomes differ by sociodemographic characteristics and certain clinical factors. Although certain factors leading to mortality are not adjustable, others such as screening or education imply that strategies can be developed to improve patient final outcomes. These findings have important implications, especially since the reduction of health disparities is recognized as a priority issue by the National Institutes of Health (National Cancer Institute, 2003), whereas Healthy People 2020 calls for the elimination of health disparities among different groups of residents living in the same community (U.S. Department of Health and Human Services, 2011). Future studies are needed to investigate mortality outcome as well as the specific health-system, sociodemographic, and biologic factors that may be responsible for disparities.
Footnotes
Appendix
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This study was funded by Grant #RSGT-10-082-01-CPHPS from the American Cancer Society. Dr. Goovaerts’ work was partially funded by grant 1R21 ES021570-01A1 from the National Cancer Institute. The views stated in this publication are those of the author and do not necessarily represent the official views of the NCI.