
Abstract
Veterans comprise 10% of the population, and suicide among Veterans has garnered national media and policy attention. Existing research suggests that intimate partner violence (IPV) is a risk factor for suicidal behaviors among some high-risk populations. This report offers a new perspective: the intersection between Veterans’ suicidal thoughts and IPV, both victimization and perpetration. The data were obtained from a northeast telephone survey of Veterans (n = 296) using Veterans Health Administration services and yielded a 27% participation rate. Findings suggest male Veterans who are IPV involved have increased odds of suicidal thoughts and behaviors.
The Department of Veterans Affairs and Department of Defense have allocated myriad resources to addressing suicidal burdens among those who serve, or have served, in the U.S. military. These efforts include a national toll-free crisis line (Knox, Kemp, McKeon, & Katz, 2012), targeted public awareness campaigns (Katz, 2012), and expansion of mental health services. However, suicide rates for those who use Veterans Health Administration (VHA) services exceed rates found in the U.S. general population (Blow et al., 2012). Overall, rates of suicide among those who use VHA services were highest among males between 30 and 64 years of age (Blow et al., 2012). Despite evidence of excess risk, comparatively little is known about the relationship between nonclinical risk factors and suicide.
Intimate partner violence (IPV) is a risk factor for suicide among individuals in community settings, clinical facilities, and social services agencies (Berrios & Grady, 1991; Heru, Stuart, Rainey, Eyre, & Recupero, 2006; Kaplan, Asnis, Lipschitz, & Chorney, 1995; Kaslow et al., 1998; McCauley et al., 1995; Rees et al., 2011). Male IPV victims report higher rates of depression and posttraumatic stress disorder (PTSD) than non-IPV-involved males (Cerulli, Bossarte, & Dichter, 2014; Straus et al., 2009), and the rates of male victims may be higher than previously recognized.
In one study, 30% of males drawn from a sample of private insurance records reported lifetime victimization, and 20% reported physical violence in the past year (Reid et al., 2008). In a recent national telephone survey, 5% of males reported IPV abuse within the past year compared with 5.9% of females, and 28.5% of men reported that they had experienced stalking, rape, or physical abuse in their lifetime (Black et al., 2011). Few studies to date have reported on male Veteran IPV victimization, with a recent report indicating that among those who participated in a community-based telephone survey, male Veterans were less likely than non-Veterans to report IPV (9.5% vs. 12.5%; Cerulli et al., 2014). Furthermore, Veterans who were IPV involved had two times the risk for depression and smoking (Cerulli et al., 2014). In another recent study, IPV emerged as a risk factor for suicide ideation among a sample of U.S. Air Force members, most of whom were male (Langhinrichsen-Rohling et al., 2011).This current study further examined male Veterans’ IPV status in relation to their suicidal thoughts to assess whether IPV was associated with increased odds for suicide ideation and attempts. The study hypothesis proposed that IPV involvement would be associated with increased suicidal thoughts and behaviors.
Method
Data were collected via a telephone survey conducted among a simple random sample of male Veterans enrolled for VHA services in upstate New York. The research staff was composed of the preliminary investigator (author RB), a PhD in sociology, and multiple research assistants. All research assistants participated in formal training in survey research methods as well as human subjects protection. The Veteran Affairs Medical Center provided institutional review board approval.
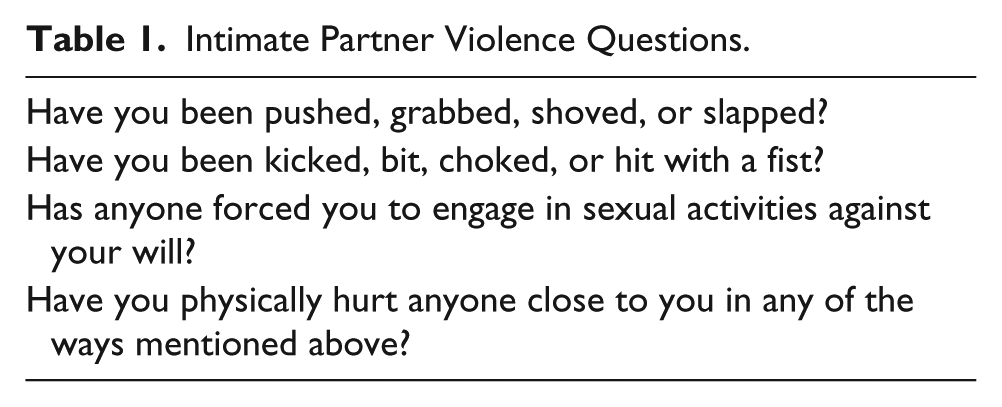
Research staff reached 1,102 out of 3,010 Veteran households, and 296 agreed to participate, resulting in a 27% participation rate. Subjects were offered a $5.00 incentive for their contribution. Data were collected between June 2010 and January 2012 and included 28 questions about suicide and a broad range of risk factors, including IPV. The data comprise all self-report information, and the research team did not use standardized measures to validate participants’ self-report for mental health diagnoses. Suicide questions explored whether the respondent had ever thought about, planned, or attempted suicide. IPV was assessed via questions about perceived safety at home regarding firearms, and lifetime psychological and physical abuse. One question assessed perpetration. Table 1 provides the IPV questions that were asked.
Intimate Partner Violence Questions.
The sample was bifurcated by IPV, involved or not, if the respondent answered any of the IPV questions affirmatively. The dependent variable, suicidal thoughts, was coded dichotomously if someone endorsed ever having considered suicide. Chi-square and Fisher’s exact tests were used to investigate associations between covariates and IPV. Logistic regression explored risk factors that increased the odds of suicidal thoughts. Due to concerns about multicollinearity among the variables, the final model included age and IPV and is presented as the best model fit with main effects only.
Results
The sample was composed of 296 males. Their mean age was 64 years (SD = 13.93), and they were mostly White (n = 284, 95.9%). Many of the participants were married (n = 193, 65%) and retired (n = 154, 52%). Slightly more than a third of the cohort had PTSD (n = 108, 36.5%), but few endorsed having other psychiatric burden (n = 28, 9.5%). For a more detailed description of the sample, see Table 2.
Sample Description and IPV Status (N = 296).

Note. IPV = intimate partner violence; FET = Fisher’s exact test; PTSD = posttraumatic stress disorder; MH = mental health; SA = sexual assault.
Only asked of individuals who endorsed suicide thoughts. .05=*, .01=**, .001=***
Fifty-three out of 296 participants (17.9%) reported IPV involvement, with only one Veteran reporting perpetration in isolation of victimization. Those reporting IPV involvement were more likely to be unemployed (χ2 = 39.73, p < .001), to have been deployed to Iraq or Afghanistan (χ2 = 9.57, p < .01), and to have diagnoses of PTSD (χ2 = 27.53, p < .001) or other psychiatric illnesses (χ2 = 21.67, p < .001).
IPV-involved Veterans reported suicide ideation almost three times more than those who were not (32 [60.4%] vs. 55 [22.6%], χ2 = 29.87, p < .0001, phi = .3177). Of those who endorsed suicide ideation, IPV involved individuals were more than twice as likely to have attempted suicide (31.25% vs. 16.98%, odds ratio [OR] = 2.22, confidence interval [CI] = 0.79, 6.26). IPV-involved Veterans were over three times more likely to be in mental health and substance abuse counseling than non-IPV involved Veterans. The multivariate logistic regression, controlling for age, revealed that IPV-involved individuals were 4.5 times more likely to have suicidal thoughts (OR = 4.51, CI = 2.40-8.64), with the probability declining with age. Although age was significant, it was not practically significant (OR = 0.98, CI = 0.96, 0.99).
Discussion
Findings support the hypothesis that IPV involvement is associated with suicidal thoughts among male Veterans. Much of the discussion about male Veteran IPV has involved perpetration, but this sample identifies the rate of IPV victimization is almost 18% with only one participant reporting perpetration without victimization, which warrants further attention. This finding suggests that the typology of common couple violence, which is bidirectional, may apply to Veteran populations (Johnson, 1995). Respondents’ participation in counseling indicates that they are linked to services that might incorporate IPV screening.
As with all studies, certain limitations warrant caution in interpreting the results of the cross-sectional data. The data collection methods impeded our ability to assess and interpret sexual victimization. Additionally, the low participation rate (27%) may limit generalizability of results, as well as a small sample size limited to one state. The authors have no way to estimate the sample bias. Other considerations include the use of self-report data, and that IPV perpetrators may be likely to underreport both their victimization and mental health burdens. The survey was a total of 28 questions that were not tested for alpha coefficient given the unique nature of each question. Last, because this is a cross-sectional study, the authors are unable to assess for causality and whether suicidal thoughts and behaviors preceded IPV, or vice-versa. This warrants further exploration.
Male Veterans face psychosocial uphill battles postdeployment. These include returning from war to altered family dynamics, lost job opportunities, and a disconnectedness from individuals they served with during their deployment. These factors could affect Veterans’ self-esteem and self-perceptions regarding their place in their postdeployment worlds, and consequently lead to depression and mental health risks for suicide. While much is known about Veteran suicide and suicide attempts, little is known about whether there is a causal relationship between Veterans’ IPV involvement and suicidal thoughts and behaviors. A potential causal connection warrants further inquiry given that IPV involvement places a Veteran at a 4.5 times increased risk for suicidal thoughts. Currently, IPV assessment and awareness may not be prevalent among providers, causing missed opportunities to recognize this suicide risk factor. Understanding the intersections of IPV, suicidal thoughts, and increased mortality in the male Veteran population should be a research and policy priority.
Footnotes
Acknowledgements
The authors would like to thank Jennifer Thompson Stone for her editorial work.
Authors’ Note
The contents of this article do not necessarily represent the views of the Department of Veterans Affairs or the U.S. Government.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.