
Abstract
Although the Latino American male population is increasing, the subgroup Latino men’s health remains underinvestigated. This study examined the overall pattern of Latino male health and health care utilization in major subgroups, using a nationally representative sample (N = 1,127) from the National Latino and Asian American Study. The authors evaluated rates of chronic, behavioral, and mental health service utilization in this first nationally representative survey. The results identified significant cross-subgroup differences in most physical and chronic conditions with Puerto Rican American men having high rates in 8 of 15 physical ailments, including life-altering conditions such as cardiovascular diseases. Despite differences in racial/ethnic, socioeconomic, and cultural factors, Cuban American men shared similar rates of heart diseases and cancer with Puerto Rican American men. In addition, Puerto Rican American men had higher rates of substance abuse than other Latinos. For health providers, the authors’ findings encourage awareness of subgroup differences regarding overall health issues of Latino American men to provide culturally appropriate care.
Keywords
Introduction
Latino Americans constitute the fastest growing ethnic minority populations in the United States, projected to more than double between 2000 and 2050 (Ortman & Guarneri, 2009). Latinos have become the largest ethnic minority group in the United States, comprising more than 15% of its population (U.S. Census Bureau, n.d.). For instance, certain Latino male subgroups are increasingly visible in the blue color work force (e.g., farm workers). Yet few studies have focused on overall health patterns of Latino American men, especially with regard to their three major subgroups—Cuban, Mexican, and Puerto Rican Americans. Latinos constitute a racially and culturally heterogeneous ethnic group that historically has arrived or remained in the United States for different reasons, including economic opportunity and/or political persecution (Derose, Bahney, Lurie, & Escarce, 2009; Guisepi, 2009; Lee & Rytina, 2008). These Latino subgroups vary considerably in racial and ethnic heritages, major residency in geographic locations, and socioeconomic status (SES; e.g., different sizes of earning gaps; Torres Stone & McQuillan, 2007). These factors require both gender- and ethnicity-specific health analyses (Flores et al., 2002; Kessler & Üstün, 2004; Torres Stone & McQuillan, 2007). Below, we summarize the current literature on physical health, behavioral health, and care utilization patterns of Latino Americans with limited available information on the Latino male subgroups.
Disparities in physical health experienced by Latino Americans have been reports from large-sample studies, especially from the National Latino and Asian American Study (NLAAS), the first nationally representative study of Latino Americans (Alegría et al., 2004; Heeringa et al., 2004). For example, Latinos, though younger (partly because of large inflows of new immigrant labor forces) compared with non-Latinos, were more likely to report having diabetes and higher mean body mass index (BMI; Borrell & Dallo, 2008). The incidence of self-reported diagnosed diabetes has increased from 6.6 per 1,000 to 9.1 per 1,000 from 1997 to 2003 among Latino Americans (Geiss et al., 2006).
Most studies on Latino Americans, however, have used self-rated health (SRH) rather than itemized chronic conditions as major causes for U.S. Latinos’ mortality (i.e., diabetes, stomach cancer, liver cancer, human immunodeficiency virus/acquired immunodeficiency syndrome, and liver disease; National Center for Health Statistics, 2011). The assessment of SRH can present limited, if not biased, information. An earlier study showed that Mexican Americans’ SRH tended to be fair or poor, whereas their doctors’ evaluations of their health tended to be excellent or very good (Angel & Guarnaccia, 1989). A recent national trend analysis found that among individuals 50 years and older, Latinos’ SRH ranked worst, when compared with their non-Latino White and African American counterparts (Liang et al., 2010). National Health Interview surveys associated poor SRH with higher levels of SES and acculturation among Mexican Americans, but this same rating was associated with lower levels of SES and acculturation among Caribbean Americans (Zsembik & Fennell, 2005). However, other researchers have suggested that differences found in SRH may or may not be attributed to SES (Bzostek, Goldman, & Pebley, 2007; Kandula, Lauderdale, & Baker, 2007; Patel, Eschbach, Rudkin, Peek, & Markides, 2003) but better explained by language difference and preference (Bzostek et al., 2007; Viruell-Fuentes, Morenoff, Williams, & House, 2011). Particularly, showing a preference for speaking in Spanish or having greater Spanish language proficiency was consistently associated with poor SRH (Bzostek et al., 2007; Viruell-Fuentes et al., 2011).
Disparities in mental health and behavioral health issues experienced by Latino Americans appear to be a complicated matter with respect to prevalence and severity. Data from the National Comorbidity Survey and its second wave suggest that Latinos have low risk for certain common internalizing disorders (e.g., depression, general anxiety disorder, social phobia, dysthymia, oppositional-defiant disorder, and attention deficit/hyperactivity disorder; Breslau et al., 2006; Ortega, Rosenheck, Alegría, & Desai, 2000) and for lifetime substance use (Breslau et al., 2006). However, though Latinos were at low risk for mood disorders (e.g., depression) when they did present with the condition, they tended to be more chronically ill (Breslau et al., 2006). Furthermore, depression as a comorbidity with physical illnesses tended to negatively affect Latinos with type 2 diabetes more than their counterparts in other ethnic groups (Mier et al., 2008). In addition, although depressed Latinos tended to have lower SRH, Bzostek et al. (2007) failed to support somatization as an explanation. Others have related increased rates of psychiatric disorders and substance abuse to U.S.-born, English language–proficient and third-generation Latinos with higher levels of acculturation (Alegría, Mulvaney-Day, Torres, et al., 2007; Ortega et al., 2000). Again, these factors underscore the importance of gender- and ethnic-subgroup analyses for Latinos’ overall health pattern given their differences in language proficiency and immigration experiences.
With respect to subgroups among Latino Americans in the NLAAS, Puerto Ricans reported the highest overall prevalence rates of psychiatric disorders (Alegría, Mulvaney-Day, Torres, et al., 2007). Subgroup data, however, were further complicated by the status of nativity. For example, the U.S.-born status was related to poor mental and physical health of Mexicans but to better mental health for Cubans and Dominicans and better physical health for Puerto Ricans (Jerant, Arellanes, & Franks, 2008). Foreign-born Mexican Americans had lower prevalence rates of most psychiatric disorders, compared with their U.S.-born counterparts (Alegría, Canino, Stinson, & Grant, 2006). The protection of nonnativity against psychiatric morbidity among Mexican Americans, however, appears not to be generalizable to Puerto Rican and Cuban Americans (Alegría et al., 2006). In this regard, Vega, Canino, Cao, and Alegría’s (2009) analyses of NLAAS offered the gender-specific information: U.S.-born Latinos were more likely to report a dual diagnosis of both substance and nonsubstance mental disorders than were foreign-born Latinos in both sexes.
Concerning utilization of physical health care, 27% to 34% of Latino Americans nationwide do not have health insurance or access to a usual source of care, respectively (Pérez-Escamilla, 2010). The Medical Expenditure Panel Survey found that all foreign-born Hispanics in the United States are less likely to have prescription medications but recent immigration was associated with being less likely to have had ambulatory or emergency room visits (Weinick, Jacobs, Stone, Ortega, & Burstin, 2004). In California, 7% of Latinos reported perceived health care discrimination and U.S.-born and foreign-born Latinos were more likely to report being discriminated against in the U.S. health care system than their non-Latino White counterparts in either category (Lauderdale, Wen, Jacobs, & Kandula, 2006). Also, within these findings were Latino subgroup differences in that Mexicans, Central Americans, Caribbeans, and Southern-Latino Americans were less likely to have any prescription medications. In addition, Mexicans and Cubans were less likely, where Puerto Ricans were more likely, to have had emergency department visits, compared with non-Latino White individuals. Cuban and Puerto Rican American elderly were 2.3 and 2.6 times more likely, respectively, to have seen a physician than were their Mexican counterparts (Burnette & Mui, 1999). Mexicans were less likely than Puerto Ricans to know about glycosylated hemoglobin and to have only one doctor for their diabetes care and management (Mainous, Diaz, Saxena, & Geesey, 2007).
On the other hand, rates of mental health service use among Latino Americans have grown considerably over the past decade, compared with rates in the 1990s (Alegría, Mulvaney-Day, Woo, et al., 2007). However, when compared with non-Latino White populations, Latinos are less likely to receive or use medications for any mental illness (Reyes, Van de Putte, Falcón, & Levy, 2004). Instead, they are more likely to prefer counseling (Cooper et al., 2003) provided by their doctors (Noël, 2010; Noël & Pomeroy, 2011), which also seems to lower their rates of outpatient mental health service use (Garland et al., 2005). Additionally, they were found to be less apt to receive specialty mental health care (e.g., psychiatrists or psychologists) than either African American or non-Latino White patients (Miranda & Cooper, 2004). In particular, Latino Americans were much less likely to report receiving recent depression care (Lagomasino et al., 2005), or to receive antidepressant medications (Miranda & Cooper, 2004), and tended to have a lower antidepression treatment rate, if diagnosed (Guevara, Mandell, Rostain, Zhao, & Hadley, 2006) than were non-Latino Whites.
Despite the increasing documentation of subgroup analysis on studies of Latino Americans, gender-specific analysis on subgroup Latino Americans remains scarce. The limited literature suggests that less acculturated Latino men were one and one half times as likely to be current smokers or have a high BMI, compared with their women counterparts (Abraido-Lanza, Chao, & Florez, 2005). Puerto Rico men were more likely than women to have better perceived mental and physical health (Albizu-Garcia, Alegría, Freeman, & Vera, 2001). Furthermore, Latino men had higher rates of dual diagnosis than women (16.88% vs. 5.02% for males, p < .000, and 7.48% vs. 0.58% for women, p < .000; Vega et al., 2009). Among Puerto Ricans, the definite need for mental health care and poor self-reported mental health had larger impacts on service utilizations for men than for women (Albizu-Garcia et al., 2001). Recently, our analysis has documented considerable variations in overall health patterns among the NLAAS Latino female subgroups. Puerto Rican American women reported the highest rate of asthma, whereas Mexican American women reported the highest rate of diabetes. Cuban American women reported the highest rate of hypertension and heart diseases (Ai, Appel, Huang, & Lee, 2012). The Cuban American women sample had the lowest rate of obesity (18.8%), compared with Puerto Ricans (30.7%) and Mexicans (32.9%; obesity = BMI ≥ 30). Puerto Rican American women saw “other health provider” the most, whereas Mexicans saw specialists the least.
To our knowledge, there has been no comprehensive gender- and ethnic-specific information on Latino men in the NLAAS. If findings on these subgroup patterns of Latino men differ from those of Latinas, then gender may play an important role in addition to biological and psychosocial subgroup factors to make impacts on their overall health and utilization. To bridge the gap, this study aims to provide the general estimation of chronic, behavioral, and mental health-related issues facing Latino American men and to provide ethnic/racial subgroup comparisons, using the first nationally representative data from the NLAAS. These analyses will also include a subgroup comparison of Latino men’s general health care–seeking pattern.
Method
The Sample and Data Source
The NLAAS is the first national population-based study of Latino and Asian American populations with data collected from May 2002 to December 2003, designed as a part of the Collaborative Psychiatric Epidemiology Studies. The NLAAS consists of primary sampling units selected with probabilities proportional to size. The three stages of sampling have been described extensively elsewhere and weights were developed to correct for sampling bias for the total sample (Alegría et al., 2004; Heeringa et al., 2004). Using the interval estimates from other Collaborative Psychiatric Epidemiology Studies, the NLAAS used Bayesian methods to produce weighted estimates.
The questionnaire is available in six languages, including Spanish. The total sample size of the NLAAS is 4,649, including 2,554 Latinos, aged 18 years or older residing in the United States. The total sample size in this analyses was 1,127, which consisted of three major subgroups of Latino American men—Cuban (n = 276), Puerto Rican (n = 213), Mexican (n = 398), and “other” (n = 240). Institutional review board approvals were gained and informed consent was received from all study participants.
Measures
The NLAAS data included social demographics, mental health screening and diagnosis, health service usage, and evaluations, among other data. Besides social demographics, this analysis used self-reported chronic conditions, mental health screening and diagnosis, and health service usage and evaluations collected by the NLAAS interviewers.
Chronic conditions
Participants were asked whether they had had any health problems at any time in their lives. The list of problems included arthritis, back problems, frequent headaches, chronic pain, allergies, stroke, heart disease, high blood pressure, asthma, chronic lung disease, diabetes, ulcer, epilepsy, and cancer.
Behavioral health indices
We calculated BMI based on self-reported height and weight to classify participants into a weight category consistent with World Health Organization standards: underweight (BMI < 18.5 kg/m2), normal (18.5-24.9 kg/m2), overweight (25-29.9 kg/m2), obese (BMI ≥ 30 kg/m2). Smoking and other drug use in the NLAAS were self-reported items. These included marijuana and cocaine, as well as other recreational drugs (“Other drug use”).
Mental health problems
Self-reported mental health measurements were based on the Diagnostic and Statistical Manual of Mental Disorders (4th ed., American Psychiatric Association, 1994). We examined the prevalence of depression over the past 12 months and rates of self-rating mental health. The World Mental Health Survey Initiative version of the World Health Organization Composite International Diagnostic Interview (Kessler & Üstün, 2004) was used to assess 12-month presence of depression using criteria from the DSM-IV. For service-seeking frequency, we included participants’ self-reported mental health service use and visits to physicians and mental health professionals.
Acculturation variables
English proficiency was constructed by averaging three items, respectively, rating speaking, reading, and writing fluencies (Cronbach’s α = .97). Birthplace was dichotomized (0 = foreign-born, 1 = U.S.-born). Years in the US was categorized as for levels (0 -5, 6 -10, 11 -20, and 21 years), while the U.S.-born participants were assigned the highest score to avoid missing values. The average time in the United States was. Acculturation stress, capturing strains associated with culture change (Cervantes, Padilla, Amando, & Salgado de Snyder, 1990), was assessed with a 10-item scale (Vega et al., 1998) for immigrant respondents, with Yes (coded 1) or No (coded 0) to each question (e.g., “Do you find it hard interacting with others because of difficulties you have with the English language?”). Items are averaged to produce a mean score (higher score indicates higher stress, α = .58), and the U.S.-born status was assigned the value 0 to avoid missing values. Discrimination was assessed using a 9-item scale on a 6-point Likert-type scale for each item (1 = never, 6 = almost every day), rating how often the respondent experienced various forms of discrimination in daily life (e.g., “You receive poorer services than other people at restaurants or stores,” “You are treated with less courtesy than other people,” and “You are treated with less respect than other people”; Gee, Spencer, Chen, Yip, & Takeuchi, 2007). The nine items were averaged to produce a mean score (α = .91).
Statistical Analysis
Analyses were conducted in two phases. First, descriptive analyses were used for all variables of major interest. The actual number of cases was reported for all Latinos in the data set and for the three major ethnic subgroups, as well as for a fourth group involving all “Other” Latinos (e.g., Chileans, Argentines). The representative percentage for each group was computed and reported using weights to correct potential sampling bias. Second, chi-square tests were performed to compare differences in categorical variables among the selected Cuban, Mexican, Puerto Rican, and other Latino American men. Weights were created for the data presented in the results to correct for sampling bias. All analyses were performed using SPSS version 18 (IBM Corporation, Somers, NY). Statistical significance was determined at an alpha level of .05 for all tests.
Results
Demographics
Average age of the sample was 39.94 years (SD = 15.5; range = 18-92 years). Average education was 11.48 years (SD = 3.94; level range = fourth grade to 17 years). Average income was 4 (SD = 3.97), measured using the 2001 Census household income/needs ratio (range = 0-17). Average English proficiency was rated at the level of 2.49 (SD = 1.15; range = 1-4), with 4 being the most proficient. The average time in the United States was rated at the level of 3.72 (SD = 1.30; categorical range = 1-5). Table 1 presents all categorical information.
Demographic and Acculturation Variables for Latino American Men in the National Latino and Asian American Study, 2002-2003 (All Sample N = 1,127)

Note. Age, acculturation stress and discrimination are continuous variables; education level ranges from fourth grade to 17 years; income is measured using the 2001 Census household income/needs ratio. English proficiency level goes from 1 to 4, with 4 being the most proficient. Years in the United States are measured in these categories: 1 = less than 5 years, 2 = 5 to 10 years, 3 = 11-20 years, 4 = ≥21 years, 5 = born in United States.
Physical Health and Chronic Conditions
As shown in Table 2, rates of physical illness conditions varied, with allergies (17.2%), back/neck pain (15.1%), hypertension (12.9%), arthritis (11.8%), headaches (10.9%) were reported most frequently, whereas chronic lung diseases (0.9%) ranked the lowest for all Latino men in the NLAAS. However, there were considerable differences in most categories among Latino American ethnic subgroups. Out of 15 chronic conditions, rate differences on eight items were statistically significant across subgroups. Puerto Rican American men had the highest rates on all of them: allergies (22.0%), arthritis (15.1%), asthma (20.4%), back/neck pain (22.7%), epilepsy (5.0%), heart disease (4.8%), heart attack (6.4%), and hypertension (18.1%). Cuban American men shared similar rates of heart diseases and cancer with Puerto Rican American men; and both had higher rates of each than did Mexican American men.
Number and Weighted Percentages of Chronic Conditions Reported by Latino American Men in Total and Ethnic Subgroups of the NLAAS

Note. NLAAS = National Latino and Asian American Study. The percentages are the weighted percentages. The weights are created based on demographical, social, and economical variables to correct sampling bias.
Other ethnic group = Costa Ricans, Ecuadorans, Guatemalans, Hondurans, and so on.
p values reported here are from chi-square crosstabs used to compare difference in percentages of self-reported chronic conditions between Latino American ethnic subgroups. p < .05 is statistically significant and indicates that comparisons of the subgroup difference are significant at .05.
Behavioral Health and Substance Use
In Table 3, we computed BMI for all Latino American men (using World Health Organization standards: 0.8% underweight, 24.9% normal, 44.4% overweight, and 29.9% obese) in the NLAAS. Across the major subgroups were substantive variations: Puerto Rican American men had the highest underweight rate (2.3%), Cuban American men had the highest overweight rate (50.4%), and Mexican American men had the highest obesity rate (32.5%).
Behavioral Risk Factors (Obesity and Substance Use) Reported by Latino American Men in Total and Ethnic Groups of the NLAAS

Note. NLAAS = National Latino and Asian American Study; BMI = body mass index; WHO = World Health Organization. The percentages are the weighted percentages. The weights are created based on demographical, social, and economical variables to correct sampling bias.
Other ethnic group = Costa Ricans, Ecuadorans, Guatemalans, and Hondurans, and so on.
p values reported here are from chi-square crosstabs used to compare difference in percentages of self-reported chronic conditions between Latino American ethnic subgroups. p < .05 is statistically significant and indicates that comparisons of the subgroup difference are significant at .05.
BMI calculations: WHO standard: underweight (BMI < 18.5 kg/m2), normal (18.5-24.9 kg/m2), overweight (25-29.9 kg/m2), obese (≥30 kg/m2).
For substance abuse, 26.4% were current smokers, 24.9% were former smokers, 39.2% had ever abused marijuana, 17.5% had ever abused cocaine, 9.7% had abused prescription medication, or ever abused other drugs, respectively. Subgroup differences across these substance abuse categories were also found with the exception of abused prescription drugs. Mexican American men reported the highest rate of ex-smokers (27.4%), whereas Cuban American men had lowest rates for all four drug-related measures. Puerto Rican American men reported the highest incidence of current smokers (33.4%), marijuana abuse (53.4%), cocaine abuse (27.3%), and other drug abuse (11.9%), which were also far above those of any other subgroups.
Mental Health Status and Health Service Seeking
For the mental health status, rates as “excellent,” “very good”, and “good” were reported by 34.6%, 27.6%, and 26.5% of the whole group, respectively, whereas rates as “fair” or “poor” were reported by 10.9% and 0.4%, respectively (see Table 4). Among the four subgroups, Cuban American men reported the highest rates of categorizing their mental health as “poor” (0.9%) and “excellent” (44.7%), whereas Mexican Americans reported the highest rates of categorizing their mental health as “fair” (13.5%). Reporting of DSM-IV major depressive disorder over the past 12 months was 6.4% with no significant difference across subgroups.
Mental Health Ratings Reported by Latino American Men in Total and Ethnic Groups of the NLAAS

Note. NLAAS = National Latino and Asian American Study. DSM-IV = Diagnostic and Statistical Manual of Mental Disorders, fourth edition. The percentages are the weighted percentages. The weights are created based on demographical, social, and economical variables to correct sampling bias.
The World Health Organization Composite International Diagnostic Interview was used to assess 12-month presence of depression using criteria from DSM-IV.
Other ethnic group = Costa Ricans, Ecuadorans, Guatemalans, and Hondurans, and so on. p values reported here are from chi-square crosstabs used to compare difference in percentages of self-reported chronic conditions between Latino American ethnic subgroups. p < .05 is statistically significant and indicates that comparisons of the subgroup difference are significant at .05.
Mental health self-rating categories: excellent = 5, very good = 4, good = 3, fair = 2, poor = 1.
As for health care–seeking patterns, Latino American men reported lifetime-ever seeking mental health service at 15.9 % (Table 5). However, their seeking levels over the past 12 months were low with respect to either the whole group or subgroups (all <5% across all types of providers). Across four subgroups, Puerto Rican American men reported the highest rate of ever-seeking mental health professionals’ service (32.1%), whereas their use of other health providers over the past 12 months appeared to be higher at a marginal level, compared with Other Hispanics. There was no significant cross-subgroup difference on visiting general practitioner or specialists, over the past 12 months.
Mental Health Service Seeking Reported by Latino American Men in Total and Ethnic Groups of the NLAAS
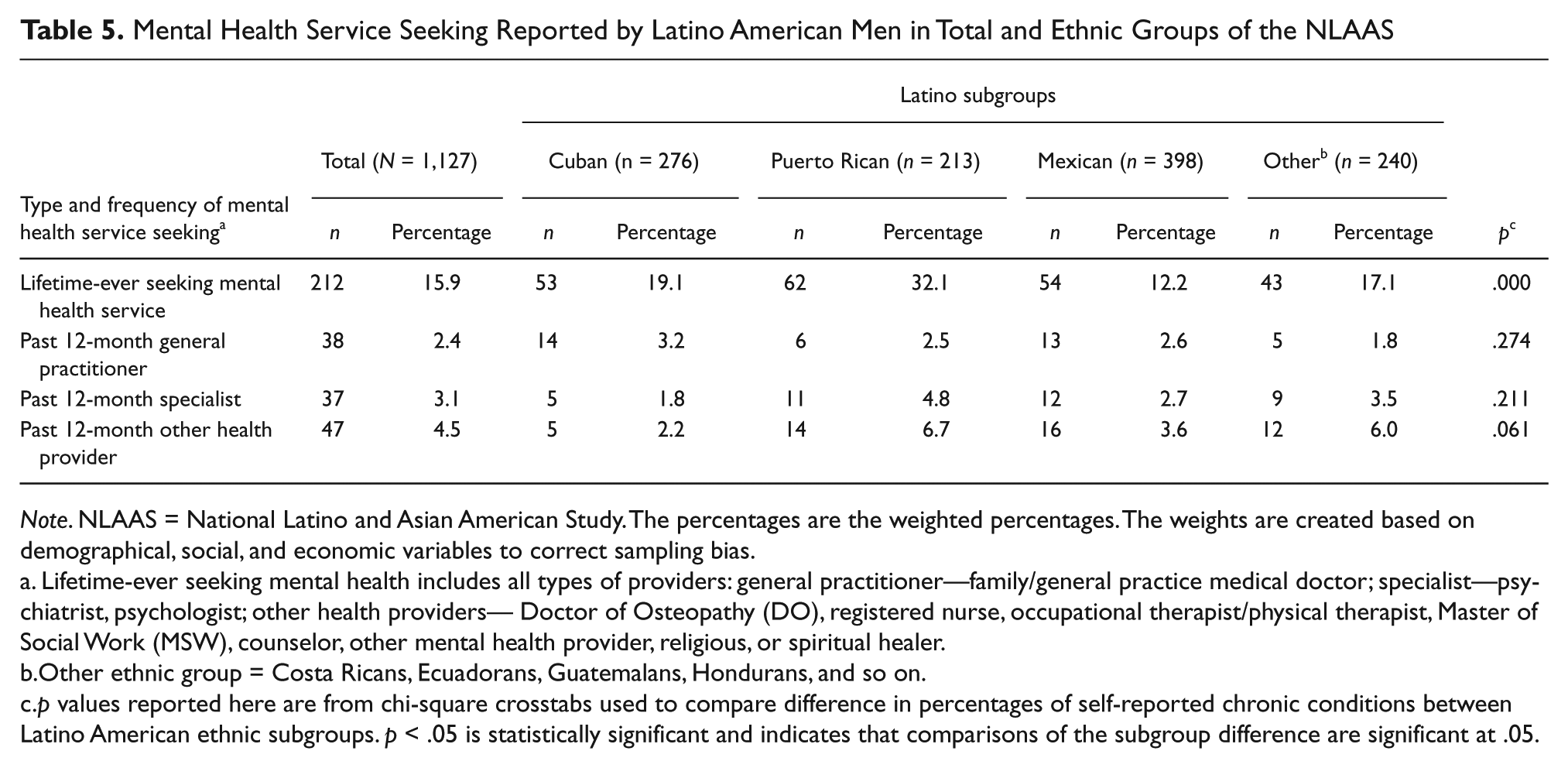
Note. NLAAS = National Latino and Asian American Study. The percentages are the weighted percentages. The weights are created based on demographical, social, and economic variables to correct sampling bias.
Lifetime-ever seeking mental health includes all types of providers: general practitioner—family/general practice medical doctor; specialist—psychiatrist, psychologist; other health providers— Doctor of Osteopathy (DO), registered nurse, occupational therapist/physical therapist, Master of Social Work (MSW), counselor, other mental health provider, religious, or spiritual healer.
Other ethnic group = Costa Ricans, Ecuadorans, Guatemalans, Hondurans, and so on.
p values reported here are from chi-square crosstabs used to compare difference in percentages of self-reported chronic conditions between Latino American ethnic subgroups. p < .05 is statistically significant and indicates that comparisons of the subgroup difference are significant at .05.
Discussion
This study provides the prevalence of the overall health and service utilization of Latino American men in a national representative database, the NLAAS. Our findings suggest that the average of this sample is relatively young (40 years) and about two thirds of participants are immigrants. Although most large-sample studies have focused on SRH (Bzostek et al., 2007, Kandula et al., 2007; Liang et al., 2010; Patel et al., 2003), this study advances the literature with an itemization of chronic conditions among four subgroups of Latino Americans from a national sample. Substantive differences are shown in most illness categories across major subgroups of Latino American men. A major finding is that Puerto Rican American men had higher rates of 8 out of 15 physical ailments. These included life-altering conditions, such as cardiovascular diseases (CVD; e.g., hypertension, heart diseases, and heart attacks), the number one killer of any racial and ethnic subpopulation in the United States (American Heart Association [AHA], 2011).
The ranking pattern of CVD rates among the three major subgroups (Puerto Ricans, Cubans, and Mexicans) appears to resemble the race-related ranking patterns of CVD rates reported by the AHA (2011). That is, African Americans have the highest CVD rates, followed by non-Latino White Americans, and then by Latinos. As can be noted, Puerto Rican Americans have higher proportion of African American heritages and Cuban Americans have higher proportion of European American heritages, respectively. However, despite differences in racial heritage, SES, and geographic locations, rates of certain CVDs (e.g., heart attack and hypertension) among Cuban American men are similar with those of their Puerto Rican counterparts (both higher than those of Mexicans), which leads to questions about the unhealthy lifestyles potentially shared between these two different Latino male subgroups.
The overall CVD rates of subgroups, however, are lower than those reported in the AHA (2011). Concerning hypertension, for example, rates of African Americans, Whites, and Latinos in the AHA (2011) were 32%, 23%, and 22%, respectively, whereas rates of Puerto Ricans, Cubans, and Mexicans in our analyses were only 18%, 17%, and 11%, respectively. Such differences between CVD rates are very likely affected by the younger age of this Latino American male subpopulation in the NLAAS, compared with that of the AHA sample (2011). Despite the seemingly parallel pattern, rates of hypertension among non-Latino Whites in the AHA fell closer to those of Latinos (2011), whereas in the NLAAS rates of Cuban men, are closer to those of Puerto Rican men. One explanation of this is that Puerto Ricans and Cuban Americans are predominantly city dwellers, they, therefore, may have faced similar levels of environmental stress or lifestyles. However, these hypotheses should be verified in the future study.
Significant differences of chronic physical and mental health issues across Latino subgroups nevertheless did not lead to considerable variation in health care utilization rates across subgroups. Contrary to another study about differential physician visits among subgroups of Latino American elderly (Burnette & Mui, 1999), our analysis does not show statistical differences in seeking health care over the past 12 months among the four NLAAS Latino men subgroups. However, since our analyses are Latino male–specific the similar visiting rates across these subgroups may partly be attributable to the younger age cohort in the present study or to the male-gender impact. The age assumption may not be held, because the recent findings on Latino American women revealed different patterns in visiting specialist (Ai et al., 2012). In particular, Cuban American and Puerto Rican Americans saw their general practitioners more often than Mexican Americans (Ai et al., 2012). Still, the flat patterns in men’s health seeking may raise questions about subgroup variations regarding certain unmet needs in health care on top of existing disparities facing Latino Americans, which may be somewhat related to SES (Bzostek et al., 2007, Kandula et al., 2007, Patel et al., 2003, Torres Stone & McQuillan, 2007) or unobserved heterogeneity (Bustamante, et al., 2009).
Concerning behavioral health, Latino American men reported high rates of overweight or obesity, including around three quarters of Mexican, Cuban, or “Other” Latino Americans and nearly two third of their Puerto Rican counterparts have BMI > 25 kg/m2. This overall pattern is alarming, given that overweight may contribute to more physical and mental health problems. Regarding substance abuse, current smoking, marijuana usage, and cocaine use are all prevalent in high rates (more than a quarter, nearly 40%, or more than one sixth, respectively) among Latino American men. Puerto Rican men reported especially high rates on all three categories (more than one third on smoking, more than a half on marijuana, and more than a quarter on cocaine, respectively), and on other drugs. Consistently with men’s data, our recent finding showed the highest substance abuse rates among Puerto Rican American women than other Latino American women (Ai et al., 2012). This cross-gender similarity thus calls for special attention to developing specialized intervention or prevention programs against substance abuse for Puerto Rican Americans as well as to further investigation in their risk behaviors. Puerto Rican men’s and women’s high prevalence of substance abuse may help partly explain their highest rates in lifetime-ever seeking for mental health service in these analyses (Ai et al., 2012), compared with Other Latino American men and women, as well as in other findings (Albizu-Garcia et al., 2001; Vega et al., 2009).
Although the National Comorbidity Survey studies documented low risk for major mental health disorders (Breslau et al., 2006; Ortega, 2000) and for lifetime substance use (Breslau, Kendler, Gaxiola-Aguilar, & Kessler, 2005) among Latino Americans, this fact may not be applicable to Puerto-Rican Americans, as noted in the NLAAS (Alegría, Mulvaney-Day, Torres, Polo, Cao, & Canino, 2007). Rates of Latino American men having a major depression diagnosis in our analysis are as high as that of their Latino American women counterparts (Ai et al., 2012). However, depression among Puerto Rican American men is much higher than that of men in other Latino subgroups. Nearly 1 of 10 Puerto Rican men met the criterion over the past 12 months, consistent with the high prevalence of depression among Puerto Rican American women (Ai et al., 2012). Additionally, given their high rates on all substance abuse items, Puerto Rican men may be more likely to have dual diagnoses, consistent with Vega et al.’s (2009) finding. Despite the greater likelihood of depression and substance use, Puerto Rican American men do not rate their mental health worse than other subgroups in our findings. Specifically, they are less likely to self-report their health as “poor” or “fair” compared with Mexican Americans. This self-evaluation may partly contribute to their service utilization at the statistically similar level of other Latino subgroups over the past 12 months.
Clearly, the present study and other NLAAS findings (Alegría et al., 2006) imply that results from one Latino American subgroup should not be generalized to other Latino subgroups. Whereas higher rates of mental and behavioral health problems of Puerto Rican American women may be attributed to their stressful overrepresentation of households headed by single women (Ai et al., 2012), this rationale cannot explain the similar high rates among Latino American men. Indeed, gender- and race-specific health analyses are essential in the U.S. Latino populations (Borrell & Dallo, 2008, Flores et al., 2002; Torres Stone & McQuillan, 2007). Given distinct differences in these Latino subgroups (Derose et al., 2009; Torres Stone & McQuillan, 2007), further research is warranted on differential risk factors in Latino male subgroups, including the interplay of biological and environmental determinants, so as to better understand their etiologies among Latinos, especially men. In addition, researchers should explore specific protective variables such as cultural beliefs, spirituality, and lifestyles that may play significant roles in seeking health services, in promoting physical well-being, and in self-reporting mental health.
Although Latino American men belong to a major minority group in consumers’ pool for care, they reported low utilization of either general practitioners or specialists over the past 12 months. The finding is consistent with those from the Medical Expenditure Panel Survey of their low rates of ambulatory visits and of prescription medications (Weinick et al., 2004). The low health care utilization could be because of the Latino men’s self-perception of better mental and physical health, as reported by Albizu-Garcia et al. (2001). Alternatively, Pérez-Escamilla (2010) noted that around one third of Latino Americans are without health insurance.
Research does support that in general, men of all ethnic/racial groups have low health care utilization when compared with women (Addis & Mahalik, 2003). These facts may contribute to low professional care–seeking rates in the current study. However, national studies conducted concurrently with the NLAAS report that Latinos are less likely (60.7%) than Whites (82.3%) to have access to care, to have a usual source of care, to be seen in physicians’ offices, and to have continuity of care with the same provider, and more likely to have poor communications with their providers (Chowdhury, Balluz, Okoro, & Strine, 2006; Freeman & Lethbridge-Cejku, 2006; Ku & Waidmann, 2003). Latinos were more likely to not receive (6.5%) or to delay (7.4%) medical care because of cost, compared with non-Latino Whites (4.9% and 7.3%, respectively; Schiller, Adams, & Coriaty Nelson, 2005). Fifty-eight percent of Latino men made office visits to a doctor or other health care professional in the past 12 months compared with 78.7% of non-Latino White men (Schiller, Lucas, Ward, & Peregoy, 2012). Only 4.8% of Latino men had an overnight hospital stay during the past 12 months, compared with 7.3% of non-Latino White men (Schiller et al., 2005), and Latino patients, overall, were less likely than Whites to use high-technology hospitals (Kim, Samson, & Lu, 2010).
Our study has several limitations. The NLAAS was based on psychiatric disorders defined by the Western DSM-IV, which allowed us to compare mental disorders within the same measure. However, rates of mental disorders may have been underestimated, as different ethnic groups might express their mental health problems in distinctive ways not identified in the DSM-IV. The NLAAS focuses on large samples of Cuban, Mexican, Puerto Rican Americans, whereas “other Latinos” were integrated into a single category even though they represent a variety of languages, ethnicities, cultures, and practices. Subgroups from Guatemala, Honduras, and other Latin American countries may not be well represented. Despite our limitations, the findings underscore the importance of increasing awareness of cross-cultural and gender differences of chronic, behavioral, and mental health issues in Latino American men to better inform health care providers and researchers.
Findings regarding subgroup differences will inform the culturally sensitive design of future physical and mental health services for such “highly heterogeneous” populations (Brady, Ho, Kelley, & Clancy, 2007). Primary care providers could deliver better care services for ethnic subgroup Latino men, if they are more adequately informed concerning the differential patterns in overall health, as presented in the current analysis.
Footnotes
Authors’ Note
Opinions presented here do not represent those of the funder.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors declared receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by a grant from the University of Pittsburgh’s Center on Race and Social Problems to the corresponding author, Amy L. Ai.