
Abstract
This article aimed to identify the determinants of tobacco consumption and illegal drug use (IDU) as well as to examine the association between these two variables using a representative sample of 3,771 Bangladeshi males aged 15 to 54 years. Data were collected through Bangladesh Demographic and Health Survey 2007. To identify the determinants, the patterns of tobacco consumption and IDU were analyzed by age, education and occupation, residence, mass media, premarital sex, wealth, and sexually transmitted infections (STIs). Prevalence of smoking cigarette and bidi was roughly 60%. However, the prevalence of IDU was 3.4%, and this proportion is statistically significant (Z = 11.32, p = .000). After bivariate analysis, almost all variables except STIs were significantly associated with tobacco consumption. Similarly, all variables except residence and mass media were associated with IDU. Based on multivariable adjusted logistic regression analysis, the likelihood of using IDU was approximately twofold (odds ratio [OR] = 1.8, 95% confidence interval [CI] = 1.23-2.53) among bidi smokers and fourfold (OR = 3.8, 95% CI = 2.62-5.56) among cigarette smokers as compared with nonsmokers.
Introduction
Tobacco consumption is one of the biggest global public health problems, causing more than 5 million deaths annually. Although tobacco-related deaths between 2002 and 2030 were projected to decline gradually in developed countries, such deaths were anticipated to increase from 3.4 million to 6.8 million in developing countries (Ezzati et al., 2002; Mathers & Loncar, 2006). Research on tobacco consumption in developing nations by sociodemographic and economic groups is limited as well as diverse depending on the nature and types of population reported. In South Asia, different types of tobacco consumption, such as cigarettes, bidis, 1 hookah, 2 and smokeless tobacco (usually consumed orally or nasally, without burning or combustion), such as chewing tobacco, 3 are more common (Chadda & Sengupta, 2002; Eriksen, Mackay, & Ross, 2012). Various socioeconomic factors are found to be associated with these tobacco patterns. Studies regarding tobacco consumption in developing countries provided mixed results. For instance, tobacco consumption was more among people of the poorest socioeconomic status in terms of poverty, low education, and manual or lower paid occupation in countries such as Bangladesh and India (Aekplakorn et al., 2008; Khan, Khandoker, Kabir, Kabir, & Mori, 2006; Schaap, van Agt, & Kunst, 2008). However, in some low- and middle-income countries, tobacco consumption, especially smoking cigarette, is more prevalent among the more affluent groups, which is not the case in high-income countries (Jha & Chaloupka, 2000).
The high level of tobacco consumption in many developing countries is alarming (Shafey, Eriksen, Ross, & Mackay, 2009). Bangladesh is an example in this regard (Global Adult Tobacco Survey, 2009; Mitra, Islam, Al-Sabir, & Jamil, 2009), which is one of the most populated countries in the world (Bangladesh Bureau of Statistics, 2008) and is located in the Southeast Asian region. This region being the largest producer and consumer of tobacco products is a special concern. The high prevalence of tuberculosis in this region also adds a new dimension to the problem of tobacco control (World Health Organization, 2009).
Tobacco-related diseases, consequences, and costs (direct and indirect) are enormous in Bangladesh. Diseases such as oral cancer, cancer of the larynx, lung cancer, ischemic heart disease, stroke, chronic obstructive pulmonary disease, pulmonary tuberculosis, and Buerger’s disease are prevalent in this country (Zaman, Nargis, Perucic, & Rahman, 2007). The estimated health care cost attributed to the tobacco-connected illnesses was around 10% of the monthly household expenditure (Zaman et al., 2007). Annually, about 1.2 million tobacco-related disability and illnesses, with an estimated death toll of more than 57,000, were reported. About 16% of deaths in adults aged 30 years or older were associated with tobacco consumption (Zaman et al., 2007). Indirect tobacco-related cost, which arises from the failure to earn due to illness, disability, or death, accounted for US$652.86 million per annum (Shafey et al., 2009). The economic cost was also enormous, as 50% of all tobacco-associated deaths were of those in the main productive ages of 30 to 69 years (Shafey et al., 2009). Moreover, about 5% of the household’s monthly expenditure was reported to be associated with the purchasing of tobacco products (Zaman et al., 2007). Similarly, about 30% of the deforestation in Bangladesh was related to tobacco manufacturing (John & Vaite, 2002).
Like widespread tobacco consumption, substance use and its impacts on the individual, family, and community levels are increasing globally. Particularly, the impacts of illicit drug use are huge in developing countries because of poor health infrastructure and limited resources (United Nations Office on Drugs and Crime [UNODC], 2010). Globally, around 155 to 250 million people (i.e., 3.5% to 5.7% of the global population) aged 15 years and older have used illegal drugs at least once. Of these, some of the commonly used illicit drugs are cannabis (129-191 million), amphetamine-type stimulants (ATS; 13.7-52.9 million), opiates (notably heroine; 12.8-21.9 million), and cocaine (15-19 million). Opiate users experience the highest level of harm (UNODC, 2010). Particularly Bangladesh is vulnerable to the impacts of illicit drug use because of its proximity to the drug trafficking zones of the Golden Triangle and the Golden Crescent. Phensedyl (a cough suppressant syrup containing codeine phosphate) is produced lawfully in India and easily marketed in neighboring Bangladesh through drug trafficking. The overall vulnerability also increases in Bangladesh, as this country shares some border with Myanmar, the largest drug abuse country (Banglapedia, 2006). The annual prevalence of cannabis (locally known as Ganja) in the population aged 15 to 64 years was 3.3% in Bangladesh (UNODC, 2010). Besides, annually about 4 metric-tons of opium (popularly known as heroine) was consumed in Bangladesh, which is likely to increase in the future (UNODC, 2010). Almost all the heroine consumed in Bangladesh originates from India, the leading consumer of opium (UNODC, 2010).
Although numerous studies have already been conducted in developed countries to examine the association of tobacco consumption and illicit drug use, such studies are scarce in Bangladesh. Most of the studies conducted on Bangladesh so far dealt with micro-level data. Because of the lack of national-level data on tobacco and illicit drug use, little is known about the vulnerability of illegal drug use with tobacco consumption, especially among ever-married (currently married or married at least once in his life time) men in Bangladesh. This study aims to bridge this gap using nationally representative cross-sectional data collected through the Bangladesh Demographic and Health Survey (BDHS) 2007. Briefly, the current study identifies the determinants of tobacco consumption and illegal drug use as well as examines the association between these two variables among ever-married Bangladeshi men. The findings on the association between tobacco consumption and illegal drug use have important policy implications for tobacco control initiatives, and some policy strategies are suggested in the conclusion of the study.
Data and Method
Data
Data were extracted from BDHS 2007. The detailed methodology of the BDHS 2007 including the data collection method, validation, and reliability assessment is explained in a national report (Mitra et al., 2009). The 2007 BDHS is considered a nationally representative sample of the residents of private dwelling units in Bangladesh. The sampling frame for the survey was formed from the 2001 population census, and a two-stage stratified sampling was employed. At the first stage, 361 primary sampling units (PSUs) were selected, of which 227 PSUs were from rural areas and the rest from urban areas. A list of households in all the selected PSUs was prepared and used as the sampling frame for selection of households in the second stage. On an average 30 households were selected from each PSU, using an equal probability systematic sampling technique. About 10,819 households were selected, of which 10,461 were occupied. Interviews were successfully completed in 10,400 households (with a response rate of 99.4%). Next, from every second household, a total of 4,074 eligible ever-married men were selected, of which 3,771 (i.e., 92.6% of the total sample) were successfully interviewed. BDHS used the standard questionnaires from the MEASURE DHS+ model questionnaire. All questionnaires were pretested before data collection. After data collection, data processing was carried out using CSPro, including editing, coding of open-ended questions, data entry, and editing inconsistencies observed in the computer program. To ensure the quality of the data, every stage of the survey was carefully monitored by USAID, NIPORT, Mitra and Associates, Ministry of Health, and Macro International based in the United States (Mitra et al., 2009).
Variables
The BDHS 2007 collected information on socioeconomic and demographic characteristics, health and lifestyle factors, marriage and family planning, health care facilities, HIV/AIDS, sexually transmitted diseases (STDs), and domestic violence. A number of variables from the large data set, namely, respondent’s age, education, occupation, place of residence, exposure to mass media (print and electronics), premarital engagement in sex, wealth index, incidence of STIs, and tobacco consumption in different forms and illegal drugs, were used. It should be mentioned that the selection of variables was not arbitrary; rather, it was guided by relevant literature (Choudhury, Hanifi, Mahmood, & Bhuiya, 2007; Kamal, Islam, & Raihan, 2010; Khan et al., 2006, Khan, Khan, Kraemer, & Mori, 2009; Schaap et al., 2008) on tobacco and illicit drug use. To collect information about types of tobacco consumption (cigarettes, bidis, smokeless tobacco such as chewing tobacco), several questions were asked during the survey:
Do you currently smoke cigarettes/bidis?
In the last 24 hours, how many cigarettes/bidis did you smoke?
Do you currently smoke or use any other type of tobacco?
If yes, what types of tobacco (smoke or smokeless tobacco) do you currently use?
The question on the illicit drug 4 usage was the following:
In the last 3 months preceding the survey, have you ever taken any illicit drug?
Before asking questions regarding illicit drug use, the respondents were ensured of the confidentiality of the information they provided.
Analysis
Statistical analyses were performed using SPSS Version 18 (IBM SPSS Inc., Chicago, IL) to identify the determinants of tobacco consumption and illicit drug use and then to examine the association between these two variables. Frequency runs were generated to compute the prevalence rates of tobacco consumption and illicit drug use. The prevalence rates of tobacco consumption and illicit drug use were also computed for selected background characteristic variables to identify the determinants. The determinant variables considered include age (15-24, 25-34, 35-44, 45-54 years), educational attainment (no education, complete primary, complete secondary, college and higher), place of residence (urban, rural), exposure to mass media 5 (no media exposure, exposure to any media), engagement in premarital sex (yes, no), occupation (unemployed; farmers, workers, labor, semiskilled; small and large business; high skilled; others), incidence of STI (yes, no), and wealth index (poorest, poor, average, rich, richest). The significance of the determinant variables was evaluated using Pearson’s chi-square (χ2) test (Chan, 2003). The null hypothesis of no relationship between tobacco consumption (illicit drug use) and the determinant variable is rejected if the p value of the χ2 statistic is less than 5%. Both the χ2 statistic and its p value are reported in the results.
To examine the association between tobacco consumption and illicit drug use, an analysis was performed using the following logistic regression:

where Yi = 1 if respondent i is a drug user and 0 otherwise, Xi = 1 if respondent i is a tobacco user and 0 otherwise, and Z1, Z2, . . ., Zk are variables representing the background characteristics that affect illicit drug use.
Two different dependent variables were considered. The first one is whether a respondent had taken any form of drug, and Yi was assigned a value of 1 if the respondent had taken one or more drugs. The second dependent variable (Yi) was assigned a value of 1 if the respondent had taken only one type of drug. The tobacco use variable Xi was assigned a value of 1 if the respondent had ever used any tobacco product. For comparison purposes, the regression was also estimated separately for different forms of tobacco consumption, including cigarettes, bidis, and other types of tobacco. The odds ratios (ORs) in favor of illicit drug use were further compared for the frequent and nonfrequent smokers. Significant determinants of illicit drug use Z1, Z2, . . ., Zk were included in the logistic model to control for the effects of the confounding factors. A total of 14 logistic regressions were estimated for different measures of Yi and Xi. The OR and its 95% confidence interval (CI) for illegal drug use were estimated for each of the measures.
Results
About 70% (2,644 men) of the respondents used any of three tobacco products (smoking cigarettes, bidis, and use other forms of tobacco). Among the tobacco users, 78% (2,057 men) consumed only one of the three types, 20% (537 men) consumed any two of the three types, and only 2% (47 men) used all three types of tobacco products (Table 1). The overall prevalence of smoking cigarette and bidi were roughly same (about 60%, 2,263 men), and on an average, men smoked five cigarettes/bidis a day. The prevalence of using other forms of tobacco (i.e., chewing tobacco leaves or sada pata or gul, betel quid [pan masala] with tobacco or zarda) was about 21% (807 men). About 33% (737 men) smoked more than six times a day, with an average of 13 cigarettes per day; 28% (629 men) smoked bidi more than 11 times a day, with an average of 20 bidis per day. About 3.4% (124 men) of the respondents used illicit drugs, and this proportion is statistically significant (Z = 11.32, p = .000). Among them, 84% (104 men) used only one type of drug and 16% (20 men) used two or more types (Table 1).
The Prevalence of Tobacco Consumption and Illegal Drug Use Among Males, BDHS 2007

Total is not always 3,771 due to missing values.
Chewing tobacco leaves or sada pata or gul, betel quid (pan) with tobacco or zarda.
Drug includes ganja, charas, phensidyl, pethedine, heroin, morphine, and injectable drugs.
To assess the significance of the determinant variables for tobacco consumption, the χ2 test was performed (Table 2). Tobacco consumption was significantly related to the respondent’s age (χ2 = 68.14, p < .001). The older age groups were more likely to smoke bidis and other tobacco products, whereas the younger group had a higher tendency to smoke cigarettes. Literacy is another significant determinant (χ2 = 227.60, p < .001). The prevalence of tobacco consumption among males with no education was 1.8 times higher than those with at least college education. Tobacco consumption (in any form) was higher (χ2 = 19.91, p < .001) among rural males, although cigarette smoking was significantly (χ2 = 56.68, p < .001) higher among urban males than their rural counterparts. Other forms of tobacco and bidi consumption were higher (χ2 = 177.60, p < .001) among rural inhabitants. Exposure to mass media was also a significant determinant (χ2 = 113.78, p < .001) of tobacco consumption. Besides, premarital sex showed a positive relationship (χ2 = 14.52, p < .001) with all types of tobacco consumption except bidi smoking. Tobacco consumption was significantly dependent on occupation (χ2 = 100.37, p < .001) and wealth status (χ2 = 128.91, p < .001). Cigarette smoking was more prevalent in the affluent group, whereas the poor tended to smoke bidis and other forms of tobacco. In sum, the significant determinants of tobacco consumption were age, education, place of residence, exposure to mass media, engagement in premarital sex, wealth status, and occupation.
Prevalence of Tobacco Consumption Among Bangladeshi Males by Selected Background Characteristics, BDHS 2007
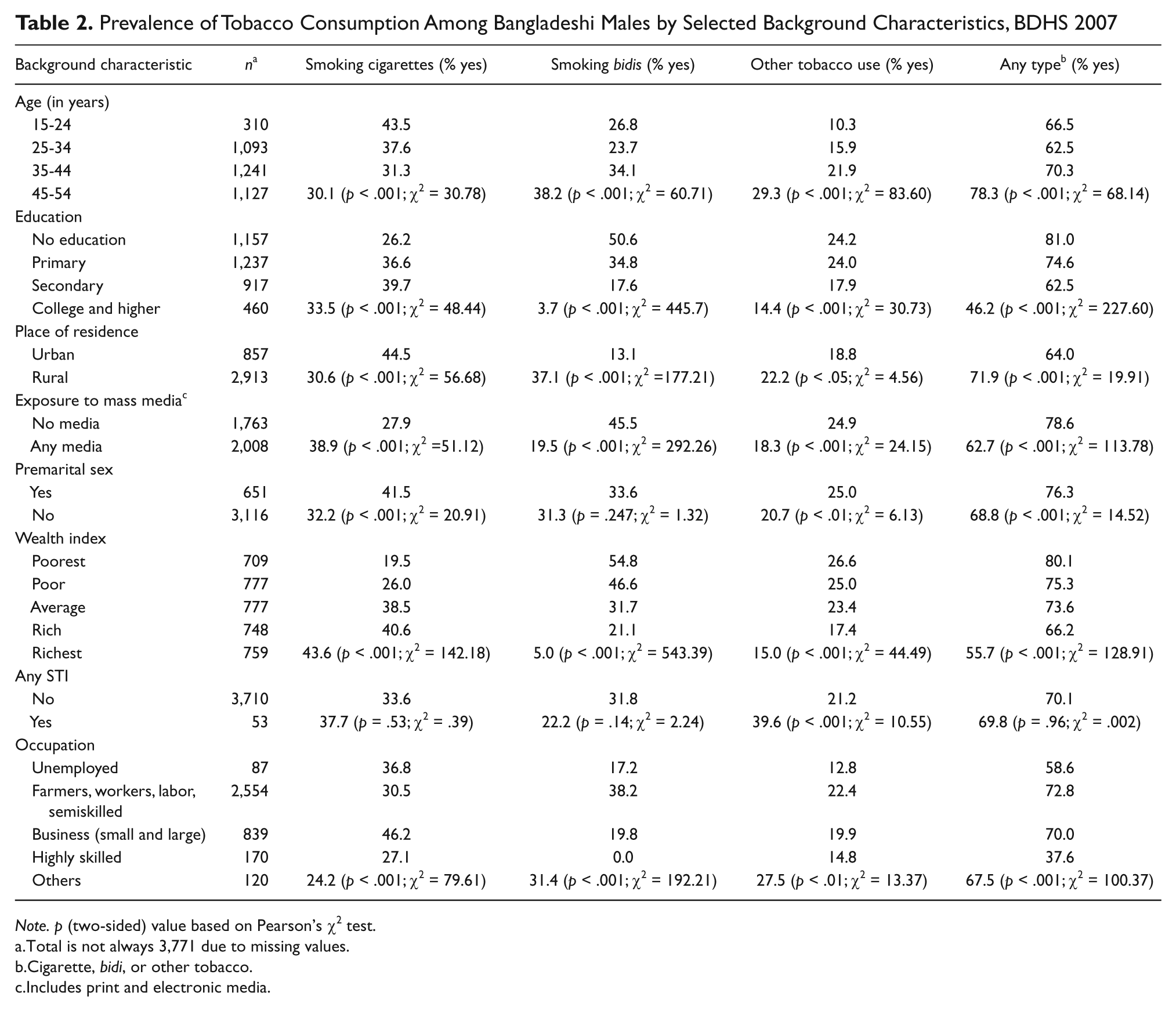
Note. p (two-sided) value based on Pearson’s χ2 test.
Total is not always 3,771 due to missing values.
Cigarette, bidi, or other tobacco.
Includes print and electronic media.
The χ2 test was also performed to identify the determinants of illicit drug use (Table 3). The significant determinants for this variable include age (χ2 = 6.56, p < .08), education (χ2 = 12.10, p < .007), engagement in premarital sex (χ2 = 59.56, p < .001), wealth status (χ2 = 15.08, p < .005), incidence of STI (χ2 = 11.47, p < .001), and occupation (χ2 = 10.30, p < .03). Some groups like those younger than 24 years old, men with no education, living in urban areas, and had premarital sex revealed higher prevalence of illicit drug use. Similarly, those who had no exposure to media, from the fourth quintile (rich group) of wealth index, experienced STIs, and from the semiskilled occupational groups were associated with higher rate of illicit drug use (any type).
Prevalence of Illegal Drug Use Among Bangladeshi Males by Selected Background Characteristics, BDHS 2007

Note. p (two-sided) value based on Pearson’s χ2 test.
Total is not always 3,771 due to missing values.
Any type means use of any drug in last three months
Taking only one prominent drug.
Includes print and electronic media.
The logistic regressions controlling for the confounding factors of respondent’s age, education attainment, place of residence, exposure to mass media, premarital sex, occupation, incidence of STI, and wealth index were estimated to examine the association between tobacco consumption and illicit drug use. These factors were the significant determinants of illicit drug use reported earlier. The ORs for illegal drug use by different types of tobacco and the estimated 95% CI for these ORs are presented in Table 4. The OR provides an indication of the likelihood of illicit drug use among the tobacco consumers compared with the nontobacco consumers, while the CI states the lower and upper bounds of the OR. According to our multivariable analyses, the respondents who smoked cigarettes, bidis, and used other forms of tobacco revealed 3.8, 1.8, and 2.0 times higher likelihood of using any illicit drug compared with the corresponding reference category of no tobacco consumption. In addition, the respondents who used any tobacco product (cigarettes, bidis, or any other form of tobacco considered together) were 19.6 times more likely to use illicit drug compared with those who did not use any tobacco product. The likelihood of using any illicit drug also increased with more frequent smoking, and this was found true for any type of tobacco consumption. For example, the OR for those who smoked 6 cigarettes or more per day was 5.3, whereas the odds ratio was much lower (2.0) for those who smoked 1 to 5 cigarettes per day. The results from the logistic regressions also suggested that tobacco consumption carried by far the highest association with drug use among all variables. 6
Odds Ratio (OR) and 95% Confidence Interval (CI) for Illegal Drug Uses by Tobacco Consumption, Controlling for Possible Confounding Factors Among Bangladeshi Males, BDHS 2007

Any drug means use of drugs as mentioned in footnote of Table 2.
Only one drug means any prominent drug.
p < .001. **p < .01. *p < .05.
Discussion
This study found several socioeconomic, demographic, cultural, and behavioral factors that were significant determinants of tobacco consumption and illegal drug use. It also identified a positive association between tobacco consumption in various forms and illegal drug use among Bangladeshi men. The study revealed a high prevalence of tobacco use (about 70%; 2,644 men) among Bangladeshi men aged 15 to 54 years. The finding is consistent with a recent adult tobacco survey in Bangladesh (Global Adult Tobacco Survey, 2009). Similar to other studies (Choudhury et al., 2007; Finney Rutten, Auguston, Moser, Beckjord, & Hesse, 2008; Khan et al., 2006), all types of tobacco consumption except cigarette smoking were more prevalent among the poor with low education and occupational status and residing in rural areas. The pattern of cigarette smoking was contradictory, which could be attributed to various factors such as the mildness of cigarette, Westernized lifestyles, glamour, and fashion (Schaap et al., 2008). Compared with cigarette smokers, the bidi smokers (cheapest substitute for cigarettes) and other forms of tobacco users were socioeconomically poor, characterized by low income, poor education, and rural background. The poor are more likely to consume tobacco, which are more harmful and likely to be malnourished and particularly ill-equipped to protect against respiratory and other tobacco-related diseases. In addition, the poor are less able to afford health care services, which could deteriorate their overall health situation further (Choudhury et al., 2007; Kamal et al., 2010). Consistent with other studies (Kamal et al., 2010; Khan et al., 2009), a positive association was found between health awareness gained via mass media and tobacco consumption. It is very apparent that education level and health knowledge is positively related to each other and also important determinants of tobacco consumption. Therefore, increasing education and awareness about the adverse health effects of tobacco should be a noteworthy policy for reducing the social and economic burden of tobacco consumption in Bangladesh. Behavioral factors such as premarital sex were associated with tobacco use except bidi smoking. Incidence of STI was found to be statistically insignificant.
The incidence of illegal drug use in Bangladeshi men was 3.4%, which is similar to another study (UNODC, 2010). Illicit drug use was significantly associated with socioeconomic factors such as educational and occupational status, wealth index, as well as behavioral aspects, namely, premarital sex and being infected by STI. However, urban–rural differences and mass media association were inconsistent. Therefore, further studies are recommended in this regard.
The revealed positive association between tobacco consumption and illicit drug use is also found to be consistent with other studies (Algotar et al., 2011; Chen, Chen, Fagot-Campagna, Narayan, 2001; Hanna & Grant, 1999; Kamal et al., 2010; Khan et al., 2006; Mohler-Kuo, Lee, & Wechsler, 2003; Padrão, Silva-Matos, Damasceno, & Lunet, 2011; Richter, Ahluwalia, Mosier, Nazir, & Ahluwalia, 2002). Some further supporting evidence for this association is as follows. The increased frequency of cigarette smoking may be a marker for more serious patterns of illegal drug use (Bailey, 1992). Mohler-Kuo et al. (2003) reported a positive association between smoking regularly and illicit drug use. Another study showed regular tobacco use was the predictor of life-time drug use (Hanna & Grant, 1999). Besides, a positive association between tobacco consumption and illicit drug use was also reported in Khan et al. (2006). Chen et al. (2001) found that the use of illicit drugs was 6.4 times greater (p < .001) among tobacco users than nonusers. In addition, there is evidence that cannabis use during teenage and young adulthood is associated with an increased risk of tobacco use and nicotine dependence (Patton, Coffey, Carlin, Sawyer, & Lynskey, 2005). Moreover, the life-time smoking was linked significantly to alcohol, cannabis, hard drug, and multiple drug use disorders, which was reported by Lewinsohn, Rohde, and Brown (1999). Padrão et al. (2011) also reported a positive association between tobacco consumption and alcohol use.
Since positive association between tobacco and illicit drug use are identified, some programs at the government, community, family, and individual levels should be undertaken to provide interventions and to develop appropriate tobacco control policies.
According to the National Strategic Plan of Action for Tobacco Control, 2007-2010 (NSPATC; Ministry of Health and Family Welfare, 2007) in Bangladesh, some options, namely, setting appropriate price and tax policies; prohibition of advertisements and sponsorship along with awareness by training, education, and communication; ban on sale of tobacco products to and by minors; packaging and labeling of tobacco products; research and partnership building for tobacco control along with control of illicit trade, may be useful to reduce the consequences of tobacco consumption (NSPATC, 2007). Some of these strategies are already enacted in Bangladesh. For instance, advertisements of cigarettes or bidis now include a warning message stating that smoking is harmful to health. Besides, health warnings are also mandatory on packages of cigarettes and bidis. Unfortunately, these printed messages are not effective in Bangladesh as about 46% of the adult population in Bangladesh is still illiterate and hence they cannot read the message on packets. Moreover, many smokers buy a single stick rather than the full packet of cigarettes/bidis. Therefore, they miss the warning message written on the packets (Choudhury et al., 2007; Khan et al., 2009).
Some more strategies such as involvement of religious leaders, health services providers, teachers, community leaders, and mass media can reduce tobacco consumption among males in Bangladesh (Khan et al., 2006). In connection with other interventions or policies in Bangladesh (Choudhury et al., 2007; Khan et al., 2006, 2009; NSPATC, 2007), we would like to propose some recommendations: First, given the importance of awareness, short documentaries on the adverse effect of tobacco consumption could be broadcasted before the national news, or popular drama series, or sport events that are more likely to draw a large audience. Second, religious leaders especially Imams (the head of a mosque) could play a vital role in preventing tobacco consumption by addressing the gatherings for Friday prayers (a special prayer for Muslims and majority of them attends that prayer). Imams can speak briefly about the harm of tobacco use from the religious perspective. This approach is especially important as more than 85% of the populations in Bangladesh are Muslim and tobacco use is more prevalent among Muslims than others (Mitra et al., 2009). Third, given the higher prevalence rate of tobacco consumption among the families with lower socioeconomic status, the government could provide support by cash to quit from this hazardous activity. At the same time, the government could provide health cards for those who are illicit drug users, followed by tobacco users. In conclusion, tobacco consumption among Bangladeshi ever-married males is high and found to be associated positively with illegal drug use. In fact, tobacco consumption has the highest influence on illicit drug use among the variables considered. Since both tobacco and illegal drugs are hazardous in all aspects, comprehensive strategies as proposed in this study along with existing policies should be implemented to reduce their use. At the same time, the positive association between tobacco use and illicit drug use would also imply that any of such policies and strategies will serve as a two-pronged approach.
Limitations
Self-reported data on tobacco consumption and illicit drug use from BDHS 2007 could suffer from recall bias and deliberate misreporting. Even though anonymity and confidentiality were ensured during the survey, respondents might have underreported or overreported, as tobacco consumption and illicit drug use in Bangladesh are not widely acceptable social norms. This misreporting could influence both the prevalence of tobacco consumption and illicit drug use and their association. Furthermore, engagement of premarital sex and STIs may be underreported. Premarital sex is not acceptable in the society both culturally and from the religious point of view. For similar reasons, the negative social stigma associated with STIs will put some pressure on the respondents in revealing the truth. Therefore, the behavioral factors explored in this study are preliminary. Although many variables were analyzed, exclusion of some other important variables might limit our findings. Finally, since the data were cross-sectional, cause–effect relationships could not be inferred.
Footnotes
Acknowledgements
The authors are extremely thankful to S. N. Mitra, CEO, Mitra and Associates, Dhaka, Bangladesh; the Director General, National Institute of Population Research and Training (NIPORT), Ministry of Health, Government of Bangladesh; and Macro International, USA, for giving permission to use their database. We are also grateful to two anonymous referees and the editor for useful comments and suggestions.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.