
Abstract
The role of social support in the mental health of formerly incarcerated Latino men (FILM) is an issue overlooked in public health prevention efforts. The objectives of this analysis were to (a) describe the levels of social support perceived and received by FILM; (b) identify the associations, if any, between levels of social support and mental health indicators such as depression and anxiety; and (c) explore the impact of familism and hypermasculinity on the receptivity of social support and the potential role of these factors in mediating associations between social support and mental health indicators. To accomplish the objectives, we conducted a cross-sectional survey with FILM (n = 259), ages 18 to 59, in New York City, and one nominated member of their social network (n = 130 dyads). In this analysis, we examined four dimensions of social support (instrumental, informational, appraisal, and emotional) from two perspectives: provided (as reported by members of the social networks) and perceived (as reported by FILM). The major outcome variables for this analysis were the presence/absence of major anxiety and depressive symptoms. Our logistic regression analyses suggest that perceived emotional support was inversely associated with both anxiety and depression. Our findings suggest that familism mediated the association between perceived emotional support and anxiety/depression. Therefore, we must consider designing network enhancement interventions that focus on both FILM and their social support systems.
Rates of depression among male inmates in the United States are estimated at between 17% and 40%, which is 2% to 9% higher than rates among the general population (Boothby & Durham, 1999; Domalanta, Risser, Roberts, & Risser, 2003; McMurran & Christopher, 2009). The presence of depression and anxiety significantly affects the quality of life and presents considerable barriers for formerly incarcerated men reentering the community. Incarcerated populations are thought to be particularly susceptible to mental health disorders through two major pathways. First, mental illness is often present preceding the entrance into the criminal justice system; and second, depression can result as an outcome of circumstances surrounding incarceration or reentry into society.
Scholars have argued that the number of mentally ill within the criminal justice system have increased along with other groups with a high rate of arrest—such as drug addicts and those with minimal education and income—as a result of their social vulnerability (Draine, Salzer, Culhane, & Hadley, 2002). Furthermore, jail/prison diversion programs intended to identify mentally ill prisoners early in their incarceration process and divert them into mental health programs have been largely ineffective (Draine & Solomon, 1999; Watson et al., 2010), thus further populating prisons with people whose mental illnesses have gone undetected. Incarceration in itself can be a painful and distressing event that may be difficult or impossible for some men to overcome (Visher & Travis, 2003). On leaving prison, former inmates are faced with transitioning from a highly structured environment of command and instruction to the often frenzied milieu of modern life (Visher & Travis, 2003). Men adjusting to life postrelease have been found to struggle with the formation of social relationships that could aid this transition, resulting in aggravation and disappointment (Seal, Eldrige, Kacanek, Binson, & MacGowan, 2007). Indeed, if we examine the social and interpersonal environments of formerly incarcerated men, they are potentially at risk of depression for their exposure to well-documented environmental causes of depression, including (a) abuse and childhood trauma, (b) interpersonal conflict, (c) social isolation, (d) high chronic illness, and (e) substance abuse (Alavi, Grebely, Matthews, Petoumenos, & Yeung, 2012; Beard, Tracy, Vlahov, & Galea, 2008; Kendler, Gardner, & Prescott, 2006; Penzak, Reddy, & Grimsley, 2000; Sullivan, Goulet, Justice, & Fiellin, 2011); however, the causation of these environmental causes on depression among formerly incarcerated Latino men (FILM) have not been demonstrated empirically.
For formerly incarcerated men to access mental health services, they must address multiple stigmas and life constraints. Discrimination associated with imprisonment ranges from societal prejudices against criminal records to internalized stigmas related to mental health issues (Draine, Blank Wilson, Metraux, Hadley, & Evans, 2010; Draine & Herman, 2007; Link, Phelan, Bresnahan, Stueve, & Pescosolido, 1999; Stuber, Meyer, & Link, 2008). Further barriers to depression care include lack of knowledge about depression and treatment, negative attitudes toward depression care, and not recognizing depression as a treatable medical illness (Cabassa, Hansen, Palinkas, & Ell, 2008; Cabassa, Lester, & Zayas, 2007; Givens, Houston, Van Voorhees, Ford, & Cooper, 2007; Interian, Ang, Gara, Rodrieguez, & Vega, 2011; Interian, Martinez, Guarnaccia, Vega, & Escobar, 2007; Pincay & Guarnaccia, 2007; Vega, Rodriguez, & Ang, 2010). Recent studies indicate that racial and ethnic minorities are disproportionately affected by depression. Latinos, in particular, experience significantly higher rates of current depression symptoms (11.4%) compared with their White counterparts (7.9%; CDC, 2010). Rates of depression among male inmates are estimated between 17% and 40%—2% to 9% higher than rates among the overall general population (Boothby & Durham, 1999; Domalanta et al., 2003; McMurran & Christopher, 2009).
A critical factor affecting ethnic minority men’s health in the United States is hyperincarceration, which began in the late 1970s and peaked less than a decade ago (Pettit & Western, 2004). We used the term hyperincarceration as defined by Loic Wacquant in opposition to “mass incarceration” since U.S. incarceration targets a specific vulnerable population, that is, poor African American men and poor Latino men (Goldberg, 2009; Gottschalk, 2010; Wacquant, 2008, 2009). The socioeconomic phenomena of the “the Prison Industrial Complex” has been defined as the combination of tough-on-crime legislation and the public policy of encouraging increases in spending on imprisonment (Andrews & Bonta, 2010; Caplow & Simon, 1999; Smith & Hattery, 2006). The rates of incarcerated populations increased more than three times between 1990 and 2008 to close to 0.9% of the total U.S. population, one of the highest incarceration rates globally, with a disproportional representation of ethnic minority men (mostly African American and Latino men; Andrews & Bonta, 2010; Caplow & Simon, 1999; Glaze & Parks, 2012; Smith & Hattery, 2006; VERA Institute of Justice, 2011). Over the past 4 years, the annual rates of imprisonment have not increased and maintained steady or decline in some states (Glaze & Parks, 2012). Yet the number of people nationwide who continued to be involved with the criminal justice system have not diminished, given that the high proportions of people serving sentences outside prison (in jails or community correctional facilities) and the number of people in probation (offenders on ordered to follow certain conditions set forth by the court and under supervision) have increased (VERA Institute of Justice, 2011). Nationally, Latinos are overrepresented in correctional facilities, constituting more than 25% of the incarcerated population, but only 13% of the overall U.S. population (U.S. Department of Justice, 2008). By December 31, 2011, Latino men represented 21.6% (331,500 out of 1,537,415) of the sentenced individuals under state and federal criminal justice systems in the United States (U.S. Department of Justice, 2012). In 2011, there were 688,384 releases from state or federal prisons, with approximately 16% of them representing Latinos (U.S. Department of Justice, 2012).
The large majority of persons who enter the prison system return to their families and/or former living arrangements, becoming reconnected with others and “institutions of society” that become paramount to their ambitions and development (Visher & Travis, 2003). Indeed, social support is critical during the postrelease period to ease transition, avoid recidivism, and reduce the likelihood of engaging in both health-risk practices and reoccurrence of criminal behavior (Halsey, 2007; Seal et al., 2007). At the same time, based on the literature on social networks, any network can influence men’s health either by increasing risk and poor coping strategies or by serving as protective sources of support, thus reducing risk (Griffith, Ellis, & Allen, 2012; Mount et al., 2012, Murphy, Gordon, Sherrod, Dancy, & Kershaw, 2013). After leaving correctional facilities, men most often look to their family network for support and assistance during their reentry process (Grinstead, Comfort, McCartney, Koester, & Neilands, 2008; Picó, 1994). When traditional family networks are not found, or are problematic to the men, the notion of family is redefined to include two additional, often overlapping, networks: close friend/peer networks and street/prison gang-related networks. The relationships between men and their kinship and social networks are critical to build a system of social support that can potentially assist in dealing with the process of reentry and the risk for suffering from anxiety and depression. In this analysis, we draw on the concept of familism as an indicator of the emotional and tangible connections with men’s familial social environment (see Conceptual Framework section below).
The present exploratory analysis seeks to identify the role of social support in potentially addressing depression and anxiety among FILM. As a minority group, FILM face the challenges of postincarceration—work discrimination, family conflict—in a context of institutionalized racism (Muñoz-Laboy & Perry, 2011). In addition to the trauma of incarceration, prior studies by the authors have identified that FILM experience high rates of both street violence and excess mortality in their kinship and social networks (Muñoz-Laboy et al., 2012). Authors have found that while many FILM may be surrounded by others on the street and in social and kinship networks, they often experience a lack of opportunity or comfort to talk openly about issues that affect them most, leaving them to deal with symptoms of anxiety and depression alone (Muñoz-Laboy et al., 2012). The importance of social networks and support for men experiencing depression and in the aftermath of loss is well-documented (Aho, Tarkka, Astedt-Kurki, & Kaunonen, 2009; Watkins, 2012), as are the negative mental health consequences for men whose social bonds have deteriorated (Oliffe, Han, Ogrodniczuk, Phillips, & Roy, 2011).
There are limited data on the role of social support in Latino men’s mental health outcomes after incarceration. Limited research on sources of social support for FILM suggests that there are four types of social networks under the label of “family” that serve as sources of support. These include kinship/familial networks, friend/peer networks, gang-related networks, and pro-prisoner rights mobilization networks. Examining the role of social support in formerly incarcerated men’s lives is both theoretically important and practically relevant, since social support could be an important predictor of positive mental health outcomes as well as a key resource for men coping with challenges known to circumscribe their options, including unemployment, social isolation, housing issues, and substance abuse (El-Bassel et al., 1995).
Conceptual Framework
Social Support
House (1981) defines social support as perception and actuality that one is cared for, has assistance available from other people, and that one is part of a supportive social network. Social support has been conceptually divided into four domains: informational (information provided to another during a time of stress), instrumental (the provision of tangible goods and services or tangible aid), appraisal (the communication of information which is relevant to self-evaluation rather than problem solving), and emotional support (the provision of caring, empathy, love, and trust; House, 1981; Krause, 1987; Weinert, 1987). Studies on social support suggest that there is a difference between social support provided and social support perceived to be received, with one of the current debates in the literature being which type of support is more impactful in the life of the recipient. Perceived emotional support has been shown in a number of studies to be associated with fewer symptoms of anxiety and depression, whereas received emotional support had limited effects (Dunkel-Schetter & Bennett, 1990; Kessler, Kendler, Heath, Neale, & Eaves, 1992; Wethington & Kessler, 1986). In our conceptualization of social support for FILM, we included perceived and received instrumental, informational, emotional, and appraisal support. In addition, because a number of studies have reported that the positive effects of perceived social support are dependent on a number of recipient-level factors including recipients’ personality traits, coping skills, coping styles, and personal network characteristics (Thomas, Simpson, Tarver, & Gwede, 2010; Ueno and Adams, 2001), we designed our conceptual framework to reflect FILM’s reception of social support as related to attitudes toward families (positively influencing their receptiveness of social support) and traditional values of hypermasculinity (negatively influencing receptiveness of social support).
Familism
The connection between the social organization of the family and individual’s health has often been studied through the construct of “familism,” conceptualized as a culturally specific set of values that creates interdependence among nuclear and extended family members via notions of support, loyalty, and solidarity (Lugo-Steidel & Contreras, 2003). Individuals’ perception of their emotional closeness, loyalty, and prioritizing the collective good of the family over individualistic gains have been demonstrated to serve as a mediating factor between individual-level factors and risk-taking practices, self-esteem, and self-efficacy among adolescents (Bush, Supple, & Lash, 2004; Ramirez et al., 2004; Schwartz, 2007; Unger et al., 2002).
(Hyper)masculine Ideologies
Drawing on the perspective that perceived support is influenced by individuals’ receptivity, conscious or unconscious denial of support received to maintain image of self-reliance, and independence (Ueno & Adams, 2001), we propose that to fully understand the relationship between social support and mental health outcomes, we must take into consideration FILM’s notions of masculinity and health. In a prior analysis with FILM, we identified a stronger adherence to nonegalitarian gender perspectives (i.e., hypermasculine views such as “It is more important for a woman to learn how to take care of the home and the family than it is for her to get a college education;” “It is important to be ‘macho’ in order to get the attention of women”) were correlated with lower utilization of health and social services (Muñoz-Laboy et al., 2012). Although recent research suggests that strong adherence to traditional notions of masculinity may be protective factors for men’s health (Berger, Levant, McMillan, Kelleher, & Sellers, 2005; Levant & Richmond, 2007), our measures of masculinity focused on nonegalitarian views of gender and display of power, control, and domination over women and other men, which we conceptualized as hypermasculinity. Because ideologies of hypermasculinity seem to reduce FILM’s likelihood of seeking and accessing health and social services, our present analysis aims to provide insights into the effects of masculinity in social support and its potential relationship to mental health indicators among FILM.
Our analysis for this article consisted of answering the following research questions:
Convinced that a deeper understanding of social support among FILM was thus both relevant and timely, we developed a self-administered survey to examine the social networks and risk factors of FILM in New York City. The results of the self-administered survey are the focus of this article.
Methods
Study Design
The examination of the associations between social support and depression/anxiety was embedded within a larger mixed-methods study that sought to examine the social network determinants of health risk behaviors among FILM. The analyses presented in this article focus exclusively on data collected through the self-administered surveys of FILM and their support person. The cross-sectional survey phase of the study was originally designed to recruit 200 FILM and 200 individuals that they considered their closest source of support (regardless of whether the individual was a family member or a friend). During the data collection process, a considerable number of FILM were unable to identify an individual as their closest source of support. Thus, we received permission from our institutional review board and funding agency to alter our inclusion criteria and allow FILM without sources of support into the study (no demographic differences were found between those with and those without nominated sources of support). Of the 350 men we recruited, 88.6% (n = 310) met the eligibility criteria for the study; of those, 12.9% refused to participate due to time constraints or a lack of interest and 3.5% began but did not complete the survey. In other words, of the 350 men originally recruited, 259 (74%) completed the survey (n = 259).
Data Collection Procedures
Five trained community field researchers recruited participants from three geographic areas in New York City: the Bronx, Brooklyn, and Upper Manhattan. One quarter of participants (n = 65) were recruited from referrals from flyers posted in the research sites. The remaining participants (n = 194) were recruited on the street or at community events through person-to-person outreach. The men in the study self-identified as Puerto Rican, Neyorican, or Latino. Approximately one quarter of the sample were born in Puerto Rico, and the remaining were born in New York or the Northeast of the United States to Puerto Rican parents. Individuals were included in the study if they were male, they were between the ages of 18 and 59, and they had been in jail or prison within the past 5 years (see Table 1).
Study Sample Characteristics: Formerly Incarcerated Latino Men (N = 259).

Data collection took place during data collection events at facilities of the Mailman School of Public Health at Columbia University. Individuals who had been deemed eligible for the study first completed informed consent procedures with trained staff in a private setting near the recruitment site or in field staff offices and there they were asked to complete the survey on a laptop computer in the same private setting or office where consent had been ascertained. The survey took 45 to 90 minutes to complete. The survey was distributed from March 2010 to April 2011. Before initiating the survey, participants were, once again, asked to indicate their consent to participate by agreeing to a voluntary participation statement on the computer screen. Each participant was compensated $50 for participating in the survey. Additionally, a Certificate of Confidentiality was obtained from the National Institute of Mental Health to protect the privacy and confidentiality of the study participants, and any contact information linking study participants to participation in the cross-sectional survey phase of the study was destroyed after completion of the survey. This study was approved by the Columbia University Institutional Review Board (protocol number: IRB-AAAE4697).
Measures
Guided by our conceptual framework, we used the following measures in the analysis. Our four dimension scale of social support was based on House’s (1981) conceptualization of social support as adapted and validated by Bernal, del Río, and Moldonado-Molina (2003) for Puerto Ricans, who comprise the majority of our sample. All measures were examined for reliability prior to data analysis. Where appropriate, we have reported the Cronbach’s alpha (CA) reliability coefficients for each measure.
Based on the above studies, social support measures included (a) Instrumental support: a composite measure of a series of questions on the supportive behaviors (e.g., doing groceries, accompanying person to an appointment) of the nominated member of the social support of FILM toward the FILM over the past 2 months (6 items, CA = .87); (b) Informational support: a composite measure of a series of questions on the level of communication regarding employment and accessing other resources (e.g., telling person about a job opening) from the nominated member of the social support of FILM toward the FILM over the past 2 months (2 items, CA = .84); (c) Appraisal support: a composite measure of a series of questions on the frequency of contact with FILM to assist in FILM’s self-evaluation that nominated support individuals provided to FILM over the past 2 months (3 items, CA = .68); and (d) Emotional support: a composite measure of a series of questions on the frequency of contact with FILM with the purpose of listening to problems “venting,” planning activities to reduce stress, or being present in the good and bad times for FILM over the past 2 months (3 items, CA = .71).
Perceived instrumental, informational, emotional, and appraisal support were assessed from the data provided by FILM on the support that they perceived to be receiving by the closest five members of their social networks. Participants were asked to list the most important people in their lives (i.e., their network referents) with a maximum list of five individuals. They were then asked to classify the individuals into one of 15 categories (i.e., close friends, lovers, girlfriends, boyfriends, uncle, cousin, wife/cohabiting partner, etc.) and provide detailed information about the characteristics of each individual and the nature of their relationship. These individuals included the nominated social support person who participated in our study. Within these questions we measured perceived support in terms of perceived instrumental and informational support collapsed into one measure (4 items, CA = .83), emotional support (5 items, CA = .98), and appraisal support (4 items, CA = .70). Each of these scales were added by each type of network and divided by each of the number of individuals represented in the network to obtained standardized measures of perceived support. Our measures of mediating variables were familism (Lugo-Steidel & Contreras, 2003), 18 items, CA = .93; and hypermasculine attitudes (Cuellar, Arnold, & Gonzalez, 1995), 22 items, CA = .85.
Our dependent variables were depression (6 items, CA = .92) and anxiety (6 items, CA = .95). Depression and anxiety were measured using the Brief Symptom Inventory (BSI). The BSI consists of 53 items covering 9 symptom dimensions, of which depression and anxiety are two of them. FILM ranked each feeling item (e.g., “your feelings being easily hurt”) on a 5-point scale ranging from 0 (not at all) to 4 (extremely). Rankings characterize the intensity of distress during the past 7 days. The BSI is the short version of the SCL-R-90 (Derogatis, 1975; Derogatis & Cleary, 1977), which measures the same dimensions. Items for each dimension of the BSI were selected based on a factor analysis of the SCL-R-90, with the highest loading items on each dimension selected for the BSI (Derogatis, 1993; Derogatis & Cleary, 1977; Derogatis & Spencer, 1982); therefore, BSI score cutoffs are highly correlated with being symptomatic of the mental health disorder dimension, in our case chronic depressive disorder and chronic anxiety disorder. Raw scores from participant responses were converted to T scores using the tables provided in the BSI manual and interpreted by comparison to age–gender appropriate normative data of nonclinical samples of adults, and we determined the cutoff score for depression at 2.20 and for anxiety at 2.40 (Derogatis, 1993; Derogatis & Cleary, 1977; Derogatis & Spencer, 1982).
Statistical Analysis
Data were extracted from the survey database and imported into IBM SPSS Statistics 20.0.1. Because our intention was to identify the role of different types of social support on mental health indicators of FILM, each domain of social support was treated independently throughout our analysis. We performed logistic regression modeling to test the associations between social support dimensions and the presence/absence of depression and/or anxiety. After examining the associations between social support dimensions and mental health indicators, we tested for mediation effects of familism, hypermasculinity, and both factors. Mediation functionality will be determined on meeting the following conditions: (a) level of social support will be associated with likelihood of anxiety or depressive disorders, (b) changes in familism/masculinity will be associated with changes in anxiety or depressive disorders (outcome indicators), (c) level of social support will be associated with familism/masculinity, and (d) associations between social support factors and anxiety/depressive disorder outcome indicators will be weaker when controlled for familism/masculinity measures. This analytical procedure represents the Barron and Kenny (1986) method of mediation analysis. In the following section, we present the results of our analyses.
Results
Context
The vast majority of the men in our study reside in urban poor communities in New York City. The majority (84.5%) of the participants served in prison/jail for drug related charges and the minority (15.5%) were convicted for violence-related crimes. Most participants were 18 to 39 years of age (57.5%) and unemployed (74.9%). The most commonly reported reason for unemployment was inability to find work (42.2%), followed by illness, disability, or inability to work (30.7%). See Table 1 for additional demographic data.
Social Support and Demographic Differences
Sources of social support identified by FILM in our sample were (a) parents, grandparents, or uncles/aunts (35.7%); (b) friends (29.4%); (c) spouses and/or cohabitating female partners (23.2%); and (d) girlfriends/noncohabitating female partners (11.7%). None of the respondents had male partners at the time of the study. Most of the men (64.4%) identified only two individuals as people they feel supported by. Yet 35% of FILM in the study were unable to list one person they felt close to or cite as a source of support.
The demographic characteristics for sources of support who participated in the study (n = 130) were as follows: 78.1% was female and 35.9% was within the ages between 30 and 45 years. Sources of social support that provided data on the types and frequencies of social support provided (n = 130) had a similar socioeconomic profile as the FILM in the study. We found no statistical differences by education, income, and employment history for FILM or their sources of support (findings not included in the tables). Sources of support who participated in the study (n = 130) were mostly female (78.1%) and were more likely to be older than FILM with 51.6% above the age of 45.
Social Support: Provided Versus Perceived
In our analysis, we regressed each of the types of support provided by the nominated member of the FILM social network onto FILM’s own perceived dimension of social support. We found that (a) high instrumental support provided was positively associated with perceived instrumental/informational and perceived emotional support; (b) high informational support provided was positively associated with perceived instrumental/informational support; (c) high appraisal support provided was positively associated with perceived instrumental/informational support; and (d) high emotional support provided was positively associated with perceived emotional support (see Figure 1). In our sample, the type of social support provided predicted the type of social support perceived to be received except in the case of appraisal support.

Regression coefficient intervals between dimensions of social support provided and perceived social support.
Familism, Hypermasculinity, and Social Support
As predicted, it was identified that familism was strongly associated with social support among FILM. High levels of familism were positively correlated with each dimension of support provided to FILM and perceived social support among FILM (see Figure 2). Variations in levels of hypermasculine attitudes were not associated with differences in levels of social support provided to FILM or perceived social support (findings not presented in tables).
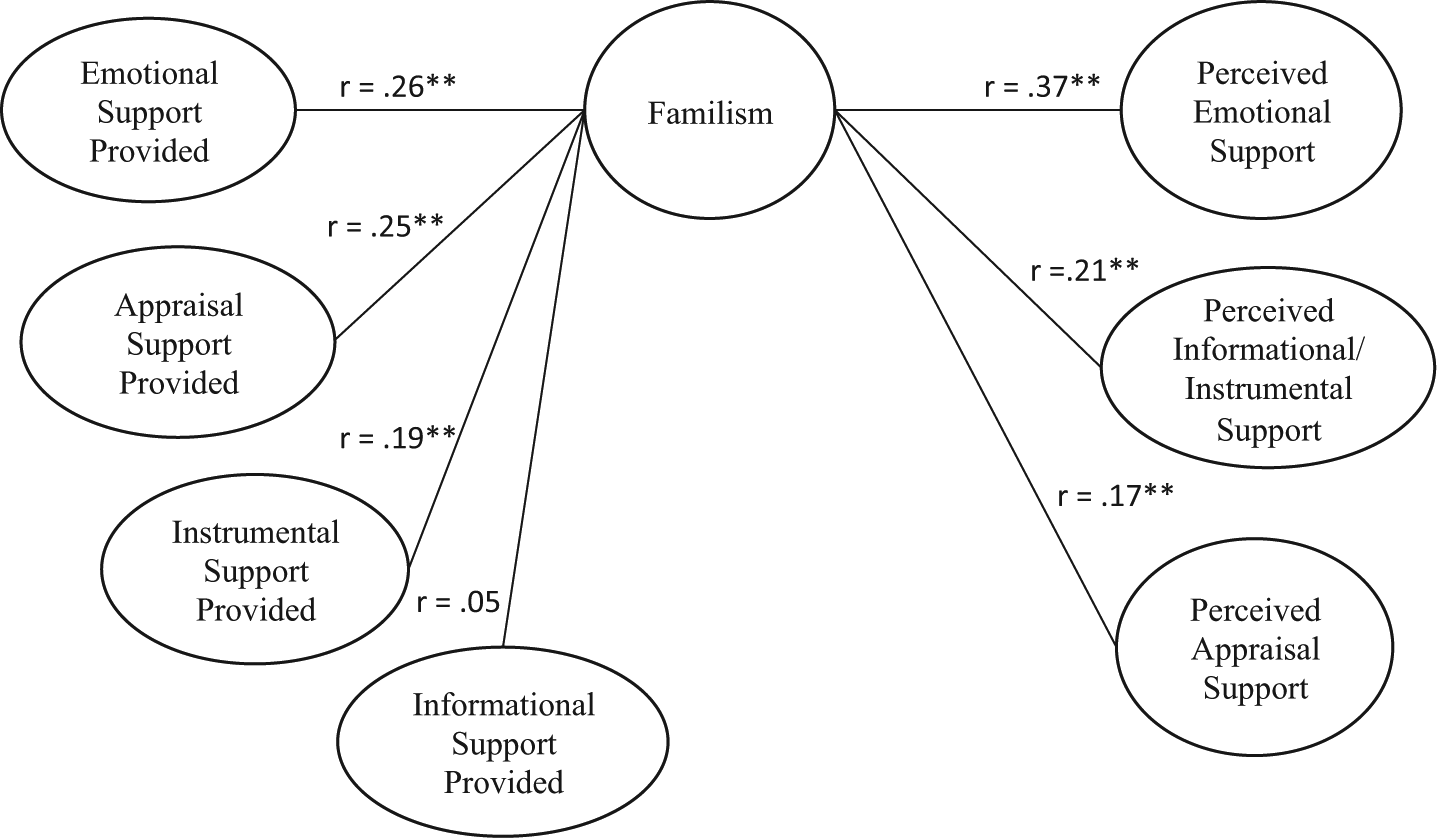
Pearson correlations coefficients (r) between dimensions of social support and familism.
Mental Health Indicators and Demographic Differences
In terms of depression and anxiety, 26.9% and 30.5% met the thresholds of chronic depressive and anxiety disorders, respectively. We conducted our analysis using these variables as separate mental health indicators to be able to specify the associations between social support and mental health. In our sample, we identified that differences in depression or anxiety status were not associated with FILM demographic factors or in the size of men’s social network or the number of social support individuals.
Anxiety, Depression, Social Support, and Familism
For FILM in our sample, perceived emotional support was inversely associated with anxiety and depression (see Table 2, Model 1; Table 3, Model 1). Our findings from our logistic regression models indicate that the higher men’s perceived emotional support, the lower their likelihood of anxiety and depressive disorders. The other forms of support identified in the study were not associated with differences in the likelihood of anxiety/depression. High levels of familism were associated with lower likelihood of anxiety and depressive disorders (see Table 2, Model 2; Table 3, Model 2). Our findings suggest that familism mediated the association between perceived emotional support and anxiety/depression because of the following reasons: (a) the level of perceived emotional social support was associated with likelihood of anxiety/depression; (b) the level of perceived emotional social support was associated with familism; and (c) changes in familism were inversely associated with the likelihood of anxiety and depression. After introducing the interaction term in both models (anxiety and depression), only the interaction factor was statistically significant, while the independent predictors of perceived emotional support and familism became not significant (see Table 2, Model 4; Table 3, Model 4). Contrary to our hypotheses, hypermasculinity was not associated with the likelihood of neither anxiety or depression (see Table 2, Model 3; Table 3, Model 3) or social support. Therefore, none of the conditions for mediation functionality were met for the effects of hypermasculine attitudes.
Social Support, Familism, and Masculinity Factors in Likelihood Anxiety Disorder Among Formerly Incarcerated Latino Men (n = 259).

Note. CI = confidence interval; AOR = adjusted odds ratio .The values in boldface indicate that the AOR are statistically significance (p < .05).
Social Support, Familism, and Masculinity Factors in Likelihood Depressive Disorder Among Formerly Incarcerated Latino Men (n = 259).
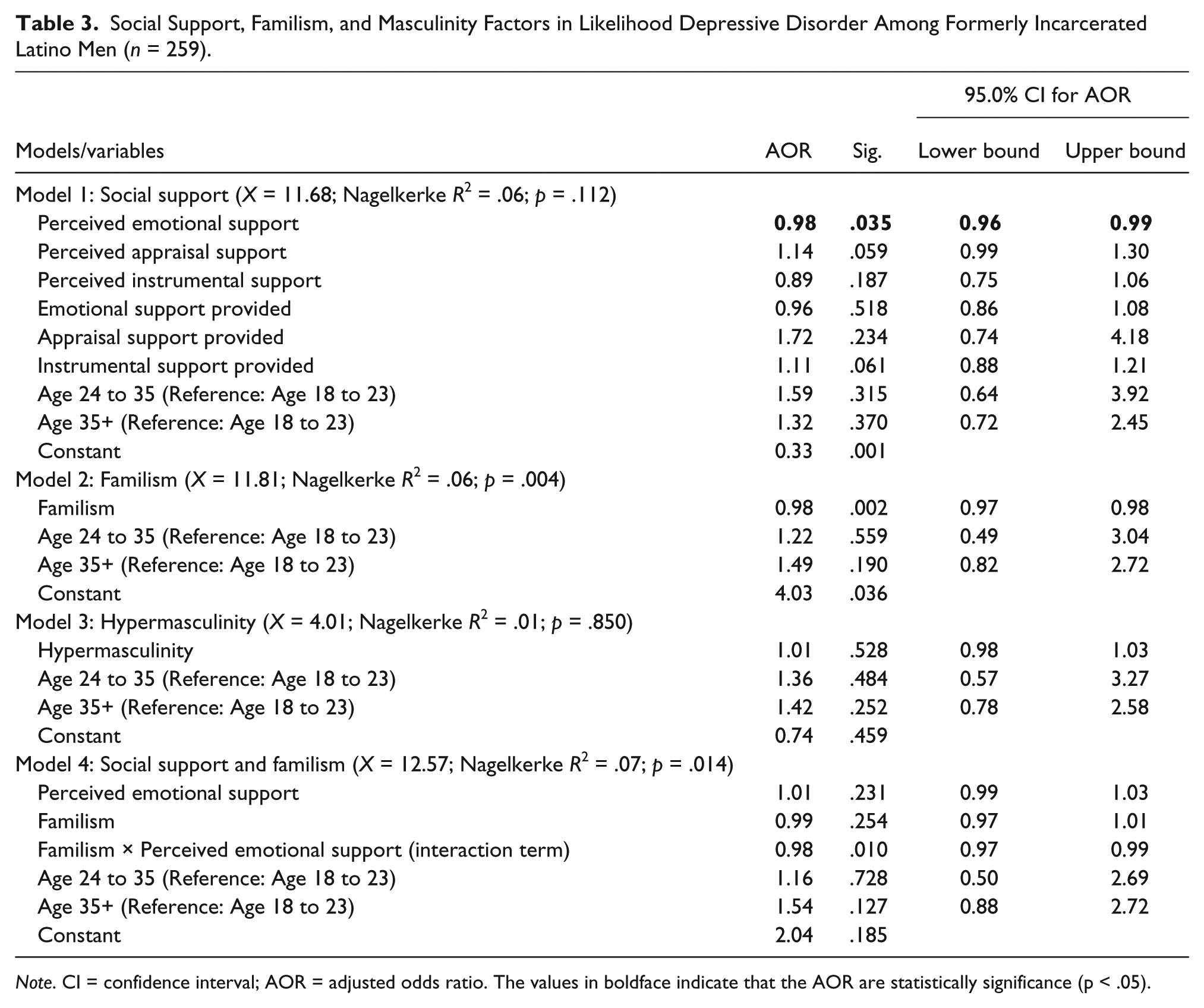
Note. CI = confidence interval; AOR = adjusted odds ratio. The values in boldface indicate that the AOR are statistically significance (p < .05).
It should be mentioned that the survey component itself was anonymous to protect the confidentiality of study participants because of the sensitive nature of the questions asked. By the time of data analysis, we could not trace those who met the anxiety and depression criteria to recommend treatment—something we are planning for future studies with this population. We did provided a list of referrals to services and our contact information if participants felt distressed because of the interviews or wanted to discuss issues further or seek connections to health-related services but individual counseling was not provided.
Discussion
In this study, we found that all dimensions of support reported by social networks of FILM, with the exception of appraisal support, were positively associated with each of the corresponding dimensions of perceived support. Contrary to our expectations, only one dimension of social support—perceived emotional support—was inversely associated with the likelihood of depression and anxiety. This suggests that perceived support availability may function as a cognitive mechanism to help men process information about what support they receive. This is further confirmed by our finding that perceived emotional support positively interacted with familism: high perceived emotional support in combination with high familism significantly reduced the likelihood of anxiety disorder, beyond the independent effects of familism or perceived emotional support. Our findings therefore support the notion that strengthening family relations and men’s perceptions of the positive aspects of family connectedness can reduce men’s likelihood of anxiety.
Our evidence did not support our hypothesis that hypermasculine (nonegalitarian views of gender, strong adherence to notions of control, domination, and power) ideologies mediated the relationship between perceived emotional support and mental health indicators. However, our lack of empirical evidence could be the result of selecting a single measure rather than multiple indicators, or otherwise inadequate measures of hypermasculine ideologies. And because of the well-documented connection between masculine ideals and the lessened likelihood of seeking care for mental health symptoms (Muñoz-Laboy et al., 2012; Rochlen et al., 2010; Oliffe et al., 2011), we suggest further research before this lack of association is conclusive.
Limitation
Studies suggest that perceived and received support are often conceived and measured at different stages in the coping process, whereby perceived support is a coping resource available prior to the occurrence of life events that required support (Lindsey & Marcell, 2012; Ueno & Adams, 2001). Consequently, received support is usually mobilized after the life events. This assumption of time is critical in both understanding the relationship between social support received and perceived and in empirically testing the effects of social support on mental health. Although we found an association between received and perceived support, because our study was cross-sectional, we have a limited understanding of the directionalities of these relationships. Furthermore, because we measured anxiety and depression simultaneously with social support we cannot determine the full effects of received social support.
Ueno and Adams (2001) have shown that, if mental health outcomes are measured immediately after the life events, the initial increase of received support may suppress the beneficial effects because received support may gradually improve mental health over time. Because individuals tend to perceive less support to be available than they actually receive (Dunkel-Schetter & Bennett, 1990), which may be the result of recall biases (Ueno & Adams, 2001), subjective determinations if support received warranted being labeled as support, or conscious efforts to suppress memories of support received in order to sustain self-efficacy and a sense of independence. Measuring the effects of perceived social support represents a continuing challenge in cross-sectional design studies. Thus, longitudinal studies on the impacts of social support in the lives of FILM are urgently needed.
Another limitation of our cross-sectional design is the potential for endogeneity, that is, a correlation between the variable and an error term, between our independent variables and our outcome variables. In other words, the estimated effect of a regressor on an outcome is inconsistent when that regressor is determined simultaneously with that outcome (Foster, 1997), that is, a FILM’s chances of anxiety and depressive disorders could potentially be jointly determined by the variables that we identified in the models and unspecified factors. For example, our findings suggest strong statistical associations between high likelihood of depression and low perceived emotional support. Yet depression could be the cause of low perception of emotional support, and having low social support could be the cause of depression. Using instrumental variables estimation (i.e., in essence conducting statistical modeling using variables that are uncorrelated with the outcome variable but correlated with the independent variable) is a means of obtaining consistent parameter estimates in this situation (Foster, 1997). Foster has argued that the best-known form of instrumental variables is two-stage least squares; unfortunately, this procedure cannot be simply extended to nonlinear models such as our logistic regression modeling because our outcome variables (anxiety and depression) are binary (presence or absence), and although there are other methodologies such as Generalized Method of Moments that use instrumental variables, these are most adequate when the data collected are longitudinal. Therefore, our study findings must be taken as exploratory and further longitudinal research designs are needed to examine the causal linkages between social support and anxiety/depression.
Implications
Investigations into sources of social support for Latino men, particularly FILM, are scant, despite the fact that FILM face numerous stressors. Most of the public health research on incarcerated populations has focused narrowly on recidivism, drug rehabilitation, and HIV risk, ignoring environmental risk factors—such as lack of social support—that leave men vulnerable to mental disorders like anxiety and depression. Our analysis suggests that enhancing multiple dimensions of social support maybe critical to decrease the prevalence of anxiety and depression among FILM. We must consider how bonds between men and their families are sustained or ruptured as a result of incarceration experiences; how these disruptions may lead to the onset of mental health disorders; and how some FILM manage mental health stressors through various coping mechanisms that may mitigate or exacerbate the onset of mental health disorders like depression and anxiety. This is not to suggest that other forms of support are less important. Indeed, both informational and instrumental support are essential for FILM to access health and social services and employment—particularly when facing significant challenges obtaining jobs in the formal economy (Muñoz-Laboy et al., 2012; Muñoz-Laboy et al., 2013). It is important to take into account the fact that FILM families, who most often share the socioeconomic environments and position as FILM, may be ill-equipped to provide the necessary social support. Therefore, we must consider designing longitudinal research on how to enhance social support systems for families of FILM; on the role of social support and the onset of depression and anxiety for formerly incarcerated men; and if social support systems prove decrease depression and anxiety overtime (or increase early treatment and adherence to these conditions) among FILM during the postincarceration period, further research is needed on piloting innovative strategies to enhance FILM’s social support systems. By investigating and constructing interventions into the social support environment (Rhodes, 2002), we can move beyond a reliance on informational support to address the formation of effective emotional and familial support linkages, a critical positive determinant to formerly incarcerated men’s health.
Footnotes
Acknowledgements
We would like to extent our gratitude to our research participants and we thank the members of our research team: Ilka Bobet (field coordinator) and Samuel Santiago, Santos Bobet, Francisco Quinones, and Hector Ramos (field researchers).
Authors’ Note
The content of this article is solely the responsibility of the authors and does not necessarily represent the official views of NIMH or the NIH, the funding agency.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This article was supported by the U.S. National Institute of Mental Health (Grant Number: 1 RC MH 088636-01; Principal Investigators: Miguel Muñoz-Laboy and Vincent Guilamo-Ramos).