
Abstract
The onset of an eating disorder in middle-age men is poorly researched as are eating disorders in men generally. Therefore, life events that influence eating disorders in men, including delayed onset of an eating disorder remains unknown. Given the limited understanding of males with eating disorders and limited access to large samples of men with eating disorders, an in-depth analysis of a single case of a male in middle age with an eating disorder was chosen to gain insight and understanding into this phenomenon. A Life History approach explored the case of Joseph (pseudonym), who was diagnosed at age 44 years with an Eating Disorder Not Otherwise Specified. Data were collected through (a) life course open-ended questioning through interviews, (b) written statements, and (c) comments on transcripts. Three themes emerged, loss and unworthiness, becoming bigger, and wanting to change reflecting eating behaviors associated with attachment disruption, loss and trauma, body dissatisfaction, and negative affect. Later in life, an emotional “tipping point” precipitated an eating disorder. Results indicate traumatic loss leading to early attachment disruption as influential in Joseph’s delayed onset of an eating disorder. The value of thorough narrative life histories during therapy when eating disorders occur late in life is discussed as well as the significance for men.
Eating disorders are serious and frequently fatal mental illnesses. However, eating disorders are generally considered to be low-prevalence diseases, more common among females than among males. Overall, research is limited regarding how and why eating disorders develop in males. Even less is known about why males develop eating disorders later in life. This present study is concerned with enhancing our knowledge of late-onset eating disorders in males older than 40 years. Using a case study life history approach (Denzin, 1989a, 1989b), we sought to explore the subjective understanding of gender-specific life events that may have contributed to this unique phenomenon, that of delayed onset of an eating disorder in a male older than 40 years.
The Diagnostic and Statistical Manual of Mental Disorders, fourth edition, text revision (DSM-IV-TR; American Psychiatric Association, 2000) recognizes two distinct eating disorders, anorexia nervosa and bulimia nervosa. It also provides a classification, eating disorder not otherwise specified (EDNOS) for eating disorders of clinical severity that do not meet the criteria for anorexia or bulimia. While anorexia nervosa is characterized by extremely low body weight and fear of its increasing, bulimia nervosa involves repeated binge eating and compensatory behaviors. EDNOS includes subthreshold variants of these disorders and other syndromes, such as binge eating disorder (BED).
Eating disorders in males are probably underreported because of the stigma associated with these largely female conditions (Morgan, 2008). They may also be less easily recognized by clinicians because most eating disorders in males do not meet criteria for anorexia nervosa or bulimia nervosa and are therefore likely classified as EDNOS. For example, the lean muscularity of the ideal male body protects against the low weight required for a diagnosis of anorexia nervosa but the pursuit of this ideal can still lead to disordered eating (Crosscope-Happel, Hutchins, Getz, & Hayes, 2000; Jones & Morgan, 2010; Pope, Phillips, & Olivardia, 2000; Raevuori et al., 2008). Hudson, Hiripi, Pope, and Kessler (2007) reported that males had lower lifetime prevalence rates than females for anorexia nervosa (0.3% vs. 0.9%), bulimia nervosa (0.5% vs. 1.5%), and BED (2.0% vs. 3.5%), but higher rates for subthreshold BED (1.9% vs. 0.6%). Unfortunately, it is difficult to obtain accurate estimates of prevalence because of the tendency of people with eating disorders to conceal their illness and avoid professional help (Hoek, 2006).
Onset of eating disorders typically occurs in adolescence or early adulthood. Rates of onset are low over the age of 25 years (Hay, 2004; Hoek, 2006; Hudson et al., 2007, Patrick & Stahl, 2009) and rarely reported over the age of 40 years. The few studies available include 2 patients with onset after 40 years (Mynors-Wallis, Treasure, & Chee, 1992), a single case study with onset at 41 years (Gupta, 1990), 2 patients with onset in the 40s (Tobin, Molteni, & Elin, 1995), and 11 patients with onset over the age of 40 years (Beck, Casper, & Andersen, 1996). Cumella and Kally (2008) reported 50 cases with onset at 40 years or older. All the above patients were female. One case of anorexia nervosa symptoms has been reported in a 72-year old male who was known to have a long history of food preoccupation and restrictive eating habits (Manejias Parke, Yager, & Apfeldorf, 2008).
The growing body of research on eating disorders in younger males frequently makes comparisons with eating disorders in females (Bramon-Bosch, Troop, & Treasure, 2000; D. L. Braun, Sunday, Huang, & Halmi, 1999; Button, Aldridge, & Palmer, 2008; Carlat, Camargo, & Herzog, 1997; Crisp, 2006; Crosscope-Happel et al., 2000; Fernandez-Aranda et al., 2004; Striegel-Moore et al., 2009; Strober et al., 2006). Most of these comparisons either explicitly concentrate on younger people (Austin et al., 2004; Beato-Fernandez & Rodriguez-Cano, 2005; Lewinsohn, Seeley, Moerk, & Striegel-Moore, 2002; Mitchell & Mazzeo, 2005; Raevuori et al., 2008) or are based on predominantly young samples (e.g., Pritchard, 2008). Many studies have reported that eating disorders present similarly in males and females (Bramon-Boschet et al., 2000; D. L. Braun et al., 1999; Carlat et al., 1997; Crosscope-Happel et al., 2000; Fernandez-Aranda et al., 2004; Lilenfeld, Wonderlich, Riso, Crosby, & Mitchell, 2006; Strober et al., 2006; Woodside et al., 2001; Woodside et al., 2002). However, differences are noted, though the strength and consistency of evidence is variable. On the whole, females make greater use than males of laxative, diuretic, diet pills, vomiting, and fasting, but not exercise and other compensatory behaviors (Anderson & Bulik, 2004; Striegel-Moore et al., 2009). Not all studies however were as conclusive with Lewinsohn et al. (2002) reporting greater female use of inappropriate compensatory behaviors. Food hoarding is more common among females (Crisp, 2006) who also report binge eating, body checking, and avoidance more commonly than males (Striegel-Moore et al., 2009).
Although risk factors for eating disorder are varied and common (Stice, 2002), there are gender-specific risks for males, including premorbid obesity (Crosscope-Happel et al., 2000; Fernandez-Aranda et al., 2004), parental obesity (Carlat et al., 1997; Crisp, 2006), parental divorce (D. L. Braun et al., 1999), involvement in sport (Crosscope-Happel et al., 2000), family overprotectiveness/enmeshment (Crisp, 2006), high psychiatric comorbidity (Bramon-Bosch et al., 2000; Carlat et al., 1997; Raevuori et al., 2008), gender identity concerns, and homosexuality (Austin et al., 2004; Bramon-Bosch et al., 2000; Carlat et al., 1997; Crosscope-Happel et al., 2000).
Trauma and loss in early life can set the stage for later behaviors that inadvertently distract from psychological pain and distress. As a consequence, eating disorders are often associated with a history of childhood physical abuse and neglect (Mitchell & Mazzeo, 2005), with males experiencing eating disorders reporting higher incidences of being beaten in childhood, mother–child abuse, and sexual abuse than noneating disordered men (Olivardia, Pope, Mangweth, & Hudson, 1995).
However, although traumatic and complex challenging events can have negative consequences for an individual, the potential for positive psychological growth is now recognized following a wide range of life events and distress (see Joseph, 2011). Furthermore, those experiencing ongoing distress from vicarious exposure to parental trauma as children, or partner trauma, have used those experiences to redefine their own lives positively (McCormack, Hagger, & Joseph, 2011; McCormack & Joseph, 2013; McCormack & Sly, 2013). This study is interested in both the positive and negative interpretations that influence individual eating patterns and behaviors in males.
Although research has found many similarities and differences in the presentation of eating disorders in males and females, the nature and extent of these presentations are little understood. As such, how individuals might positively or negative interpret these experiences is unknown. What we do know comes from research on populations mostly composed of adolescents and young adults, and theories that reference their developmental stage. Males who present with eating disorders in later life may exhibit a very different clinical picture and challenge clinical understanding of these debilitating conditions.
Qualitative methods are providing insight into the hermeneutic possibilities that individuals bring to both primary and secondary traumatic, painful, and chronic life events (Smith, Flowers, & Larkin, 2009), and this is relevant to research into early life trauma and late onset eating disorders. Therefore, the aim of this study is to explore the “lived” experience of a male with middle-age onset of an eating disorder. An in-depth, thematic analysis of a single life history case study was conducted to understand how the participant made meaning of this unique experience.
Method
Participant
Joseph (pseudonym), aged 45 years, was approached to participate in this case study given his unique understanding of experiencing an eating disorder in middle age. Joseph was provided with details of the research and informed consent was obtained. Ethical clearance was gained through the university. Joseph was born in England in 1965, the second of three children. When he was 8 months old, his older brother died of cancer. The family moved to Australia when Joseph was 5 years. At the time of the study, he was an information management professional who had developed a severe eating disorder at age 43 years and lost one third of his body weight in 7 months. No medical explanation was able to shed light on the weight loss. At that time, he sought psychological therapy for a period of 2 years and was diagnosed with an EDNOS. Joseph’s history taking revealed significant trauma as a child as well as experiences of depression and anxiety over his lifetime that was relevant to his diagnosis of EDNOS and treatment.
Procedure
In line with a life history method, data were obtained from several sources. First, an interview schedule was developed (Appendix A and B) for three 2-hour interviews that were conducted over consecutive weeks. A follow-up interview was conducted after transcribing to further probe interpretation and meaning (see Appendix C) The first interview, conducted in Joseph’s home, was composed of a series of open-ended interviews structured around Joseph’s life course, to maximize the breadth of information obtained (see Appendix A). For the second and third interviews, a supplementary interview schedule (see Appendix B) was introduced based on the Eating Disorder Questionnaire 9.0 (Mitchell, 2008), to obtain specific information about eating and weight-related behaviors. The follow-up interview probed for affective understanding of cognitive interpretations within the data (see Appendix C). Each interview was recorded on a digital voice recorder. Data from the interviews were transcribed verbatim. Second, Joseph provided written statements, including comments on the interview transcripts, and spreadsheets he had used to monitor his weight loss. Third, he completed an Eating Disorder Inventory–3 (EDI-3) and a self-report measure of psychological traits shown to be clinically relevant in individuals with eating disorders (Garner, 2004). An individual case study was chosen as the most suitable way of investigating the data that reflect a subjective continuum of events across a lifetime.
Epistemology
Epistemologically, this study relies on the philosophies of phenomenology, critical realism, and symbolic interactionism (Denzin, 1995) by describing the way in which the world of Joseph is socially constructed, interpreted, and understood around this unique phenomenon (Smith, 2004; Spinelli, 2005). As such, it provided a platform for exploring the complexities of a late onset eating disorder through a process of understanding and interpretation. As access to the individual’s world is always mediated, a critical realist position is a comfortable fit with symbolic interactionism, which is concerned with the way people: (a) act toward things based on their subjective meaning; (b) bring meaning to social interaction; and (c) interpret and modify fluid and ambiguous meaning.
Drawing on these philosophies, the authors sought the essence or the underlying meaning making of this participant’s subjective “lived” experiences relating to his late onset eating disabilities. The theories of trauma and growth influenced the interpretation of data and the development of the themes (V. Braun & Clarke, 2006). At the same time, the authors were challenged to reflect on their own subjectivity and knowledge of the phenomenon under investigation and to consciously recognize their own biases and presuppositions that may have interfered with interpretation of data (Gadamer, 1983; Heidegger 1927/1962).
Analytic Strategy
As there is a paucity of research into the experiences and life history affecting on late-onset eating disorders, a qualitative, Life History methodology was used (Cole & Knowles, 2001). The authors felt that this poorly understood phenomenon was best viewed through the subjective “lived” experience lens of the participant and thereby inform future research. It did not aim to offer generalizability or cause and effect. This method emphasizes the inner experience of individuals and its connection with the phases and events of their life course. The life history method is particularly suited to the study of eating disorders, where events across the life course, both positive and negative, (disturbances in early attachment, parental control and maltreatment, gender role orientation, and early learning about self-control, eating, and body shape and weight), have been proposed as predisposing factors for the development of a late onset eating disorder (Koskina & Giovazolias, 2010; McEwen & Flouri, 2009). Similarly, a life history approach allowed the participant to subjectively explore his experiences in multiple forms. It also provided a breadth of data that could be analyzed through a method of reduction to specific interactions, statements, and themes in search for all possible meanings.The interviews were structured around the phases of Joseph’s life. For each phase, Joseph was asked to report on his perception of the following experiences: activities, major events, relationships, physical and mental health, substance use; and his relationship with his body and with food, including weight, disordered eating, exercise, other weight-related behaviors and body image concerns.
Analysis and Results
Joseph’s perceptual narrative of his life journey and his relationship with eating was constructed from the information obtained in the interviews, written statements, and spreadsheets as well as a follow-up interview targeting the affective and cognitive elements of his experience. Joseph’s life may be conceptualized as comprising 10 distinct phases, some of which contain distinct subphases. The major phases are described in Table 1.
Ten Distinct Phases of Participant’s Life History.
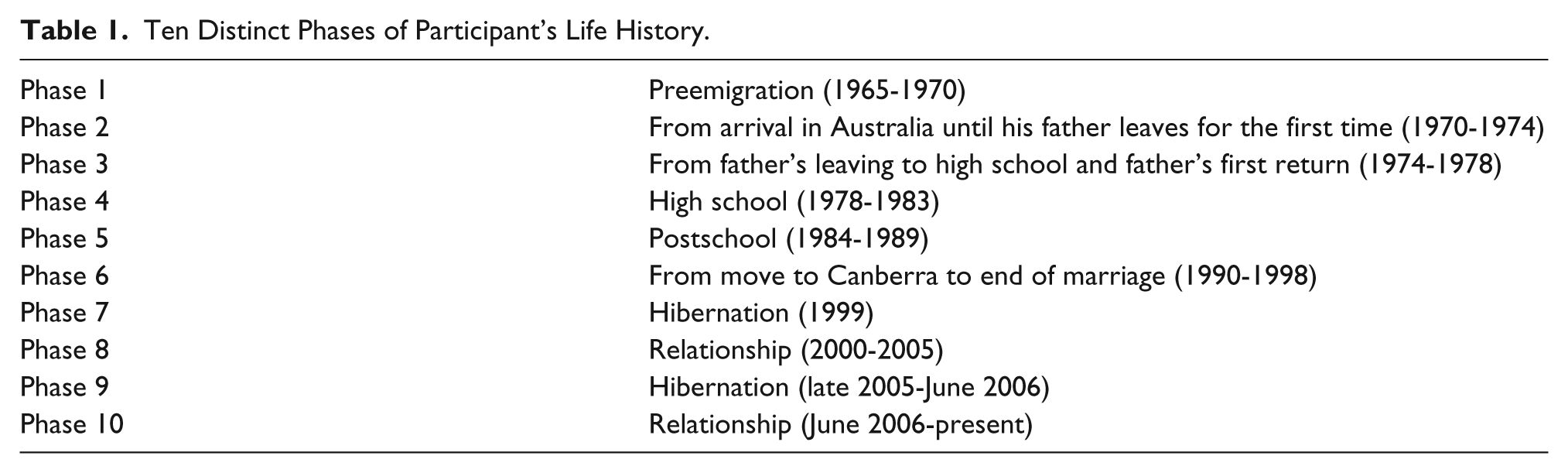
Three distinct themes emerged throughout these phases: Loss and Unworthiness, Becoming Bigger, and Wanting to Change. A theory of the origin and maintenance of Joseph’s eating disorder was developed and discussed in the context of both his beliefs and the emotional intensity with which those beliefs are experienced by Joseph.
Loss and Unworthiness
Joseph believed that early family of origin cumulative losses and negative early life events affected his feelings of unworthiness. From a personal narrative perspective, Joseph was able to recall events and family history. However, the intensity of his emotions left him feeling a “numbness” and “a mental block” when trying to bring meaning to his feelings around his parents’ treatment of him, particularly his father. In the earlier interview, Joseph was able to narrate the early life events that he believed influenced his sense of self, relationship patterns, and eating behaviors but was left struggling to make sense of that “numbness” and “mental block.” In the follow-up interview, the researchers explored Joseph’s beliefs in relation to his status in the family and based on his mother’s advice on his role as a family member. There were also certain emotional responses noticed as a consequence of these beliefs that remained over the years.
Trauma and Abuse/Becoming Invisible
The first experience of family loss Joseph believed influenced the way he viewed his importance within the family. He recognized this event as pivotal in learning to be “invisible” within the family while his parents were preoccupied with his terminally ill sibling:
You can just imagine that probably from the time I was born a lot of attention was placed on my older brother and taking him to hospital and things like that. And then of course in dealing with his death I imagine that things were not necessarily the happiest.
However, it is his memory of immigrating to Australia at 5 years of age that seems to consciously consolidate for Joseph, his need to be “invisible” and avoid drawing attention to himself. When leaving behind a supportive family network, he recalled being told that he would have to be good for his mother. Joseph came to value his mother’s self-sacrifice,
Her parents were still alive in England and she was an only child, so it must have been wrenching
and thereby came to believe that there was value in putting others’ needs ahead of his own needs. In emulating his mother, her perceived unhappiness was also something for him to embrace: “I don’t deserve to be happy.” Therefore, Joseph chose solitary activities or activities that benefited others rather than himself throughout his life. This included intimate relationships. For example, Joseph described that he found decision making difficult and waited to be directed in his current relationship: “I can’t do something just for me, that doesn’t sit right for me.”
Joseph’s father first left the family in Australia when Joseph was 8 years old. In the follow-up interview, Joseph explored the intensity of his feelings toward his father, particularly his memory of him as an angry, controlling, and emotionally abusive man whose needs came before others. Joseph was surprised by his response to this memory and reflected on how these childhood events affected his future eating habits. First, he described feeling devastated by his father’s departure. He believed he was the only one of his friends without a father and that he was not adequately socialized into the masculine role. He remembers that the usual solitary boy became “disruptive” at school:
All of a sudden I come home one day and Dad was gone. I think it was around Grade 3 or 4. That was around when I started getting comments on the reports about not joining in, about being a little disruptive.
While recounting these memories, Joseph became tearful and was visibly shaken stating that despite his efforts to remain “invisible” to his father, he had still left him. Despite its failure to gain his father’s care and love, he deliberately sought invisibility throughout his adolescence and adult life to keep him safe from emotional hurt:
I wanted to be invisible and unnoticed and not draw attention to myself.
When probed further on the origin of his feelings of invisibility, Joseph was able to recognize that the early life practice of remaining invisible to an abusive father had become life-long self-protective behaviors:
If I was quiet and invisible then dad would leave me alone.
Second, in recognizing that his fear of his father’s anger and abuse left him unable to challenge his father, he accepted his father’s abuse as his mother had self-sacrificed her needs. Joseph described his eating disorder as an “an obvious way of being invisible.” When he became emaciated: “If no one sees me, I can’t fail.”
Similarly, Joseph was asked how his father’s message to him as a child not only influenced his thinking as an adult but affected the intensity of his feelings. He described that feelings of abandonment and unworthiness plagued him during adult relationships and that partners left him just as his father had left him. He felt that his failure in adult relationships was driven by the inner voice of his father: “I don’t deserve to be treated well.” Furthermore, as the years passed and relationships failed, his father’s message that he had done something wrong and deserved to be punished was self-administered. These feelings were so intense that when Joseph felt bad about himself he would not only punish himself through eating or not eating, but would “often deliberately kick myself” or doing something that caused pain and injury.
Punishment/Worthless Adult
Unable to feel a sense of worth, “Like I was discarded as no good” his father’s legacy was an inaccurate account of himself. He believed he deserved punishment and self-harm became the vehicle:
I felt that dad leaving me and mum was punishment . . . Not eating, exercising until I feel pain and hitting myself are all ways I punish myself . . . I don’t deserve to feel good.
These beliefs continued throughout his life. His father’s comings and goings from the family and his mother’s health needs had reinforced the belief that he was unimportant and others’ needs were more important than his own:
Since as long as I can remember, I’ve never liked myself and don’t understand why others would like me either.
Fear of abandonment and rejection inhibited healthy adult attachment. In his adolescence, he was unable to talk with anyone about his feelings. When he finally sought counselling, his habit of prioritizing the needs of others often sabotaged his therapeutic work:
It is legitimate to do things for others but not for me.
Though Joseph’s father returned home two or three times while Joseph was in high school, the last return (when Joseph was 15 years and after his father had gone blind following a stroke) was the longest and most difficult for Joseph. Joseph recalled that his father was “irritable and intimidating.” The return of this invalidating “not good enough” message would plague him throughout adult life.
Joseph was surprised that he felt relief when at 16 years of age his father left for the last time. However, equally surprising to Joseph, self-loathing and feelings of guilt emerged. He recalled the impact of this final assault that led him to resort to excessive eating in an attempt to sooth these negative feelings. As his weight began to escalate, unwanted attention was drawn to his appearance and behavior at school. “Invisibility” was challenged. He frequently sought to avoid school by feigning, and then inducing, illness. Over time, inducing vomiting became an automatic response to stressful situations:
“. . . had a massive plate of food and pigged out until I was sick.
Shame and self-harm became partners for validating feelings of unworthiness. “Deliberately going out in the rain and exacerbating injuries” was becoming a regular practice. He stated that he did these things partly to “feel something, partly to experience pain like the pain other people experience and partly to seek attention,” but with the intention of not getting attention, and thereby proving that he was not worthy of attention. In adult life, Joseph continued to hurt himself through hitting and injuring himself to feel something negative: I feel guilty if I feel good . . . I don’t deserve to feel good.
Unable to Connect/Becoming Isolated
Toward the end of high school, Joseph discovered that his preferred career path was closed to him. This reinforced his belief that he had no control of his life. Early attempts at relationships with girls were equally unsuccessful. He did have one significant 18-month relationship with a woman 8 years his senior. However, feeling a sense of loss and hurt when it ended, he remembered thinking that it was best not to become too attached to anyone or anything.
Joseph spent a year on unemployment benefits after which he went to university and studied psychology. Though he graduated, from the course he concluded that he was not fit to help people, and was again unemployed for a year. When asked about his current employment and whether he enjoys it, Joseph stated he doesn’t enjoy it at all but “couldn’t let people down” by changing careers or his role. He explained that he really struggled to see how further study that would benefit him could be justified as benefiting others was the only way change would make it legitimate to him.
Joseph reported that he has always thought he was overweight and probably has been overweight for most of his life. However, throughout his childhood and youth, his eating was unremarkable: he ate regular meals, occasionally overindulged, and occasionally skipped a meal. It was not until he began to study at university that Joseph started using diet pills to control his weight, and had a brief episode of starvation when, unable to face a woman with whom he had had a relationship, he isolated himself in his room and spent a week consuming nothing but appetite-suppressing fiber drink. He believed that if he was thinner he may be less repugnant and might stand a chance in relationships.
These intense episodes resurrected the dichotomous feelings of hope and invalidation that he had experienced with his father. He described it as a seesaw feeling and an “inability to read messages” reinforcing isolation and an “inability to connect.” In these early relationship attempts, he felt unable to advocate for his own needs and in a follow-up interview recognized that he participated in a revolving and powerless situation similar to that with his father:
Do you want to come over tonight? . . . I don’t want to see you again.
Joseph remembered internalizing this as him doing “something wrong.” He recalled that these intense feelings were expressed through isolation and poor self-care. Joseph retreated to his university room alone and “effectively spent a week where I couldn’t eat a thing.” After a week, he collapsed in class and started eating again.
Unable to connect in a meaningful relationship, his sense of isolation intensified. He now entered a period where he stopped trying to please others with his appearance. He stopped using diet pills and paid little attention to his presentation. He reached 90 kg (body mass index [BMI] 29.4), his maximum weight to that time, and then dropped to 85 kg (BMI 27.8) after he injured his back playing hockey. Joseph’s sense of isolation escalated leaving him feeling again that he deserved to be punished.
Becoming Bigger
At 25 years of age, Joseph joined the Public Service. He has spent most of the time since working with data, has completed further postgraduate degrees, and for much of the past 20 years has defined himself by his work.
Joseph remembers that during much of this time he felt worthless and unlovable. Becoming bigger was a form of acceptable punishment: “Why should I take care of myself?.” In a follow-up interview, Joseph reaffirmed that becoming bigger at this stage of life helped him remain invisible and isolated. But he was also becoming conscious of the complexity of his behaviors and how they inhibited social engagement and change. He recognized that he was “invisible at work” too much of the time, not engaging with others socially and trying to stay “under the radar.” He reported that he had wanted to change roles and do something more interesting but was unable to because “that would mean drawing attention to myself.” It would also challenge his beliefs: “doing something that I enjoy.” During the follow-up interview, he was able to muse over the dilemmas he had so often faced:
. . . I have a real problem with doing things just for myself . . . I might also let [my workplace] down [by leaving].
At the end of his first year in the public service, Joseph entered a relationship and married Karen (a pseudonym) a year later. He recalled that before long, he and his wife developed different interests and lived separate lives. Joseph felt “trapped” in an unhappy marriage. On further probing, Joseph stated that at the time he was unable to leave even though he knew he was unhappy because earlier life practices of being invisible and not prioritizing his own needs sabotaged his actions:
. . . if I just stayed out of the way, it was ok . . . I was waiting for her to make the decision to leave.
He cooked to express himself, overindulged on food and alcohol, and put on weight. By the end of the marriage Joseph weighed 100 kg (BMI 33.0). In a later interview, he again recognized this “overeating” as a form of “self-harm and punishment for not being good enough.” With insight, he also recognized that the marriage had supported his self-abuse and disclosed that his drug and alcohol problems started during this relationship as “she was” his main supplier:
It wasn’t good for me to be with her and I see that now.
Joseph had made no attempts at intake restriction or compensation, and his weight continued to accelerate to 110 kg (BMI 36.3) when he moved in with Karen. Joseph described his relationship with Karen as “unhealthy.”
It was always one of those situations where I couldn’t win. I have never wanted to be where I wasn’t wanted and so when she handed me this letter (to leave), after getting over the initial shock, I went “Oh right then”. . . . “Right, you want me to move out, then fine, OK” but apparently I was supposed to fight . . . It was not a very healthy relationship.
His harmful eating, drinking, and smoking cannabis continued to increase when he was alone. By the end of the marriage, he was bingeing at least twice a week and probably met criteria for BED. His weight increased to 120 kg (BMI 39.6) and he made halfhearted attempts to lose weight without changing his eating. Joseph reported that when Karen “kicked him out,” he was ready to leave. He recognized a pattern in relationships. Similar to his previous relationship, he had felt unhappy in the marriage for some time but was waiting for the other person to make the decision. Negative self-talk would contribute to indecision. Without healthy strategies to manage this, Joseph used drugs and alcohol to switch off and “escape my head.”
Joseph moved out and spent 8 months alone. He felt out of control in most aspects of his life. He was overeating, drinking two thirds of a bottle of spirits (16 standard drinks) two to three times a week, and smoking cannabis every night. By May 2006, Joseph weighed 125 kg (BMI 41.3) and experienced chest pain and tachycardia. He consulted his general practitioner who warned that he was “heading towards an early grave.” Shortly afterward, Joseph fell down the stairs at home and, as he lay on the floor, he decided it was time to seek help to change his life patterns. Unfortunately, the focus remained one of focus on others and “not be a burden on others” rather than one of self-care and worthiness.
Joseph’s desire to change at that time was short-lived. He moved out of the marriage and “hibernated,” living on takeaway food, alcohol, and cannabis. Joseph’s mother died in this year after a short illness. He described losing her as the worst thing that he had ever been through. She was the only person with whom he had had an ongoing and meaningful relationship:
The one person I would never want to disappoint or cause waves or trouble for was no longer there and I was scared of whom or what would hold me accountable now.
Joseph stated he felt overwhelmed with sadness at the loss of his mother. He was also overwhelmed with “numbness” in regard to himself. When asked to explore how feeling overwhelmed with sadness and numbness could coexist, he was able to describe sadness as a physical feeling that linked him to self-destructive behaviors. The combination of self-harming and negative feelings maintained and legitimized beliefs of poor self-worth:
to legitimie how badly I was feeling about myself . . . if I had a physical injury, I could feel pain . . . and that was acceptable to me.
Numbness, on the other hand, disallowed acceptance and a right to honor his own distress. On further questioning, Joseph stated that he felt and still feels great loss even to this day. The one person whose needs he had prioritized over his own had taken his sense of purpose. He described that feeling of “underlying sadness” as a “lost sense of purpose.” He was not able to determine if that explained the way he felt as an adult toward himself, seemingly having a psychological protective barrier to this way of thinking stating “that’s too much for me to get my head around.”
Wanting to Change
Joseph started seeing Sally (pseudonym) in June a year later. Sally was 8 years older than Joseph. He described her as solid and strong, and the relationship as good and stable. Sally encouraged and supported Joseph to lose weight. His initial self-directed efforts achieved some success until his weight plateaued at 117 kg (BMI 38.6). Joseph joined a weight loss program the following year. Four months later, Joseph weighed 93 kg (BMI 30.7) but the weight loss company ceased operations. Disillusioned, Joseph stopped trying to lose weight temporarily.
The following year, at 43 years of age, Joseph weighed 94.4 kg (BMI 31.2). He commenced an intensive, self-directed weight loss program combining a strict, calorie-controlled diet with intensive exercise. Joseph revised his targets as he reached them. His initial target of 85 kg became 80 kg in July 2008 and 75 kg in August 2008. Achieving targets clearly increased the momentum for further weight loss. In January 2009, Joseph achieved his minimum weight of 63.4 kg (BMI 20.9) and experienced dizzy spells and lack of energy. Joseph saw a sports nutritionist who advised him to eat more carbohydrates. When Joseph demurred, the nutritionist referred him to eating disorders therapy. Although Joseph’s minimum BMI was in the healthy weight range, this period of weight loss most closely resembles anorexia nervosa restricting type in that Joseph maintained a strict discipline and was in close control of his food intake and continually revising down his weight goals. It is likely that he would have kept going if he had not experienced debilitating physical symptoms related to his weight loss. Joseph self-diagnosed anorexia nervosa and began therapy a year later. His therapist also diagnosed depression, which she manages jointly with his general practitioner. Joseph reported past episodes of apparent social phobia and depression (neither of which was formally diagnosed) and no family history of mental illness. After 12 months in therapy, Joseph has put on 15 kg.
Initially, Joseph continued to believe he was not worthy of help or prioritizing his needs. He made the comment, “I don’t know why I should feel better . . . what right have I got . . . I can’t justify feeling better for me.” It was through therapy that he started to change these beliefs and see that he did have a right to be happy. With much effort and support, he began to give himself permission to enjoy activities. He was unable to completely separate his needs and others needs; however, he found ways to combine others’ and self-needs. He started playing a musical instrument and played for pleasure believing that this would bring happiness to both Joseph and his new partner. Although he was able to now connect with his own right to be happy, it was still important for others’ needs to be met.
Joseph moved in with Sally in the following year. He disclosed to Sally his long history of eating disorder and depression and states that she has been very supportive and understanding. Joseph’s eating pattern have improved to some degree, usually having two main meals each day. Living with Sally has restricted his ability to engage in disordered food-related behavior. However, he remains unable to be totally open to Sally. If she is not home, he does not eat disguising this from Sally. He often pretends to eat when she is there. In therapy, he is more open. Joseph explained that he eats little in public and restricts his food intake through small portion sizes, skipping meals, and avoiding foods high in fat, carbohydrates, or calories. Joseph uses a variety of compensatory behaviors. He goes to the gym four to five times a week for 1 to 2 hours cardio workout to control weight and still uses diet pills. Joseph had not vomited for weight loss before past year. He vomited for 2 weeks past year and throughout March this year. The vomiting began when one day he swallowed instead of spat and decided to see “what all the fuss was about.” He still occasionally vomits. He has vomited twice in the past month but says that he prefers not to as he finds it distasteful and difficult to conceal.
Joseph reported that the work he is doing with his therapist has saved his life and sanity. He still hates his weight and shape, which greatly influence how he feels about himself. He hates looking in mirrors and at photos and weighs himself every morning. While he remains unhappy with the numbers, he knows he has more energy and is thinking more clearly, and notices deterioration in energy and cognition when he does not eat well. Joseph is trying to eat regularly, think less about food, and avoid vomiting. Having identified as a person with an eating disorder, Joseph has investigated both proanorexia and prorecovery websites. The proanorexia sites have increased his repertoire of disordered behavior.
He is disappointed with the role alcohol has played in his weight increase. He explained that when consuming one glass of wine a week, his weight went below 65 kg. Joseph currently drinks up to three quarters of a bottle of red wine (five to six standard drinks) per night. He finds it easier to eat when he has been drinking as it lowers inhibitions and either generates, or allows him to feel, hunger. Joseph stated that he finds the correlation disturbing because he does not want to be reliant on alcohol to relax or to enable him to eat. “If I do want to eat I want to be able to do it myself.” He fears he has gained weight only because of his drinking. Part of his feeling uncomfortable with his current weight is that, in part, it represents loss of control.
Joseph returned a valid result on the EDI-3. His scores on all scales with the exception of Body Dissatisfaction and Maturity Fears were in the elevated clinical range, meaning that they were between the 67th and 99th percentile for the U.S. Adult Combined Clinical sample (composed of adult females with eating disorder diagnoses). Body Dissatisfaction was at the 66th percentile and Maturity Fears at the 51st percentile. These results indicate a high degree of both eating disorder symptoms and general psychological maladjustment. Joseph scored at the 67th percentile on the Drive for Thinness scale and at the 87th percentile on the Bulimia scale. His highest score was on the Interpersonal Insecurity Scale, which assesses discomfort, apprehension, and reticence in social situations, at the 99th percentile. He scored at the 97th percentile on Interoceptive Deficits, which measures confusion related to accurately recognizing and responding to emotional states. High scores on this scale have been associated with poor progress in follow-up and predictive of self-injury in patients with bulimia nervosa. His score on the Asceticism scale is at the 96th percentile (Garner, 2004). These scores are consistent with Joseph’s reported history. Based on interviews and the results of the EDI-1, Joseph met the criteria for EDNOS as per the DSM-IV-TR criteria (American Psychiatric Association, 2000).
Joseph is now able to speak more consciously about feeling depressed and the strong connection he experiences with physical hurt and negative feelings. He recognizes his strong desire to self-harm is linked to feeling pain, which allows him to “legitimize” his psychological suffering. Getting help meant sitting with the intense feelings of unhappiness and wanting to self-harm yet not act. Therapy slowly untwined this strong connectedness and allowed feelings to be experienced separately to physical suffering. It took Joseph several years of therapy to reduce the intense feelings of the need for pain and suffering and recognize and enjoy feeling happy and well.
Unconditional self-regard was a difficult concept for Joseph. He reported that his biggest struggle in therapy had been doing things for himself. “I feel uncomfortable with this concept.” He stills struggles to view others’ needs as more “legitimate” than his own. Similarly, he finds it difficult to set goals in seeking help that do not include benefit for his partner. On further interviewing sometime after his initial interviews, Joseph was able to realize that his hardest struggle is
being able to do things solely for me . . . I need to learn how to be happy for me, not for other . . . I know this now . . . but that is hard, a real hard battle which will take me some time.
Joseph reported that he is still undergoing therapy and that he acknowledges that he
still (has) a lot of work to do . . . I have to change my thinking about myself or I’ll never be happy . . . I have and always will struggle with doing things for me . . . but it is getting easier with help from those I know care about me (referring to his therapist and partner).
Discussion
This life history thematic analysis has shed light on a relatively unknown eating condition occurring in males. In particular, it highlights that late-onset eating disorders are possible in males and that thorough attention to gathering an early life history in relation to current distress levels in this cohort may be therapeutically beneficial. Apart from a tipping point that may have precipitated an eating disorder after 40 years of age, this study suggests that positive support may assist a growthful redefinition of self around worthiness and eating, including seeing oneself as legitimate and worthy of happiness.
A Tipping Point
For many years, Joseph had several risk factors for eating disorders identified in previous research: parental divorce; parental emotional abuse and control; gender role confusion; family overprotectiveness/enmeshment; overweight, body dissatisfaction, and negative affect. However, this case contributes to the literature in that the participant did not develop an eating disorder until at least his late 30s when he probably met criteria for BED in the context of an unhappy relationship. Onset of binge eating in response to negative affect is supported in the literature (Stice, 2002) and often occurs well into adulthood (Striegel-Moore & Bulik, 2007). Joseph did not attract clinical attention until, at age 44 years, he sought treatment for an eating disorder closely resembling restricting anorexia nervosa in the context of premorbid obesity, dieting, and health concerns, an important contributor and trigger for older-onset patients.
Although psychological distress can negatively affect dieting and binge eating, a more at-risk group may be those who rely on moderate or intermittent dieting to relieve distress (Grilo, Masheb, & Wilson, 2001). As such, an individual may have many risk factors for eating disorders without exhibiting obvious or regular behaviors. In this case study, the onset of an eating disorder became apparent only in later life despite early life distress and highlights the externalisation of distress may well be disguished through a complex interaction of risk and protective factors. The authors suggest that a tipping point for the externalization of distress in the form of an eating disorder may be reached when an existing risk factor becomes of sufficient intensity, possibly in the context of other stressors (e.g., negative affect in combination with obesity), or new factors emerges (e.g., support from a significant other to lose weight, dieting success, health concerns). The death of Joseph’s mother may have heralded such a tipping point.
It is likely that the illness and death of Joseph’s older brother when Joseph was 8-months old caused significant stress in his family leading to unavailability of his primary caretaker/s, and consequent early attachment development difficulties (Bowlby, 1973). Joseph’s history provides ample evidence of a disturbance of attachment: his difficult relationship with his father, his idealisztion and emulation of his mother, and his relational difficulties with females during adolescence and adulthood. His restrictive eating at times of relational difficulty suggests a complex link between attachment and eating disorders. Without robust positive self-regard, feelings of unworthiness maintained his self-harm behaviors and inhibited change that would increase feelings of self-worth. However, despite his early life distress, this study highlights that positive support from significant others and/or therapists may have contributed to positive change and a redefining of self-care, particularly when a tipping point event in life triggers self-exploration. Of therapeutic importance is that despite years of poor interrelational interactions cumulative on early life trauma and abuse, positive psychological support has contributed to positive change for Joseph.
Future Research
Future research is needed concerning the role of attachment, trauma, and abuse in eating disorders where onset occurs in later life. This study supports a number of established risk factors and has also raised a number of issues that have previously received little attention. Of note are self-induced illness in anxious avoidance, particularly in light of early life trauma, abuse, and disrupted attachment; significant relationship changes; and opportunity to engage in disordered behavior. Further case studies exploring delayed onset in males could assist in isolating critical risk factors specific to gender.
Strengths and Limitations of the Study
The methodological approach of this study has allowed the researchers to access a broad range of information and potentially explore issues not canvassed in previous research. Examining a single case in detail encouraged the participant to explore deeper meaning making at times; however, depth of meaning was sometimes limited because of the participant’s reticence to explore more deeply.
The major limitation of this study is the dependence on memory (which can often be unreliable) of only one person over a lifetime. However, by allowing Joseph to provide input in various ways: interview, written statements, spreadsheets contemporaneous with his weight loss, and the EDI-3, the researchers have been able to cross-reference memory to a greater or lesser degree.
Though qualitative case studies do not offer generalizability or cause and effect, they can generate hypotheses for further investigation. As such, they offer the opportunity to explore previously poorly researched phenomena and complement the extant quantitative literature.
Suggestions for Clinical Practice
This study has highlighted several points of significance for clinical practice. Clinicians treating clients for obesity need to be aware of the potential for eating disorders to develop at any stage of the life cycle. For example, in weight loss programs that monitor progress particularly in a group setting, patients could make extraordinary efforts to perform well to gain praise, or avoid disapproval, or to satisfy their own perfectionistic standards (e.g., starving themselves for a day or two because of an obsessive need to be lighter). Weight loss programs should be required to insure that participants’ mental health, particularly any eating pathology, is thoroughly assessed before they commence on any program accompanied by regular monitoring of mental health throughout the program.
Clinicians treating clients with eating disorders need to be aware of the importance of both positive and negative interrelational influences that affect eating habits and particularly those that may trigger past traumatic events and avoidance behaviors. This is particularly important when there is a trauma history, especially betrayal trauma. A full trauma history may allow traumatic memories’ verbal expression, so that they can be retrieved from autobiographical memory as required. Without the opportunity to narrate, traumatic memories may be stimulated by unexpected events maintaining behaviors that although protective at another time in life, may reinforce feelings of blame, shame, and ongoing psychopathology.
Finally, therapists need to be alert to the possibility that late onset eating disorders may be more prevalent in males than previously recognized particularly if there is a history of early life loss and trauma, the client is overweight, and/or has chronically presented with associated and persistent psychopathology throughout life.
Footnotes
Appendix A
Semistructured Life Circumstances Interview Outline.
| We will begin by getting an idea of who you are now, how you fit into the world, and your relationship with your body. |
| At this stage, I would also like to get an outline of your history. |
| Later we will go back over your history to better understand your lived experience at different times of your life and how that was affected by events in your life at those times. |
| Looking back over your life, can you identify any distinct phases, that is, times when your life had a certain consistency that was different from that following some change or transition. For example, most people would consider that their life changed in a major way when they started or left school, or lost a parent, starting or losing a job, or a relationship could also be a boundary between phases of life. |
| Overall, how do you feel about your life as it is now? |

Appendix B
Supplementary Structured Interview in Relation to Current Relationship With Body and Eating and Weight-Related Behavior.
| We will now turn to your current relationship with your body and a brief history of your eating and weight-related behavior. |
| Weight history |
| How much do you weigh now? |
| How tall are you? |
| How much would you like to weigh? |
| What was your highest weight since age 18? |
| How old were you? |
| What was your lowest weight since age 18? |
| How old were you? |
| What was your highest weight between ages 12 and 18? |
| How tall were you? |
| How old were you? |
| What was your lowest weight between ages 12 and 18? |
| How tall were you? |
| How old were you? |
| How do you feel about your current weight and shape? |
| How much do you fear gaining weight? |
| How important is your weight and shape in affecting how you feel as a person? |
| How do you feel about different parts of your body? |
| On average, how often do you weigh yourself? |
| Dieting behavior |
| On average, how many main meals do you have each day? |
| On average, how many snacks do you have each day? |
| Are there any foods you try to avoid in order to influence your shape or weight? |
| If so, what foods? |
| Have you ever been on a diet, restricted food intake, and/or restricted the amounts or types of food eaten to control your weight? |
| (If NO, go to Binge eating behavior) |
| At what age did you first begin to diet, restrict your food intake, and/or reduce the amount or types of food eaten to control your weight? |
| At what age did you first begin to diet, restrict your food intake, and/or reduce the amount or types of food eaten to lose weight? |
| Over the last year, how often have you begun a diet that lasted more than 3 days? |
| Over the last year, how often have you begun a diet that lasted 3 days or less? |
| What are your preferred ways of dieting? |
| Have you ever used a supervized diet program? |
| What programs have you used? |
| How old were you? |
| Weight at beginning? |
| Weight at end? |
| Have you ever used medication for obesity? |
| What medications have you used? |
| How old were you? |
| Weight at beginning? |
| Weight at end? |
| Have you ever used psychotherapy for eating problems, weight loss, or weight gain? |
| How old were you? |
| What forms of psychotherapy? |
| Weight at beginning? |
| Weight at end? |
| Have you ever used psychotherapy for eating disorder? |
| What forms of psychotherapy? |
| How old were you? |
| Weight at beginning? |
| Weight at end? |
| Have you ever used medication for eating problems/weight problems? |
| What medications and what doses? |
| How old were you? |
| Have you ever used a self-help group? |
| How old were you? |
| Have you ever had a surgical procedure to change your weight or body shape? |
| How old were you? |
| Weight at beginning? |
| Weight at end? |
| For each diet with major weight loss |
| How old were you? |
| Weight at start? |
| Weight at end? |
| Type of diet? |
| Have you ever had significant physical or emotional symptoms while attempting to lose weight or after losing weight? |
| If Yes, describe your symptoms, how long they lasted, if they made you stop your weight loss program, and if they made you seek professional help. |
| Binge-eating behavior |
| Have you ever had an episode of binge eating characterized by |
| (a) eating, in a discrete period of time (e.g., within any two hour period), an amount of food that is definetely larger than most people eat in a similar period of time? |
| (b) a sense of lack of control over eating during the episode (e.g., a feeling that one cannot stop eating or control what or how much one is eating)? |
| (If No go to Weight-control behaviors) |
| Please indicate how characteristic the following symptoms were of your binge eating. Options: Never, Rarely, Sometimes, Often, Always |
| (a) feeling that I can’t stop eating or control what or how much I eat |
| (b) eating much more rapidly than usual |
| (c) eating until I feel uncomfortably full |
| (d) eating large amounts of food when not feeling physically hungry |
| (e) eating alone because I am embarrassed by how much I am eating |
| (f) feeling disgusted with myself, depressed, or very guilty after overeating |
| (g) feeling very distressed about binge eating |
| How old were you when you began binge eating? |
| When did binge eating start to occur regularly, on average at least 2 times each week? |
| What was your height and weight at this time? |
| What is the total duration of time you had a problem with binge eating? |
| Weight-control behaviors |
| Vomiting |
| Have you ever self-induced vomiting after eating in order to get rid of food eaten? |
| (If NO, go to Laxatives) |
| How old were you when you induced vomiting for the first time? |
| How old were you when you first induced vomiting on a regular basis (on average at least two times each week)? |
| How long did you self-induce vomiting? |
| Laxatives |
| Have you ever used laxatives to control your weight or “get rid of food?” |
| (If NO, go to Diuretics) |
| How old were you when you first took laxatives for weight control? |
| How old were you when you first took laxatives for weight control (on a regular basis on average at least two times each week)? |
| How long did you use laxatives for weight control? |
| What type and amounts of laxatives have you used? (Indicate all types that apply and the maximum number used per day) |
| Diuretics |
| Have you ever used diuretics (water pills) to control your weight? |
| (If NO, go to Diet pills) |
| How old were you when you first took diuretics for weight control? |
| How old were you when you first took diuretics for weight control (on a regular basis, on average at least two times each week)? |
| How long did you use diuretics for weight control? |
| What type and amount of diuretics have you used? (Indicate all that apply and the maximum number used per day.) |
| Diet pills |
| Have you ever used diet pills to control your weight? |
| (If NO, go to During the entire LAST MONTH) |
| How old were you when you first took diet pills for weight control? |
| What amounts and types of diet pills have you used in the last month? |
| During the entire LAST MONTH, what is the average frequency that you have engaged in the following behaviors? |
| Binge eating |
| Vomiting |
| Laxative use to control weight |
| Use of diet pills |
| Use of diuretics |
| Use of enemas |
| Use of Ipecac syrup |
| Exercise to control weight |
| Fasting (skipping meals for entire day) |
| Skipping meals |
| Eating very small meals |
| Eating meals low in calories and/or fat grams |
| Chewing and spitting out food |
| Rumination (vomit food into mouth, chew, and reswallow |
| Saunas to control weight |
| Herbal products (“fat burners”) |
| During any 1-month period, what is the HIGHEST frequency that you have engaged in the following behaviors? |
| Binge eating |
| Vomiting |
| Laxative use to control weight |
| Use of diet pills |
| Use of diuretics |
| Use of enemas |
| Use of Ipecac syrup |
| Exercise to control weight |
| Fasting (skipping meals for entire day) |
| Skipping meals |
| Eating very small meals |
| Eating meals low in calories and/or fat grams |
| Chewing and spitting out food |
| Rumination (vomit food into mouth, chew, and reswallow |
| Saunas to control weight |
| Herbal products (“fat burners”) |
| Exercise |
| How frequently do you exercise? |
| If you exercise, how long do you usually exercise each time? |
| If you exercise, please indicate the types of exercise you do (fill in all that apply). |

Appendix C
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.