
Abstract
Although the Asian American population is increasing, Asian American men’s health remains underinvestigated. This study examined the overall pattern of their health and health care usage. Using a nationally representative sample (N = 998) from the National Latino and Asian American Study (2002-2003), the first comprehensive epidemiological survey, rates of chronic conditions, behavioral health, and mental health service utilization (e.g., general medical, specialty mental health, and any medical services) were computed. The ages ranged from 18 to 95 and the mean age was 41. Of the sample, there were no ethnic subgroup differences in most of the physical and chronic conditions, with the exception of allergies/hay fever, arthritis, asthma, and high blood pressure. Behavioral health problems and substance use varied among Asian American men with more Vietnamese American men reporting that they are current smokers and more Filipino American men reporting having ever used drugs and having higher rates of obesity. Levels of mental health status and health services–seeking behaviors also varied among Asian subgroups. Variations exist among the three subgroups of Asian American men with regard to chronic, behavioral, and mental health issues. The results provide greater understanding of the heterogeneity and relationships among the Asian American subgroups with respect to physical, behavioral, and mental health concerns. Similarities and differences in prevalence rates and use of health services must include examining the social context. Social factors such as immigration status, living environments, lifestyle, culture, and health insurance may help explain the variations among Asian American men.
Introduction
Asian Americans are one of the fastest growing ethnic minority populations in the United States. In fact, a recent survey conducted by the Pew Research Center (2012) indicates that Asian Americans have recently surpassed Latinos as the largest group of newly arrived immigrants to the United States. Research on the physical and mental health of Asian Americans is still insufficient, even after the National Latino and Asian American Study (NLAAS), the first national population-based study of Latino populations was recently made available (Alegría et al., 2004; Heeringa et al., 2004). Previous research included Asian American subgroups but with limited samples. Specifically, little is known about the overall health patterns of Asian American men, especially with regard to three subgroups: Chinese, Filipino, and Vietnamese. Given the increasing visibility of Asian Americans, more knowledge regarding their chronic, behavioral, and mental health service use will be essential for public health providers to establish culturally appropriate physical and mental health services for these groups.
With respect to substance use and behavioral issues, previous research found that Asian Americans have high rates of cigarette smoking (Centers for Disease Control and Prevention, 2004), with higher prevalence in Filipino, Korean, and Vietnamese American men compared with Chinese American men (An, Cochran, Mays, & McCarthy, 2008). Another study by Kandula, Wen, Jacobs, and Lauderdale (2009) from the California Health Interview Survey showed that Chinese men have the highest smoking rate compared with other Asian counterparts. In a study with 154 Asian American college men, Liu and Iwamoto (2007) found that almost 50% reported having drunk alcohol, 18% having used marijuana, and 8% having used any other illicit drug in the preceding 30 days before completing the survey.
In terms of obesity in Asian Americans (both foreign-born and U.S.-born) as measured by body mass index (BMI), BMI was strongly associated with length of residence in the United States. Asian Americans living in the United States in general have higher levels of abdominal fat at lower BMIs compared with Whites (Cho & Juon, 2006). Filipino Americans and Asian Indians have higher BMIs compared with Chinese Americans and “Other Asians” (Barnes, Adams, & Powell-Griner, 2008; Lee, Brancati, & Yeh, 2011). A recent study in California also showed that Filipinos have higher BMI and obesity compared with other Asian subgroups (Palaniappan, Wong, Shin, Fortmann, & Lauderdale, 2011). Self-reported racial discrimination is associated with higher BMI and obesity, and the association is stronger the longer a person has lived in the United States (Gee, Ro, Gavin, & Takeuchi, 2007). However, Asian American adults are less likely than White adults to have heart disease and hypertension (Office of Minority Health, 2011).
There are mixed findings regarding the predictive pattern of immigration variables with respect to physical health service use (Atkinson, Lowe, & Matthews, 1995; Gim, Atkinson, & Whitely, 1990). Immigration status presents significant challenges for mental health systems in minority communities, particularly in determining whether current services can adequately meet the needs of diverse Asian American groups. Asian Americans born in the United States are more likely than those who immigrated to the United States to use health care services (Kung, 2004). Asian immigrants may have unique help-seeking patterns and receive a different quality of care from mental service providers compared with their U.S.-born counterparts (Leong & Lau, 2001; U.S. Department of Health and Human Services, 2001). Also, Asian Americans are deterred from seeking mental health care and following appropriate treatment guidelines (Grant et al., 2005). With respect to health service use, social and cultural environments influence an individual’s decision to seek health services, which include cultural values and belief systems (Uehara, 2001). Manifestation of distress, negative emotion, and depression in Asians are more somatic than emotional (Takeuchi et al., 1998). Acculturation may play a role among these Asian Americans as well. For example, there are more U.S.-born Filipino living in Honolulu compared with San Francisco and more psychological distress and alcohol use among Filipinos living in San Francisco compared with Honolulu (Kim, Kim, & Nochajski, 2010). Also, Vietnamese males living in Massachusetts have a higher smoking rate compared with Vietnamese men in Seattle (N. L. Chan et al., 2007)
National data suggest that Asian immigrants generally have lower rates of major depression than U.S.-born Asians (Sue, Sue, Sue, & Takeuchi, 1995; Takeuchi et al., 1998). This is similar to data from the second wave of the National Comorbidity Survey that found that Latinos have low risk for depression (Breslau et al., 2006; Ortega, Rosenheck, Alegría, & Desai, 2000). However, in their respective cultures, somatic symptoms of mental health problems are generally accepted (Ai, 2010; Herrick & Brown, 1999). According to traditional Asian values, particularly those derived from Confucianism (Ai, Bjorck, Huang, & Appel, in press), the male is the head of the household and the primary economic provider, and help seeking may be viewed as a sign of weakness (Sue, 1996). In general, Asian American men underuse mental health services and are less likely to reveal mental health problems than White Americans (Sue, Fujino, Hu, Takeuchi, & Zane, 1991; Zhang, Snowden, & Sue, 1998). Similarly, Asian American men who support the masculine norm self-reported higher levels of depressive symptoms compared with those who do not (Iwamoto, Liao, & Liu, 2010). Cultural beliefs concerning the perceived cause of specific physical symptoms play a role in understanding an individual’s decision to seek professional health and mental health services (Fung & Wong, 2007; Hwang, Myers, Abe-Kim, & Ting, 2008). Mental illness can affect a family’s reputation for generations (Tabora & Flaskerud, 1994). Males with untreated or inadequately treated depressive symptoms show less depressive symptoms than do females (Shim, Baltrus, Ye, & Rust, 2011)
There is evidence suggesting many barriers to help-seeking patterns in Asian Americans. They include distrust of or stigma attached to psychiatric services, lack of awareness of mental health services (Boey, 1997), lack of time, insurance, English proficiency, self-reported racial discrimination (Li, Logan, Yee, & Ng, 1999), and lack of culturally and linguistically responsive mental health services (Sue et al., 1991). Research also shows that Asian refugees are more likely to report depressive symptoms than are Asian immigrants who voluntarily came to the United States (Gee, Spencer, Chen, Yip, & Takeuchi, 2007; Marshall, Schell, Elliot, Berthold, & Chun, 2005). Additionally, regional differences may influence perceived health issues. More than half of Asian Americans reside in California, New York, and Hawaii (Barnes et al., 2008). In these regions, perceived health problems may depend on the density of Asians living in that area. For example, Filipinos in Honolulu appear to have greater social support than Filipinos in San Francisco (Gee et al. 2006).
To date, most studies on Asian American men have used local samples or focused on a particular Asian subgroup. To bridge the gap, this study aims to provide an overall estimate of the chronic, behavioral, and mental health-related issues facing Asian American men, including their general health care seeking pattern, using the first nationally representative data from the National Latino and Asian American Study. In addition, we examined annual use of mental health-related services and the associations among different features of immigration, including nativity, length of residency, age of arrival, and generational status based on data from the NLAAS.
Method
Data Source and the Sample
The NLAAS is the first national population-based study of Latino and Asian American populations with data collected from May 2002 to December 2003, designed as a part of the Collaborative Psychiatric Epidemiology Studies (CPES). The sample for NLAAS consists of primary sampling units selected with probabilities proportional to size. The three stages of sampling have been previously documented and weights were developed to correct for sampling bias for the total sample (Alegría et al., 2004; Heeringa et al., 2004).
The sampling procedure for the NLAAS was previously documented and weights were developed to correct for sampling bias for the total sample and for the four Asian American subgroups (Chinese, Filipino, Vietnamese, and “Others,” which includes Koreans, East Indians, Japanese, Laotian, and so on; Alegría et al., 2004; Heeringa et al., 2004). The three stages of sampling have been previously documented and included (a) core sampling, in which primary sampling units (defined as metropolitan statistical areas or county units) and secondary sampling units (formed from contiguous groupings of census blocks) were selected with probability proportionate to size, from the primary and secondary units, housing units, and household members were sampled; (b) high-density supplemental sampling to oversample census block groups with >5% density of target ancestry groups; and (c) second respondent sampling to recruit participants from households in which one eligible member had already been interviewed (Alegría et al., 2004; Heeringa et al., 2004). Individuals of Asian ancestry who did not belong to the target groups under which these geographical areas were classified were still eligible to participate.
The sample for NLAAS consists of primary sampling units selected with probabilities proportional to size. In cases where a member of the survey population reported belonging to more than one Asian American target population the following order of priority was used to assign individuals to a single group for the purpose of the stratified sample selection: Vietnamese, Filipino, and Chinese. Using the interval estimates from other CPES studies, the NLAAS uses Bayesian methods to produce weighted estimates. The institutional review boards at the University of Washington, Cambridge Health Alliance, and the University of Michigan reviewed and approved all study protocols and procedures.
Targeting three major Asian American subgroups (Chinese, Filipino, and Vietnamese) and “Others” (Koreans, East Indians, and Japanese), with “Others” being lumped together since the sample size for these individual groups were very small. The questionnaire was available in six languages; all participants were interviewed by trained bilingual interviewers. The total sample size was 4,649, including 2,095 Asian Americans, aged 18 years or older residing in the United States. Our study sample comprised 998 Asian American men, including 284 Chinese, 235 Filipino, 243 Vietnamese, and 236 other Asian Americans.
Measures
Besides social demographics, we used chronic conditions, mental health screening and diagnosis, and health service usage and evaluations in the NLAAS data. For self-reported chronic conditions, participants were asked whether they had any health problems at any time in their lives. The list of problems included: arthritis, back problems, frequent headaches, chronic pain, allergies, stroke, heart disease, high blood pressure, asthma, chronic lung disease, diabetes, ulcer, epilepsy, and cancer.
Behavioral and drug and substance use
We calculated BMI based on self-reported height and weight to classify participants into a weight category consistent with World Health Organization (WHO) standards: underweight (BMI < 18.5), normal (18.5-24.9), overweight (25-29.9), obese (BMI ≥30). Because Asians have different associations between BMI and body fat, compared with Caucasians, we also classified the four Asian subgroups according to the BMI categories using the Asian standard (Nishida, 2004): underweight (BMI < 18.5), normal (18.5-22.9), overweight (23-24.9), and obese (≥25). Smoking and other drug use were also assessed and were self-reported. We used self-reported substance use items, including recreational drugs (“Other drug use”) such as marijuana and cocaine.
Mental health issues
Self-reported mental health measurements were based on the Diagnostic and Statistical Manual of Mental Disorders, fourth edition (DSM-IV; American Psychiatric Association, 1994). We also examined the prevalence of 12-month depression and self-rating. The World Mental Health Survey Initiative version of the World Mental Health Survey Initiative of the World Health Organization Composite International Diagnostic Interview (WMH-CIDI; Kessler & Ustun, 2004) was used to assess 12-month presence of depression using criteria from the DSM-IV. For service seeking frequency, we included participants’ self-reported mental health service use and visits to physicians and mental health professionals.
Statistical Analysis
We performed descriptive analyses for selected variables. The actual number of cases was reported for the whole group, three major subgroups, and for “Other group.” Their representative percentage in the population was computed and reported using weights to correct potential sampling bias. The weights are created based on demographical, social, and economical variables. Chi-square tests were used to compare subgroup differences in categorical variables among men in four categories. All analyses were performed using SPSS version 18 (IBM Corporation, Somers, NY); statistical significance was determined at p < 0.05.
Results
Demographics
Among the Asian American men in our analysis, the median age was 39 years and the mean was 41.3 years, ranging from 18 to 95 years; the median education was 15 years, and the mean was 14.01, ranging from fourth grade to 17 years. The income is measured using the 2001 Census household income/needs ratio, with a median of 5 and a mean of 6.03, ranging from 4.95 to 17. The average English proficiency was 2.87 (range = 1-4), with 4 being the most proficient. The years in United States was coded in 5 categories to show the relative length of immigration to this country and in the case of native born. They were given the rank a level higher than the highest rank in terms of years: 1 = <5 years, 2 = 6 to 10 years, 3 = 11 to 20 years, 4 = ≥21 years, 5 = Born in the United States. The median category was 3 and the mean was 3.3 (range = 1.33-5.00). Subgroup differences in these variables are presented in Table 1.
Demographic and Acculturation Variables for Asian Men, National Latino and Asian American Study, 2002-2003 (N = 998)

Other ethnic group: East Indians, Japanese, Koreans, etc.
p values reported here are from chi-square crosstabs for percentages or analysis of variance for means among different ethnic groups.
Physical Health and Chronic Conditions
There are no ethnic differences among 11 out of 15 physical illness conditions, but the remaining rates varied among ethnic subgroups. Chinese had the highest rates for allergies/hay fever whereas the “Other group” had the lowest. Filipinos had the highest rate of high blood pressure and asthma, whereas both Chinese and Vietnamese had the lowest rates (Table 2).
Number and Weighted Percentages of Chronic Conditions Reported by Asian American Men by Ethnic Subgroup, National Latino and Asian American Study, 2002-2003
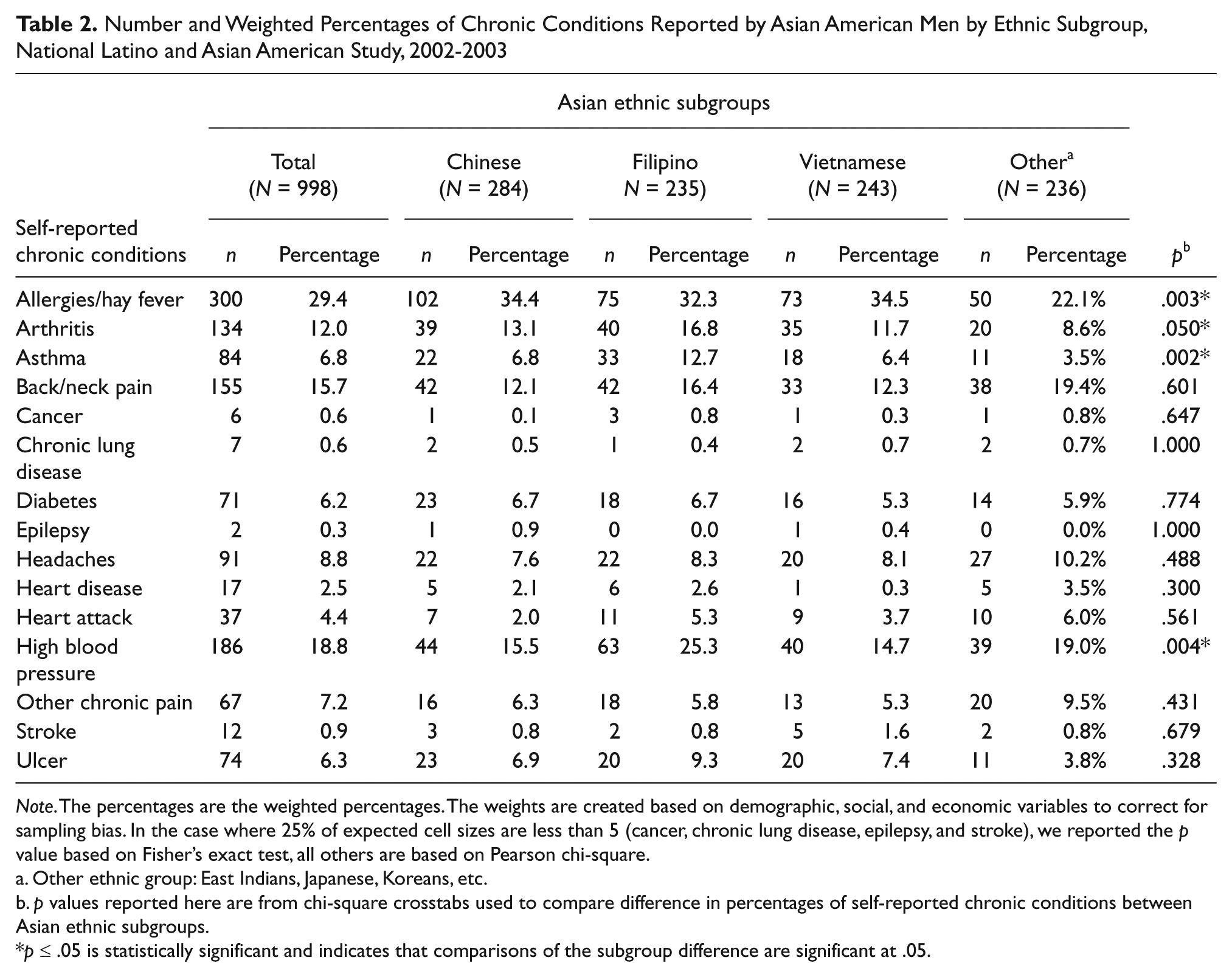
Note. The percentages are the weighted percentages. The weights are created based on demographic, social, and economic variables to correct for sampling bias. In the case where 25% of expected cell sizes are less than 5 (cancer, chronic lung disease, epilepsy, and stroke), we reported the p value based on Fisher’s exact test, all others are based on Pearson chi-square.
Other ethnic group: East Indians, Japanese, Koreans, etc.
p values reported here are from chi-square crosstabs used to compare difference in percentages of self-reported chronic conditions between Asian ethnic subgroups.
p ≤ .05 is statistically significant and indicates that comparisons of the subgroup difference are significant at .05.
Behavioral Health and Substance Use
In Table 3, we computed BMI for Asian American men (using WHO standard): 2.3% underweight, 51.4% normal, 36.5% overweight, and 9.7% obese. However, using the BMI (Asian) categories, there were 2.3% underweight, 30.8% normal, 20.6% overweight, and 46.2% obese men. There were considerable variations across four subgroups: Filipino Americans had the highest obesity rates (20.7%) and overweight (44.8%; BMI using WHO standard), followed by “Others” (43.3% overweight) and Chinese Americans (31.1%). Vietnamese American men had the highest rate of normal weight (76.6%). For substance use, 20.1% were current smokers, 21.4% were former smokers, 24.6% had ever used marijuana, 6.2% had ever used cocaine, 6.1% had abused prescription medication, and 5.2% had ever used other drugs. Subgroup differences were as follows: Vietnamese American men had the highest rate of current smokers (29.4%) and past smokers (27.4%), Filipino Americans (25.0% and 27%, respectively). On the other hand, Filipino American men reported the highest rate of marijuana use (46.1%), cocaine use (12.7%), prescription drug abuse (12.1%), and other drug use, far above any other subgroups, whereas Vietnamese American men had lowest rates for all four drug-related measures.
Behavioral Risk Factors (Obesity and Substance Use) in Asian American Men by Ethnic Subgroup, National Latino and Asian American Study, 2002-2003
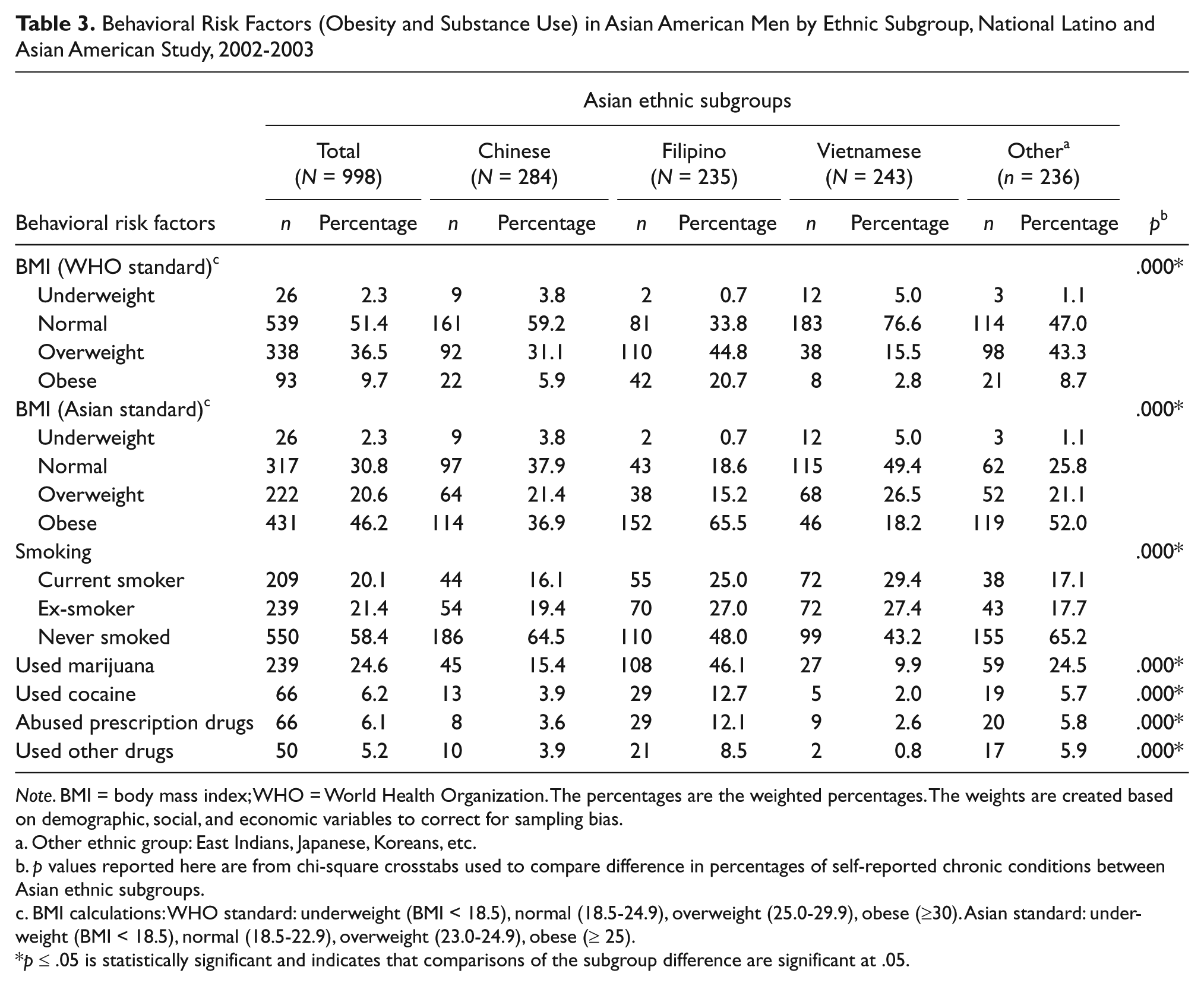
Note. BMI = body mass index; WHO = World Health Organization. The percentages are the weighted percentages. The weights are created based on demographic, social, and economic variables to correct for sampling bias.
Other ethnic group: East Indians, Japanese, Koreans, etc.
p values reported here are from chi-square crosstabs used to compare difference in percentages of self-reported chronic conditions between Asian ethnic subgroups.
BMI calculations: WHO standard: underweight (BMI < 18.5), normal (18.5-24.9), overweight (25.0-29.9), obese (≥30). Asian standard: underweight (BMI < 18.5), normal (18.5-22.9), overweight (23.0-24.9), obese (≥ 25).
p ≤ .05 is statistically significant and indicates that comparisons of the subgroup difference are significant at .05.
Mental Health Status and Health Service Seeking
Table 4 presents the mental health ratings of Asian American men. The rates of mental health status as “excellent,” “very good,” and “good” were 37.3%, 32.7%, and 23.3%, respectively, whereas rates identified as “fair or poor” were 6.0% and 0.7%, respectively, for the overall sample. Reporting of DSM-IV major depressive disorder over the last 12 months was 4.6%, for the overall sample. The levels of self-rating of mental health and the levels of seeking help varied among Asian subgroups. Among all subgroups, Vietnamese American men reported the highest rates of “poor” mental health (3.6%), whereas Chinese Americans reported the highest for “fair” mental health. There is little group difference on rates of depression.
Asian American Men’s Mental Health Ratings by Ethnic Subgroup Using National Latino and Asian American Study, 2002-2003

Note. The percentages are the weighted percentages. The weights are created based on demographic, social, and economic variables to correct for sampling bias. The World Health Organization Composite International Diagnostic Interview (WMH-CIDI) was used to assess 12-month presence of depression using criteria from DSM-IV.
Other eEthnic group: East Indians, Japanese, Koreans, etc.
p values reported here are from chi-square crosstabs used to compare difference in percentages of self-reported chronic conditions between Asian ethnic subgroups.
Mental health self-rating categories: excellent = 5, very good = 4, good = 3, fair = 2, poor = 1.
p ≤ .05 is statistically significant and indicates that comparisons of the subgroup difference are significant at .05.
Overall, Asian American men reported low levels of health care seeking patterns with respect to either the whole group or subgroups (all <4% across all types of providers). Across all subgroups, Chinese American men and Vietnamese American men had a lower rate of ever seeking mental health professionals compared with Filipino American men (Table 5).
Asian American Men’s Mental Health Service Seeking by Ethnic Subgroup Using National Latino and Asian American Study, 2002-2003

Note. The percentages are the weighted percentages. The weights are created based on demographic, social, and economic variables to correct for sampling bias.
Lifetime-ever seek includes all types of providers—general practitioner, family/general practice medical doctor; specialist—psychiatrist, psychologist; other health providers—DO, RN, OT/PT, MSW, counselor, other mental health provider, religious or spiritual healer.
Other ethnic group: East Indians, Japanese, Koreans, etc.
p values reported here are from chi-square crosstabs used to compare difference in percentages of self-reported chronic conditions between Asian ethnic subgroups.
p ≤ .05 is statistically significant and indicates that comparisons of the subgroup difference are significant at .05.
Discussion
As public health providers often need to address the individual and community health, this study provides the prevalence of the overall health of Asian American men in the first nationally representative database, the NLAAS. Further, our findings demonstrate chronic, behavioral, and mental health issues in three Asian American subgroups as well as “Other Asians”. In this regard, this national study may be among the first of its kind to show the variations among subgroups of Asian American men. Although there are both differences and similarities across the four categories, Asian American men as a whole subpopulation in the United States constitute a significant patient pool with very high mental health utilization rates. These patterns appear to contradict the earlier assumptions (Sue et al., 1991; Zhang et al., 1998) but are consistent with recent findings in health care service use (Kung, 2004). This fact may result from the combination of available health insurance for more recent educated immigrants adhering to Asian heritages and collectivist cultural traditions of respecting authorities (Ai, Huang, Bjorck, & Appel, 2012).
Given our findings, public health practitioners may be better prepared to serve, and have greater impact on, the Asian American population if they are equipped with more pertinent knowledge of their overall health. We used a nationally representative sample surveyed in a culturally and linguistically appropriate way, which improved from previous studies with data limitations. As indicated from our results, Asian American men in the sample had high rates of chronic conditions, namely allergies/hay fever and high blood pressure, but they also experience high prevalence of back/neck pain. The latter may partly reflect the high tendency of somatization reported in Asian American health literature (Ai et al., 2012). Despite high rates of hypertension, rates of heart attack or stroke are relatively low. Particularly noteworthy, Filipino American men had considerably higher rates of hypertension compared with other subgroups, though their high rates of diabetes are about the same as Chinese American men. These cross-ethnic differences may be partly attributable to varied living environments, lifestyles, and cultural heritages. However, this assumption needs further investigation to prepare culturally appropriate intervention with different subgroups.
Nearly half of Asian American men in the study meet the criteria for being overweight or obese. This behavioral risk factor could be greater, given that Asian Americans living in the United States tend to have higher levels of abdominal fat at lower BMIs compared with Whites (Cho & Juon, 2006). In particular, our findings indicate alarming levels of overweight and obese Filipino Americans (66%). Accordingly, their high prevalence of hypertension and weight may qualify more Filipino Americans for metabolic symptoms that need clinical attention, more than any other Asian American men’s subgroups. Latinos have comparable rates of obesity and high BMI compared with Asian American men (Borrell & Dallo, 2008). In terms of substance abuse, smoking and marijuana usage are prevalent in one fifth to one fourth of all Asian American men, the latter rate being substantially higher than in a recent report (18% marijuana use; Liu & Iwamoto, 2007). Again, Filipino American men reported the highest prevalence of using or abusing all studied drug categories, compared with other subgroups in the study, whereas their smoking rates is similar to that of Vietnamese.
Interestingly, more Filipino American men rate their mental health as excellent or very good compared with self-reports by Chinese and Vietnamese American men, whereas the Vietnamese group reports the highest rates of major depression over the last 12 months. The majority of Asian American men rate their mental health as good to excellent and less than 5% reported a diagnosis of major depression over the preceding 12 months, similar to Asian American women (Appel, Huang, Ai, & Lin, 2011). However, cautious interpretation of these apparently favorable rates of mental health is warranted because somatization is culturally acceptable in Asian traditions and mental health problems could manifest as chronic pain (Ai et al., 2012). Our findings also show high rates of chronic pain among Asian American men, which could be somatic or could indicate stress. Indeed, the literature found the lack of awareness of mental health services among Asian Americans (Boey, 1997) and related immigration stress and discrimination factors to their physical, behavioral, and mental health (Ai et al., 2012; Atkinson et al., 1995; Gee et al., 2008).
The low help-seeking patterns in Asian Americans may be due to distrust or a stigma attached to seeking services (Boey, 1997), lack of English proficiency (Li et al., 1999), or culturally insensitive providers (Sue et al., 1991). Even so, Asian Americans rank their health higher compared with Latino Americans, who rank their health the lowest compared with Whites and African Americans (Liang et al. 2010). Health care systems and practitioners must develop culturally responsive services to meet the needs of minority groups in order to form efficient and cost effective care. Such sensitivity might result in better communication and treatment between health and social care providers and Asian American consumers. Therefore, it is beneficial for public health providers to learn more about the chronic issues affecting various subgroup populations in the United States. Although this study provides an overview of major health issues facing Asian Americans, marked differences among the major ethnic groups warrant further investigation, paying attention to the cultural context. Future research should explore protective and risk factors in Asian American subgroups to provide more evidence and awareness of the importance of culturally appropriate treatments. Practitioners and researchers should also examine whether variables such as health beliefs may play a part in seeking health care services for behavioral, physical, and mental health services, and whether cultural factors play a role as well in self-reported mental health. Finally, there might be major regional differences within these Asian American subgroups, and future research should consider such differences.
Limitations
Several limitations should be acknowledged. The cross-sectional data do not permit any assumption about causality. Because the NLAAS underinvestigated three major subgroups of Asian America men (East Indian, Japanese, and Korean Americans), the findings in this study may not be generalizable. The “Other” group is a mixed group and individual subethnicity cannot be identified in the public data that are available for analysis for this article. Even for the three big groups that are identified as “Chinese,” “Vietnamese,” and “Filipino,” the data are unconfirmed self-report and we should only make conservative inferences since self-reported health conditions present a limitation of the existing dataset. Additionally, the NLAAS public data provides very limited regional information, which prevented us from analyzing possible regional differences within the Asian subgroups for chronic conditions, behavioral health, and mental health care utilization. Furthermore, the NLAAS was based on psychiatric disorders defined by the Western DSM-IV, which allowed us to compare mental disorders within the same measure. However, rates of mental disorders may have been underestimated, as different ethnic groups might express their mental health problems in distinctive ways not identified in the DSM-IV.
Finally, the NLAAS data are now nearly 10 years old. Compared with their conditions during 2002 to 2003, some changes have occurred relative to the health of the new generation of Asian American immigrants and their service utilization. Similar to our results, other studies found that Asians have lower rates of overweight and obesity than Whites (J. C. N. Chan et al., 2009). Although Asians have lower body mass index, they have higher rates of type 2 diabetes compared with whites (Palaniappan et al., 2011). Moreover, the report released by the Pew Research Center (2012) provides a comprehensive picture of Asian Americans compared with other racial groups (Whites, Hispanics, and Blacks) on several measures. Although health data were not included in the report, several measures related to health may be worth noting—education, income, language, group relations, residential segregation, sense of identity and belonging, and perceptions of discrimination (Pew Research Center, 2012). Even so, our research underscores the importance of increasing awareness of cross-cultural and gender differences of chronic, behavioral, and mental health issues in Asian American men to better inform health care providers and researchers since there are limited research about Asian American men. The health of Asian Americans has major implications for the future of public health since they are a rapidly growing population and relatively young because of the large proportion of new immigrants.
Despite the limitations, our findings are important to increase awareness of cross-cultural differences and similarities with regard to chronic, behavioral, and mental health issues among various Asian American subgroups that may also apply to other racial groups such as Hispanics and Blacks. Our findings on Asian American subgroup differences will inform the culturally sensitive design of future physical and mental health services for such “highly heterogeneous” populations (Brady, 2007) and extend our understanding of subgroup differences in other racial groups. For example, findings from the same data set indicate subgroup differences among Latino American men’s health and health care utilization (Ai, Noel, Appel, Huang, & Hefley, in press). Our results reveal the majority of Asian Americans are foreign-born (77%), which mean their diversity will provide opportunities for research on acculturation, assimilation, and socioeconomic factors in physical and mental health issues. Public health and clinical providers could deliver better care services for ethnic subgroup Asian American men, if they are more adequately informed concerning the differential patterns in overall health, as presented in the our analysis. Practitioners should be attentive to comorbid mental and physical health issues related to immigration. Specifically, rates of comorbid disorders, help seeking, and use of health services may differ for Asian Americans who have recently immigrated to the United States, compared with U.S.-born Asian Americans.
Footnotes
Authors’ Note
The opinions expressed in this article are those of the authors and do not necessarily reflect the views of the Pittsburgh Center for Race and Social Problems.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was supported by a grant from the Pittsburgh Center for Race and Social Problems to Amy L. Ai.