
Abstract
The mortality rate of men is generally higher than that of women, irrespective of the age group. Currently, a key concern for health care professionals is the prevalence of risk factors associated with cardiovascular disease and metabolic syndrome. This study aimed at assessing the prevalence of individual risk factors for cardiovascular disease as well as the prevalence of metabolic syndrome among men serving in the Military Police Corps of the state of Bahia, Brazil. This service employs mostly men, and they are known to experience high levels of occupational stress and professional victimization. We conducted a cross-sectional study among military police soldiers (n = 452) who were candidates for a military police training course in Bahia, Brazil. All candidates who attended the selection process were evaluated according to the criteria of the National Cholesterol Education Program’s Adult Panel III in order to assess the presence of medical disorders that could contribute to cardiovascular disease and metabolic syndrome. The authors identified a high prevalence of hypertension (55.76%), hypertriglyceridemia (50.85%), waist circumference of >102 cm (31.76%), low high-density lipoprotein cholesterol levels (30.46%), and impaired fasting glucose (28.15%) in our subjects. The overall prevalence of metabolic syndrome was 38.54%. The authors suggest that measures should be taken to ensure that military policemen receive continued medical care, both in their professional capacity and in their personal circumstances, and that attention be focused on intervention programs.
The life expectancy of men is nearly 8 years less than that of women, and social factors are known to contribute to the morbidity and mortality rates of men. Men in almost all age groups have higher mortality rates from non-sex-specific diseases than women (Chagas, Zilli, Ferreira, Moretti, & Ramos, 2009). The differences in the rates of morbidity and mortality between men and women may well be explained by genetic and hormonal factors, lifestyle, and habits (alcohol, smoking, working conditions), but they could also be a consequence of the way in which men are raised and the way in which gender roles are assigned in different societies. Therefore, in the process of acquiring a masculine role, men adopt behaviors that subjectively, but ostensibly, renounce that they are childish, homosexual, or feminine. In an effort to renounce these features, behaviors that are associated with sensitivity and tenderness are suppressed. This includes the denial of pain. Men would reduce their self-preservation in an effort to affirm the role of a strong provider and leader (Braz, 2005). The prevalence of cardiovascular diseases has been one of the key concerns for health professionals and organizations worldwide. Some of the World Health Organization (WHO) projections forecast a 250% increase in morbidity and mortality events due to cardiovascular diseases in the Brazilian population. Intervention programs that could reduce cardiovascular risk factors among Brazilians are thus urgently needed (Chagas et al., 2009). Metabolic syndrome (MS) encompass a group of cardiovascular risk factors such as dyslipidemia (including increased triglycerides and reduced high-density lipoprotein [HDL] cholesterol levels), abnormal glucose metabolism (elevated fasting glucose), hypertension, and central obesity (characterized primarily by an increased waist circumference). All of these clinical conditions are superimposed on insulin resistance (usually manifested as hyperinsulinemia and altered glucose metabolism, with metabolic consequences; (Rosenbaum & Ferreira, 2003). A population-based study, conducted in a capital city in northeast Brazil, randomly sampled 1,663 individuals aged between 25 and 64 years and found the prevalence of MS in this population to be 29.8%. The prevalence of MS in men and women were similar, but it progressively increased with age. Parameters of MS most frequently seen in men were (in order of highest to lowest prevalence) hypertension, hypertriglyceridemia, low HDL-cholesterol, abdominal obesity, and hyperglycemia, whereas parameters of MS in women were hypertension, low HDL-cholesterol, abdominal obesity, hypertriglyceridemia, and hyperglycemia (Salaroli, Barbosa, Mill, & Molina, 2007).
The Military Police Service is generally considered a dangerous profession with members experiencing high levels of occupational stress and professional victimization. The Brazilian Police Services mostly employ men, and the results of a study that investigated the health status of military policemen may well—at least partly—be extrapolated to men in general. To our knowledge, the prevalence of MS among military police officers in Brazil has not yet been investigated even though there have been studies that considered specific cardiovascular risk factors such as obesity and physical inactivity. A study that enrolled 1,110 military policemen from the city of Rio de Janeiro, Brazil, showed that among those most were men (96.3%) aged 31 to 40 years (43.1%). Most of the men were married (75.4%), and 48.2% were of mixed race. Seven percent of these men (n = 35, 95% confidence interval = 32.9% to 38.6%) experienced psychological distress, as indicated by the Self-Report Questionnaire for the detection of psychological distress and minor psychiatric disorders. The authors of the study concluded that men’s dissatisfaction with their ability to react to difficult situations, which frequently occur in the execution of police activities, and their dissatisfaction with life in general, were better indicators of psychological distress than the men’s sociodemographic circumstances (Salaroli et al., 2007; Souza, Minayo, Silva, & Pires, 2012). Similar to other service sectors, the public security sector in Brazil, has, for a long period of time, been excluded from economic studies. In addition, when Brazil was governed by dictators, the public and intellectuals’ opinions were mobilized against this professional segment. The public security sector was included in the social reconstruction process for democratic change in the 1990s, and scholars and scientists who study occupational health conditions have only recently turned their focus on public security professionals (Souza & Minayo, 2005). Therefore, because of the current lack of knowledge regarding factors that affect men’s health in general, or the health of men serving in the military police, studies that would improve understanding of the risk factors of morbidity and mortality from cardiovascular causes in this population are necessary. This study was part of a doctoral thesis that focused on the health of men, and the main objective of the study was to improve knowledge and understanding of the living conditions and the risks of morbidity and mortality from cardiovascular causes in military policemen in Bahia, Brazil.
Material and Method
This was a cross-sectional study with qualitative as well as quantitative components. The aim of the qualitative part of the study was to improve understanding of how the subjects, enrolled in the study, live and how they experience a range of conditions related to health and disease. The quantitative part of the study included sociodemographic and anthropometric data, blood pressure, clinical and laboratory data, as well as information related to the criteria for a diagnosis of MS. The study population included military police soldiers of the State of Bahia, Brazil. Two groups of soldiers were enrolled (n = 452): the first group (n = 256) convened in January 2012 and the second group (n = 196) in March 2012, and selected to attend a training course designed for military police corporals. This course is a prerequisite for promotion to a higher rank, and the men underwent expert medical evaluation and physical fitness tests as part of the selection process. The two groups were formed by the only criterion of admission date (date of joining the Corporation), and the vacancies rigorously filled by the older, forming the variable to be analyzed later as working time.
During the selection process, the policemen appeared in front of the medical board with their test results, including the results for fasting glucose, total and HDL-cholesterol, and triglyceride fractions. Anthropometric data (weight, height, body mass index, waist circumference) and blood pressure measurements as well as information about the presence of previously diagnosed diseases and treatment were also presented, if available. Results from the physical examination and the laboratory test were presented to the panel for verification. These results were also used to assess a possible diagnosis of MS, according to the criteria of the National Cholesterol Education Program’s Adult Panel III (NCEP-ATP III). NCEP-ATP III criteria for a diagnosis of MS in men are as follows: a systolic blood pressure of ≥130 mmHg and/or a diastolic blood pressure of ≥85 mmHg, triglycerides ≥150 mg/dL, fasting glucose ≥100 mg/dL, HDL-cholesterol <40 mg/dL, waist circumference >102 cm (Grundy, Brewer, Cleeman, Smith, & Lenfant, 2004). The NCEP-ATP III criteria were used, without any mention to race, because miscegenation is a fundamental characteristic of the Brazilian population’s ethnicity; the National Survey by Sample of Households, conducted in 2009 by the Brazilian Institute of Geography and Statistics, showed that when questioned about race, 44.2% of the respondents declared themselves “brown,” a term that usually means the result of a union between a Black person and another of a different skin color. In such a situation, most scientists state that in the case of Brazil, talking about race sounds like something vague, subjective, and therefore devoid of scientific value. SPSS version 17 software was used for the analysis of sociodemographic, anthropometric, clinical, and laboratory data as well as descriptive analysis, focusing measures of frequency, central tendency, and dispersion. The study was approved by the Ethics Committee of Complexo Universitário Professor Edgard Santos, Federal University of Bahia, and was conducted in accordance with the principles of Ethics in Research with Humans and the Declaration of Helsinki.
Results
Four hundred and fifty-two subjects were enrolled, with the mean age being 45 years. Subjects were divided into two subgroups, using the mean age as a cutoff value: subjects aged <45 years (n = 234) were assigned to the “younger group,” and subjects aged ≥45 years (n = 217) were assigned to the “older group.” Details of sociodemographic data and previously diagnosed medical conditions are reported in Table 1.
Sociodemographic Data and Previously Diagnosed Medical Conditions.

Sociodemographic data identified that 68.61% of the subjects were married, and the majority of them (86.41%) had a high school diploma. The prevalence rate among the older and younger groups for the presence of medical history of conditions considered as cardiovascular risk factors (hypertension, diabetes mellitus, dyslipidemia) and coronary atherosclerosis itself identifies a greater involvement related to older age, according to data from the medical literature (Chagas et al., 2009; D’Agostino et al., 2008).
The frequencies of physical and laboratory data relevant for a diagnosis of MS are reported in Table 2.
Results of the Physical Examination and Laboratory Tests.

Note. BMI = body mass index; BP = blood pressure; HDL = high-density lipoprotein; LDL = low-density lipoprotein; VLDL = very low-density lipoprotein.
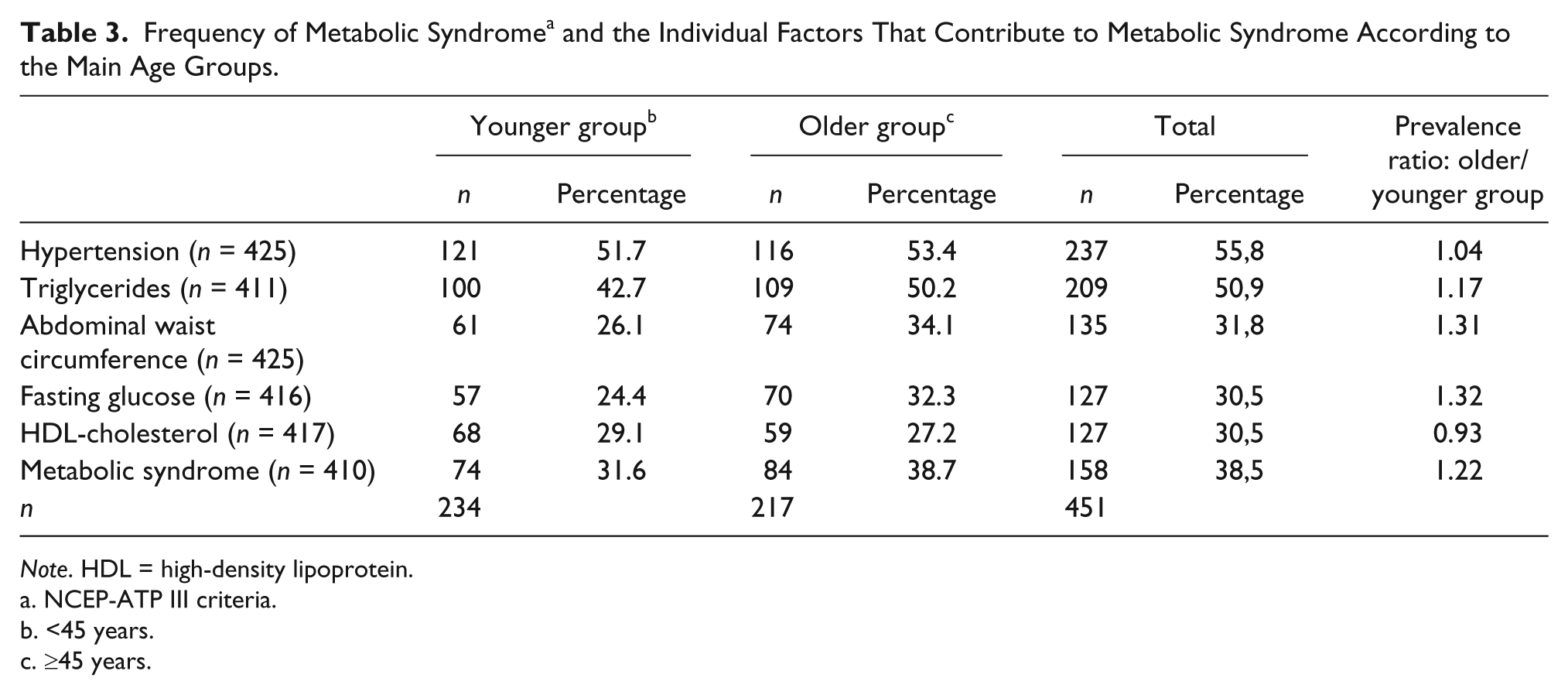
On the basis of the mean BMI—27.85 kg/m2—the majority of subjects could be considered overweight or obese; 72.64% of the subjects had a BMI ≥25 kg/m2. The mean abdominal circumference of the subjects was 97.12 cm, considerably greater than the normal value for men—<94 cm. According to the WHO, values of abdominal circumference in men >94 cm are considered to be at increased cardiovascular risk, and values ≥102 cm are considered to be at substantially increased risk for cardiovascular diseases (Patry-Parisien, Shields, & Bryan, 2012). The mean fasting glucose of subjects—99.70 mg/dL—was almost equal to the cutoff value for impaired fasting glucose (≥100 mg/dL), as described by the International Diabetes Federation (IDF), whereas the mean level of triglycerides was higher than the cutoff value considered by the NCEP-ATP III as a risk factor for MS (≥150 mg/dL). Low levels of HDL-cholesterol (<40 mg/dL), another cardiovascular risk factor, usually associated with irregular physical activity or a sedentary lifestyle was present in 30.46% of the subjects (Hardman, 1999; Mahanonda et al., 2000). The assessment of the frequency of MS components, individually or grouped, is reported in Table 3.
Frequency of Metabolic Syndrome a and the Individual Factors That Contribute to Metabolic Syndrome According to the Main Age Groups.
Note. HDL = high-density lipoprotein.
NCEP-ATP III criteria.
<45 years.
≥45 years.
As reported, the authors identified a high prevalence of hypertension (55.76%), elevated levels of triglycerides (50.85%), abdominal waist circumference >102 cm (31.76%), abnormalities in fasting glucose (30.53%), and low levels of HDL-cholesterol (30.46%). Thus, according to NCEP-ATP III criteria, an overall prevalence of 38.54% of MS was identified among the subjects.
Discussion
The majority of the subjects (72.64%) had a BMI greater than 25 kg/m2; thus, they could be considered overweight or obese. This is troubling, since policemen are expected to be in good shape and to be able to perform with physical strength and agility in their daily professional activities. A population-based study conducted in a city in southeastern Brazil found that 43.3% of men enrolled in the Family Health Program were overweight/obese, 28% participated in irregular physical activity/inactivity, 25.3% smoked, and 24% were hypertensive (Khanna et al., 2013; Van Eyken & Moraes, 2009). The mean abdominal circumference of the subjects was 97.12 cm; 33.9% of the subjects had values of abdominal circumference ≥94 cm but ≤102 cm (considered of increased cardiovascular risk, according to the WHO), and 29.9% had values above 102 cm (substantially increased risk of cardiovascular diseases, according to the same criteria). As a whole, 63.8% of the subjects presented values of abdominal circumference above the normal. The WHO states that both the abnormal mean BMI and mean abdominal circumference are associated with an increased risk for cardiovascular diseases (Patry-Parisien et al., 2012). A population-based study conducted in a city in southern Brazil showed that a BMI of >25 kg/m2, which is considered overweight, and a waist circumference of >102 cm increases risk of hypertension by 1.66 and 1.48 times, respectively (Ulbrich et al., 2012). The mean fasting glucose of our subjects—99.70 mg/dL—was almost equal to the cutoff value for impaired fasting glucose (≥100 mg/dL), as described by the International Diabetes Federation (IDF), whereas the mean level of triglycerides—187.14 mg/dL—was higher than the cutoff value considered by the NCEP-ATP III as a risk factor for MS (≥150 mg/dL). Furthermore, it is known that high alcohol intake is associated with elevated levels of serum triglycerides, cardiovascular disease, fatty liver disease, and acute pancreatitis of alcoholic etiology (Klop, Rego, & Cabezas, 2013); alcohol intake per se was not addressed in this study. In the present study, 72.64% of subjects were overweight/obese. The authors identified a high prevalence of hypertension (55.76%), elevated levels of triglycerides (50.85%), abdominal waist circumference >102 cm (31.76%), abnormalities in fasting glucose (30.53%), and low levels of HDL-cholesterol (30.46%). Thus, according to the NCEP-ATP III criteria, the authors report an overall prevalence of 38.54% of MS among the subjects.
In a study conducted in Doha, Qatar, 69.4% of patients (n = 467) who were hospitalized due to acute coronary syndrome met the criteria for a diagnosis of diabetes mellitus. The following factors associated with MS were prevalent in those patients: reduced HDL cholesterol (94.1%), impaired fasting glucose (89.8%), elevated triglycerides (81.8%), increased waist circumference (61.7%), and hypertension (40.4%; Al-Aqeedi et al., 2013). A study conducted in India among 900 police officers between 26 and 58 years of age, using the NCEP-ATP III criteria, found that 41.4% of subjects had hypertension, 75.2% had triglyceride levels of >150 mg/dL or HDL-cholesterol levels of <40 mg/dL, 13.7% had abnormalities in fasting glucose, and 16.8% were diagnosed with MS. Among subjects with MS, 86.2% had hypertension, 82.6% had hypertriglyceridemia, 71% had an increased abdominal waist circumference, 41.3% had reduced HDL-cholesterol levels, and 38.4% had abnormalities in fasting glucose levels (Thayyil, Jayakrishnan, Raja, & Cherumanalil, 2012). A systematic review of articles, whose subjects were apparently healthy, of both genders aged 18 to 65 years concluded that the overall prevalence of MS in Latin America was 24.9% (range 18.8% to 43.3%; Marquez-Sandoval et al., 2011; Salaroli et al., 2007). In a cross-sectional study involving 1,383 men assigned to military organizations of the Brazilian Navy in the City of Natal, Rio Grande do Norte State, aged 18 to 62 years, a MS prevalence of 17.6% was reported; the most prevalent risk factors were low HDL-cholesterol and abdominal obesity (Costa, Montenegro, Lopes, & Costa, 2011; Salaroli et al., 2007). The overall prevalence of MS found in our subjects—38.54%—can be considered significantly higher than those found among police officers in India—16.8% (Thayyil et al., 2012), 24.9% in Latin America (Costa et al., 2011; Marquez-Sandoval et al., 2011), 25% in the United States (McCullough, 2011), and 29.8% in a population-based study in Vitória, Espírito Santo State, southeastern Brazil (Costa et al., 2011; Marquez-Sandoval et al., 2011; Salaroli et al., 2007).
Final Considerations
Male gender is considered a risk factor for morbidity and mortality in all age groups and from all non-sex-specific diseases. The Brazilian Military Police Service mainly employs men, and the data from studies that investigate the health of military police officers can be—at least partially—extrapolated to men in general. Unhealthy lifestyles lead to an increase in the prevalence of chronic diseases such as diabetes mellitus, hypertension, obesity, and dyslipidemia, which are important risk factors for illness and death from cardiovascular causes. MS comprises a group of cardiovascular risk factors, and their prevalence should be studied, especially in vulnerable populations such as military police officers, who are often exposed to occupational stress and professional victimization (Minayo, Hartz, & Buss, 2000; Minayo, Souza, & Constantino, 2007). The authors identified a high prevalence of hypertension (55.76%), hypertriglyceridemia (50.85%), waist circumference of >102 cm (31.76%), high frequency of abnormalities in fasting glucose (30.53%), and low levels of HDL-cholesterol (30.46%) in our group of subjects. Thus, according to the NCEP-ATP III criteria, an overall MS prevalence of 38.54% among the subjects is reported. These findings clearly show that police officers experience an increased risk for cardiovascular disease, and it generates concern for the true prevalence of cardiovascular risk factors among men in general. As a relatively small group of officers was enrolled, it may not be appropriate to extrapolate these findings to the general population. This is the main limitation of this study. Nevertheless, considering that the subjects were selected by the human resource administration sector and that selection was based on time of employment in the Military Police Service only (94.8% of subjects had 20-25 years of service), it is likely that these individuals comprise a generation of men who are about to complete 30 years of service in the public safety sector in a profession known for high levels of stress and risks. The authors propose that military police officers receive special medical attention to ensure that all their health requirements are met and that attention is given to intervention programs to reduce or limit the risks of cardiovascular disease in men.
Footnotes
Acknowledgements
We thank Editage for their professional service in translating and editing our article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.