
Abstract
Sexual risk behaviors account for most HIV infections in men who have sex with men (MSM), and the risk of exposure from each sexual encounter increases with age. The focus of this study was to investigate which behaviors in midlife and older MSM influence their sexual risk/protection. Cross-sectional data were collected from a community-based sample of 802 MSM aged 40 years and older from community venues (e.g., bars) who completed an anonymous questionnaire. Data from a subset of 420 MSM who were HIV-negative (aged 40-81 years) were used to investigate which behaviors were associated with greater risk for unprotected anal sex. Regression analyses indicated that erection difficulties (odds ratio [OR] = 4.7; 95% confidence interval [CI] = 1.8-12.2), practicing safe sex with outside partners but not with one’s primary partner (OR = 0.54; 95% CI = 0.3-0.94), and recreational drug use (OR = 2.6; 95% CI = 1.3-5.1) were associated with higher risk for unprotected receptive anal intercourse. Younger age (OR = 0.96; 95% CI = 0.9- 0.9), not telling partners about HIV status (OR = 3.2; 95% CI = 1.5-6.5), finding partners in backrooms/sex clubs (OR = 2.8; 95% CI = 1.1- 6.8), and erection difficulties (OR = 10.3; 95% CI = 2.8-37.8) were associated with higher risk for unprotected insertive anal intercourse. These data indicate there may be certain factors specific to older MSM that influence their sexual risk taking behaviors. Programs may be more effective if they are tailored for older cohorts of MSM and address interpersonal communication, erection problems, and substance use to reduce health risks and promote healthier lifestyles.
Men who have sex with men (MSM) 1 represent approximately only 4% of the U.S. population but account for about half (53%) of all people living with HIV (Centers for Disease Control [CDC], 2010). As a group, MSM have an increased chance of being exposed to HIV because of the large number of MSM living with HIV. The CDC found that in 2008 one in five (19%) MSM in 21 major U.S. cities were infected with HIV. MSM are 44 to 86 times as likely to be diagnosed with HIV compared with other men and 40 to 77 times as likely as women (CDC, 2010).
Research indicates many MSM in the United States engage in unprotected anal intercourse (UAI). A large surveillance study conducted by the CDC (Finlayson et al., 2011) indicated that 54% of 8,175 MSM surveyed reported UAI with a male partner, 37% reported having unprotected anal sex with a main male partner (someone with whom the participant had sex and to whom he felt most committed, such as a boyfriend, spouse, significant other, or life partner), and 25% reported having unprotected anal sex with a casual male partner (someone with whom the participant had sex but with whom he did not feel committed, did not know very well, or had sex with in exchange for something such as money or drugs). There is a misperception among some MSM that the insertive or “active” partner in anal intercourse is at minimal or no risk of HIV infection (Beck, McNally, & Petrak, 2003). Although there is evidence to suggest HIV infection is less likely among those who solely take the insertive role compared with those who engage in both roles, or who practice receptive anal intercourse only (Jin et al., 2009), the risk for the insertive partner has been shown in cohort studies (Keet, Albrecht van Lent, Sandfort, Coutinho, & van Griensven et al., 1992) and by the high levels of HIV in rectal secretions (Zuckerman et al., 2004). Unprotected receptive anal intercourse (URAI) can pose up to a 10-time greater risk of infection than insertive anal intercourse (IAI; Vittinghoff et al., 1999).
Complex factors affect sexual risk for HIV among MSM and include drug use (Mattison, Ross, Wolfson, Franklin, & HNRC Group, 2001; Ostrow et al., 2009), sildenafil (Viagra) use (Fisher, Reynolds, & Napper, 2010; Nettles, Benotsch, & Uban, 2009; Paul, Pollack, Osmond, & Catania, 2005; Sanchez & Gallagher, 2006), sex with multiple partners (Diaz, Heckert, & Sanchez, 2005; Lim et al., 2011; Stall & Purcell, 2000), ethnic/cultural issues (Coleman, Jemmott, Jemmott, Strumpf, & Ratcliffe, 2009; De Santis et al., 2012; De Santis, Arcia, Vermeesch, & Gattamorta, 2011; Fields, Malebranche, & Feist-Price, 2008; Fernández, Jacobs, Warren, Sanchez, & Bowen, 2009), and internalized homonegativity, which may be associated with compulsive sexual behavior and depression (Ross, Rosser, & Neumaier, 2008). Although some studies have included older MSM in their samples, only a few studies have investigated sexual risk and HIV issues specifically in midlife and older MSM (Dolcini, Catania, Stall, & Pollack, 2003; Jacobs et al., 2010; Lelutiu-Weinberger et al., 2011; Lim et al., 2011; Murray & Adam, 2001; Ober, Shoptaw, Wang, Gorbach, & Weiss, 2009; Pope, Wierzalis, Barret, & Rankins, 2007). Rates of HIV infection among older urban MSM in the United States are very high, particularly among those in their 50s. Dolcini et al. (2003) reported that HIV prevalence was 19% for MSM in their 50s and 3% for men in their 60s. Prevalence was at high levels for older Blacks (30%), MSM who are injection drug users (21%), moderately heavy drug users (35%), and less closeted men (21%). High-risk sex between serodiscordant partners was 4% to 5% across age groups older than age 30 years and decreased in MSM in their 70s. A recent study by Lim et al. (2011) reported risk behaviors among MSM in their 50s, including high incidence of sex with multiple partners in the past 6 months (69.2%), with 11.4% reporting 30 or more partners.
Substance use, psychological aspects, and difficulties using condoms are central themes for MSM and non–condom use (Adams & Neville, 2009). Risky sex without disclosure of serostatus is not uncommon in persons with HIV (Ciccarone et al., 2003). Barriers to disclosing or even broaching the subject of serostatus between partners include, aside from recreational drug use and alcohol-related impairment, the fear of rejection or the threat of violence (Eaton et al., 2007). Many midlife and older MSM do not recognize the risk of unprotected sex and believe HIV is no longer a serious health threat. (Jacobs et al., 2010; Jimenez, 2003; MacKellar et al., 2007). Not all MSM get tested, and those who do may do so infrequently while continuing to have unprotected sex with nonmonogamous partners.
To understand sexual risk-taking in midlife and older MSM, it is important to consider the context of the lived experience of this group. The developmental process of growing into midlife (i.e., aged 40-59 years) and beyond involves coming to term with diminished physical attractiveness (Elder & Kirkpatrick Johnson, 2003). This developmental process can be particularly challenging for MSM aged 40 years and older, because mainstream gay culture places high value on youth and looks (Kertzner, Meyer, & Dolezal, 2004). Changes in physical appearance may lead some older MSM to feel less sexually desirable and less appreciated in mainstream gay dating circles (Murray & Adam, 2001; Pope et al., 2007). Midlife and older MSM may find that their pool of available partners has been diminished and experience more difficulty in finding a sex partner. They may also be more willing to engage in unprotected sex as a way to attract a desired man or as a way to cope with feelings of inadequacy or low physical attractiveness. As an alternative to being rejected, some may choose to not discuss HIV status (Murray & Adam, 2001). Erection difficulties may pose challenges to condom use, or men chose not to use them in order to find closeness and intimacy (Berg, 2009).
The high prevalence of HIV among MSM creates a greater risk for exposure, and the risk of exposure from each sexual encounter also increases with age (CDC, 2010). The high rates of HIV infection among MSM aged 40 years and older coupled with the significant proportion of MSM who acquire HIV infection during their middle years heightens the urgency to develop HIV prevention interventions that influence HIV risk and sexual health in this group. The purpose of these analyses was therefore to evaluate specific risk factors for high-risk sexual activity in MSM aged 40 years and older.
Method
A cross-sectional, correlational research design was used to investigate which sexual behaviors in midlife and older MSM influence their sexual risk and protection. The independent variables were sexual communication, condom use, and sexual behaviors; the outcome variable was unprotected anal intercourse. The data were analyzed using Pearson’s r correlation and binary logistic regression.
The Sample and Data Collection
After obtaining approval from the institutional review board, data were collected from December 2007 through May 2008 by anonymous pen-and-paper questionnaires using a community-based sample of self-identified MSM aged 40 years and older in South Florida. Eligibility criteria included (a) have had sex with men, (b) be aged 40 years and older, (c) reside in South Florida, and (d) be able to speak/read English. The questionnaire included items on condom use, HIV communication, sexual behaviors, HIV testing, substance use, and sociodemographic items (e.g., relationship status, ethnic identity, age, income, education).
Potential participants were approached by the researcher or research assistant at community venues (i.e., gyms, bars, clubs, community centers, LGBT events) frequented by MSM and older MSM in particular. Once the men agreed to participate in the study, they were each given a questionnaire, a pen or pencil, and an envelope in which to place the questionnaire once completed. Participants were given instructions verbally and in writing. These instructions communicated the purpose of the study, consent to participate, benefits of and risks related to participation, directions for completing the questionnaire, an assurance of anonymity, and plans for the dissemination of research findings. Participants received a small gift (worth about US$1.00) for their time. The 121-item assessment battery took between 20 and 30 minutes to complete and measured the following domains.
Instrument
After an extensive review of the literature, topics of interest linked to midlife and older MSM and HIV risk and sociodemographic items were selected to include in the survey and subsequent analysis. Validated psychosocial scales were also included in the questionnaire but are not included in this analysis as they were not required for the focus of this study. Information on the scales used in this study can be found in our previous publications (Jacobs et al., 2010; Jacobs & Kane, 2012).
Sociodemographic factors
Single items were used to assess participants’ age, ethnicity, partnership status, sexual orientation, educational level, employment status, and other sociodemographic information.
HIV communication
This study included data in response to (a) “In the last 6 months, how often have you discussed with sex partners your/their HIV status?” (b) “Do you have a regular male sexual partner who has a different HIV status to yourself (where one of you has HIV and the other does not)?” (c) “In the last 6 months, how often did you tell sex partners about your HIV status?” (d) “I don’t use condoms if my partner tells me he is ‘clean’ or HIV-negative.” (e) “I assume my sex partners are HIV positive and therefore I always use condoms.” Data for these items were collected using a using a 3-point Likert-type format (1 = always, 2 = sometimes, and 3 = never).
Sexual risk/protection
Participants were asked to report their sexual behaviors in the previous 6 months including (a) number of male sex partners, (b) if they had met any new partners in the past 6 months, and (c) venues through which they met new partners. Dichotomous items were included to assess whether the participants engaged in URAI and unprotected insertive anal intercourse (UIAI) and whether the serostatus of their partner was known (and if so, was it discordant). Participants were asked about their condom use, for example, if in the past 4 weeks they were unable to use condoms due to difficulties with erections before/during sex or in general.
Substance use
Participants were also asked to report their alcohol use and use of each of the following drugs 2 hours before or during sex: crystal methamphetamine, poppers, marijuana, cocaine, ecstasy, GHB, ketamine, heroin, and hallucinogens (within the past 6 months). Items that addressed sildenafil (Viagra) use were included. Participants were asked to report venues in which they had met new male sexual partners in the last 6 months (e.g., bar, sex club, ads, Internet, bath house, private party, gym).
Preliminary Data Analysis
Response rate
Through convenience sampling strategies, a total of 1,317 men were approached and invited to participate. Of the 1,317 men, 1,146 (87%) were eligible, and 70% of the eligible men completed the survey, resulting in a sample size of 802.
Analysis Plan
Using data from a subset of 420 self-identified MSM aged 40 to 81 years (M = 55.5 years; SD = 10.7) who reported being HIV-negative (n = 385, 91.7%) or of unknown status (n = 35, 8.3%) and having had one or more male sex partners in the past 6 months, sexual behaviors and HIV-related communication among this group are reported (N = 420). Descriptive data were analyzed using cross tabs and frequencies. The variable drug use was dichotomized into some drug use and no drug use. Based on levels of risk described above, the outcome variable “unprotected anal intercourse” was divided by sexual positioning (unprotected receptive and insertive anal intercourse). Then URAI was dichotomized to “URAI” and “no URAI” and UIAI was dichotomized to “UIAI” and “no UIAI” (in the past 6 months). Because of the characteristics of the data, logistic regression models were developed. Analyses were conducted in PASW (formally SPSS) 19.0 (IBM, 2011).
Results
Sample Characteristics
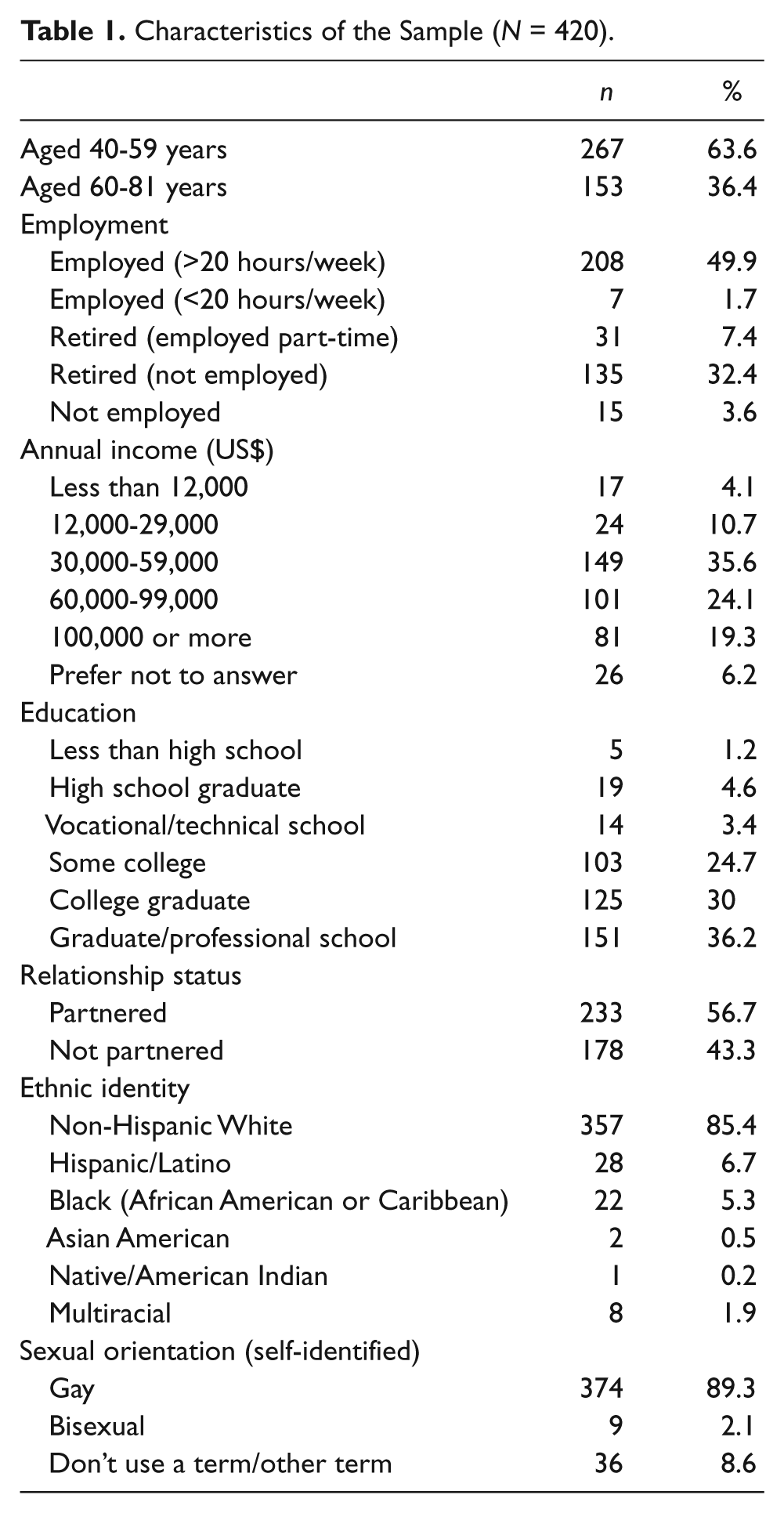
Table 1 reports the characteristics of the sample. The study used data from 420 male respondents aged 40 to 81 years who self-identified as gay, bisexual, or another descriptive (e.g., queer, homosexual). The mean age was 55.5 years (SD = 10.7). Half of the participants were employed full time, were partnered, and had at least a college degree. The majority (85.4%) of the sample was non-Hispanic White.
Characteristics of the Sample (N = 420).
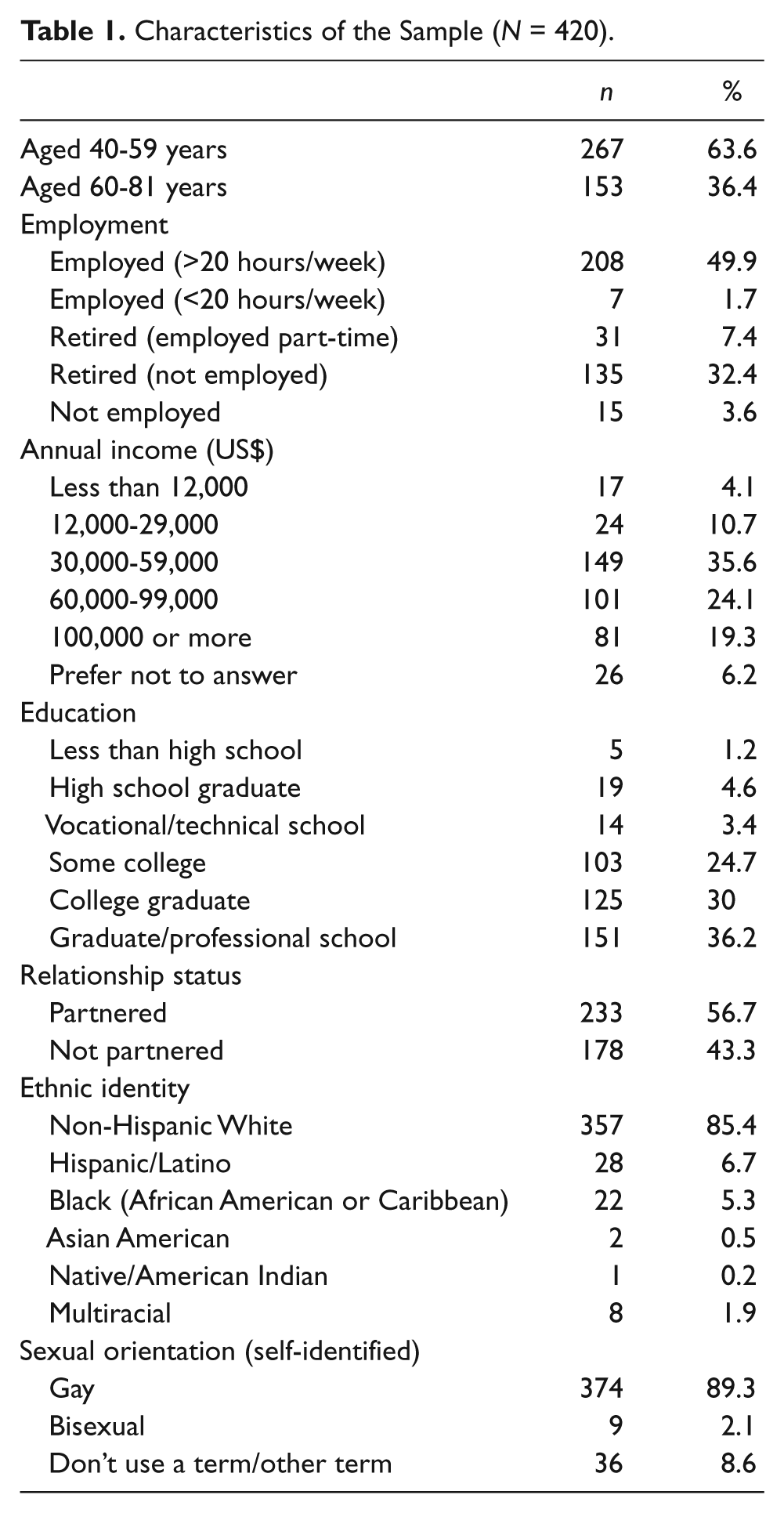
Table 2 reports recent condom use, sexual risk/protective, and testing behaviors of the participants. One third of the men who reported engaging in receptive anal intercourse (RAI) and about 40% who reported engaging in IAI did not use a condom. Only 10% reported having a serodiscordant regular partner. Many participants reported that they never discussed HIV status; however, many also assumed their partners were persons infected with HIV and always used condoms. The majority of participants had multiple partners and one third had met a new partner in the past 6 months. Thirty-one percent used some type of recreational drug before or during sex. More than half reported they do not test regularly. The majority felt they did not put themselves at risk for HIV exposure.
Sexual Risk/Protective Behaviors in the Past 6 Months.
Models Predicting Unprotected Anal Intercourse
Pearson correlation analyses were performed to examine intercorrelations among the variables. Variables that were correlated with the dependent variables were entered into the models (see Table 3). The regression model predicting URAI is presented in Table 4. Not using condoms due to difficulty with erections (before/during sex), practicing safe sex with outside partners but not with primary partner, and recreational drug use before/during sex were entered as predictor variables. The model significantly predicted URAI (χ2 = 23.426, df = 3, p < .001). Erection difficulties (odds ratio [OR] = 4.7; 95% confidence interval [CI] = 1.8-12.2), practicing safe sex with outside partners but not with one’s primary partner (OR = 0.54; 95% CI = 0.3-0.94), and drug use (OR = 2.6; 95% CI = 1.3-5.1) were associated with higher risk for URAI.
Variables Correlated With Unprotected Receptive and Unprotected Insertive Anal Sex (URAI, UIAI).

Correlations significant at the .01 level (2-tailed). *Correlations significant at the .05 level (2-tailed).
Regression Model for Unprotected Receptive Anal Intercourse.

The regression model predicting UIAI is presented in Table 5. The variables chronological age, serostatus disclosure (i.e., “How often do you tell your partners about your HIV status?”), met new partners in the past 6 months, met partners in backroom/sex club, met partners via the Internet, not used condoms due to erection difficulties, and recreational drug use before/during sex were entered. The model significantly predicted UIAI (χ2 = 48.486, df = 7, p < .001). Younger age (OR = 0.96; 95% CI = 0.9-0.9), not telling partners about HIV status (OR = 3.2; 95% CI = 1.5-6.5), finding partners in backrooms/sex clubs (OR = 2.8; 95% CI = 1.1-6.8), and erection difficulties (OR = 10.3; 95% CI = 2.8-37.8) were associated with higher risk for UIAI.
Regression Model for Unprotected Insertive Anal Intercourse.

Discussion
This study identified risk and protective factors in a community sample of HIV-negative MSM aged 40 to 81 years and older. Participants reported a range of risk-management strategies, including assuming partners are HIV positive and thus using condoms, communication, and safe sex with partners outside of the primary relationship. Many participants reported high-risk behaviors, including UAI with a partner whose serostatus was unknown or known to be a person with HIV infection. This finding is noteworthy given reports of (a) serodiscordant partners, (b) recent new partners, (c) multiple partners, (d) feeling they had put themselves at risk for HIV exposure, and (e) infrequent testing. However, these reports of unprotected sex do not take into account type of partner (e.g., monogamous partner with seroconcordant status vs. multiple partners with HIV-positive status). It could be that some men who report unprotected sex are engaging in this activity with monogamous, seroconcordant partners and may not feel the need to use condoms. As there are few empirical reports to date that have investigated HIV risk behaviors in HIV-negative MSM aged 40 years and older, this study has little previous data with which to compare these findings. However, one recent study by Lelutiu-Weinberger et al. (2011) found that older and more anxious MSM had more frequent instances of sexual risk and younger participants who identified with the gay community reported less sexual risk.
Factors Associated With Unprotected Anal Intercourse
Non–condom use related to erection problems was significantly associated with both URAI and UIAI. Erection difficulties become increasingly more common with increasing age. It is acceptable in most gay communities to be openly sexual, to have multiple partners, to negotiate openly for sex, and to enjoy sex freely (Bronski, 2000; Crossley, 2004). Given this, there may be less permission for gay men to have a low level of sexual interest, and even for them to be struggling with sexual difficulties such as erection problems. Because of the emphasis in many gay communities on youth, physical attractiveness, and sexuality (Schope, 2005; Smit et al., 2012; Wierzalis, Barret, Pope, & Rankins, 2006), older MSM may experience a pressure to look attractive and often are expected to be able to follow through on any sexual opportunities that arise. It is also much more acceptable and possible in some gay subcultures to use sex as a way to deal with stress and feelings of isolation (Murray & Adam, 2001). Older MSM with erection difficulties may try to manage the issue by opting for more risky sex, which can result in the acquisition of HIV.
Unprotected Receptive Anal Intercourse
URAI was associated with practicing safe sex with outside partners, although not always doing so with primary partners. This may be may be due to trust, perceptions of safety, and desire for intimacy within the primary relationship, in couples that may be seroconcordant, monogamous, and playing safe with outside partners as well. This may be one of the prevention strategies that arises from men’s awareness of risk with casual partners whose serostatus is unknown. Regardless, there is some risk with unprotected sex with primary partners if the partners are engaging in risky behaviors outside of the primary relationship, especially among highly sexually active MSM. Nonetheless, these men evidence natural strengths and resiliencies that may promote protective behaviors needed to reverse the trends in HIV infection among MSM older than 40 years. Further research is needed to understand the implications of sexual decision making in older MSM to help understand the intricacies of HIV risk and protection to guide prevention efforts.
Recreational drug use has consistently been reported as a major predictor of risky sexual behaviors among gay and bisexual men (Colfax et al., 2005; Greenwood et al., 2001; Halkitis, Parsons, & Stirratt, 2001; Klitzman, Pope, & Hudson, 2000) and young MSM (Garofalo, Mustanski, McKirnan, Herrick, & Donenberg, 2007) and remains prevalent in the gay/bisexual male community (Klitzman et al., 2000). Drug use has been described as an important element of many gay men’s lives (Adams & Neville, 2009; Halkitis & Parsons, 2002). Therefore, our finding that recreational drug use was associated with higher risk for URAI in older MSM was not surprising. Interesting, however, is that drug use was not associated with UIAI, indicating a difference regarding sexual positioning and substance use. Previous studies (Darrow et al., 2005; Lyons, Chandra, Goldstein, & Ostrow, 2010; Ostrow et al., 2009; Semple, Strathdee, Zians, & Patterson, 2010; Wells, Golub, & Parsons, 2011) have linked drug use in MSM men to risky sexual behaviors and to higher rates of HIV infection, but most of these studies have focused primarily on specific time points and on younger MSM. A few studies have written about or investigated drug use as risk for HIV in older MSM populations (Heath, Lanoye, & Maisto, 2011; Jacobs et al., 2010; Ostrow et al., 2009), but they were not specific to HIV-negative older MSM. More data are needed to understand how drug use affects risky sexual behaviours among MSM with negative serostatus in mid- and later life.
Unprotected Insertive Anal Intercourse
Chronological age
It is not surprising that younger men in the sample (i.e., aged 40-59 years) were more likely to engage in unprotected sex than their older counterparts (i.e., aged 60 years and older). Regarding age, midlife is a time when men shift from seeing the future in terms of their potential and begin to see it in terms of limitations (Dittman-Kohli, 2005), which could contribute to increased risk. Changes in physical appearance and increased vulnerability to chronic disease (Hutchison, 2008; Whitbourne, 2001) lead to increased awareness of less time remaining in life and an enhanced personalization of mortality. Midlife and older MSM may experience discontentment or boredom, which can create risk for them during this period of life. Some MSM continue with old patterns developed in adolescence and young adulthood and have difficulty adopting new patterns conducive to a healthier transition to older age. Making successful transitions from young adulthood to midlife and adjusting to these life changes requires internal resources and social and community supports that are not always available to heterosexual men and are even less available for MSM who have lived much of their life in a society that stigmatizes homosexuality and a gay culture that emphasizes youth and beauty (D’Augelli, Grossman, Hershberger, & O’Connel, 2001; Isensee, 1999; Murray & Adam, 2001; Pope et al., 2007; Schope, 2005; Sharma et al., 2007).
Disclosure
Results of the analysis indicated that the more often men discussed their HIV serostatus with partners the more likely they were to use condoms. HIV disclosure is a complex process characterized by communicating something, timing, and contextual environment; protecting someone; and relationship status (Eustace & Ilagan, 2010). For these reasons our findings are difficult to interpret. First, the questionnaire did not have items inquiring about specific partners and under which conditions serostatus disclosure was ensured. For example, it might have been possible that some participants had unprotected sex only after disclosing their serostatus, which generally opens up the topic for disclosure of the partner (who may in fact be a person infected with HIV). Second, there may be some quality to the relationship that may not only facilitate disclosure but permits more effective condom negotiation (Simoni & Pantalone, 2004). Nearly half (46.4%) of the participants reported they assume partners have HIV and thus always use condoms. Therefore, it is uncertain if disclosure actually facilitates safer sex any more than nondisclosure promotes riskier sex.
UIAU was associated with meeting partners in backroom/sex clubs. Sex clubs sometimes, but not always, attract men who engage in risky behavior. High-risk MSM are more likely than their peers to go to sex clubs (Binson et al., 2001) and more than half of all nontesting high-risk MSM go to sex clubs (Binson, Woods, Pollack, & Sheon, 2005). For older MSM, who may not be accepted in gay mainstream dating circles, sex clubs may offer an alternative for meeting partners.
Implications for Public Health Practice
Several implications emerge from this study. Although generalizations must be made cautiously, some thoughts are presented for directions for practice and further study.
Results from this study indicate that age and sexual difficulties, in addition to contextual factors specific to older MSM, influence their sexual risk taking behaviors. Understanding sexual risk behaviors in HIV-negative midlife and older MSM might help guide prevention efforts targeted to this group, which may influence the factors affecting their ability to engage in safer sex practices. Programs may be more effective if they are tailored for older cohorts of MSM and include personal communication and social skills to reduce health risks and promote healthier lifestyles. Interventions that focus on the specific sexual health concerns (i.e., erection difficulties) that affect condom use might prove useful. Approaches focusing on interactions with partners, particularly regarding serostatus disclosure and safer sex practices, should take into account the dynamic nature of sexual interaction that is subject to individual processes (e.g., fear of rejection) and socio-environmental processes (e.g., HIV-stigma) that influence interpersonal interactions. These findings also reinforce the importance of implementing interventions that target the reduction of recreational drug use as part of comprehensive and efficacious HIV prevention strategies. HIV prevention counseling during testing is an opportune time to incorporate substance use reduction strategies while negotiating concrete, achievable behavior-change steps that will reduce HIV risk in this group.
Community-based public health programs may be more effective if they are tailored for older cohorts of MSM and include personal communication and social skills programs to reduce health risks and promote healthier sexual lifestyles. Addressing erectile dysfunction (ED) management in HIV prevention programs for older MSM is warranted. The medical and therapeutic community must maintain equal treatment standards for ED between heterosexual men and MSM, regardless of their HIV status and other medical issues. Not considering the needs of older MSM with sexual difficulties is akin to the past when homosexuality itself was considered to be dysfunctional. Moreover, providers need to help gay men address the issue of ED in an open and honest way.
Research that focuses on skill building may be needed in that communication styles used by midlife and older MSM to negotiate safer sex can be learned and increased. Providing HIV education, creating awareness of risk factors, and changing midlife and older MSM’s low perception of risk for HIV may help decrease the stigma attached to the disease. Moreover, strategies to decrease drug use that are incorporated into safer sex interventions that promote skills to enable older MSM to be assertive, effective communicators, and informed about the risk/protection associated with disclosure may prove useful. More research is needed to investigate at-risk older MSM’s behavioral responses to serostatus disclosure to determine the effectiveness of HIV-status discussions as an HIV prevention strategy and to identify ways in which the effectiveness of this communication can be enhanced.
Sex clubs offer an opportune environment in which to target this otherwise hard-to-reach population with appropriate prevention interventions (Woods, Euren, Pollack, & Binson, 2010). Although not without its challenges, there is evidence to support implementing HIV testing programs in clubs (Bingham et al., 2008; Daskalakis et al., 2009; Spielberg et al., 2005) and that such in-club testing has been associated with a reduced risk behavior (Huebner et al., 2006, 2010). The scientific literature indicates a wide range of HIV prevention programs, and services have been initiated in clubs to try to reach MSM at risk with HIV prevention services and information (Bingham et al., 2008; Huebner et al., 2010; Woods et al., 2010).
Limitations
There are several limitations in the present study. First, the data are cross-sectional and do not permit longitudinal examination of the associations or change over time, and generalizations cannot be made regarding cause-and-effect relationships. Second, although it was a community-based sample, it was not necessarily representative of the broader population of midlife and older gay men in the United States. Rather, our generalizability is limited to midlife and older gay men who visit community venues in catering to or frequented by other midlife and older gay men, and consequently, future studies are needed using different samples of men who do not. Third, high-risk sexual and substance use behaviors are self-reported and subject to underreporting. Fourth, data about whether unprotected sex was with main or casual partners and the age of each partner were not collected. UAI with regular, monogamous seroconcordant partners poses quite different risk from that with casual partners. Fifth, although the sample size was adequate, it consisted of mostly non-Hispanic White gay and bisexual men older than 40 years; the findings need to be validated in multiethnic samples of midlife and older gay men. Sixth, that the questionnaire was offered in English only may have inadvertently excluded non-English speaking older MSM. This is an important consideration given the large Spanish-speaking population in South Florida. This limitation may affect the usefulness of the results in addressing the HIV prevention needs of this population in that the findings may not be culturally relevant to non-English speaking groups of older MSM. Last, because of the unique characteristics of the region where the study was conducted, there is a possibility that findings from our study may not be fully generalizable to other metropolitan areas or rural regions of the United States.
Conclusion
Midlife and older MSM may engage in risky and/or protective sex for a variety of reasons. For the men in this sample, these sexual activities are influenced by age, difficulties with condom use due to erection difficulties, serostatus disclosure, and substance use. Older MSM have received less attention in the literature than younger MSM. Results indicate that age and sexual difficulties in addition to contextual factors specific to older MSM influence their sexual risk taking behaviors.
The findings from this study highlight the complexity of a sexual risk and protection in older MSM, driven in some cases possibly by aging concerns that may be causing internal conflict or the strengths and resilience that develops from surviving years of oppression, discrimination, decimated social networks, and loss of loved ones from the devastating effects of the AIDS pandemic. Older MSM face a unique historical background and current circumstances that may hinder or facilitate the factors affecting their ability to engage in safer sex practices. Understanding these influences will help guide and inform prevention efforts for this underserved and overlooked group.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.