
Abstract
Diminished exercise capacity is a fundamental symptom of heart failure (HF), which is particularly disadvantageous for men for whom exercise capacity contributes significantly to their gender identity, self-esteem, and quality of life. In this study, we aimed to examine whether psychological gender would be different in men with systolic HF as compared with their healthy peers. The authors examined 48 men with systolic HF (age = 64 ± 10 years; body mass index = 28.3 ± 3.4 kg/m2; NYHA I/II/III [%] = 25/65/10; left ventricular ejection fraction [LVEF] = 32.1 ± 7.8%) and 15 age-matched healthy men. Based on the results of the Polish version of the Bem Sex Role Inventory, the examined men were divided into four types of psychological gender: “masculine” (M), “feminine” (F), “unspecified” (U), and “androgynous” (A). None of the men with HF presented M type of psychological gender, whereas this type was found in 27% of the healthy men (p = .0002). The prevalence of both A (38% vs. 47%) and F (10% vs. 20%, both p > .05) types of psychological gender was similar between men with HF versus without HF. More men with HF fulfilled the criteria of the U type of psychological gender as compared with healthy peers (51% vs. 7%, p = .002). Men with HF and the F type of psychological gender were treated with spironolactone more frequently than those classified with the U and A types (both p < .05). The lack of “psychologically masculine” and the overrepresentation of “psychologically unspecified” gender types in the HF group suggests that psychological gender may be affected among men with HF.
Introduction
It has been well established that various chronic diseases (diabetes, chronic kidney disease, chronic obstructive pulmonary disease, asthma), and especially chronic terminal diseases (e.g., cancer) are a significant psychological burden for patients (Burke, Lowrance, & Perczek, 2003; Furgał, Nowobilski, de Barbaro, Polczyk, & Szczeklik, 2011; Laudański, Nowak, & Wańkowicz, 2010; McClellan et al., 2010; Ng et al., 2007; Sheard & Maguire, 1999; Slean, Jacobs, Lahiff, Fisher, & Fernandez, 2012; Zabora, Brintzenhofeszoc, Curbow, Hooker, & Piantadosi, 2001). This observation applies to cardiovascular diseases (Pelle et al., 2010). Heart failure (HF) is a cardiovascular disease known as the main cause of mortality in developing countries (McMurray, & Stewart, 2000), which is both chronic and terminal. Currently, 5.1 million Americans suffer from HF. It is estimated that the prevalence of HF in 2030 will be increased by 25% in relation to the current estimates (Go et al., 2013).
There is evidence that HF is accompanied by social withdrawal (Friedmann et al., 2006), depression, anxiety, reduced quality of life (Gutzwiller et al., 2013; Shalaby, Brumberg, El-Saed, & Saba, 2012; Yohannes, Willgoss, Baldwin, & Connolly, 2010), and general psychological burden (Pelle et al., 2010), similar to other chronic and terminal diseases. However, studies on psychological aspects of HF are mostly limited to the assessment of three problems mentioned above: depressive symptoms, anxiety, and/or quality of life. Studies on psychological aspects concerning patients with HF are relatively exhaustible as compared with evidence regarding psychological aspects of other cardiovascular diseases (Batlis & Small, 1982; Courtenay, 2000; Helgeson, 1990, 1991, 1995; Helgeson & Taylor, 1993; Radley, Grovea, Wrightb, & Thurstonc, 2000) or to studies related to psychological aspects of chronic diseases in general (e.g., Ridder, Geenen, Kuijer, & van Middendorp, 2008).
Psychological gender is a system of psychological characteristics associated with the sociocultural definitions of femininity and masculinity, which may exist in accordance with the biological sex (Udry, 1994). The range of attributes and behaviors associated with being a man or a woman refers to gender roles in everyday life (also in the context of work and/or competence; Thompson, Glenn, & Vertein, 2011), as well as in common beliefs about the uniqueness of each gender. In other words, the psychological gender defines psychological experience of being a man or a woman related to the awareness of belonging to a particular gender (Bem, 1974).
The change of the psychological gender as a consequence of health condition changes is clear and visible in the context of illnesses that are directly related to the biologically understood gender, such as chronic prostatitis (Ku, Jeon, Kim, Lee, & Park, 2002). It has been shown that such relationships occur between the psychological gender and health behaviors (Christy, Mosher, & Rawl, 2013; Levant, & Wimer, 2013): more masculine men are characterized by a greater tendency to perform health behavior, which lead them to a faster recovery after myocardial infarction (Batlis & Small, 1982; Radley et al., 2000). Moreover, people with androgynous (i.e., mixed feminine and masculine) type of psychological gender rate themselves as healthier than people with other types of psychological gender (Batlis & Small, 1982; Gale-Ross, Baird, & Towson, 2009).
There is evidence showing that the psychological gender may be important in the context of cardiovascular diseases (Helgeson, 1990; Radley et al., 2000). For example, psychological gender appears as a stronger predictor of the severity of myocardial infarction as compared with “Type A personality behavior” or as more accurate a predictor of the general health condition in comparison with the biological sex (Helgeson, 1990; Radley et al., 2000). Helgeson reported that masculinity characterizes poor health outcomes, more severe myocardial infarction, and more severe chest pain (Helgeson, 1990, 1991, 1995; Helgeson & Taylor, 1995). Other studies report that high femininity predicts better outcome among men after myocardial infarction (Barrett-Connor, 2007, Helgeson, 1991; Hunt, Lewars, Emslie, & Batty, 2007).
Interestingly, the problem of psychological gender has not been studied in the field of HF. It is surprising because the main symptom of this chronic and terminal disease is diminished exercise capacity leading to a number of everyday-life limitations (Jankowska & Ponikowski, 2010; Pihl, Fridlund, & Mårtensson, 2011). Physical weakness is particularly disadvantageous for many male patients, because the general fitness based on exercise capacity and physical strength contributes significantly to masculine gender identity, self-esteem, and quality of life (Blashill, 2011; Bosworth et al., 2004; Jankowska et al., 2008; Spence, 1984). After a diagnosis of HF, men often have to change their lifestyle significantly (for instance, they have to quit their job, because they are not allowed to make any physical effort). As a result they cannot take on the role of the so-called “head of the family,” responsible for the financial support (Oliffe & Han, 2013; Oliffe, Han, Ogrodniczuk, Phillips, & Roy, 2011). It is known that losing a job elicits serious psychological burden in men, even leading to depression and/or suicide (Mäki & Martikainen, 2012; Oliffe & Han, 2013).
In the view of all the information above, it may be hypothesized that men with HF and age-matched men without HF may have different experiences of their psychological gender. The authors investigated these differences using the Bem Sex Role Inventory.
Method
Participants
The study was carried out at the Department of Cardiology of the 4th Military Hospital in Wroclaw in Poland. Patients with HF were recruited from those visiting the outpatient cardiac clinic. The control group consisted of randomly selected healthy volunteers.
The criteria for study inclusion for the group of men with HF were age between 40 and 80, a documented history of HF of ≥7 months, left ventricular ejection fraction (LVEF) ≤45% as assessed by echocardiography (performed at the time of screening using Simpson’s planimetric method to determine LVEF), clinical stability, and unchanged medications for ≥1 month preceding the study. The exclusion criteria included acute coronary syndrome, coronary revascularization, or any major surgery within the 3 months preceding the study; unplanned hospitalization because of HF deterioration or any other cardiovascular reason within 1 month preceding the study. The criteria for study inclusion for the group of men without HF were age between 40 and 80 and no history of any acute or chronic illness.
The study protocol was approved by the local ethics committee and all subjects gave written informed consent. The study was conducted in accordance with the Declaration of Helsinki.
Materials and Procedure
In all patients, venous blood samples were taken the morning following an overnight fast. Each patient underwent a physical examination with routine laboratory tests and standard transthoracic echocardiography. The following hematinics were measured using an automatic system ADVIA 120 (Siemens, Healthcare Diagnostics, Deerfield, IL): Hemoglobin concentration (g/dL) was measured using an automatic system ADVIA 120 (Siemens, Healthcare Diagnostics, Deerfield, IL).
Plasma concentration of N-terminal pro-type B natriuretic peptide (NT-proBNP, pg/mL) was measured using immunoassay based on electrochemiluminescence on the Elecsys 1010/2010 System (Roche Diagnostics GmbH; Middle, 2005). Serum concentration of sodium (Na, mmol/L) and high-sensitivity C-reactive protein (hs-C-reactive protein, mg/L) were assessed using standard methods (Rifai, Tracy, & Ridker, 1999).
Renal function was assessed using the estimated glomerular filtration rate (mL/min/1.73m2), calculated from the Modification of Diet in Renal Disease equation (Levey et al., 1999). Afterwards, each patient completed psychological questionnaires.
Assessment of exercise capacity was conducted using the spiroergometric test based on RAMP protocol (1.35 MET/min), which consisted of a maximum of 10 three-minute stages (treadmill grade and speed increases in every stage) and using continuous measurement of gas exchange parameters (Ultima System, Medgraphics, St. Paul, MN), which allowed determination of peak oxygen consumption (mL/kg/min; Frankenstein et al., 2007; Jankowska et al., 2003).
Psychological gender was evaluated using the Polish version of the Bem Sex Role Inventory (BSRI)—adapted by Kuczyńska (Kuczyńska, 1992a). The BSRI is a measure of masculinity–femininity and gender roles. The BSRI consists of a list of 35 adjectives. Fifteen are related to female characteristics (femininity subscale) and another 15 to male characteristics (masculinity subscale). The remaining five adjectives are related to neutral features. The subjects expressed which of those adjectives were consistent with their individual psychological identification with the particular gender using a 5-point scale, where 1 means the subject does not identify with the particular feature at all and 5 means that he identifies with the particular feature completely (Bem, 1974). Although the adaptation of the Polish version does not include the normalization process, the accuracy factors are 0.78 for the femininity subscale and 0.79 for the masculinity subscale, and the tool has a satisfactory theoretical validity (Kuczyńska, 1992a).
The final gender assignment was based on taking the sum of points collected in masculinity and femininity subscales and comparing these results with medians of the normalization group (consisting of young, healthy women and men). This enabled us to state whether the subjects’ results in masculinity were high or low. Low result meant ≤ 51 points in the femininity subscale, and ≤ 48 points in masculinity subscale. High result meant ≥ 52 points in femininity subscale and ≥ 49 points in masculinity subscale. Then, it was possible to assign each subject to one of four types of psychological gender: U, unspecified (U, low results in both subscales), androgynous (A, high results in both subscales), masculine (M, low results in femininity subscale, high results in masculinity subscale) or feminine (F, high results in femininity subscale) and low results in masculinity subscale; Grygorczuk, 2008; Kuczyńska, 1992b).
Due to equivocal relations between the psychological gender and age (Erdwins, Tyer, & Mellinger, 1983; Puglisi, 1983; Shimonaka, Nakazato, Kawaai, & Sato, 1997), the authors compared the psychological gender of men in the following age groups—40 to 60 years old and 61 to 80 years old—and analyzed the potential relationship between age and scores on BSRI subscales.
Statistical Analysis
Normally distributed continuous variables were shown as mean values ± standard deviations. Continuous variables with a skewed distribution are shown as median values with upper and lower quartiles (were log transformed in order to normalize their distribution) and categorical variables as absolute numbers and percentages.
Differences between normally distributed continuous variables were tested using the Student t test for unpaired samples, continuous variables with a skewed distribution using the Mann–Whitney U test, and categorical variables using the χ2 test. Relationships between analyzed variables were assessed using Pearson’s correlation coefficients (for normally distributed continuous variables) or Spearman’s rank correlation coefficients (for variables with a skewed distribution or categorical variables).
The statistical analysis was performed using the STATISTICA 9.1 software (StatSoft, Inc). A p value <.05 was considered statistically significant.
Results
The baseline clinical characteristics of the 63 recruited patients (48 with HF) are shown in Table 1. Men with HF had higher concentration of biomarker reflecting the severity of HF: NT-proBNP as well as echocardiography parameters reflecting impaired systolic function (i.e., lower LVEF; both p < .001). As expected, men with HF were characterized by reduced exercise capacity (interpreted as lower peak oxygen consumption, indicating maximum capacity of an individual’s body to transport and use oxygen during incremental exercise) as compared with the healthy men (p < .001). Men with HF had significantly lower scores in the masculinity subscale compared with the healthy subjects (p = .02, Figure 1), whereas the feminine subscale scores for both groups were the same (p = .3; Figure 1).
Clinical and Laboratory Parameters and the Treatment Applied in Men With and Without HF.

Note. Results are presented as mean ± standard deviation, median of the lower and upper quartiles, or as a percentage. HF = heart failure; BMI = body mass index; LVEF = left ventricular ejection fraction; LVEDD = left ventricular end diastolic diameter; NTpro-BNP = N-terminal brain natriuretic propeptide; NYHA = New York Heart Association; NT = hypertension; DM = diabetes; eGFR-MDRD = estimated glomerular filtration rate calculated using the MDRD formula; MDRD = Modification of Diet in Renal Disease; hsCRP = C-reactive protein; ACEI = angiotensin-converting-enzyme inhibitors; ARB = angiotensin receptor antagonist.
p < .05. **p < .001.
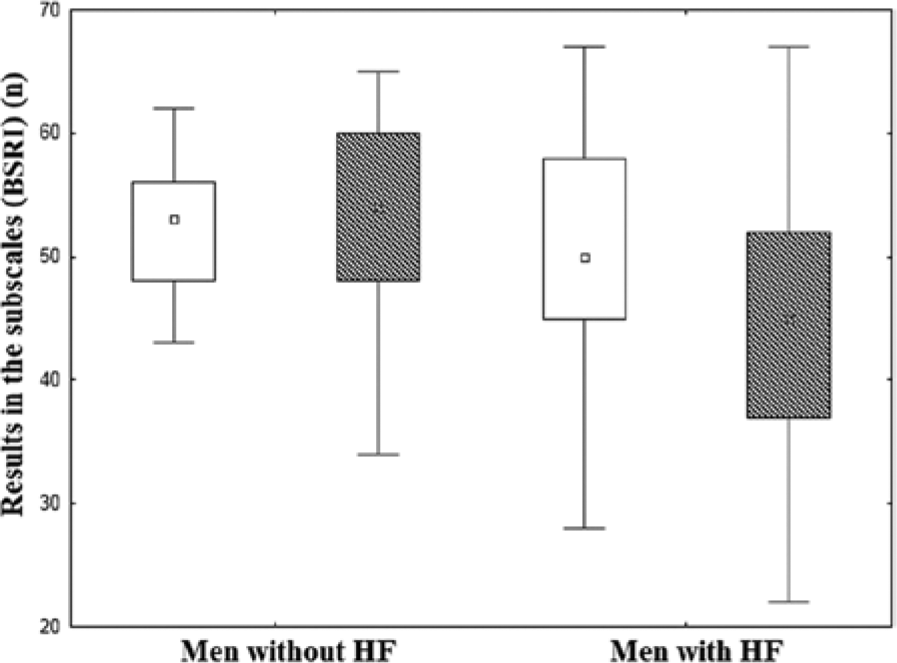
Comparison of the results of the masculinity and femininity subscale (BSRI) in men with and without heart failure (HF) (accordingly, p = .015; p = .49).
The control group included in the present study did not differ from the other group of 86 healthy men from Poland (age between 20 and 30) described in the available literature in terms of the distribution of psychological gender types (all p > .05; Lelakowska & Zdrojewicz, 2008).
None of the men with HF presented the M type of psychological gender, whereas 27% (n = 4) of healthy men demonstrated the M type of psychological gender (p = .0002). The incidence of men with the U type of psychological gender was significantly higher in men with HF as compared with the control group (n = 25, 52%, vs. n = 1, 7%, p = .002; Figure 2). There were no differences regarding the distribution of the A and F types of psychological gender (Figure 2; p > .05).

Types of psychological gender distribution in men with and without heart failure (HF).
Patients with HF and the F type of psychological gender were treated with nonselective aldosterone antagonists (spironolactone) more often than patients with the U and A types (both p < .05; Table 2, Figure 3).
Applied Treatment in Men With HF Divided Into Types of Psychological Gender.

Note. Results are presented as mean ± standard deviation, median of the lower and upper quartiles, or as a percentage. ACEI = angiotensin-converting-enzyme inhibitor; ARBs = angiotensin receptor antagonists.
p < .05 concerns the comparison between the frequency of use of spironolactone feminine type to others type and the other two types of psychological gender. There were no other differences between the compared groups.
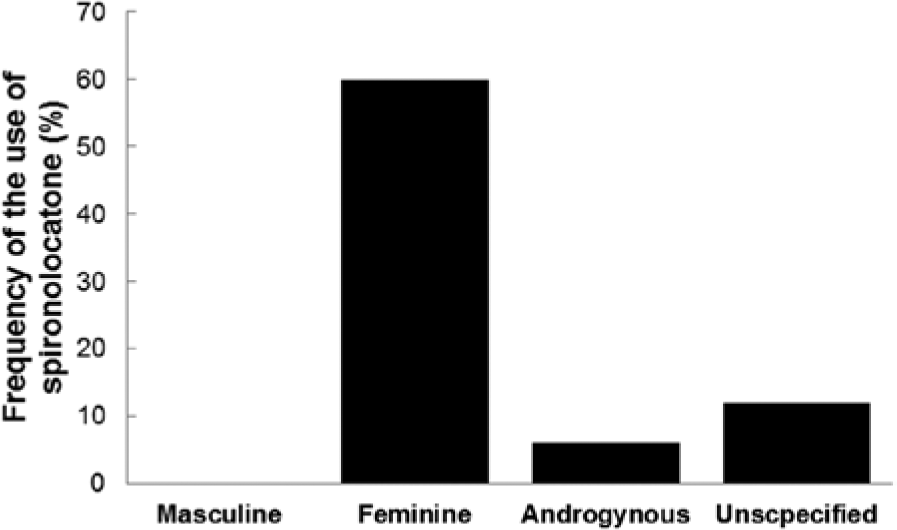
Frequency of the use of spironolactone in men with heart failure (HF) with three types of psychological gender.
There were no differences concerning the prevalence of all types of the psychological gender between the two subgroups divided according to the age (Table 3). There were also no relations between age and scores in feminine and masculinity subscale of BSRI (all p > .8).
Psychological Gender of Men in the Age Groups: 40 to 60 Years Old and 61 to 80 Years Old.
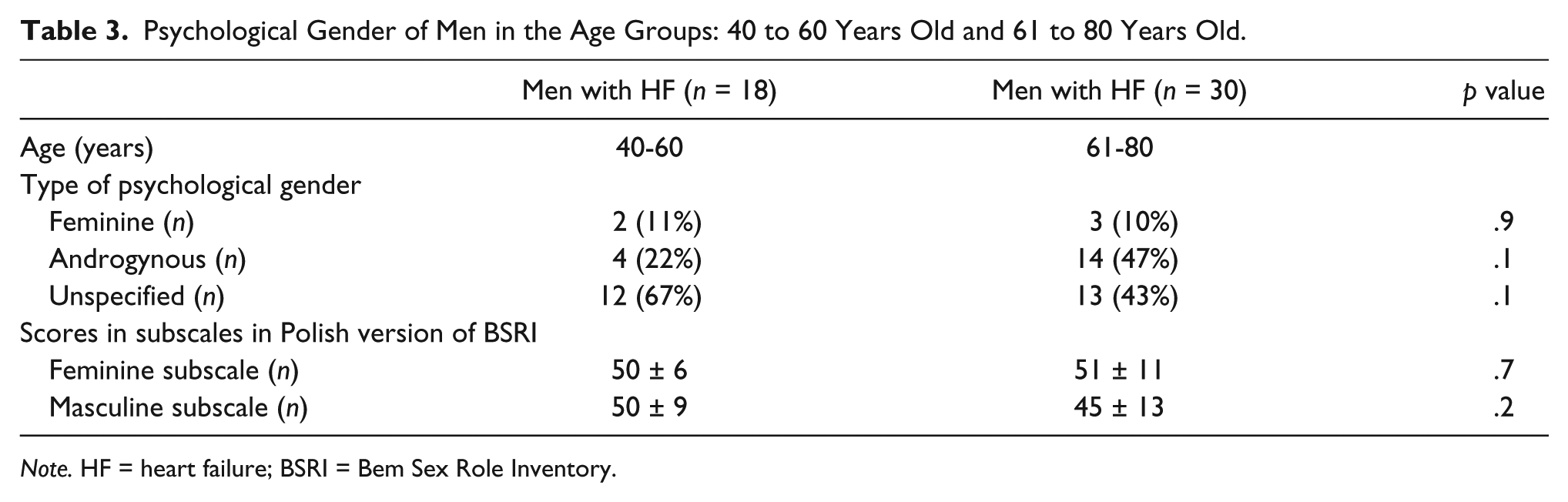
Note. HF = heart failure; BSRI = Bem Sex Role Inventory.
Discussion
In the present study, it has been reported that none of the examined men with HF identify with the M type of psychological gender. Moreover, the U type of psychological gender was more frequent among patients with HF as compared with the healthy men.
The lack of men that identify with type M suggests that none of the HF patients were able to describe themselves using typically masculine (or simply attributed to masculine social role) adjectives. Moreover, the results showed that men with HF tended to describe themselves using a generally low number of adjectives, which resulted in high prevalence of the U type among men with HF.
This research is cross-sectional, so there is no clear causal relationship. However, it can be hypothesized that among men with HF there is lack of “masculine” men because masculine men do not suffer from HF. On the other hand, it can be hypothesized that psychological gender has changed as an adaptive consequence of developing HF.
The first hypothesis, suggesting that masculine men are those who do not suffer from HF, is questionable. It has been reported that people with the M type of psychological gender often demonstrate “Type A personality behavior” as compared with the other types of psychological gender (Batlis & Small, 1982). Type A personality behavior is a well-established predictor of the development of various cardiovascular diseases (Haynes, Feinleib, Levine, Scotch, & Kannel, 1978) because Type A people are aggressive, competitive, impatient, easily irritated, and they lead an accelerated, rapid life. Adjectives included in the masculinity subscale of BSRI are very similar to those characterizing Type A (i.e., aggressive, competitive, ambitious; Batlis & Small, 1982; Gallacher, 2003). Moreover, although (as it is mentioned in the introduction) psychological masculinity might be favorable during convalescence after myocardial infarction (Radley et al., 2000), there is evidence that it is not favorable in the context of long-term medical consequences (Courtenay, 2000; Helgeson, 1990, 1991, 1995; Helgeson & Taylor, 1993). In sum, the assumption that men with the M type of psychological gender do not suffer from heart problems is questionable. Moreover, verification of this assumption would require a longitudinal study.
The second interpretation, suggesting that psychological gender has changed under the influence of the disease (perhaps as an adaptation) is more likely. As stated, changes of health status might be accompanied by changes of the psychological gender (Behar, de la Barrera, & Michelotti, 2001; Gale-Ross et al., 2009; Kowalczyk et al., 2012; Ku et al., 2002; Patten, Williams, Lavorato, & Bulloch, 2010; Radley et al., 2000; Sajatovic, Micula-Gondek, Tatsuoka, & Bialko, 2011; Wysocka-Bobryk, Procner, & Tchórewska, 2001). It has been also reported that even apparently adverse psychological changes (for instance developing depression) can be interpreted as an adaptation to new, more difficult life conditions (Andrews & Thomson, 2009). Thus, the authors suggest that psychological gender can be interpreted as a strategy aimed to cope with disease.
The observed differences might be interpreted as a psychological adaptation of patients with HF, evoked by their physical weakness, which excluded them from their masculine role (requiring physical fitness). Perhaps men with HF revise their ability to identify with features associated with the typical definition of masculinity (such as “strong” or “independent”). In other words, the authors suspect that men developing HF may become less “masculine” to accept their new role in the family and in society. However, the observed differences between healthy men and men with HF should be supported by data from longitudinal studies, which will verify if psychological gender has changed as a result of suffering from HF.
Among patients with HF, lack of men with type M was accompanied by overrepresentation of men with type U. This is alarming because the U type among healthy people is characterized by the highest level of stress (known as a risk factor for cardiovascular diseases) and by the highest risk of developing depression, which is a common comorbidity of HF (Drohomirecka, Jankowska, Banasiak, & Ponikowski, 2008; Jankowska et al., 2010; Lipińska-Grobelny, 2008; Patten et al., 2010; Prakash et al., 2010). In other words, type U can be interpreted as the least favorable type in the context of general health status and emotional comfort.
Perhaps (in the view of the results mentioned above) psychological support addressed to patients with HF can include the redefining psychological gender of patients. However, it should aim to elicit identification with type A or even F but not U.
In our study, the authors have observed an interesting relation between the psychological gender and the treatment administered for HF: Men treated with spironolactone have the F type of psychological gender more frequently. Although this observation was performed in a very small group (n = 5) the difference was statistically significant. It is known that some medications (including spironolactone, which is an antagonist of the androgen receptor) have an influence on the metabolism of hormones, that is, long-term application of spironolactone can lead to hypogonadism resulting in gynecomastia (Bridgett & Mookadam, 2009; Carr, 1986; Jankowska et al., 2006). In other words, it could be assumed that changes in the psychological gender of patients suffering from chronic diseases and thus receiving long-term pharmacological treatment might result from side effects of these therapies (Hassler & Nieschlag, 1989; Jankowska et al., 2006). The extent of changes in the human psyche in patients with HF can be very wide and can also depend on medications.
Conclusions
In the presented study, the authors analyzed a particularly important psychological feature, that is, the psychological gender. Preliminary observations identified that the psychological gender was different in males with HF as compared with healthy men: there were no men with the M type of psychological gender. Moreover, men with the U type of psychological gender were overrepresented among patients with HF in comparison with healthy, age-matched controls. The authors believe that the observed pattern of the psychological gender of patients with HF reflects an adaptation occurring within widely understood psychological structure of those patients, aimed to cope with psychological and emotional burden resulting from a chronic, terminal disease, like HF.
Study Limitations
There are some limitations related to the applied methodology, which need to be acknowledged. First, the Polish version of BSRI did not include the normalization process, thus our analysis was limited to comparisons between patients and a (smaller) group of healthy controls. Moreover, it can be presumed that the influence of the somatic disease on the tendency to express features related to the psychological gender might also affect the process of filling in the survey related particularly to the questions of gender. Third, the presented results were derived from a typical cross-sectional study. Longitudinal studies should be performed to verify a hypothesis regarding the potential changes of psychological gender as a result of suffering from HF.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The project was funded by statutory activities of Polish Academy of Sciences - Anthropology Unit, in 2007/8.